Embed Size (px)
Citation preview
M A J O R A R T I C L E
High Morbidity and Mortality in AdultsHospitalized for Respiratory Syncytial VirusInfections
N. Lee,1,2 G. C. Y. Lui,1 K. T. Wong,3 T. C. M. Li,1 E. C. M. Tse,1 J. Y. C. Chan,4 J. Yu,3 S. S. M. Wong,3 K. W. Choi,1
R. Y. K. Wong,1 K. L. K. Ngai,5 D. S. C. Hui,1,2 and P. K. S. Chan2,5
1Department of Medicine and Therapeutics, 2Stanley Ho Center for Emerging Infectious Diseases, 3Department of Radiology and Organ Imaging,4The Jockey Club School of Public Health and Primary Care, and 5Department of Microbiology, Chinese University of Hong Kong, Hong Kong SpecialAdministrative Region, China
Background. Better understanding of complications and outcomes of adults hospitalized with respiratory syn-cytial virus (RSV) infection is necessary.
Methods. A retrospective cohort study was conducted on all adults (≥18 years) admitted to 3 acute care generalhospitals in Hong Kong with virologically confirmed RSV infection during 2009–2011 (N = 607). Adults hospital-ized for seasonal influenza during the period were used for comparison (n = 547). Both infections were prospectivelydiagnosed following a standard protocol. Independent reviews of chest radiographs were performed by radiologists.Main outcome measures were all-cause death, respiratory failure requiring ventilatory support, and hospitalizationduration. Cox proportional hazards models were used for analyses.
Results. The mean age of RSV patients was 75 (SD, 16) years; 87% had underlying conditions. Lower respiratoryand cardiovascular complications were diagnosed in 71.9% (pneumonia, 42.3%; acute bronchitis, 21.9%; chronic ob-structive pulmonary disease/asthma exacerbation, 27.3%) and 14.3% of patients, respectively; 12.5% had bacterialsuperinfections. Supplemental oxygen and ventilatory support were required in 67.9% and 11.1%, respectively.Crude all-cause mortality was 9.1% and 11.9% within 30 days and 60 days, respectively; mean length of stay of survi-vors was 12 (SD, 13) days. Advanced age, radiographic pneumonia, requirement for ventilation, bacterial superin-fection, and elevated urea level and white blood cell count were independently associated with poorer survival.Systemic corticosteroid use was associated with longer hospitalization and secondary infections. The overall out-comes of survival and length of stay were not significantly different from those in influenza.
Conclusions. RSV can cause severe lower respiratory complications in older adults, resulting in respiratoryfailure, prolonged hospitalization, and high mortality similar to seasonal influenza. Corticosteroids did not seem toimprove outcomes. The unmet need for antiviral therapy and vaccination against RSV in adults should be promptlyaddressed.
Keywords. RSV; hospitalization; respiratory failure; lower respiratory tract infection; adults.
Respiratory syncytial virus (RSV) is known to be animportant cause of lower respiratory tract infection in
infants and young children, leading to hospitalizationsand deaths [1]. Its impact in adults, however, has onlybeen appreciated in recent years. It has been estimatedthat RSV infects 3%–10% of adults annually; althoughmost infections are mild, increasing evidence suggeststhat severe lower respiratory tract infections can occur,especially among older adults and those with underlyingconditions [2–4]. RSV may have accounted for 5%–15%of community-acquired pneumonia, 9%–10% of hospi-tal admissions for acute cardiorespiratory diseases, andexcessive deaths during seasonal peaks [3, 4]. The disease
Received 23 March 2013; accepted 8 June 2013.Correspondence: N. Lee, MD, Chinese University of Hong Kong, 9/F Clinical
Sciences Bldg, Prince of Wales Hospital, Shatin, Hong Kong, SAR ([email protected]).
Clinical Infectious Diseases© The Author 2013. Published by Oxford University Press on behalf of the InfectiousDiseases Society of America. All rights reserved. For Permissions, please e-mail:[email protected]: 10.1093/cid/cit471
Outcomes of Hospitalized Adults With RSV • CID • 1
Clinical Infectious Diseases Advance Access published August 13, 2013
by Norm
an Sharples on August 20, 2013
http://cid.oxfordjournals.org/D
ownloaded from

burden of RSV can approach that of influenza [3, 5–8]. However,except, perhaps, in the profoundly immunosuppressed, little isknown about the clinical manifestations, complications, and out-comes of severe RSV infections in adults. Factors associated withsevere and fatal infections are largely unknown. Data from Asiancountries are particularly scarce [9–12].
This study examined a large cohort of adults hospitalizedwith laboratory-confirmed RSV infections in Hong Kong, China.Clinical, laboratory, and radiological findings were reported andanalyzed to identify factors associated with pneumonia develop-ment, respiratory failure, and death. Their severity of illness andoutcomes were compared with patients admitted for seasonalinfluenza during the same period. Such information, whenavailable, not only improves our understanding on severe RSVdisease in adults and its impact on the healthcare system, butalso provides valuable data to support future planning of clini-cal trials on RSV therapeutics and prevention.
METHODS
Study Population and Case Finding ProceduresA retrospective cohort study on hospitalized adults with RSVinfections was conducted. All patients aged ≥18 years admittedto 1 of the 3 participating medical units between 1 January2009 and 31 December 2011 (ie, 36 months) with laboratory-confirmed RSV infections were studied (N = 607). In HongKong, peak RSV activities occur in spring or summer, or both,with yearly variations [12, 13]. No case was excluded from theanalysis. All 3 participating hospitals (A, B, and C) are acutecare, general public hospitals operating under the Hospital Au-thority of Hong Kong. The 3 hospitals serve an urban popula-tion of >1.5 million accounting for >20% of the population inHong Kong [14, 15]. The Hospital Authority is the main pro-vider of acute medical care in Hong Kong. Ethical approval forthe study was obtained from the institutional review boards ofthe Hospital Authority of Hong Kong and the Chinese Univer-sity of Hong Kong.
During the study period, respiratory viral infections includ-ing RSV and influenza in the hospitalized adults were prospec-tively diagnosed according to a standard protocol as part ofpatients’ routine care, as previously described [14–16]. In brief,patients presenting with symptoms of acute respiratory infec-tions were admitted if they developed potentially seriousmedical conditions and/or if their exacerbation of chronic ill-nesses or their severe symptoms were considered to be impossi-ble to be managed at home [14, 16]. Nasopharyngeal aspirates(NPAs) were collected at presentation from all such patients,regardless of perceived etiology and disease severity, to test forRSV and influenza antigens using an immunofluorescenceassay (see next section) [4, 12, 14–16]. In a minority of caseswhere NPA cannot be performed, nasopharyngeal flocked
swabs were collected for testing. Test results were generallymade available to physicians within a few hours to assist patientmanagement and infection control precautions. In addition,chest radiography was performed at admission for all patients,and sputum samples were routinely collected for bacterialculture. Blood cultures were also performed when there weresigns of sepsis [14–16].
Data Collection and Definitions of VariablesAll patients with laboratory-confirmed RSV infections admit-ted during the study period were identified from a computer-ized laboratory record system. Patients’ electronic (hospitalClinical Management System [CMS]) and written records werereviewed, and the clinical and laboratory information was sys-tematically recorded using a standardized research tool [14–16]. Clinical data collected included demographics, comorbidi-ties, illness onset time, presenting symptoms, cardiorespiratorycomplications, requirement for supplemental oxygen therapyand/or ventilatory support, antibiotic use, use of systemic corti-costeroids (eg, intravenous hydrocortisone, oral prednisolone),hospitalization duration, and all-cause death. Laboratory dataincluded routine blood test results and bacterial pathogens cul-tured from respiratory and/or blood samples at presentationand during hospitalization [14]. Pneumonia was defined asphysician-diagnosed pneumonia based on symptoms and signsof acute lower respiratory tract infection together with new pul-monary infiltrates on a patient’s chest radiographs [5, 14–17].Acute respiratory failure requiring ventilatory support wasdefined as persistent respiratory failure despite supplementaloxygen therapy (eg, SaO2 <92%) which necessitated the use ofnoninvasive positive pressure ventilation (NIPPV) or invasivemechanical ventilation for support [14, 15]. The main outcomemeasure in this analysis was all-cause death; the secondaryoutcome measures were (1) development of acute respiratoryfailure requiring ventilatory support and (2) total duration ofhospitalization among survivors [14, 15]. In addition, we com-pared the RSV patients with a cohort of patients admitted tothese hospitals for seasonal influenza in 2009–2011 [14, 15].The same research tools and definitions were used for bothstudy cohorts. Patients hospitalized with pandemic 2009 H1N1infections were not included for comparison as they were sig-nificantly younger and shown to have a different clinical coursecompared to seasonal influenza, as described elsewhere [15].
Virological InvestigationsAll NPAs collected were subjected to viral antigen detection fora panel of respiratory viruses including RSV, influenza A and B,and parainfluenza 1, 2, and 3 viruses using an immunofluores-cence assay (IFA) as previously described [14–16]. NPA containedmore abundant epithelial cells for immunofluorescence staining;false-positive results are rare (see Discussion) [3, 4, 12, 18–20].
2 • CID • Lee et al
by Norm
an Sharples on August 20, 2013
http://cid.oxfordjournals.org/D
ownloaded from

In brief, NPA samples were washed with phosphate-bufferedsaline. The cells were fixed on the wells of a glass slide withacetone and stained with respiratory virus–specific antibodies(LIGHT DIAGNOSTICS Respiratory Syncytial Virus FITCReagent, Chemicon/Millipore). Specific fluorescent signalswere cross-checked by 2 experienced technicians and reviewedby clinical virologists. A repeat sample would be requested ifnecessary. Virus isolation was performed for all influenza casesusing methods previously described (but not routinely for RSVbecause of its low sensitivity and logistic demands) [4, 16, 12].
Radiographic AssessmentTo further characterize RSV-related lower respiratory tractcomplications and their impacts in adults, additional, detailedradiographic review was performed for all RSV cases admittedto the largest study site (hospital A, n = 286; 47% of the entirecohort). The chest radiographs at admission were reviewed by 2independent, experienced radiologists using dedicated PictureArchiving and Communication System workstations in retro-spect; images were interpreted in consensus for the few discrep-ant cases [21–23]. The reviewers were blinded to all clinicalinformation of patients and their outcomes. Previous chest ra-diographs were used for comparison whenever available (86%).The chest radiographs were assessed for the presence of anyactive lung parenchymal changes (including consolidation,ground glass opacity, and reticulonodular shadows) that werecompatible with the diagnosis of pneumonia, and their patternsand extent [22, 23]. Radiologists’ reviews were considered final.
Statistical AnalysisThe Student t, Mann-Whitney U, and χ2 tests with continuitycorrection were used for univariate comparisons whenever ap-propriate. Variables with P values < .1 in the univariate analyseswere entered into multivariate Cox proportional hazardsmodels (backward, stepwise regression) to determine indepen-dent factors associated with death that occurred within 30 daysand 60 days from time of hospitalization [6, 8, 14, 15]. Variablesincluding demographics, comorbidities, cardiorespiratory com-plications, ventilation requirement, bacterial superinfection,and corticosteroid use were examined. Adjusted hazard ratios(AHRs) and 95% confidence intervals (CIs) were calculatedfor each explanatory variable. An AHR >1 indicated a higherchance of death. A Kaplan-Meier curve was constructed toshow survival of patients with or without pneumonia develop-ment, and compared using the log-rank test. Cox regressionmodels were also used to determine independent factors associ-ated with time to hospital discharge. Multivariate logistic re-gression was used to analyze factors associated with pneumoniaand acute respiratory failure requiring ventilatory support; ad-justed odds ratios (AORs) and 95% CIs were reported for ex-planatory variables [14–16]. Analyses of clinical outcomes were
performed for the whole cohort, and repeated in the subgroupwith additional radiographic reviews performed. We also com-pared the manifestations and outcomes of RSV patients to aconcurrent seasonal influenza cohort using similar analyticmethods [14, 15]. All probabilities were 2-tailed, and a P valueof <.05 was considered to indicate statistical significance. Wealso calculated a conservative, Bonferroni-adjusted P valuethreshold (P < .002) for the multiple comparisons in Table 1 forreference. Statistical analysis was performed using PASW Sta-tistics software, version 18.0.
RESULTS
Patient Descriptions and Clinical ManifestationsDuring the 3-year study period, a total of 607 RSV cases werediagnosed among the hospitalized adults: 2009, n = 123; 2010,n = 237; 2011, n = 247. The median RSV-positive rate amongsubmitted respiratory samples during the seasonal peaks of theyears was: 5.8% (interquartile range [IQR], 4.8%–6.5%), 6.6%(IQR, 5.8%–9.8%), and 9.1% (IQR, 5.7%–13.7%), respectively(Figure 1). Patients’ baseline characteristics and clinical mani-festations are described in Table 1. The mean and median ageswere 75 (SD, 16) years and 80 (IQR, 68–86) years, respectively;87.3% had 1 or more coexisting medical conditions (eg, chroniclung diseases, 35.6%, major systemic comorbidities, 74.0%; im-munocompromised, 13.7%; see Table 1). The mean andmedian time of admission from symptom onset was 2.6 (SD,2.2) days and 2 (IQR, 1–3) days, respectively. Fever (75.0%),cough (87.5%), sputum production (81.2%), and wheezybreathing and dyspnea (68.9%) were the commonest presentingsymptoms. One or more complications were documented in80.4%. Lower respiratory tract complications were diagnosed in71.9%, including pneumonia (42.3%), acute bronchitis (21.9%),and exacerbation of chronic obstructive pulmonary disease(COPD)/asthma (with or without pneumonia, 27.3%). Bacterialsuperinfection was evidenced in 12.5% at presentation; Strepto-coccus pneumoniae, Haemophilus influenzae, and Pseudomonasaeruginosa were the commonest isolates (Table 1). Cardiovascu-lar complications (eg, exacerbation of heart failure, acute coro-nary events) were diagnosed in 14.3% of patients.
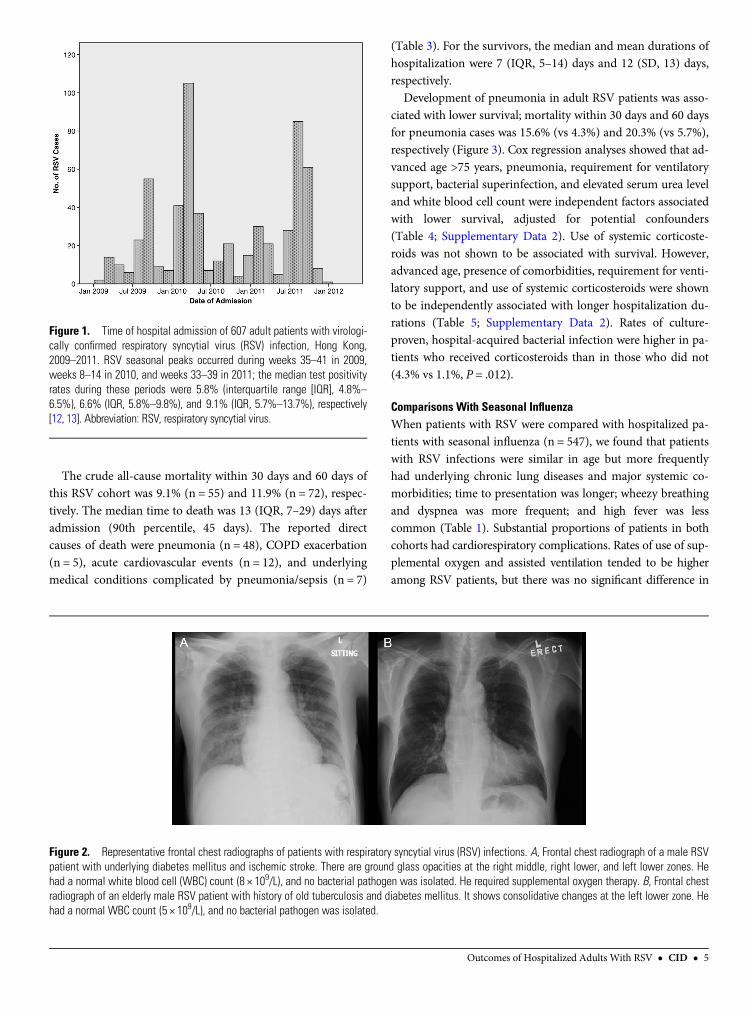
Among the subset of patients with additional radiographicreview performed, 141 of 286 (49.3%) had shown active pneu-monic changes; consolidations (23.8%) and ground-glass opaci-ties (19.9%) were the commonest findings. Most (81.8%) changeswere unilateral. Examples of patients’ chest radiographs at pre-sentation are shown in Figure 2. Symptoms associated with ra-diographic pneumonia included fever (82.0% pneumonia vs72.5% without pneumonia, P = .058) and wheezy breathingand dyspnea (79.9% vs 66.2%, P = .010). Runny nose (23.7% vs35.2%, P = .035) and sore throat (9.4% vs 16.2%, P = .086) wereless common. Multivariate analysis showed that presence of
Outcomes of Hospitalized Adults With RSV • CID • 3
by Norm
an Sharples on August 20, 2013
http://cid.oxfordjournals.org/D
ownloaded from

major systemic comorbidities (AOR, 1.85; 95% CI, 1.05–3.26)and elevated white blood cell counts (AOR, 1.07; 95% CI, 1.01–1.13, per unit increase) were independently associated with ra-diographic pneumonia, adjusted for demographic and bacterio-logical variables (Supplementary Data 1).
Patient Management and OutcomesSystemic corticosteroids were given to 38.9% of patients to treatacute airway diseases (eg, COPD/asthma exacerbations), and
antibiotics were used in 94.7% of cases. Two-thirds (67.9%) ofpatients were given supplemental oxygen therapy; 11.1% devel-oped persistent respiratory failure and required ventilatorysupport (NIPPV, 9.1%, invasive ventilation, 2.0%). Underly-ing chronic lung diseases, pneumonia (particularly the pres-ence of ground-glass opacities), and elevated serum urea andalanine aminotransferase levels were shown to be independentfactors associated with requirement of ventilatory support(Table 2).
Table 1. Baseline Characteristics, Presenting Symptoms, Complications, and Outcomes of 607 Adults Hospitalized With Respiratory Syn-cytial Virus Infection, 2009–2011
Variable RSV (N = 607) Influenza (N = 547) P Value
Age, y, mean (SD) 75.1 (16.4) 74.7 (16.6) .650
Male sex 48.6 49.5 .749Resident of long-term care facility 32.9 30.5 .378
Comorbidity, major systemic (except chronic lung diseases)a 74.0 65.8 .003
Chronic lung diseasesa 35.6 24.1 <.001Symptom onset to admission, d, mean (SD) 2.6 (2.2) 2.0 (1.7) <.001
Fever >37.5°C 75.0 94.2 <.001
Cough 87.5 85.7 .513Sputum production 81.2 72.5 .010
Wheezy breathing and dyspnea 68.9 53.2 <.001
Sore throat 11.8 14.3 .364Runny nose 25.6 30.2 .214
Pneumonia 42.3 36.7 .006
Lower respiratory complicationsb 71.9 55.6 <.001Cardiovascular complicationsb 14.3 13.3 .653
Complications, anyb 80.4 72.8 .002
Bacterial infection, overallc 14.8 14.3 .790Bacterial infection, at presentationc 12.5 9.1 .066
Supplemental oxygen therapy 67.9 59.0 .002
Ventilation, noninvasive or invasive 11.1 6.2 .00330-day mortality 9.1 8.0 .538
60-day mortality 11.9 8.8 .086
Time to death, d, median (IQR) 13 (7–29) 7 (3–13) .001Extended care in subacute hospitals 25.2 19.7 .027
Duration of hospitalization for survivors, d, median (IQR) 7 (5–14) 6 (5–11) .238
Data are percentages unless otherwise indicated. Patients hospitalized with seasonal influenza during the same period are used for comparison.
RSV cohort: hospital A, 47.4%; B, 32.5%; C, 20.1%; never-smoker, 43.7%; (non-Chinese, 1; pregnant female, 1). Specimen for diagnosis: nasopharyngeal aspirate,90.6%; nasopharyngeal flocked swabs, 9.1%; bronchial/tracheal aspirates, 0.3%. Seasonal influenza cohort: H3N2, 79.2%; H1N1, 0.7%; B, 20.1%; >95%immunofluorescence assay positive (nearly all confirmed with culture; remainder diagnosed by culture/polymerase chain reaction); 91.2% received oseltamivirtreatment [14–16]. Two patients had RSV and influenza A coinfection. A Bonferroni-corrected P value significance threshold (P < .002) is calculated for reference.
Abbreviations: IQR, interquartile range; RSV, respiratory syncytial virus; SD, standard deviation.a Major systemic comorbidity: congestive heart failure; cerebrovascular, neoplastic, and chronic liver or renal diseases; other chronic cardiovascular and neurologicconditions (except hypertension); diabetes mellitus; autoimmune disorders; immunocompromised (immunocompromising conditions and/or use ofimmunosuppressants). Chronic lung diseases: chronic obstructive pulmonary disease, asthma, bronchiectasis, and pulmonary fibrosis [14–16].b Lower respiratory complications: pneumonia, acute bronchitis, acute exacerbation of chronic obstructive pulmonary disease/asthma. Cardiovascular complications:exacerbation of heart failure, atrial fibrillation, acute coronary events, acute cerebrovascular events. Other complications: drowsiness, delirium, seizure (6.1%); syncope,fall, renal impairment, dehydration, metabolic disturbances (15.9%). Patients may have >1 complication [14–16].c Bacterial superinfection: evidenced by positive culture of a bacterial pathogen from respiratory (sputum, bronchial/tracheal aspirates) and/or blood samples; infectionswith onset >2 days after admission were considered hospital-acquired [14, 15]. At presentation: Streptococcus pneumoniae, 15; Haemophilus influenzae, 14;Staphylococcus aureus, 5; Moraxella catarrhalis, 2; Pseudomonas aeruginosa, 20; Klebsiella spp, 10; other gram-negative bacteria, 9; other gram-positive cocci,1. Hospital-acquired: P. aeruginosa, 5; other gram-negative bacteria, 9. Most (94.7%) patients received antibiotic treatment.
4 • CID • Lee et al
by Norm
an Sharples on August 20, 2013
http://cid.oxfordjournals.org/D
ownloaded from
The crude all-cause mortality within 30 days and 60 days ofthis RSV cohort was 9.1% (n = 55) and 11.9% (n = 72), respec-tively. The median time to death was 13 (IQR, 7–29) days afteradmission (90th percentile, 45 days). The reported directcauses of death were pneumonia (n = 48), COPD exacerbation(n = 5), acute cardiovascular events (n = 12), and underlyingmedical conditions complicated by pneumonia/sepsis (n = 7)
(Table 3). For the survivors, the median and mean durations ofhospitalization were 7 (IQR, 5–14) days and 12 (SD, 13) days,respectively.
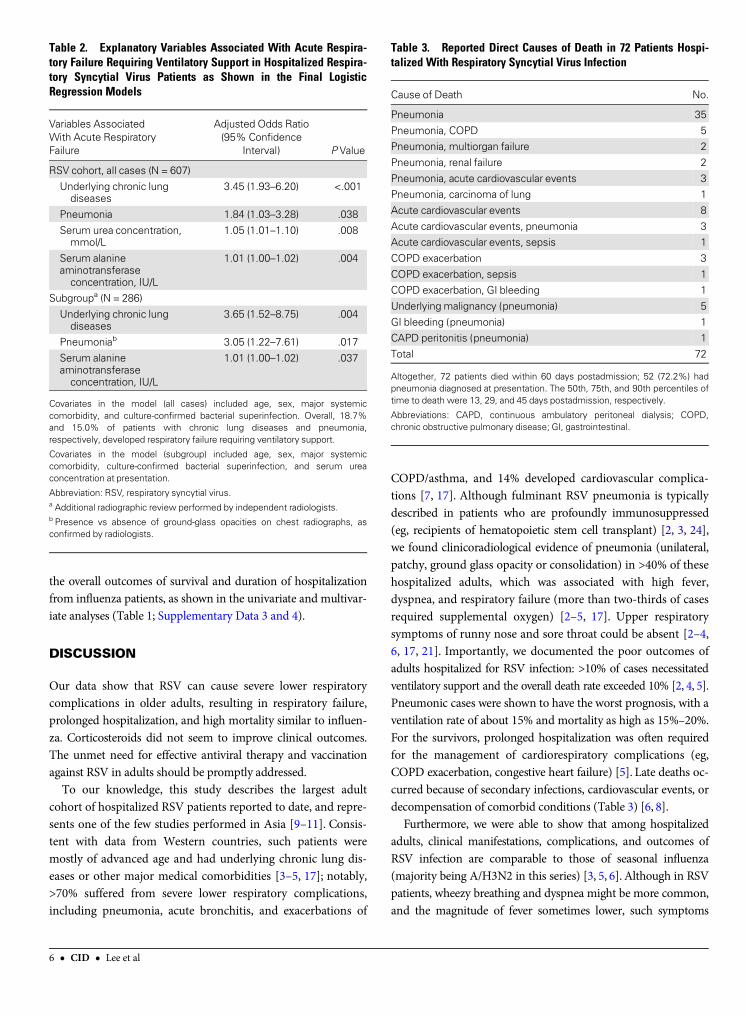
Development of pneumonia in adult RSV patients was asso-ciated with lower survival; mortality within 30 days and 60 daysfor pneumonia cases was 15.6% (vs 4.3%) and 20.3% (vs 5.7%),respectively (Figure 3). Cox regression analyses showed that ad-vanced age >75 years, pneumonia, requirement for ventilatorysupport, bacterial superinfection, and elevated serum urea leveland white blood cell count were independent factors associatedwith lower survival, adjusted for potential confounders(Table 4; Supplementary Data 2). Use of systemic corticoste-roids was not shown to be associated with survival. However,advanced age, presence of comorbidities, requirement for venti-latory support, and use of systemic corticosteroids were shownto be independently associated with longer hospitalization du-rations (Table 5; Supplementary Data 2). Rates of culture-proven, hospital-acquired bacterial infection were higher in pa-tients who received corticosteroids than in those who did not(4.3% vs 1.1%, P = .012).
Comparisons With Seasonal InfluenzaWhen patients with RSV were compared with hospitalized pa-tients with seasonal influenza (n = 547), we found that patientswith RSV infections were similar in age but more frequentlyhad underlying chronic lung diseases and major systemic co-morbidities; time to presentation was longer; wheezy breathingand dyspnea was more frequent; and high fever was lesscommon (Table 1). Substantial proportions of patients in bothcohorts had cardiorespiratory complications. Rates of use of sup-plemental oxygen and assisted ventilation tended to be higheramong RSV patients, but there was no significant difference in
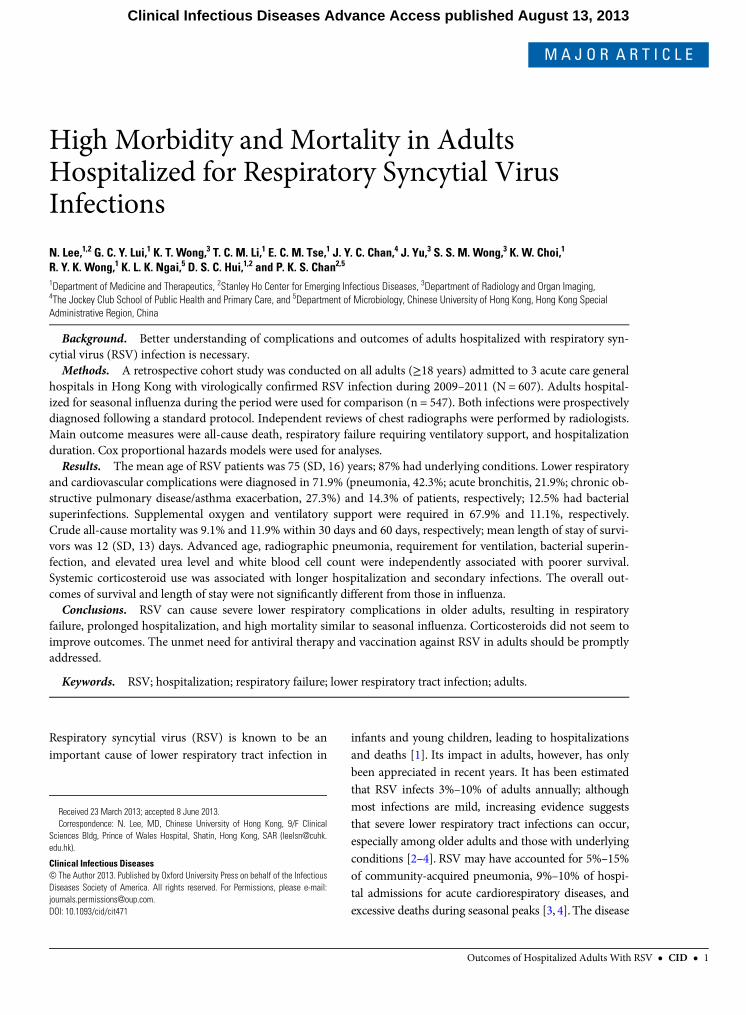
Figure 1. Time of hospital admission of 607 adult patients with virologi-cally confirmed respiratory syncytial virus (RSV) infection, Hong Kong,2009–2011. RSV seasonal peaks occurred during weeks 35–41 in 2009,weeks 8–14 in 2010, and weeks 33–39 in 2011; the median test positivityrates during these periods were 5.8% (interquartile range [IQR], 4.8%–
6.5%), 6.6% (IQR, 5.8%–9.8%), and 9.1% (IQR, 5.7%–13.7%), respectively[12, 13]. Abbreviation: RSV, respiratory syncytial virus.
Figure 2. Representative frontal chest radiographs of patients with respiratory syncytial virus (RSV) infections. A, Frontal chest radiograph of a male RSVpatient with underlying diabetes mellitus and ischemic stroke. There are ground glass opacities at the right middle, right lower, and left lower zones. Hehad a normal white blood cell (WBC) count (8 × 109/L), and no bacterial pathogen was isolated. He required supplemental oxygen therapy. B, Frontal chestradiograph of an elderly male RSV patient with history of old tuberculosis and diabetes mellitus. It shows consolidative changes at the left lower zone. Hehad a normal WBC count (5 × 109/L), and no bacterial pathogen was isolated.
Outcomes of Hospitalized Adults With RSV • CID • 5
by Norm
an Sharples on August 20, 2013
http://cid.oxfordjournals.org/D
ownloaded from
the overall outcomes of survival and duration of hospitalizationfrom influenza patients, as shown in the univariate and multivar-iate analyses (Table 1; Supplementary Data 3 and 4).
DISCUSSION
Our data show that RSV can cause severe lower respiratorycomplications in older adults, resulting in respiratory failure,prolonged hospitalization, and high mortality similar to influen-za. Corticosteroids did not seem to improve clinical outcomes.The unmet need for effective antiviral therapy and vaccinationagainst RSV in adults should be promptly addressed.
To our knowledge, this study describes the largest adultcohort of hospitalized RSV patients reported to date, and repre-sents one of the few studies performed in Asia [9–11]. Consis-tent with data from Western countries, such patients weremostly of advanced age and had underlying chronic lung dis-eases or other major medical comorbidities [3–5, 17]; notably,>70% suffered from severe lower respiratory complications,including pneumonia, acute bronchitis, and exacerbations of
COPD/asthma, and 14% developed cardiovascular complica-tions [7, 17]. Although fulminant RSV pneumonia is typicallydescribed in patients who are profoundly immunosuppressed(eg, recipients of hematopoietic stem cell transplant) [2, 3, 24],we found clinicoradiological evidence of pneumonia (unilateral,patchy, ground glass opacity or consolidation) in >40% of thesehospitalized adults, which was associated with high fever,dyspnea, and respiratory failure (more than two-thirds of casesrequired supplemental oxygen) [2–5, 17]. Upper respiratorysymptoms of runny nose and sore throat could be absent [2–4,6, 17, 21]. Importantly, we documented the poor outcomes ofadults hospitalized for RSV infection: >10% of cases necessitatedventilatory support and the overall death rate exceeded 10% [2, 4, 5].Pneumonic cases were shown to have the worst prognosis, with aventilation rate of about 15% and mortality as high as 15%–20%.For the survivors, prolonged hospitalization was often requiredfor the management of cardiorespiratory complications (eg,COPD exacerbation, congestive heart failure) [5]. Late deaths oc-curred because of secondary infections, cardiovascular events, ordecompensation of comorbid conditions (Table 3) [6, 8].
Furthermore, we were able to show that among hospitalizedadults, clinical manifestations, complications, and outcomes ofRSV infection are comparable to those of seasonal influenza(majority being A/H3N2 in this series) [3, 5, 6]. Although in RSVpatients, wheezy breathing and dyspnea might be more common,and the magnitude of fever sometimes lower, such symptoms
Table 2. Explanatory Variables Associated With Acute Respira-tory Failure Requiring Ventilatory Support in Hospitalized Respira-tory Syncytial Virus Patients as Shown in the Final LogisticRegression Models
Variables AssociatedWith Acute RespiratoryFailure
Adjusted Odds Ratio(95% Confidence
Interval) P Value
RSV cohort, all cases (N = 607)
Underlying chronic lungdiseases
3.45 (1.93–6.20) <.001
Pneumonia 1.84 (1.03–3.28) .038
Serum urea concentration,mmol/L
1.05 (1.01–1.10) .008
Serum alanineaminotransferaseconcentration, IU/L
1.01 (1.00–1.02) .004
Subgroupa (N = 286)
Underlying chronic lungdiseases
3.65 (1.52–8.75) .004
Pneumoniab 3.05 (1.22–7.61) .017
Serum alanineaminotransferaseconcentration, IU/L
1.01 (1.00–1.02) .037
Covariates in the model (all cases) included age, sex, major systemiccomorbidity, and culture-confirmed bacterial superinfection. Overall, 18.7%and 15.0% of patients with chronic lung diseases and pneumonia,respectively, developed respiratory failure requiring ventilatory support.
Covariates in the model (subgroup) included age, sex, major systemiccomorbidity, culture-confirmed bacterial superinfection, and serum ureaconcentration at presentation.
Abbreviation: RSV, respiratory syncytial virus.a Additional radiographic review performed by independent radiologists.b Presence vs absence of ground-glass opacities on chest radiographs, asconfirmed by radiologists.
Table 3. Reported Direct Causes of Death in 72 Patients Hospi-talized With Respiratory Syncytial Virus Infection
Cause of Death No.
Pneumonia 35
Pneumonia, COPD 5Pneumonia, multiorgan failure 2
Pneumonia, renal failure 2
Pneumonia, acute cardiovascular events 3Pneumonia, carcinoma of lung 1
Acute cardiovascular events 8
Acute cardiovascular events, pneumonia 3Acute cardiovascular events, sepsis 1
COPD exacerbation 3
COPD exacerbation, sepsis 1COPD exacerbation, GI bleeding 1
Underlying malignancy (pneumonia) 5
GI bleeding (pneumonia) 1CAPD peritonitis (pneumonia) 1
Total 72
Altogether, 72 patients died within 60 days postadmission; 52 (72.2%) hadpneumonia diagnosed at presentation. The 50th, 75th, and 90th percentiles oftime to death were 13, 29, and 45 days postadmission, respectively.
Abbreviations: CAPD, continuous ambulatory peritoneal dialysis; COPD,chronic obstructive pulmonary disease; GI, gastrointestinal.
6 • CID • Lee et al
by Norm
an Sharples on August 20, 2013
http://cid.oxfordjournals.org/D
ownloaded from
could not reliably differentiate it from influenza [3, 4, 17]. Highrates of respiratory (56%–72%) and cardiovascular (13%–14%)complications occurred in both infections, with substantial pro-portions of patients requiring supplemental oxygen therapy(59%–68%) and ventilatory support (6%–11%) [5, 6]. Respiratoryfailure appeared to be more common among RSV patients, butthere was a higher prevalence of chronic lung diseases amongthem. The overall outcomes of survival and hospitalization dura-tion were not shown to be significantly different between RSVand influenza patients after adjustment for confounders [4–9].Unlike influenza, antiviral treatment or vaccine is currently notavailable for RSV. Ribavirin and immunoglobulins have beenused to treat (or prevent) severe RSV pneumonia in immuno-compromised patients; however, controlled data are lacking,and whether these can be applied to the older adults are uncer-tain [3, 4, 24–26]. Our findings thus highlight the need for ther-apeutic and preventive interventions against RSV in adults.Recent progress on their development and the obstacles en-countered has been reviewed elsewhere [3, 4, 24].
In addition, we examined the roles of bacterial infections andsystemic corticosteroids in adult RSV infections. We found evi-dence of bacterial superinfection in about 15% of patients duringtheir course of illness, which was a significant contributory factorto mortality (similar in influenza diseases) [4, 5, 9, 15, 17].
As such, any bacterial infection should be promptly detectedand treated according to local resistance profiles. BesidesS. pneumoniae and H. influenzae, P. aeruginosa and othergram-negative bacilli may need to be considered in patientswith underlying chronic lung diseases [4, 9, 15]. Corticosteroids
Table 4. Explanatory Variables Associated With Death in Hospi-talized Respiratory Syncytial Virus Patients as Shown in the FinalCox Proportional Hazards Models (N = 607)
Variables AssociatedWith Death
Adjusted HazardRatio (95% CI) P Value
Events censored within 30 days postadmissionAdvanced age (>75 y) 2.85 (1.43–5.68) .003
Pneumonia 2.80 (1.53–5.14) .001
Requirement of ventilatory support 6.21 (3.39–11.35) <.001Bacterial superinfection 2.02 (1.11–3.66) .021
Serum urea concentration, mmol/L 1.04 (1.00–1.08) .035
Total WBC count, ×109/L 1.05 (1.00–1.10) .059Events censored within 60 days postadmission
Advanced age (>75 y) 2.10 (1.18–3.73) .011
Pneumonia 2.99 (1.75–5.11) <.001Requirement of ventilatory support 4.65 (2.71–7.98) <.001
Cardiovascular complications 1.71 (.97–3.02) .063
Bacterial superinfection 2.04 (1.20–3.48) .009Serum urea concentration, mmol/L 1.05 (1.01–1.08) .004
Total WBC count, ×109/L 1.06 (1.01–1.10) .009
Adjusted hazard ratio >1 indicated increased risk of death. Covariates in themodels included sex, major systemic comorbidities, chronic lung diseaseexacerbations, hospital site, and use of systemic corticosteroids. Subgroupanalysis on cases with additional radiographic reviews showed similar results(Supplementary Data 2).
Abbreviations: CI, confidence interval; WBC, white blood cell.
Table 5. Explanatory Variables Associated With Duration of Hos-pitalization Among Survivors (n = 535) as Shown in the Final CoxProportional Hazards Model
Variables AssociatedWithDuration of Hospitalization
Adjusted Hazard Ratio(95% Confidence Interval) P Value
Advanced age (>75 y) 0.74 (.62–.89) .001
Comorbidity, major systemic 0.77 (.64–.94) .010
Requirement of ventilatorysupport
0.39 (.28–.54) <.001
Use of systemiccorticosteroids
0.76 (.63–.91) .002
An adjusted hazard ratio <1 indicated a lower chance of discharge. Covariatesin the model included sex, chronic lung disease exacerbations, presence ofpneumonia, bacterial superinfection, and hospital site. Subgroup analysison cases with additional radiograph reviews showed similar results(Supplementary Data 2). The median duration of hospitalization amongpatients who received systemic corticosteroids was 8 (interquartile range[IQR], 5–18) days, and 6 (IQR, 5–12) days in patients who had not receivedcorticosteroids; 73% of patients who received systemic corticosteroids alsoreceived inhaled corticosteroids [14–16].
Figure 3. Kaplan-Meier survival curves of 607 adults hospitalized for re-spiratory syncytial virus (RSV) infection. Patients who developed pneumo-nia were shown to have lower survival. Among RSV patients who hadpneumonia, the crude 30-day and 60-day mortality was 15.6% and 20.3%,respectively (4.3% and 5.7%, respectively, in those without pneumonia).Subgroup analysis on cases with additional radiograph reviews showedsimilar results (data not shown).
Outcomes of Hospitalized Adults With RSV • CID • 7
by Norm
an Sharples on August 20, 2013
http://cid.oxfordjournals.org/D
ownloaded from

are commonly used to treat wheezy attacks and exacerbationsof COPD/asthma in adults, including those triggered by viralinfections [16, 27]. In this large RSV cohort, we did not observeany benefit on clinical outcomes with systemic corticosteroidtreatment in the multivariate analyses, adjusted for disease se-verity. Instead, increased bacterial infections and longer hospi-talization duration were found. Limiting our analysis to apatient subset presenting with wheezy breathing and dyspneashowed similar results (data not shown). We cannot eliminateindication bias, but these findings are supported by randomizedcontrolled trials in young children, which revealed lack of clini-cal benefit and inconsistent control of inflammatory cytokineresponses with corticosteroids [28–30]. A recent adult study re-ported similar findings; it also showed that humoral immunityagainst RSV was diminished, although virus control appearedunaffected [31]. Emerging evidence suggests worse outcomeswith corticosteroid use in influenza pneumonia [16, 32]. Takentogether, it is suggested that the decision to treat RSV patientswith corticosteroids should be weighed against the potentialrisks, and be limited to a short course if used [4, 25, 31].Further study is indicated.
The strengths of our study include a large sample size, multi-center design, and virological confirmation of cases. Identicalclinical settings and research methods had allowed moreprecise comparisons between the 2 viral infections. Chest radio-graphs were independently reviewed; the detailed findings willbe reported separately [22]. Our study is limited by its retro-spective nature; therefore, variables least prone to bias werechosen as outcome measures, and confounders adjusted care-fully in multivariate analyses. The use of IFA instead of PCRfor the diagnosis of RSV in our service settings could also be alimitation. IFA is highly specific (95%–99%), and moderatelysensitive (80%–94%, higher with NPA) in children; the sensi-tivity in adults is generally lower because of lower virus shed-ding levels [3, 4, 12, 18–20, 33]. Although increased testsensitivity can be expected in the older, hospitalized adults withsevere RSV disease because of their higher viral titers andlonger virus shedding durations [34–36], it is possible thatsome cases, especially the milder ones, had remained undetect-ed. Using PCR (without or without paired serology) for diagno-sis should reveal a greater disease burden [4, 34]. We haveplanned to perform PCR, neutralizing antibodies, and virussubtyping in our patients in the near future (evidence suggeststhat both serotypes A and B circulate in Asia) [10].
In conclusion, adults hospitalized for RSV infection havehigh morbidity and mortality, comparable to outcomes in in-fluenza patients. Studies on disease pathogenesis (eg, viral dy-namics, immune response, viral–bacterial interactions) [3, 4,34–36]; strategies to improve case finding, diagnosis, and infec-tion control in the hospital setting (eg, PCR, serology, aerosoltransmission) [3, 4, 17, 34, 35, 37]; and development of antiviral
therapies and immunization of high-risk adults (eg, smallinterfering RNA, fusion protein inhibitor, newer generationimmunoglobulins, subunit vaccines) [3, 4, 24, 38, 39] areurgently needed.
Supplementary Data
Supplementary materials are available at Clinical Infectious Diseases online(http://cid.oxfordjournals.org/). Supplementary materials consist of dataprovided by the author that are published to benefit the reader. The postedmaterials are not copyedited. The contents of all supplementary data are thesole responsibility of the authors. Questions or messages regarding errorsshould be addressed to the author.
Note
Potential conflicts of interest. All authors: No reported conflicts.All authors have submitted the ICMJE Form for Disclosure of Potential
Conflicts of Interest. Conflicts that the editors consider relevant to thecontent of the manuscript have been disclosed.
References
1. Nair H, Nokes DJ, Gessner BD, et al. Global burden of acute lower re-spiratory infections due to respiratory syncytial virus in young children:a systematic review and meta-analysis. Lancet 2010; 375:1545–55.
2. Cesario TC. Viruses associated with pneumonia in adults. Clin InfectDis 2012; 55:107–13.
3. Walsh EE. Respiratory syncytial virus infection in adults. Semin RespirCrit Care Med 2011; 32:423–32.
4. Murata Y, Falsey AR. Respiratory syncytial virus infection in adults.Antivir Ther 2007; 12(4 Pt B):659–70.
5. Falsey AR, Hennessey PA, Formica MA, Cox C, Walsh EE. Respiratorysyncytial virus infection in elderly and high-risk adults. N Engl J Med2005; 352:1749–59.
6. Widmer K, Zhu Y, Williams JV, Griffin MR, Edwards KM, Talbot HK.Rates of hospitalizations for respiratory syncytial virus, human meta-pneumovirus, and influenza virus in older adults. J Infect Dis 2012;206:56–62.
7. Jansen AG, Sanders EA, Hoes AW, van Loon AM, Hak E. Influenza-and respiratory syncytial virus-associated mortality and hospitalisa-tions. Eur Respir J 2007; 30:1158–66.
8. van Asten L, van den Wijngaard C, van Pelt W, et al. Mortality attribut-able to 9 common infections: significant effect of influenza A, respirato-ry syncytial virus, influenza B, norovirus, and parainfluenza in elderlypersons. J Infect Dis 2012; 206:628–39.
9. Choi SH, Hong SB, Ko GB, et al. Viral infection in patients with severepneumonia requiring intensive care unit admission. Am J Respir CritCare Med 2012; 186:325–32.
10. Xiang Z, Gonzalez R, Ren L, et al. Prevalence and clinical characteristicsof human respiratory syncytial virus in Chinese adults with acute respi-ratory tract infection. J Med Virol 2013; 85:348–53.
11. Olsen SJ, Thamthitiwat S, Chantra S, et al. Incidence of respiratorypathogen in persons hospitalized with pneumonia in two provinces inThailand. Epidemiol Infect 2010; 138:1811–22.
12. Chiu SS, Chan KH, Chen H, et al. Virologically confirmed population-based burden of hospitalization caused by respiratory syncytial virus,adenovirus, and parainfluenza viruses in children in Hong Kong.Pediatr Infect Dis J 2010; 29:1088–92.
13. Center for Health Protection, Hong Kong SAR. Seasonal increase inRSV activity. Communicable diseases watch. Available at: http://www.chp.gov.hk/files/pdf/cdw_v9_6.pdf Accessed 30 January 2013.
14. Lee N, Choi KW, Chan PK, et al. Outcomes of adults hospitalised withsevere influenza. Thorax 2010; 65:510–5.
8 • CID • Lee et al
by Norm
an Sharples on August 20, 2013
http://cid.oxfordjournals.org/D
ownloaded from
15. Lee N, Chan PK, Lui GC, et al. Complications and outcomes of pan-demic 2009 influenza A (H1N1) virus infection in hospitalized adults:how do they differ from those in seasonal influenza? J Infect Dis 2011;203:1739–47.
16. Lee N, Chan PK, Hui DS, et al. Viral loads and duration of viral shed-ding in adult patients hospitalized with influenza. J Infect Dis 2009;200:492–500.
17. Walsh EE, Peterson DR, Falsey AR. Is clinical recognition of respiratorysyncytial virus infection in hospitalized elderly and high-risk adultspossible? J Infect Dis 2007; 195:1046–51.
18. de-Paris F, Beck C, Machado AB, et al. Optimization of one-step duplexreal-time RT-PCR for detection of influenza and respiratory syncytialvirus in nasopharyngeal aspirates. J Virol Methods 2012; 186:189–92.
19. Chan KH, Peiris JS, LimW, Nicholls JM, Chiu SS. Comparison of naso-pharyngeal flocked swabs and aspirates for rapid diagnosis of respirato-ry viruses in children. J Clin Virol 2008; 42:65–9.
20. Ohm-Smith MJ, Nassos PS, Haller BL. Evaluation of the Binax NOW,BD Directigen, and BD Directigen EZ assays for detection of respirato-ry syncytial virus. J Clin Microbiol 2004; 42:2996–9.
21. Lee N, Chan PK, Wong CK, et al. Slow viral clearance and hyperacti-vated inflammatory responses in adults hospitalized for severe pandem-ic 2009 influenza A(H1N1) virus pneumonia. Antiviral Therapy 2011;16:237–47.
22. Wong S, Yu J, Lee N, Lui G, Wong KT, Ahuja A. Initial radiographicfeatures as outcome predictor of adult RSV respiratory tract infection.In: European Congress of Radiology, Vienna, Austria, March 2013(abstract).
23. Syha R, Beck R, Hetzel J, et al. Human metapneumovirus (HMPV) as-sociated pulmonary infections in immunocompromised adults—initialCT findings, disease course and comparison to respiratory-syncytial-virus(RSV) induced pulmonary infections. Eur J Radiol 2012; 81:4173–8.
24. Shah JN, Chemaly RF. Management of RSV infections in adultrecipients of hematopoietic stem cell transplantation. Blood 2011; 117:2755–63.
25. Park SY, Baek S, Lee SO, et al. Efficacy of oral ribavirin in hemato-logic disease patients with paramyxovirus infection: analytic strategyusing propensity scores. Antimicrob Agents Chemother 2013; 57:983–9.
26. van Woensel JB, Vyas H; STAR Trial Group. Dexamethasone in chil-dren mechanically ventilated for lower respiratory tract infectioncaused by respiratory syncytial virus: a randomized controlled trial.Crit Care Med 2011; 39:1779–83.
27. Rabe KF, Wedzicha JA. Controversies in treatment of chronic obstruc-tive pulmonary disease. Lancet 2011; 378:1038–47.
28. Somers CC, Ahmad N, Mejias A, et al. Effect of dexamethasone on re-spiratory syncytial virus-induced lung inflammation in children: resultsof a randomized, placebo controlled clinical trial. Pediatr AllergyImmunol 2009; 20:477–85.
29. Ermers MJ, Rovers MM, van Woensel JB, Kimpen JL, Bont LJ; RSVCorticosteroid Study Group. The effect of high dose inhaled corticoste-roids on wheeze in infants after respiratory syncytial virus infection:randomised double blind placebo controlled trial. BMJ 2009; 338:b897.
30. Fernandes RM, Bialy LM, Vandermeer B, et al. Glucocorticoids foracute viral bronchiolitis in infants and young children. Cochrane Data-base Syst Rev 2010; CD004878. doi:10.1002/14651858.
31. Lee FE, Walsh EE, Falsey AR. The effect of steroid use in hospitalizedadults with respiratory syncytial virus-related illness. Chest 2011; 140:1155–61.
32. Lee N, Hui DS. Dexamethasone in community-acquired pneumonia.Lancet 2011; 378:979–80.
33. Casiano-Colón AE, Hulbert BB, Mayer TK, Walsh EE, Falsey AR. Lackof sensitivity of rapid antigen tests for the diagnosis of respiratory syn-cytial virus infection in adults. J Clin Virol 2003; 28:169–74.
34. Walsh EE, Peterson DR, Kalkanoglu AE, Lee FE, Falsey AR. Viral shed-ding and immune responses to respiratory syncytial virus infection inolder adults. J Infect Dis 2013; 207:1424–32.
35. Duncan CB, Walsh EE, Peterson DR, Lee FE, Falsey AR. Risk factorsfor respiratory failure associated with respiratory syncytial virus infec-tion in adults. J Infect Dis 2009; 200:1242–6.
36. DeVincenzo JP, Wilkinson T, Vaishnaw A, et al. Viral load drivesdisease in humans experimentally infected with respiratory syncytialvirus. Am J Respir Crit Care Med 2010; 182:1305–14.
37. Lindsley WG, Blachere FM, Davis KA, et al. Distribution of airborne in-fluenza virus and respiratory syncytial virus in an urgent care medicalclinic. Clin Infect Dis 2010; 50:693–8.
38. Bonavia A, Franti M, Pusateri Keaney E, et al. Identification of broad-spectrum antiviral compounds and assessment of the druggability oftheir target for efficacy against respiratory syncytial virus (RSV). ProcNatl Acad Sci U S A 2011; 108:6739–44.
39. DeVincenzo J, Lambkin-Williams R, Wilkinson T, et al. A randomized,double-blind, placebo-controlled study of an RNAi-based therapy di-rected against respiratory syncytial virus. Proc Natl Acad Sci U S A2010; 107:8800–5.
Outcomes of Hospitalized Adults With RSV • CID • 9
by Norm
an Sharples on August 20, 2013
http://cid.oxfordjournals.org/D
ownloaded from




![IMAGEN Respiratory Syncytial Virus (RSV) [PT]...IMAGEN Respiratory Syncytial Virus (RSV) 1. UTILIZAÇÃO PREVISTA O IMAGEN Respiratory Syncytial Virus (RSV) é um teste qualitativo](https://img.pdfslide.net/doc/110x75/609c20ca1e0ebf036346e66d/imagen-respiratory-syncytial-virus-rsv-pt-imagen-respiratory-syncytial-virus.jpg)
























