Embed Size (px)
Citation preview
HERNIAS then (1990) and now (2011)
Steven E. Swartz, MD, FACS
Surgical Associates of Richmond
Objectives
Understand Hernia Types
Understand Where We Are Today Concerning
Repair
Understand Anatomy Associated With Various
Types Of hernia
Understanding the Repairs and What
Documentation needs to be on the report.
What do we tell patients?
Do all hernias need to be repaired?
Should mesh be used?
Open or laparoscopic?
What is a hernia?

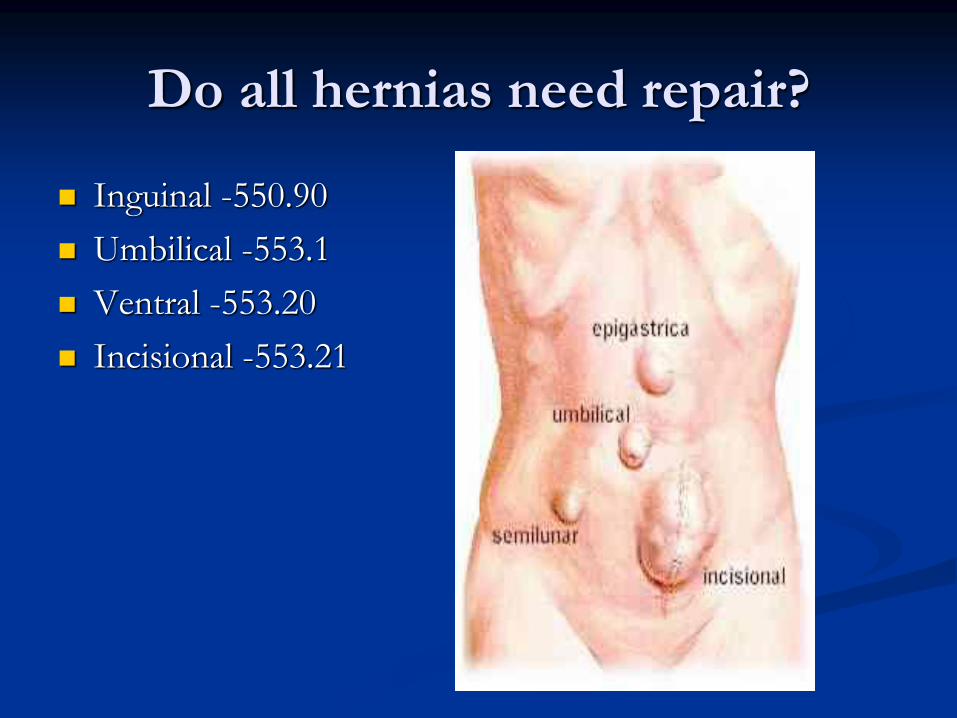
Do all hernias need repair?
Inguinal -550.90
Umbilical -553.1
Ventral -553.20
Incisional -553.21
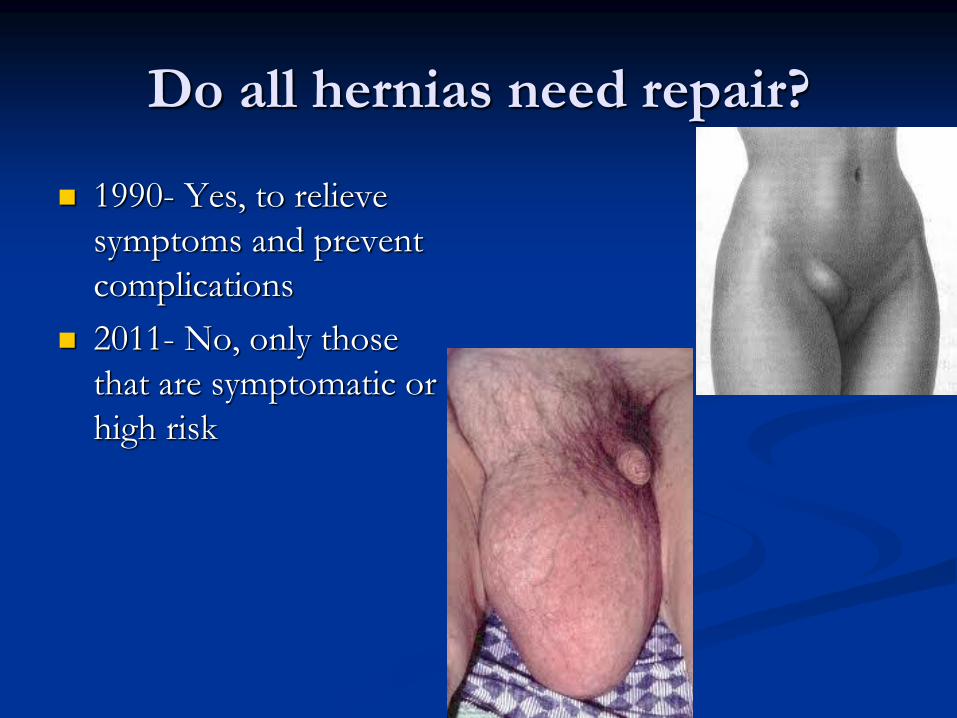
Do all hernias need repair?
1990- Yes, to relieve
symptoms and prevent
complications
2011- No, only those
that are symptomatic or
high risk
Watchful waiting
Inguinal hernias Fitzgibbons et al 720 men with
minimal symptoms
23% had surgery within 2 years
Serious complications were rare in the non-
operated group
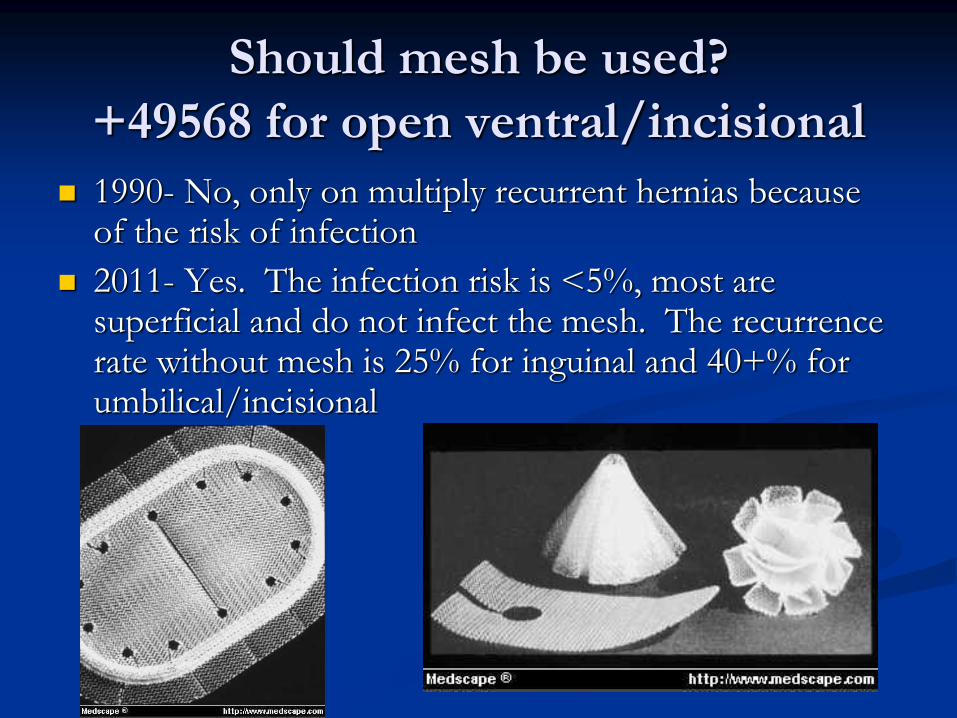
Should mesh be used?
+49568 for open ventral/incisional
1990- No, only on multiply recurrent hernias because of the risk of infection
2011- Yes. The infection risk is <5%, most are superficial and do not infect the mesh. The recurrence rate without mesh is 25% for inguinal and 40+% for umbilical/incisional
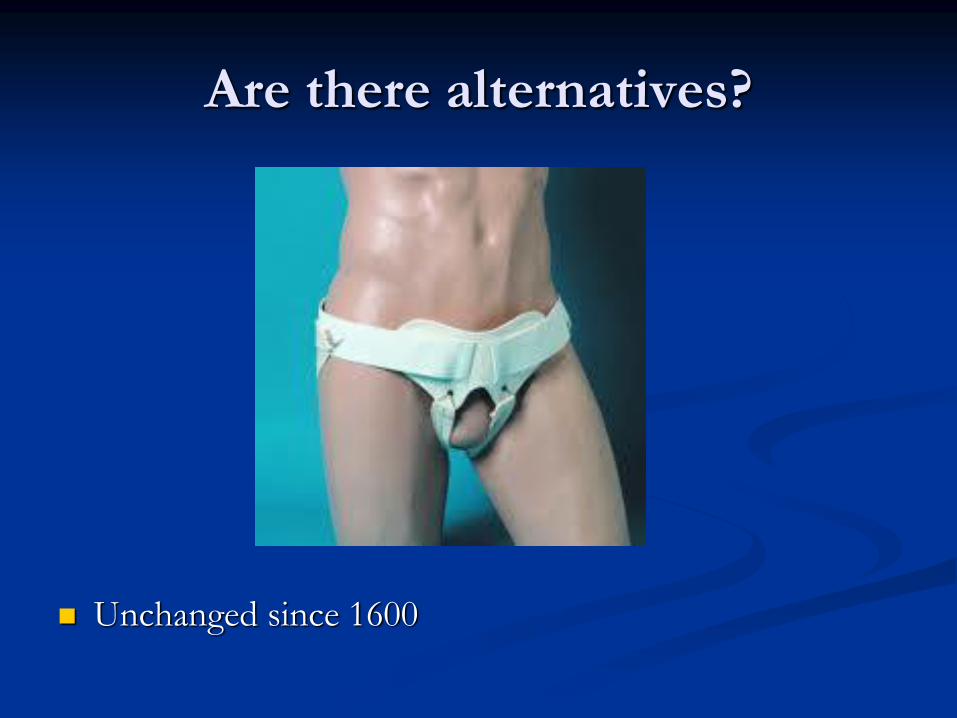
Are there alternatives?
Unchanged since 1600
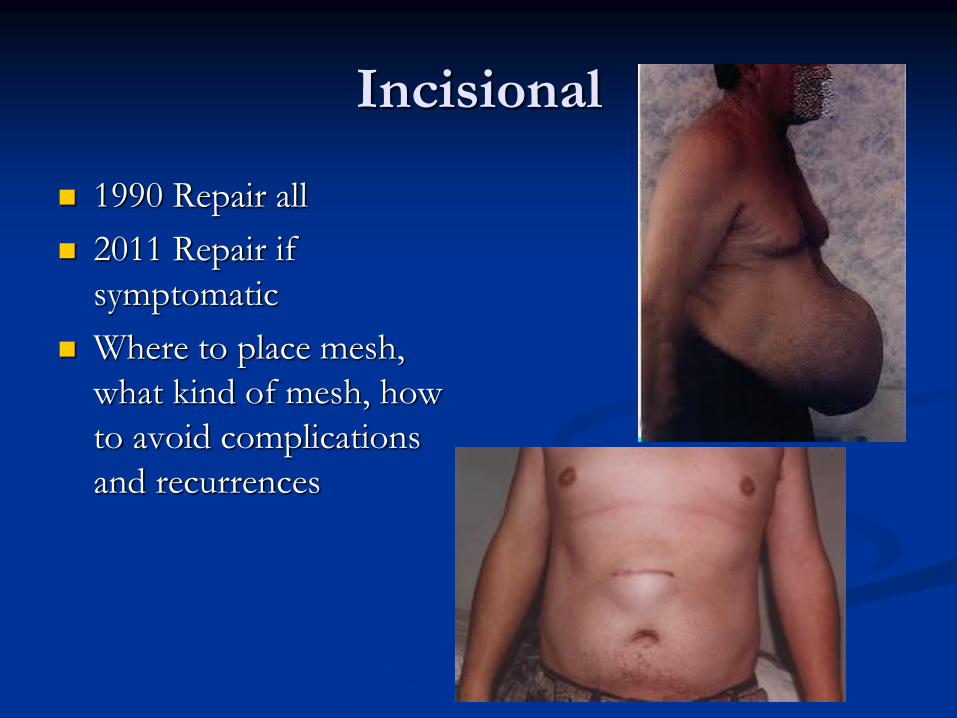
Incisional
1990 Repair all
2011 Repair if
symptomatic
Where to place mesh,
what kind of mesh, how
to avoid complications
and recurrences
Inguinal-Laparoscopic or open?
1990-Laparoscopic
General anesthesia
More difficult dissection
Less secure mesh
Higher recurrence rate
Fewer infections
More major complications
Less pain
2011-Open
Local/sedation
Quick/simple
More secure mesh
Fewer recurrences
No major complications
Modest pain-most back to work in 1 week

Incisional hernias
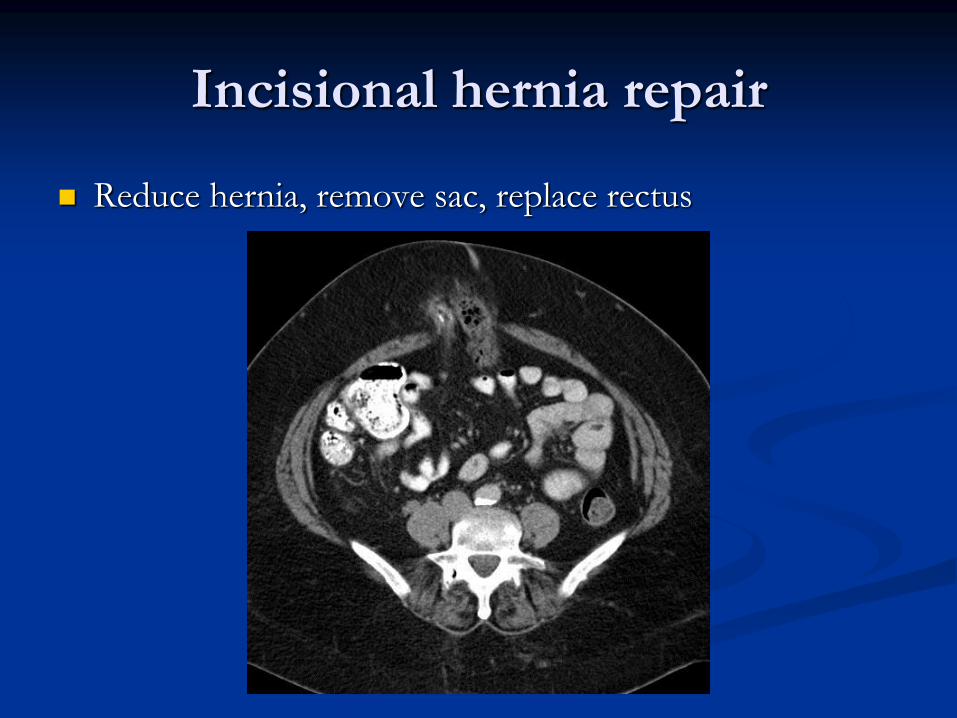
Incisional hernia repair
Reduce hernia, remove sac, replace rectus

Large Incisional Hernia
553.21/552.21
K43.91/K43.01
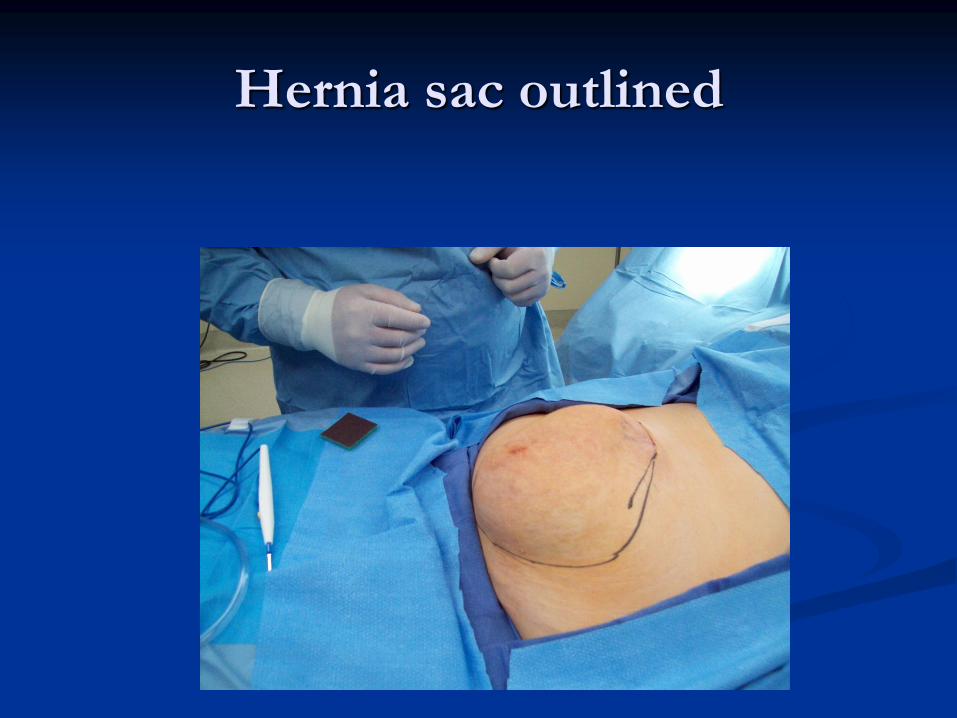
Hernia sac outlined
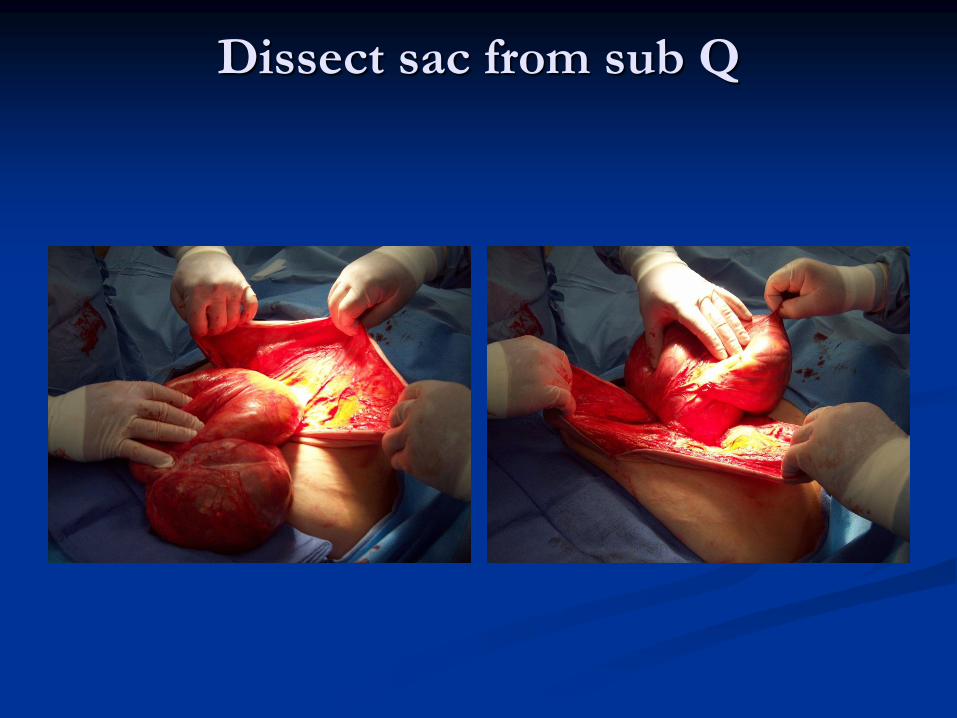
Dissect sac from sub Q

Remove sac
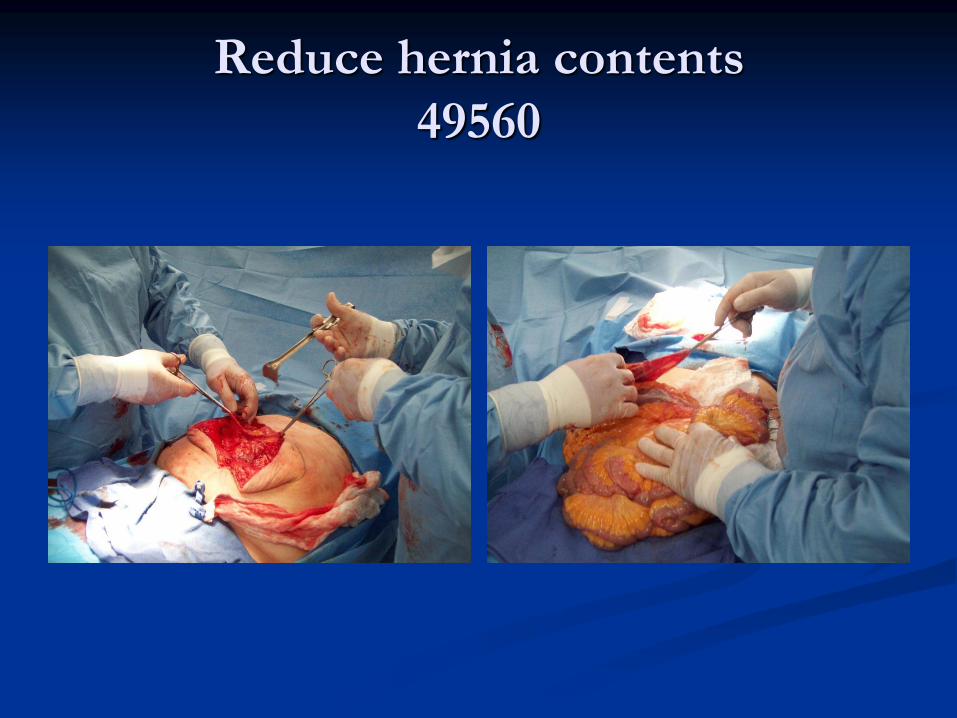
Reduce hernia contents
49560
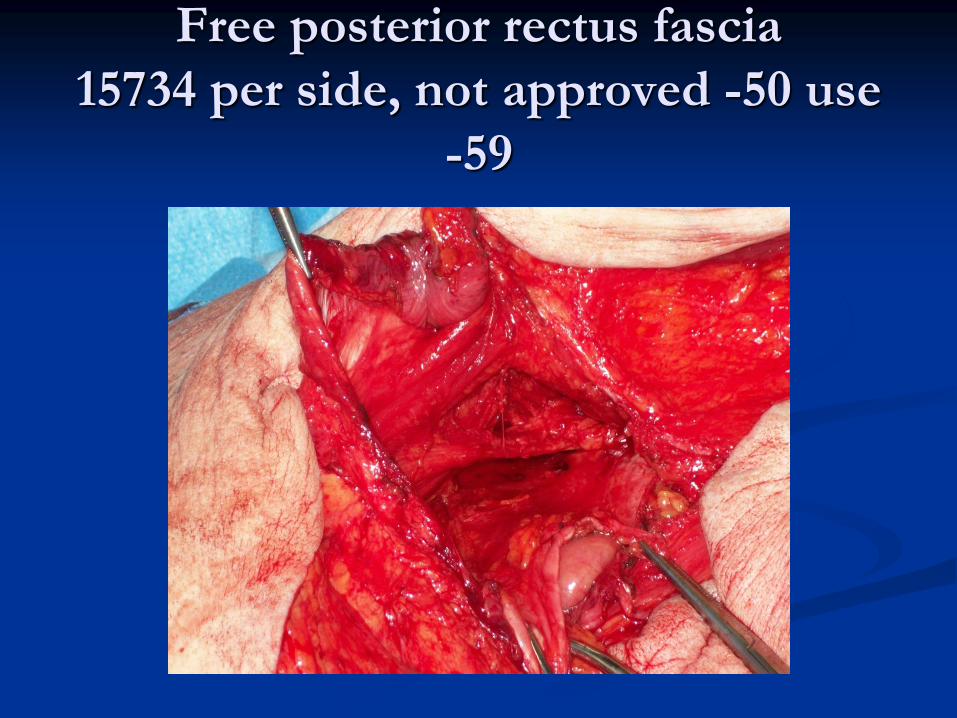
Free posterior rectus fascia
15734 per side, not approved -50 use
-59
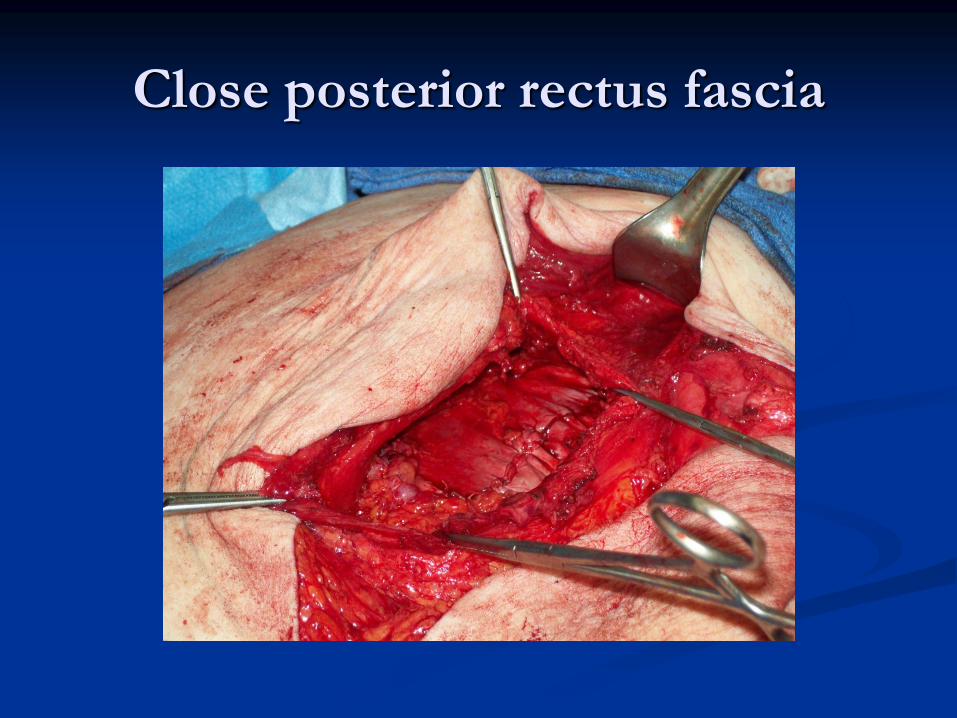
Close posterior rectus fascia
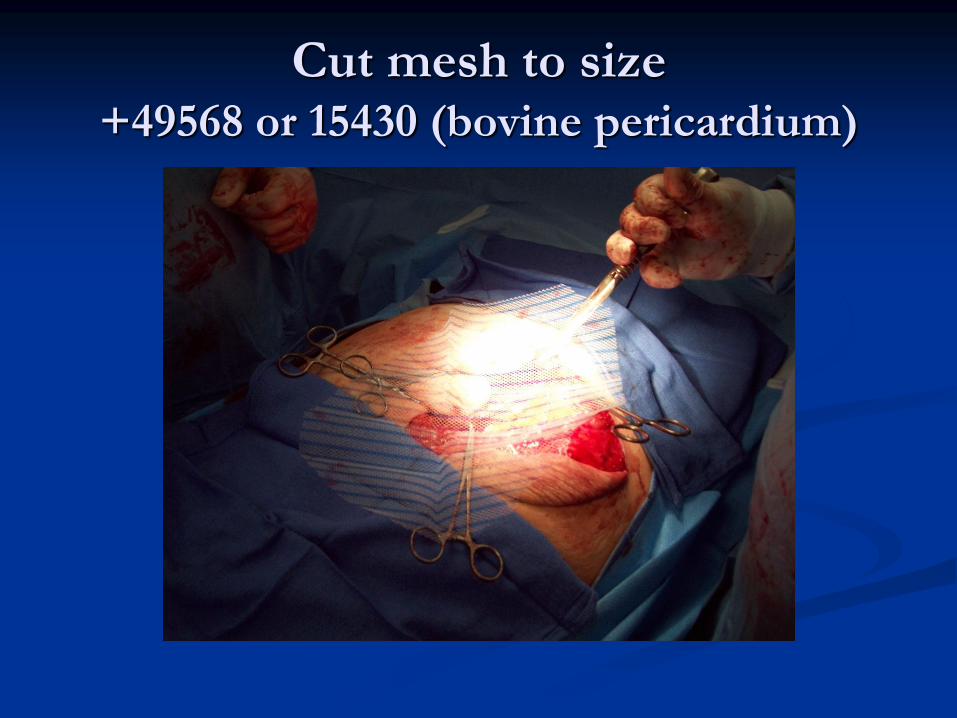
Cut mesh to size +49568 or 15430 (bovine pericardium)
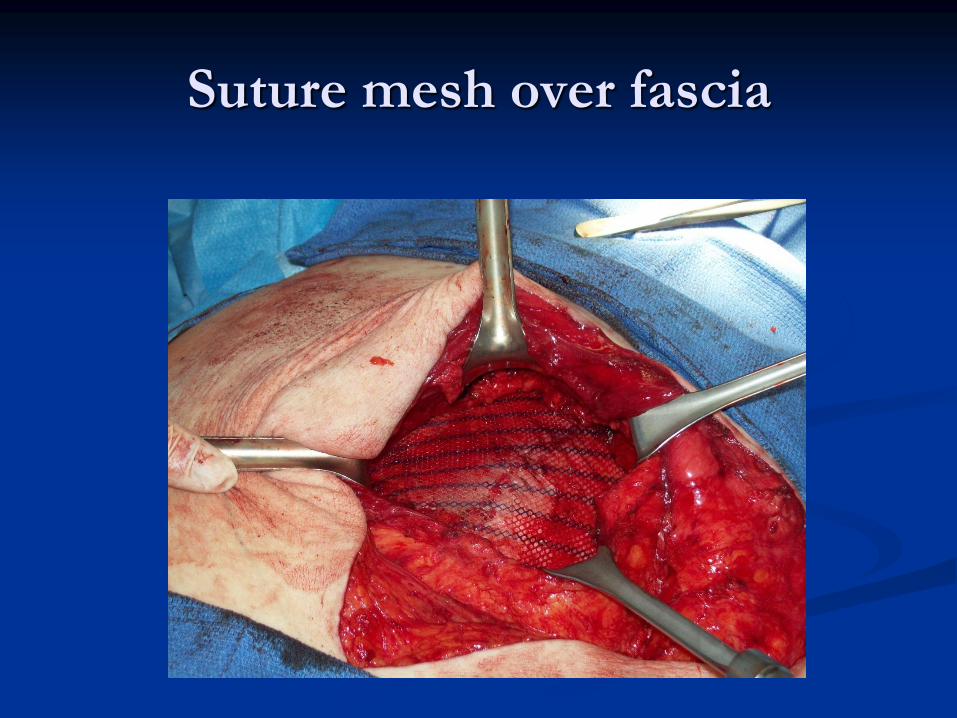
Suture mesh over fascia

Close anterior fascia over mesh

Make it pretty
13101/+13102
Complex problems
50 yo woman, prior mesh repair X 2
Chronic infected mesh (MRSA)
Morbidly obese (450 lb, 5’6’’)
Biologic mesh
Human skin, porcine skin or intestinal
submucosa, bovine pericardium
Treated to remove antigenic proteins
Reduced to collagen matrix
Attracts host stem cells which differentiate into
native tissue
Becomes vascularized/replaced
Resists infection
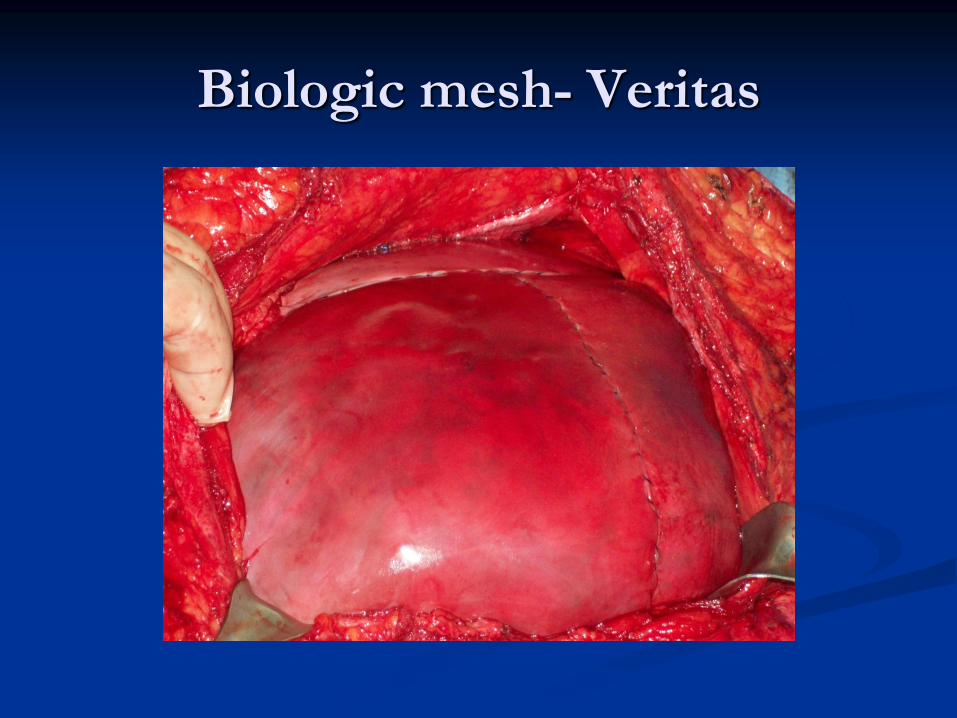
Biologic mesh- Veritas

One year later
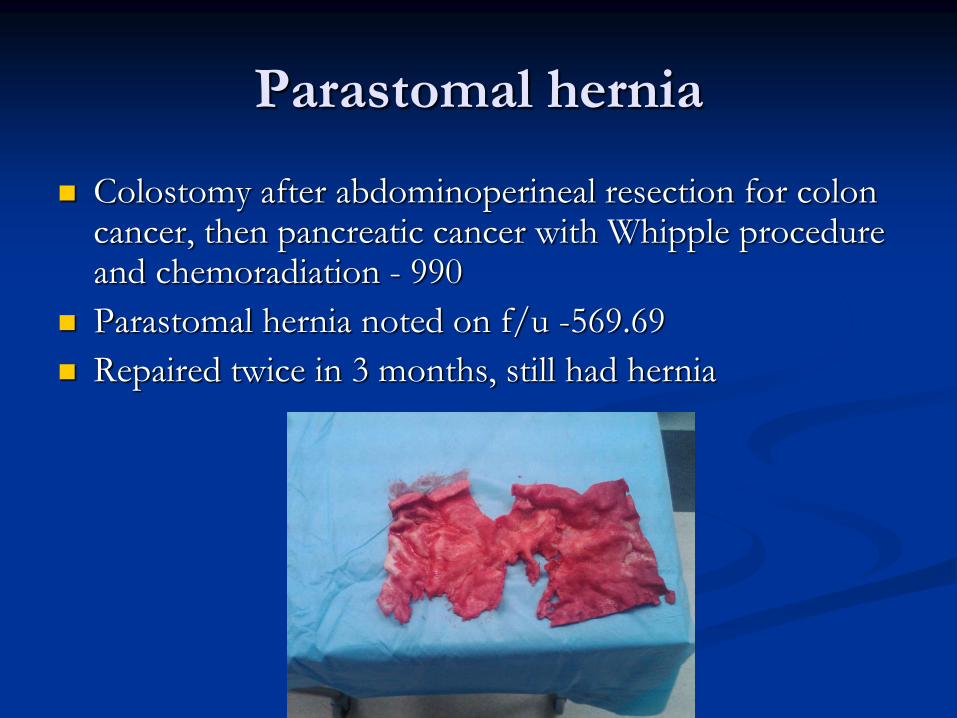
Parastomal hernia
Colostomy after abdominoperineal resection for colon cancer, then pancreatic cancer with Whipple procedure and chemoradiation - 990
Parastomal hernia noted on f/u -569.69
Repaired twice in 3 months, still had hernia
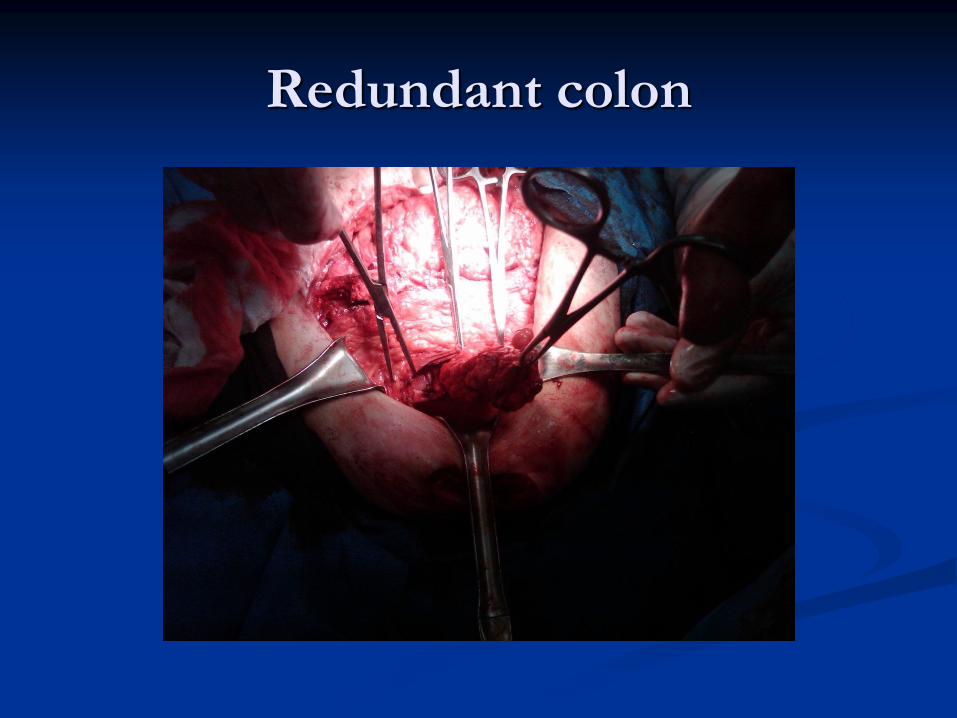
Redundant colon
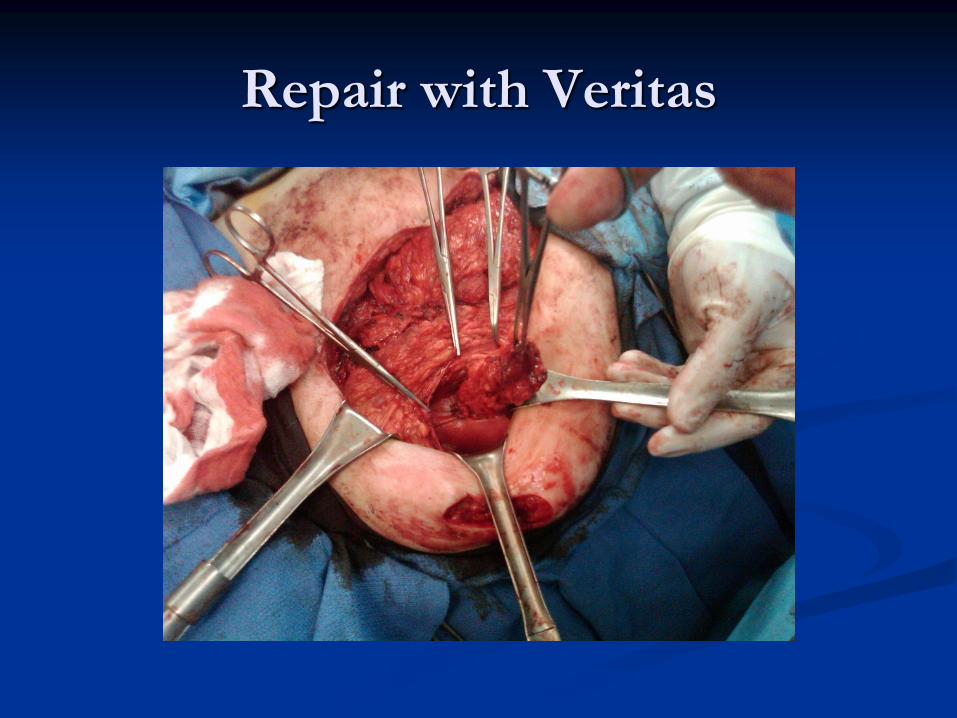
Repair with Veritas
The next generation