Embed Size (px)
Citation preview
High Risk OB Case Studies
Patricia M. Witcher, RNC-OB, MSNNorthside Hospital
Labor and Delivery, High Risk ObstetricsAtlanta, Georgia
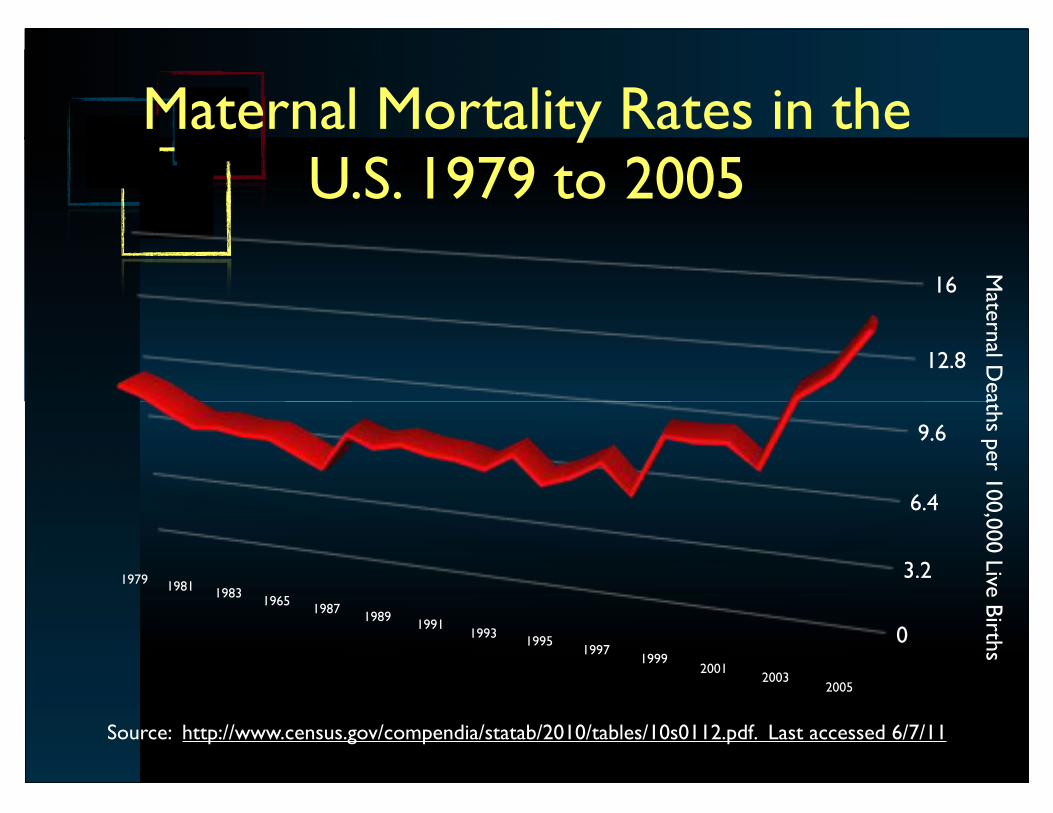
0
3.2
6.4
9.6
12.8
16
Matern
al Death
s per 1
00,0
00 Live B
irths
19791981
19831965
19871989
19911993
19951997
19992001
20032005
Source: http://www.census.gov/compendia/statab/2010/tables/10s0112.pdf. Last accessed 6/7/11
Maternal Mortality Rates in the U.S. 1979 to 2005
• Preterm labor
• Hypertensive disease
• Anemia / hemorrhage
• Infection-related
• Anesthesia-related complications
• Diabetes
• Embolism-related
Top Reasons for Hospitalization During Pregnancy
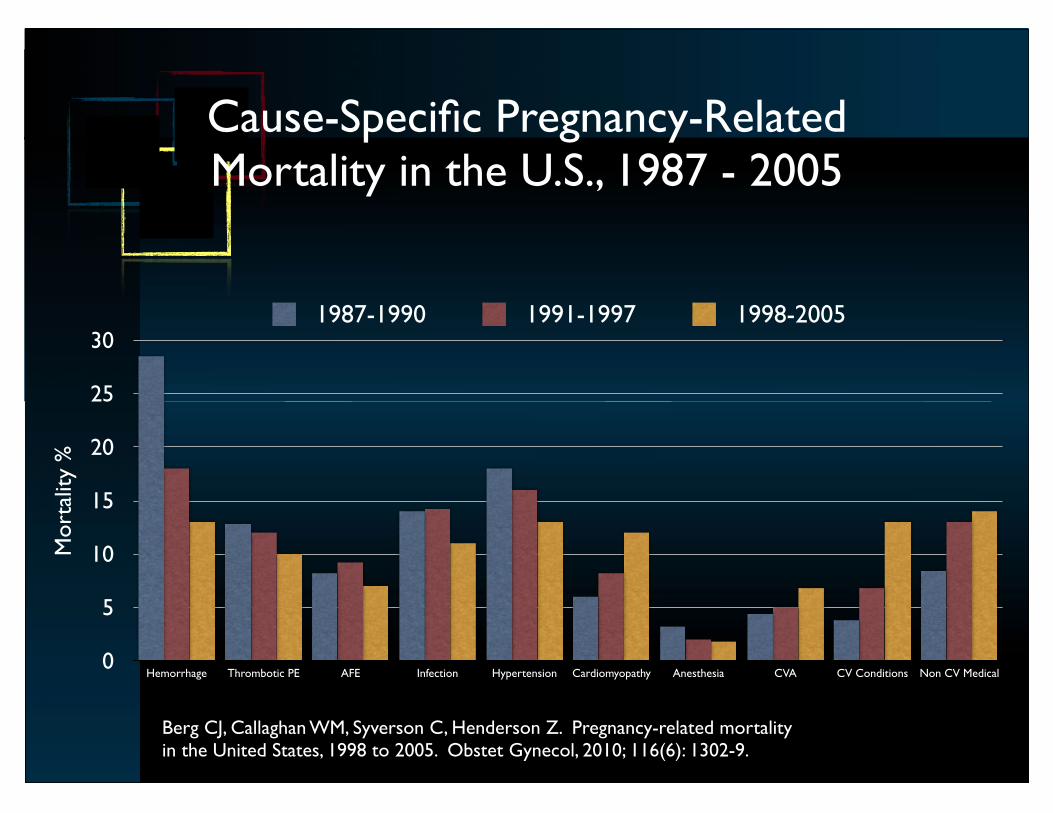
Cause-Specific Pregnancy-Related Mortality in the U.S., 1987 - 2005
0
5
10
15
20
25
30
Hemorrhage Thrombotic PE AFE Infection Hypertension Cardiomyopathy Anesthesia CVA CV Conditions Non CV Medical
Mort
ality
%
1987-1990 1991-1997 1998-2005
Berg CJ, Callaghan WM, Syverson C, Henderson Z. Pregnancy-related mortality in the United States, 1998 to 2005. Obstet Gynecol, 2010; 116(6): 1302-9.
Case Studies
• Case studies are not provided in handout material in order to protect the confidentiality of the patients and institutions from which they are derived.
Pregnancy Adaptations that Necessitate Consideration
During Assessment and Interventions
• Pregnancy does not change the overall therapeutic goal
–Restoring oxygenation is aggressive
–Interventions directed at restoring hemodynamic instability are not withheld out of concern for fetal effects
• Some clinical practices may require adaptation
General Considerations
• Hemodynamic and laboratory interpretation requires adaptation based upon normal values in pregnancy
– i.e. Septic shock criteria typically requires adaptation
– i.e. Renal insufficiency despite normal nonpregnant values
• Anticipate increased potential for anesthesia-related adverse events
– Difficult or failed airway
– Aspiration
• Pregnant women may deteriorate more rapidly due to changes in pulmonary volumes and mechanics
• Higher risk for complications (i.e. DKA)
• Increased risk for UTI and pyelonephritis
General Considerations
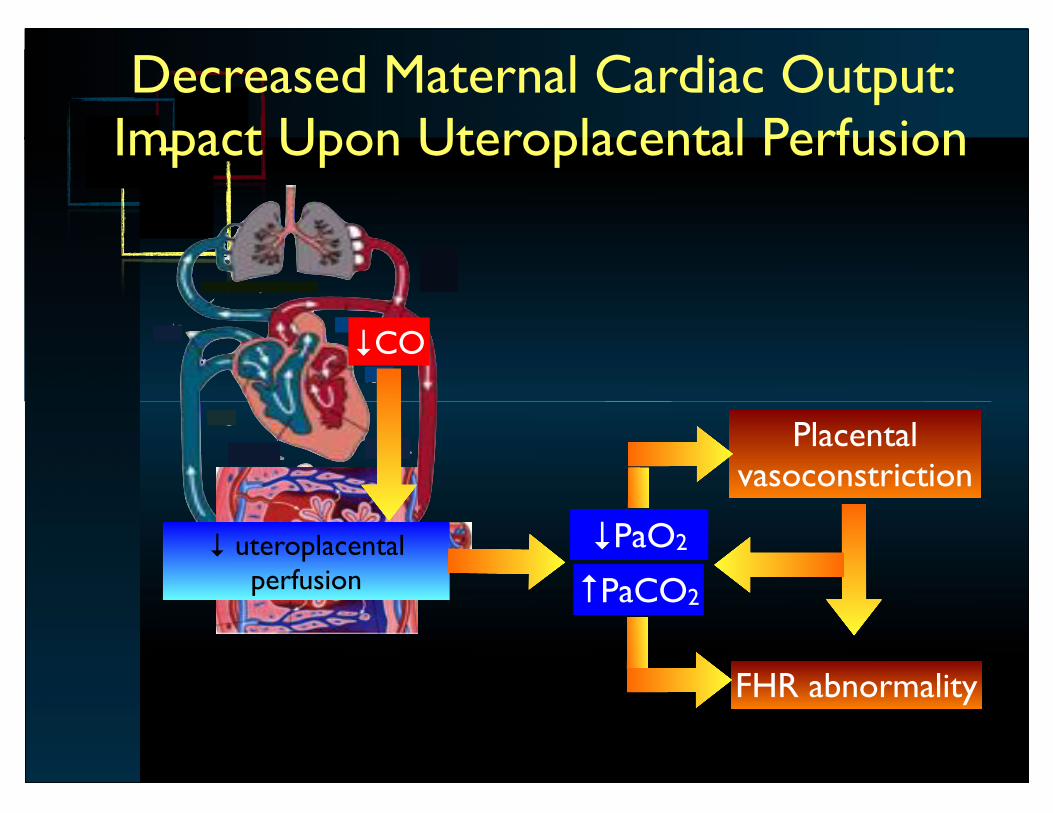
Decreased Maternal Cardiac Output: Impact Upon Uteroplacental Perfusion
!CO
! uteroplacental perfusion
!PaO2
"PaCO2
Placental vasoconstriction
FHR abnormality
• Assess according to normal hemodynamic values for pregnancy
• Ensure adequate circulating blood volume whenever possible to maintain uteroplacental perfusion
– Lateral positioning
– Judicious afterload reduction
– “Gental” diuresis in the setting of fluid overload
Hemodynamic Stabilization
• Uteroplacental perfusion
• Greatly determined by maternal cardiac output and circulating blood volume
• Maternal oxygenation status
Determinant of Fetal Oxygenation













![Ob US MRI Correlation.ppt - mc.vanderbilt.edu … · T1 and T2 Values for Brain Tissues at 1.5 Tesla ... • congenital infarction. ... Ob US MRI Correlation.ppt [Compatibility Mode]](https://img.pdfslide.net/doc/110x75/5af8a69a7f8b9a5f588d07ea/ob-us-mri-mcvanderbiltedu-t1-and-t2-values-for-brain-tissues-at-15-tesla.jpg)














