Embed Size (px)
Citation preview

J
C
HuLm
CT
a
5b
C
I
Jad
0d
ournal of Neuroradiology (2012) 39, 176—180
ASE REPORT
irayama disease: An uncommon cause of distalpper extremity deficit
a maladie d’Hirayama : une cause peu connue de déficit distal desembres supérieurs
. Darchisa,∗, S. Carona, A. Lacourb, M. Toledanoa,. Boulangera, F. Tempremanta
Service de Neuroradiologie, Hôpital Roger-Salengro, CHRU de Lille, boulevard du professeur Emile-Laine,9037 Lille cedex, FranceService de Neurologie D et centre de référence des maladies rares neuromusculaires, Hôpital Roger-Salengro,HRU de Lille, boulevard du professeur Emile-Laine, 59037 Lille cedex, France
KEYWORDSHirayama disease;Spine;MRI;Cord atrophy
Summary Hirayama disease is a myelopathy related to flexion movements of the neck thatproduce ischemic damage in the anterior horn of the cervical cord. The disease affects youngpeople and is characterized by a distal upper extremity deficit that develops gradually. Thediagnosis is confirmed by cervical magnetic resonance imaging (MRI) in flexion demonstrating aforward shift of the posterior dural sac and spinal cord compression. On radiology, there shouldbe suggestive signs in neutral position such as cord atrophy, intramedullary bilateral high signal
intensity on T2-weighted images, straightening of the cervical spine, and loss of attachmentbetween the posterior dural sac and subjacent lamina. Exploration should be completed by anMR study in neck flexion. We report here on two typical cases of the disease and also include areview of the literature.© 2011 Published by Elsevier Masson SAS.df
ntroduction
uvenile muscular atrophy of the distal upper extremity,lso termed ‘‘Hirayama disease’’, is a rare neurologicalisease reported especially in Japan. Clinically, Hirayama
∗ Corresponding author.E-mail address: [email protected] (C. Darchis).
aidcs[cm
150-9861/$ – see front matter © 2011 Published by Elsevier Masson SASoi:10.1016/j.neurad.2011.05.001
isease is characterized by weakness of the hands andorearms in association with unilateral or bilateral, usuallysymmetrical, muscular atrophy that develops graduallyn teenagers and young adults in their second and thirdecades [1]. In flexion position, the dural sac cannotompensate for the increased length of its posterior wall,
o an anterior shift of the posterior dural wall occurs2]. Ischemic damage in the anterior horn of the cervicalord attributed to arterial insufficiency during flexion andicrocirculatory changes also appear [3]. The diagnosis is.

mity
dm
meGnff
m
D
Hmsaybadbad
msnaiiiotseil
avgcdrlcamstflaoe
Hirayama disease: An uncommon cause of distal upper extre
confirmed by cervical magnetic resonance imaging (MRI) inboth neutral and flexion positions. The challenge for theradiologist is to identify signs suggestive of this pathologyon routine, non-flexion MR studies carried out to completethe examination in flexion position (approximately 30—40◦
of neck flexion) using a positioning sponge.This underdiagnosed disease has been described in only
a few reports in the literature. The present report is of twotypical cases of Hirayama disease and includes a review ofthe literature and describes the radiological signs.
Case 1
A 19-year-old Caucasian man was investigated in December2010 because of a 3- to 4-year history of insidious onset,initially slowly progressive, lower motor neuron syndrome ofthe upper limbs. His past medical history was unremarkableexcept for eczema, and his family history was negative forHirayama disease and neurological disorders. His symptomswere weakness of the left hand and, for the past 2 years,claw fingers of the right hand.
Neurological examination showed evident predominantleft muscle atrophy of both hands and also of the lower thirdof the forearms. The muscles of the upper arms and legswere completely normal. There was no proximal or lowerlimb strength deficit. Tendinous reflexes in all limbs werenormal, and there was no Babinski sign or sensory deficit.
Electromyography (EMG) of all limbs showed signs ofpredominantly left bilateral distal denervation with loss ofmotor units. No conduction blocks were identified. Nerveconduction studies showed normal sensory and motor veloc-ities of the median and ulnar nerves. In neutral position(Fig. 1), an MRI study showed flattening and atrophy of thelower cervical spinal cord at the level of C6—C7. There wasno increased signal intensity on T2-weighted images.
According to the principles by Guigui et al. [4] and Batz-dorf and Batzdorff [5], the cervical curvature was abnormaland showed straightening, which was confirmed by lateralradiography of the cervical spine. No intervertebral discherniation or degenerative change was present, nor wasthere any evidence of old traumatic injury. In flexion posi-tion (Fig. 2), anterior displacement of the posterior duralsac and cord compression were apparent. There was no fur-ther progression of symptoms at the follow-up, so no surgicaltreatment was performed.
Case 2
A 16-year-old boy presented with atrophy of the right upperlimb. His medical history was unremarkable except for dal-tonism. The patient had noticed slowly progressive weaknessof the fourth and fifth right fingers as well as atrophy of theright hand over the past year. Then, a few weeks ago, thepatient presented with weakness of the first three right fin-gers. Clinical examination showed evident atrophy of thethenar, hypothenar and interosseous muscles of the righthand. Right ulnar claw was present. There were fascicula-
tions in the first interosseous muscle. The right hand deficitwas predominantly distal and involved the flexor digito-rum, wrist flexors and interosseous muscles. Wrist extensorswere normal. There was no proximal or lower limb strengthcpsc
deficit 177
eficit; reflexes and sensation were symmetrical and nor-al. Postural tremors of the right hand were also present.EMG showed denervation changes mainly in the C8—T1
uscles. A sensory conduction study was normal. Motorvoked potentials confirmed denervation in C8—T1. Anti-M1 antibody assay was negative. An MRI study performed ineutral position and in flexion of the cervical spine showedorward displacement of the posterior dural sac extendingrom C4 to T2.
The patient’s condition remained unchanged at the 3-onth follow-up. No surgical intervention was required.
iscussion
irayama disease is a myelopathy related to flexion move-ents of the neck with an insidious onset and an initially
low progression generally followed by spontaneous arrestfter several years. Symptoms are usually seen in boys andoung adults, and progress over 1—3 years before they sta-ilize [1] with predominantly unilateral muscular atrophy,nd weakness in the hand and forearm. The first case wasescribed by K. Hirayama in 1959 [6]. Hirayama disease haseen documented in around 300 patients, mostly from Japannd other Asian countries. Only sporadic cases have beenescribed in Europe [7].
The disease is rarely familial. There is no sensory involve-ent, and typically, no pyramidal involvement. Bilateral
ymmetrical involvement has been described [8,9]. Diag-ostic criteria [2] have included the following: weaknessnd atrophy predominantly in the C7, C8 and T1 myotomesn one upper limb or asymmetrically in both upper limbs;nsidious onset in teenagers or in those in their early 1920s;nitially rapid progression for 1—3 years, followed by arrestf the disease or a relatively benign course; irregular coarseremors in the fingers of the affected hand; mild tran-ient worsening of symptoms on exposure to cold; EMGvidence of chronic denervation in the clinically or subclin-cally affected muscles; and absence of objective sensoryoss.
The disease mechanism is unclear, but symptoms arettributed to the forward displacement of the posterior cer-ical dural sac when the neck is in flexion due to imbalancedrowth between the patient’s vertebral column and spinalord [2]. However, an atypical case with anterior duraletachment was described in 2009 [7], and showed a poste-ior position of the lower cervical spinal cord mainly due to aoss of anterior attachment of the dura mater from the adja-ent vertebral body. In this case, the patient had flatteningnd atrophy of the lower cervical spinal cord. The causalechanism behind such flexion-induced myelopathy was
upported by focal ischemic damage in the anterior horn ofhe cervical cord attributable to arterial insufficiency duringexion and microcirculatory changes [3]. Compression of thenterior cervical dural sac is associated with compressionf the anterior spinal artery, resulting in focal ischemia. Anpidural mass and compressive flattening of the lower cervi-
al cord have also been observed during flexion [9]. Negativeressure created in the posterior spinal canal and compres-ion of the anterior plexus by anterior shifting of the duralanal are responsible for increased flow to the posterior
178 C. Darchis et al.
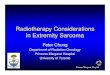
Figure 1 Case 1. In neutral position: (A): sagittal T2 weighted MRI in neutral position: cord atrophy (arrow) of the lower cervicalspine at the level C6-C7 without signal abnormality. Straight curvature is also depicted; (B1): axial T2 on neutral flexion at thepedicular level on C6: loss of attachment between the posterior dural sac and subjacent lamina (Arrow). Flattening of the lowercervical spine. (Large arrow) (B2): schema illustrating loss of attachment on neutral position. In neck flexion: (C): flexion positionsagittal T2 weighted MRI and (D): axial T1 weighted contrast-enhanced show forward displacement of the posterior dural sac andc voidl erior
is
us
12
3
ord compression (arrow). An epidural mass with multiple signalower cervical canal caused by venous engorgement of the post
nternal vertebral venous plexus. Neck flexion is also respon-ible of decreased venous drainage of the jugular vein [10].
Examination of neutral position MR imaging findings isseful for depicting Hirayama disease. This position canhow:
) lower cervical cord atrophy;) asymmetrical cord flattening and;
ss
•
s suggestive of slow flow (large arrow) is visible in the posterior epidural venous plexus during neck flexion.
) intramedullary bilateral high signal intensity on T2-weighted MR images of the anterior cervical horns.
However, at an early stage, these signs may be missing,
o the radiologist should instead be alerted by the followingigns:abnormal cervical curvature (straight or kyphotic);

Hirayama disease: An uncommon cause of distal upper extremity deficit 179
Figure 2 Case 2. (A): sagittal T1 weighted contrast-enhanced in neutral position and (B) in flexion: forward displacement of theposterior dural sac (arrow) and cord compression in flexion by the enlargement of the epidural posterior space without evident
C
Cah
D
Tc
R
abnormality in neutral position.
• forward shifting of the posterior dural sac and;• loss of attachment between the posterior dural sac and
subjacent lamina.
Separation by more than 33.3% measured at the pedic-ular level of C4—C6 is also considered a positive sign [1].An MRI study in flexion position helps to diagnose Hirayamadisease. A positioning sponge can be used to obtain approx-imately 30—40◦ of neck flexion, depending on how much thepatient can tolerate. According to the patient’s morphology,it may be of interest to use open-field MRI. A study in flex-ion can depict any forward displacement of the posteriordural sac, effacement of the cerebrospinal fluid space atmultiple levels and posterior epidural plexus engorgement[11].
Forward shifting of the posterior dural sac is also seenin normal subjects, but without spinal cord compres-sion. However, measurement criteria in a flexion positionhave been described to differentiate normal from dis-eased subjects [11]. The ratio of the anteroposteriordiameter of the posterior dural sac at maximum for-ward shift to the anteroposterior diameter of the spinalcanal should be increased in Hirayama disease, andthe ratio of the anteroposterior diameter of the spinalcord to the perpendicular transverse diameter of thespinal cord should be decreased in flexion position com-pared with that in neutral position in Hirayama disease.These ratios do not change in normal healthy sub-jects.
Differential diagnoses that should be excluded includesyringomyelia, amyotrophic lateral sclerosis, cervicalspondylotic myelopathy, expansile lesions, motor neu-ron disease and hereditary distal motor neuropathies.
To prevent functional disability, cervical-collar therapyis necessary. Cervical decompression with or withoutduraplasty as a surgical intervention has also had goodresults.onclusion
linical history and MRI signs as revealed in both neutralnd flexion positions with the use of objective measures areelpful for diagnosing Hirayama disease.
isclosure of interest
he authors declare that they have no conflicts of interestoncerning this article.
eferences
[1] Chen C, Hsu H, Tseng Y, Lyu R, Chen C, Huang Y, et al.Hirayama flexion myelopathy: neutral position MR imag-ing findings–importance of loss of attachment. Radiology2004;231(1):39—44.
[2] Xu X, Han H, Gao H, Hou C, Fan D, Fu Y, et al. The increasedrange of cervical flexed motion detected by radiographs inHirayama disease. Eur J Radiol 2011;78(1):82—6.
[3] Ciceri EF, Chiapparini L, Erbetta A, Longhi L, Cicardi B,Milani N, et al. Angiographically proven cervical venousengorgement: a possible concurrent cause in the patho-physiology of Hirayama’s myelopathy. Neurol Sci 2010;31(6):845—8.
[4] Guigui P, Benoist M, Deburge A. Spinal deformity and instabilityafter multilevel cervical laminectomy for spondylotic myelopa-thy. Spine 1998;23:440—7.
[5] Batzdorf U, Batzdorff A. Analysis of cervical spine cur-vature in patients with cervical spondylosis. Neurosurgery1988;22:827—36.
[6] Hirayama K, Toyokura Y, Tsubaki T. Juvenile muscular atro-phy of unilateral upper extremity: a new clinical entity (in
Japanese with English Abstract). Psychiatr Neurol Jpn 1959;61:2190—8.[7] Meijerink MR, Castelijnsa J, Barkhofa F. Segmental muscularatrophy of the distal upper extremity (Hirayama disease): an

1
[
[
80
atypical case with anterior dural detachment. Eur J RadiolExtra 2009;72(2):e53—5.
[8] Pradhan S. Bilaterally symmetric form of Hirayama disease.Neurology 2009;72(24):2083—9.
[9] Elsheikh B, Kissel JT, Christoforidis G, Wicklund M, KehagiasDT, Chiocca EA, et al. Spinal angiography and epidural venog-raphy in juvenile muscular atrophy of the distal arm ‘‘Hirayamadisease’’. Muscle Nerve 2009;40(2):206—12.
C. Darchis et al.
10] Chen CJ, Chen CM, Wu CL, Ro LS, Chen ST, Lee TH.Hirayama disease: MR diagnosis. AJNR Am J Neuroradiol1998;19(2):365—8.
11] Lai V, Wong YC, Poon WL, Yuen MK, Fu YP, Wong OW. Forward
shifting of posterior dural sac during flexion cervical magneticresonance imaging in Hirayama disease: an initial study on nor-mal subjects compared to patients with Hirayama disease. EurJ Radiol 2010. [Epub ahead of print].