Embed Size (px)
Citation preview
46
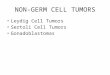
Rhabdoid TumorALL Non-CNS rhabdoid tumors treated on the High Risk Renal Tumor Protocol
Genetic Evaluation for INI-1 deletions and BAF47 expression performed on all patients
Treatment: New regimen

47
Diagnostic Difficulties
Pseudo-Rhabdoid Phenotype in Primary Renal Tumors and Metastatic Tumors– INI-1 Positive in Pseudo-Rhabdoid Tumors
Biopsy of Extra-Renal Mass
Mistaken for Rhabdomyosarcoma (RT negative for myogenic markers)
Sclerosing Pattern Resembles DSRCT
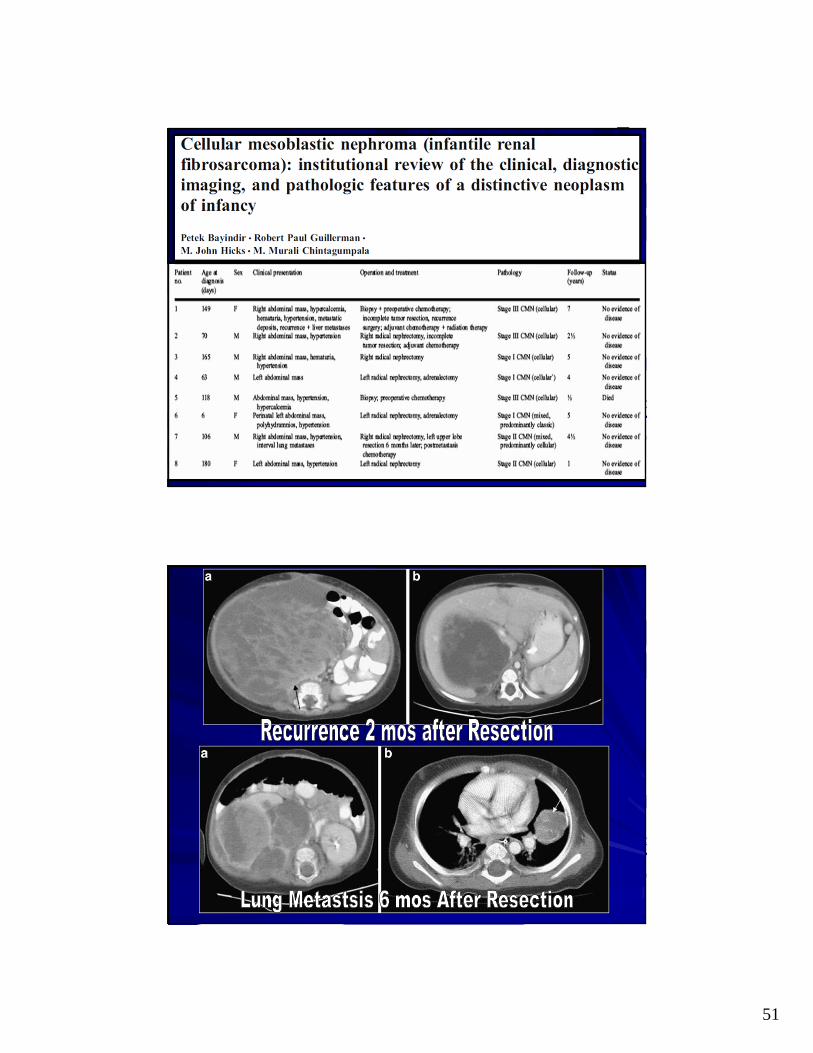
Congenital Mesoblastic Nephroma
Median Age at Diagnosis 2 Months90% in 1st Year of Life (not reported >2yr of age)Most Common Congenital Tumor of the KidneyDetection In Utero: Abdominal Mass, Polyhydramnios, Hydrops & Premature DeliverySize 0.8 to 14 cm (median 6.2cm)Solitary, Unilateral Soft to Firm Masses with Bulging Cut SurfaceCysts, Hemorrhage & Necrosis CommonNot Associated with WT or NR (rarely in BWS)
48
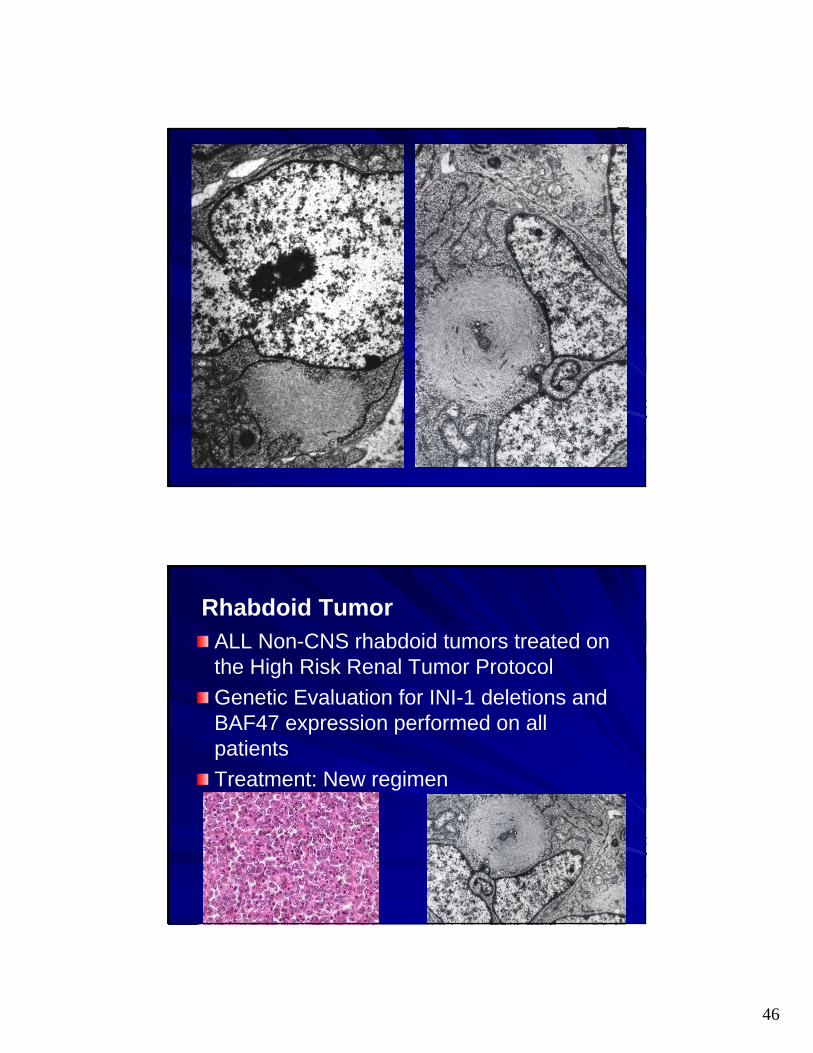
Congenital Mesoblastic Nephroma
Classic 22% Infantile fibromatosis
Cellular 58% Infantile
fibrosarcoma
Mixed 20%
Mean age all 4.4 moMean age classic 3.2 moMean age cellular 4.9 mo
49
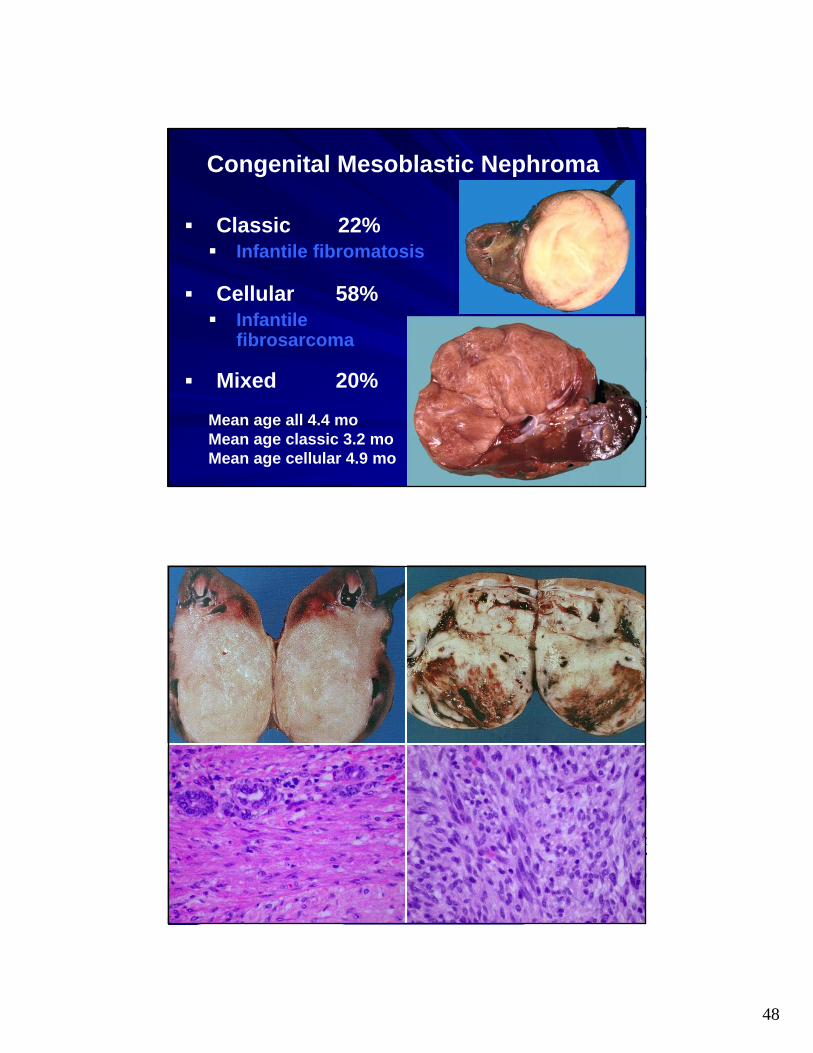
CMN: Classic vs Cellular
Classic– Interface with Kidney:
Irregular, Interdigitating
– Elongated Spindled Cells
– Infantile Fibromatosis Appearance
– Cytogenetics: ?– Mean Age: 3.2 Months
Cellular– Interface with Kidney:
Circumscribed, Not Encapsulated
– Plump, Slightly Spindled Cells
– Infantile Fibrosarcoma Appearance
– t(12;15) – ETV6/NTRK3– Mean Age: – 4.9 Months
Hypercalcemia: Prostaglandin E Produced by TumorHyperreninism: Entrapped Normal Renal Elements
50
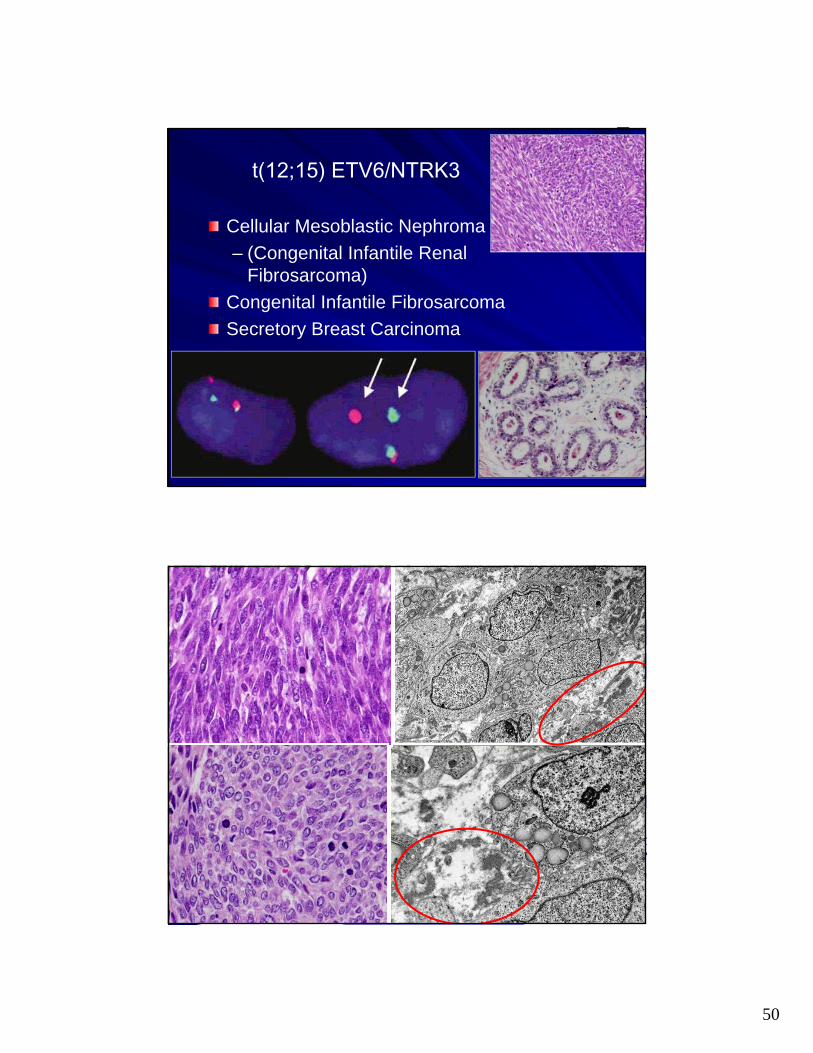
t(12;15) ETV6/NTRK3
Cellular Mesoblastic Nephroma
– (Congenital Infantile Renal Fibrosarcoma)
Congenital Infantile Fibrosarcoma
Secretory Breast Carcinoma
51
52
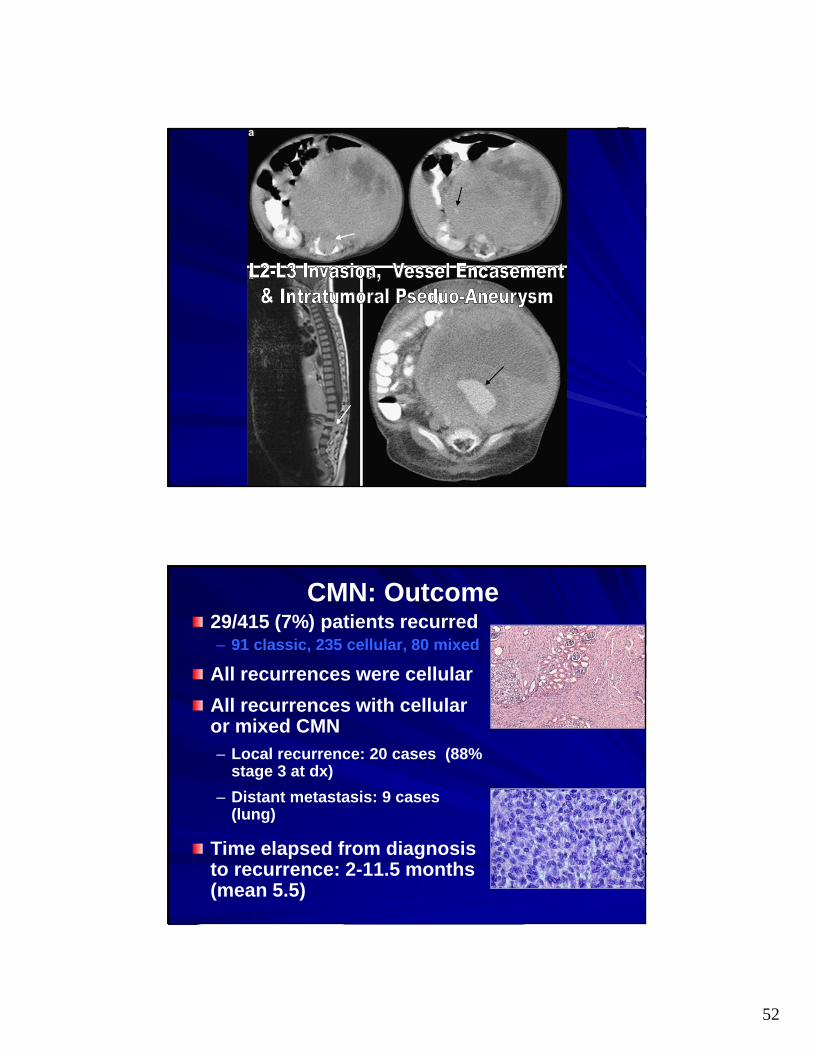
CMN: Outcome29/415 (7%) patients recurred– 91 classic, 235 cellular, 80 mixed
All recurrences were cellular
All recurrences with cellular or mixed CMN– Local recurrence: 20 cases (88%
stage 3 at dx)
– Distant metastasis: 9 cases (lung)
Time elapsed from diagnosis to recurrence: 2-11.5 months (mean 5.5)
53
CMN: ConclusionsMost Important Determinant of Recurrence is Histologic Subtype
Stage 3 disease in Cellular CMN Correlates with Local Recurrence
Cellular CMN Treated With Infantile Fibrosarcoma Therapy– No adjuvant therapy if no gross residual
tumor– Adjuvant chemotherapy if residual tumor
Cellular CMNs with Microscopic Residual Disease Monthly Abdominal US for 1 Year
Diagnostic Difficulties in CMN
Cellular CMN – Mistaken for Clear Cell Sarcoma of Kidney, Rhabdoid Tumor or Primitive Sarcoma
Stromal WT – Indistinct Border & SMA in CMN; Blastema & WT1 in WT
Metastatic CMN – Confused with Other Spindle Cell Malignancies
54
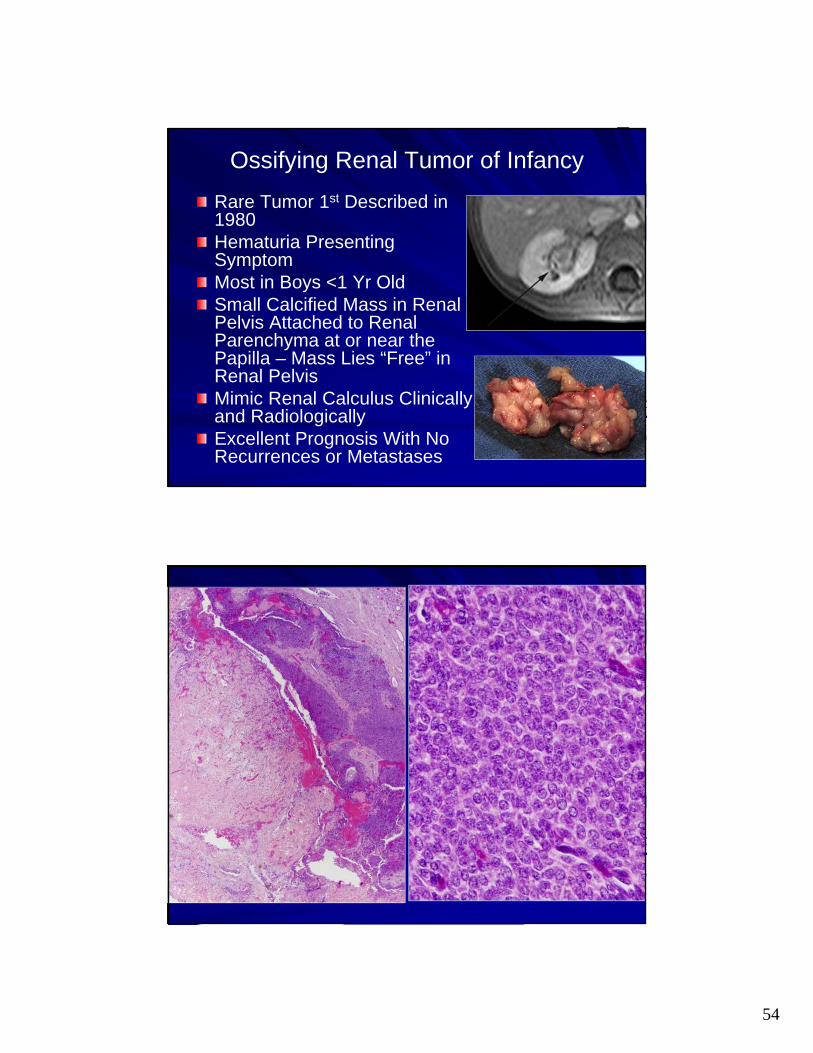
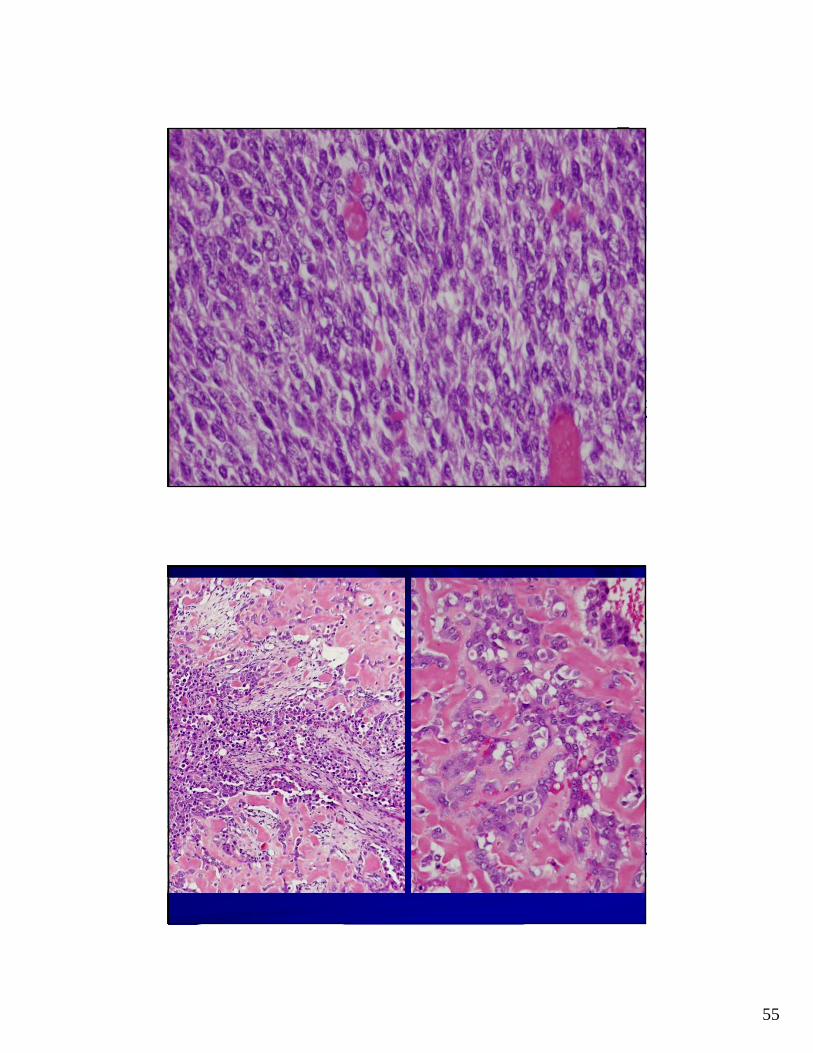
Ossifying Renal Tumor of Infancy
Rare Tumor 1st Described in 1980Hematuria Presenting SymptomMost in Boys <1 Yr OldSmall Calcified Mass in Renal Pelvis Attached to Renal Parenchyma at or near the Papilla – Mass Lies “Free” in Renal PelvisMimic Renal Calculus Clinically and RadiologicallyExcellent Prognosis With No Recurrences or Metastases
55
56
57
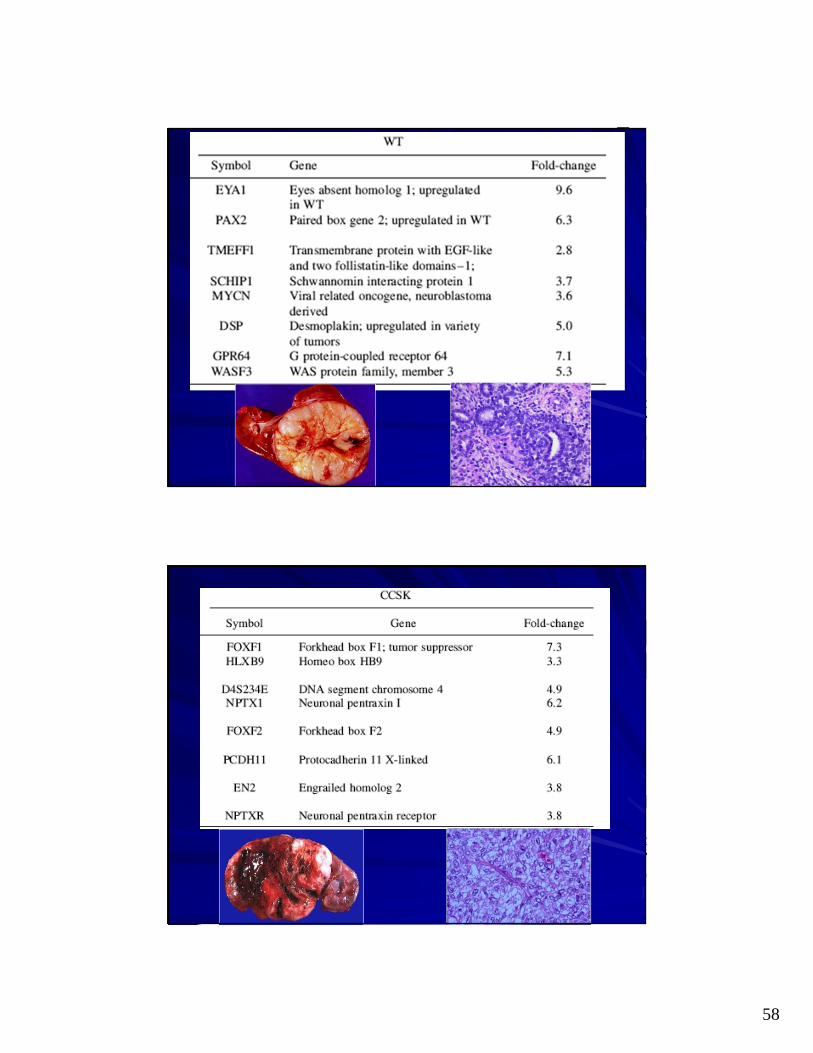
58
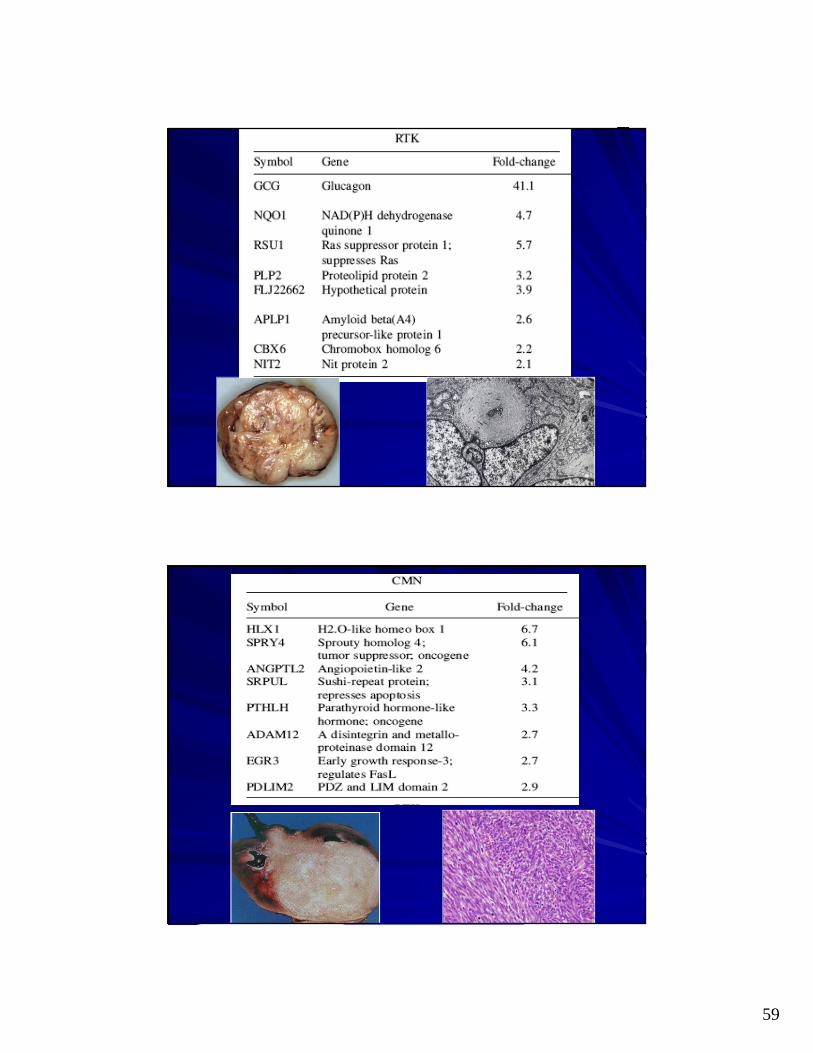
59
60
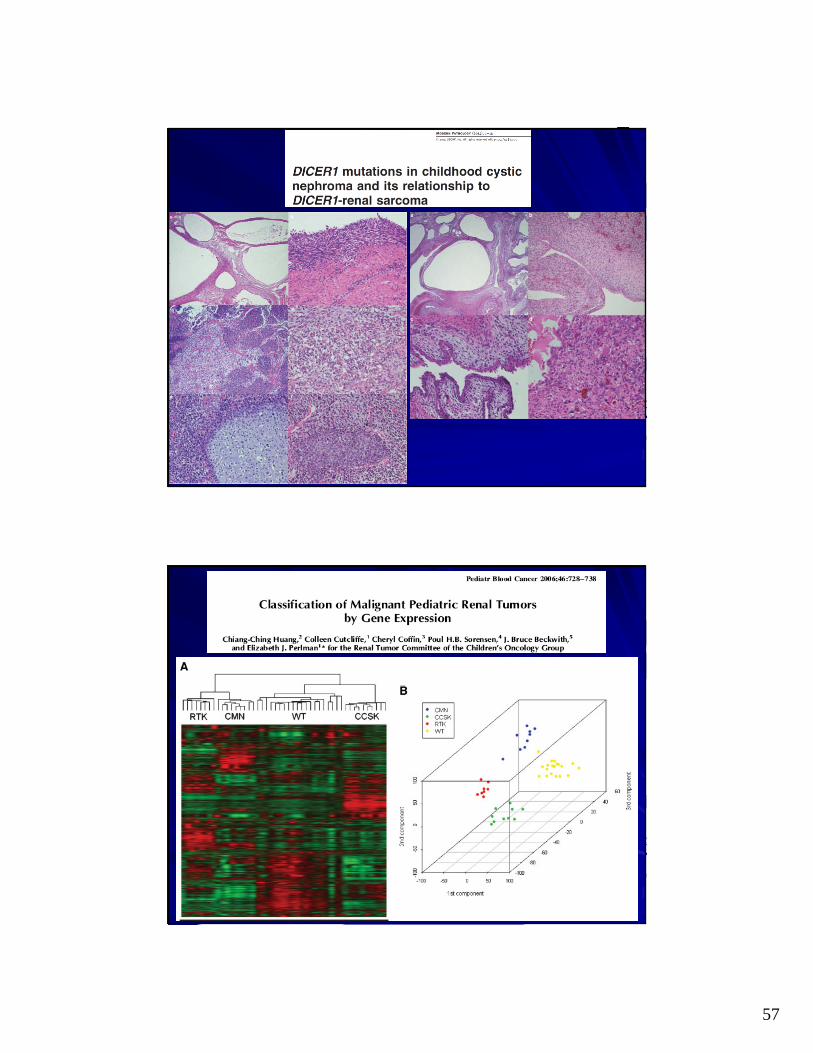
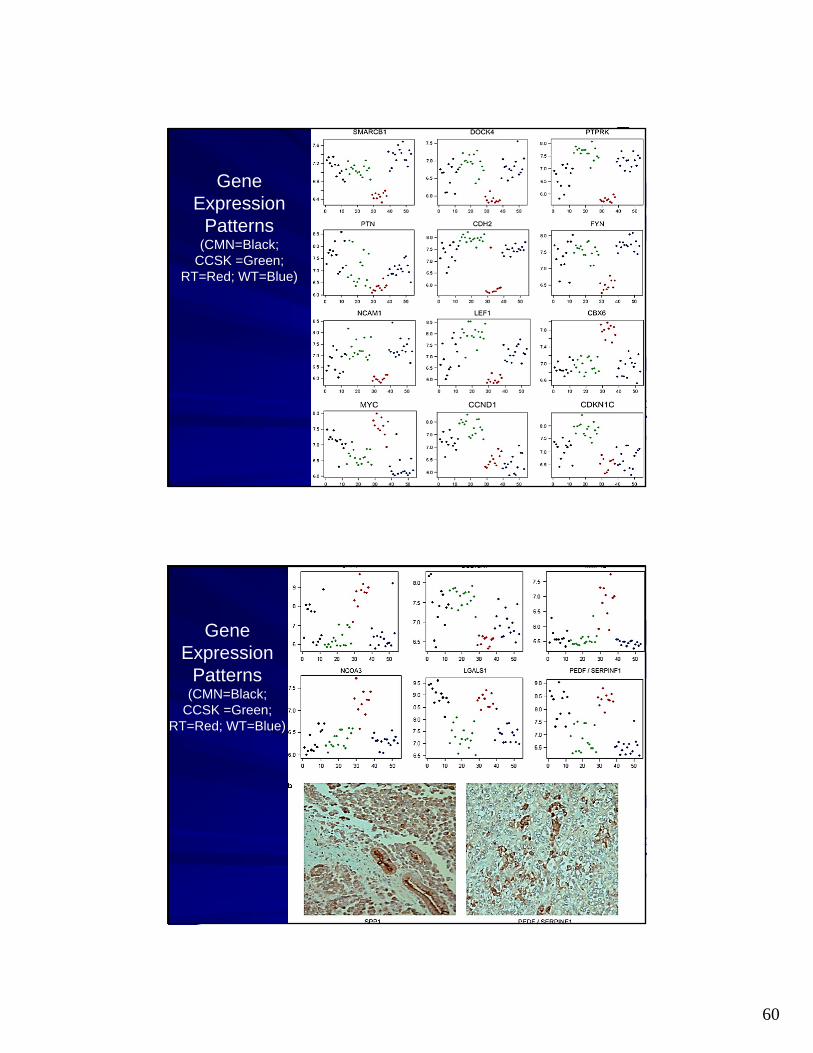
Gene Expression
Patterns (CMN=Black;
CCSK =Green; RT=Red; WT=Blue)
Gene Expression
Patterns (CMN=Black;
CCSK =Green; RT=Red; WT=Blue)





![Pseudo Limits, Biadjoints, and Pseudo Algebras: Categorical ...arXiv:math/0408298v4 [math.CT] 18 Oct 2006 Pseudo Limits, Biadjoints, and Pseudo Algebras: Categorical Foundations of](https://img.pdfslide.net/doc/110x75/60a7a6d20b1ec1029337c248/pseudo-limits-biadjoints-and-pseudo-algebras-categorical-arxivmath0408298v4.jpg)