Embed Size (px)
Citation preview

I Clin Pathol 1992;45:645-649
Occasional articles
Histology of normal haemopoiesis: Bone marrow
histology I
B S Wilkins
IntroductionThe bone marrow trephine biopsy specimenholds an unusual position among pathologicalspecimens. Having been obtained in mostcases by a haematologist, the biopsy specimenis processed in a histopathology laboratory andis then reported either by a haematologist or a
histopathologist, depending on local custom.Individual practitioners may acquire great skillin the interpretation of trephine biopsy speci-mens, but others in both branches of pathologyare sometimes perplexed when faced withtissue appearances for which other experiencewithin their individual disciplines may not haveprepared them fully. Ideally, interpretationshould be a collaborative procedure, combin-ing the clinical and cytological knowledge ofthe haematologist with the histopathologist'sskills in analysis ofnormal and abnormal tissuestructure.An important starting point for all con-
cerned is to have a good appreciation of thenormal appearances of haemopoiesis as repre-
sented in a trephine biopsy specimen, againstwhich abnormal changes can then be assessed.The purpose of this article is to describe thesenormal appearances and to indicate brieflysome uses and limitations ofvarious processingand staining techniques in bone marrow biopsyspecimen interpretation.
UniversityDepartment ofPathology,Southampton GeneralHospital, TremonaRoad, SouthamptonS09 4XYB S WilkinsCorrespondence to:Dr B S WilkinsAccepted for publication20 December 1991
General structure of bone marrow
It is impossible to describe the haemopoietictissue of bone marrow without at least a briefreference to the underlying bony structure. Atrephine biopsy specimen may have a quantityof dense, cortical bone (and even extraneouselements such as cartilage or tendon) at itsouter end, but for the most part consists oftrabecular bone-a meshwork of delicate bonyplates and strands within which the haemo-poietic tissue and its stroma are suspended.'The precise distribution of bony trabeculae, inthe iliac crest as at other sites, is determinedprimarily by mechanical aspects of bone func-tion, but the spaces of varying size and shapewhich lie between adjacent trabeculae com-
prise the basic structural units of haemo-poiesis.The trabecular surfaces are covered by a
layer of endosteal cells, usually inconspicuousbut sometimes recognisable as osteoblasts.Occasional multinucleate osteoclasts are also a
normal finding at trabecular margins. A sinu-soidal network arborises throughout the inter-
trabecular spaces,2 but little is known aboutthe dynamics of blood flow through humanbone marrow. Arterioles and venules tend to lietowards the centres of intertrabecular spaces.They are usually seen in only a small propor-tion of intertrabecular spaces in any one biopsyspecimen, suggesting that each may supply ordrain a number of such spaces.The trabeculae, arterioles, and venules form
the structural framework around whichgranulopoiesis develops. Erythropoiesis andmegakaryopoiesis occur in apposition to thefine, branching sinusoids.
MARROW STROMA
The trabecular and vascular architecture ofmedullary bone provides the basic framework,nutritional supply, and waste removal systemfor haemopoiesis, but specialised support ofthe self-renewal and differentiation of haemo-poietic precursors is provided by the bonemarrow stroma. This stroma consists of aheterogeneous mixture of adipocytes, fibro-blasts, and macrophage-like cells, togetherwith a complex extracellular matrix of reticu-lin, binding proteins, including fibronectin andhaemonectin, and proteoglycans.3 In culturesystems specific haemopoietic microenviron-ments-for example, for erythropoiesis orgranulopoiesis-can be shown to be deter-mined by the nature of the stromal cells andthe binding of growth factors to restrictedmatrix sites.4 How this correlates with thespatial distribution of haemopoiesis withinintact marrow in vivo is not yet understood.
Despite this evidence of its important con-tribution to normal haemopoiesis, bone mar-row stroma appears disappointingly bland onconventional histological examination. Adipo-cytes are readily apparent and small numbersof scattered fibroblasts can usually be dis-cerned. Reconisable macrophages are remark-ably few: those which contain storage iron canbe demonstrated by Perls's stain, but they arenot numerous in normal marrow and onlyoccasionally can they be seen to lie in closeproximity to developing erythrocytes. Immu-nostaining of paraffin wax embedded trephinebiopsy sections using macrophage reactivemonoclonal antibodies such as Mac387 (anti-calgranulin; Dako UK Ltd) and KP1 (CD68;Dako UK Ltd) also shows only small numbersof macrophages in normal marrow (unpub-lished observation).
Spindle cells expressing alkaline phospha-tase, butyrate esterase, or fibroblast associated
645
on 18 July 2018 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.45.8.645 on 1 A
ugust 1992. Dow
nloaded from

Wilkins
A~~~~~~~~~~~~,
~~~~.
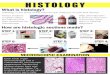
Figure i Normal paratrabecular zone of promyelocytes
and myelocytes. Streptavidin-biotin complex
immunoperoxidase technique using the monoclonal
antibody NP57, reactive with neutrophil elastase.
~~~ ~ ~ ~ ~ ~ ~ ~ ~ A
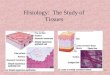
Figure 2 Normal clusters of proerythroblasts and
normoblasts. Streptavidin-biotin complex
immunoperoxidase technique using the monoclonal
antibody Ret4Of, reactive withff-sialoglycoprotein
(glycophorin C).
antigens have been shown in frozen or resin
embedded sections5` and in cultured marrow
stroma, but the precise functions of these cells
remain uncertain.
BONE MARROW CELLULARITY
This term is usually used with reference to the
haemopoietic cell content of a bone marrow
biopsy specimen relative to its adipocyte con-
tent. Biopsy specimens are generally con-
sidered to be of normal cellularity if 40-60% of
the non-bony tissue is composed of haemo-
poietic cells. Cellularity varies widely with age
and site, however, so that in a neonate normal
cellularity may be 100% and in an elderly
patient it may be 20%.8 Haematologists and
pathologists who regularly assess trephine
biopsy specimens will also be well aware that
intertrabecular spaces immediately beneath
the bony cortex are frequently hypocellular,
especially in the elderly, and may be unrepre-
sentative of the cellularity deeper in the biopsy
specimen.
GRANULOPOIESIS
The earliest recogznisable gyranulop)oietic pre-
cursors, the promyelocytes and myelocytes, lieadacent to the surfaces of bony trabeculae (fig1) and the adventitial aspect of small bloodvessels.89 With increasing distance from thetrabecula or vessel, increasing numbers ofmetamyelocytes and mature polymorphs are
seen. This radial orientation of granulopoiesiscan be appreciated easily in reactive granulo-cytic hyperplasia or chronic granulocytic leu-kaemia but is not always obvious in normalmarrow, in which the zone of promyelocytesand myelocytes may only be one or two cellsthick. In undecalcified resin-embedded biopsyspecimens the immature granulopoietic zonecan be highlighted by Leder's stain for chlor-oacetate esterase,'0 which tends to react morestrongly with promyelocytes and myelocytesthan with later granulocytes. Unfortunately,this visually impressive staining technique can-not be performed successfully with biopsyspecimens decalcified by formic or acetic acids,as the enzyme activity is lost. However, a verysimilar demonstration of the distribution ofearly granulocytes can be achieved in decal-cified, wax-embedded biopsy specimens byimmunohistochemical staining for neutrophilelastase" (fig 1).
In general, using routine stains, little granu-larity can be appreciated in granulocytes oftrephine biopsy specimens which have under-gone acid decalcification, with the exception ofeosinophils, whose granules are well pre-served.
Occasional promyeloctes and myelocytes,scattered singly or in small clusters, occur atsites distant from trabeculae and vessels, and itis therefore not necessarily abnormal to seeimmature granulocytes in the centres of inter-trabecular spaces.
MONOPOIESIS
The close association of granulopoiesis andmonopoiesis in bone marrow culture systemsin vitro'2 suggests that within intact marrowmonocyte precursors should be found in asimilar distribution to that of granulocytes.Monocytes, however, are difficult to recognisein trephine biopsy sections and little is knownabout the spatial organisation of their develop-ing precursors. No staining technique is cur-rently widely available for reliable and specificdemonstration of monocytes in fixed trephinebiopsy specimens. Butyrate esterase enzymeactivity does not survive routine processing,although it may be preserved by some resin-embedding protocols.6 Most immunohisto-chemical agents which will react in decalcified,wax embedded trephine biopsy specimens fordemonstration of monocytes (Mac387, CD 15,C68) also react strongly with granulo-cytes,'3- ' which predominate in normal mar-row and tend to obscure any monocytespresent.
ERYTHROPOIESIS
Erythrocytes develop in small clusters whichare dispersed throughout the intertrabecularspaces9 but which tend not to encroach on theparatrabecular and perivascular zones of earlygranulocytes. In a trephine biopsy sectionthese clusters measure about 5-10 cells indiameter. Erythroid clusters have a radialorganisation, with proerythroblasts in the cen-tre and progressively more mature formstowards the periphery (fig 2). Convincingevidence of a close spatial association between
646
on 18 July 2018 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.45.8.645 on 1 A
ugust 1992. Dow
nloaded from

Histolog, oJ'noriwral haemopoiesis: Bone marrou, histol(gy Is ^ ...w ... ^ w
.> t? 5 v6@Jgge . :.@
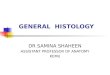
(B)Figure 3 (A) Appearance of normal erythroid cells following decalcification andwax-embedding: shinkage artefact causes perinuclear halo formation. (B) Normaleythroid ceUs in an undecalcified, resin-embedded trephine biopsy specimen. Theircytoplasmic margins are indistinct, giving the clusters a syncytia-like appearance.
Figure 4 Normal megakaryocyte in close association with a marrow sinusoid (theretraction is artefactual). Inset A: small, mononuclear megakaryocyte, presumablyimmature. Inset B: irregular bare nucleus, presumed to represent a senescentmegakaryocyte.
such clusters and marrow sinusoids can rarelybe seen in routine histological sections.
Erythroid clusters are usually readily appar-ent in normal marrow trephine biopsy speci-mens by virtue of the dense blue-black colourof the compact, round nuclei of mid- and latenormoblasts in sections stained with haema-toxylin and eosin. Giemsa staining showsintense cytoplasmic basophilia in proerythro-blasts and early normoblasts. Immunohis-tochemical staining of a and /3 sialoglycopro-teins (glycophorins A and C)'6 17 can also beused to demonstrate erythropoiesis (fig 2).A helpful artefact occurs in decalcified, wax
embedded trephine biopsy specimens whichcontributes to the ease of recognition oferythroid cells. Shrinkage of the nucleus leavesa clear perinuclear halo in each cell (fig 3A).This can assist in distinguishing erythroid cellsfrom lymphocytes, which have darkly stainingnuclei of a similar size to those of latenormoblasts. Fortunately, although perinu-clear haloes are absent from undecalcified,resin-embedded biopsy specimens, the mor-phology of red cell precursors is usually dis-tinctive in haematoxylin and eosin or Giemsastained sections from bone marrow biopsyspecimens processed in this way (fig 3B).
MEGAKARYOPOIESISMature megakaryocytes can easily be identi-fied in tissue sections because of their largesize, voluminous cytoplasm and nuclear multi-lobulation. They are found scattered singlythroughout intertrabecular spaces,9 evenly dis-tributed, except that they are usually absentfrom the immediate paratrabecular and peri-vascular zones occupied by early granulocytes.As with erythroid clusters, it is often difficult tosee sites of intimate association between mega-karyocytes and sinusoids (fig 4). However,electron microscopic studies have shown thatperipheral cytoplasm of megakaryocytes pro-trudes into sinusoidal lumina and is shed intothe intravascular compartment in the form ofpro-platelets which subsequently fragment togive rise to platelets.9 18The precursors of megakaryocytes cannot
always be readily identified within normal bonemarrow trephine sections. Occasional, small,mononuclear forms can be found (fig 4; insetA), but their ontogenic relation to maturemegakaryocytes is not known. The difficulty ofrecognising early megakaryocyte precursorsexists because such cells are smaller than theirprogeny and may resemble promyelocytesmorphologically. Giemsa staining can showcells in trephine biopsy sections which areprobably megakaryocyte precursors: they havegrainy lilac-pink cytoplasm resembling that oftheir mature counterparts. Some of the subtlevariation in cytoplasmic coloration betweenhaemopoietic cell lineages afforded by Giemsastaining is absent from decalcified biopsyspecimens, and an alternative approach is toperform immunohistochemical staining forfactor 8 related antigen or CD6 1 (plateletglycoprotein 3a)." Low numbers of small,mononuclear cells, presumed to be mega-karyocyte precursors, are present which
(A)
647
on 18 July 2018 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.45.8.645 on 1 A
ugust 1992. Dow
nloaded from

648
express these antigens. Such cells are appar-ently randomly distributed throughout inter-trabecular spaces.
Also normally present in small numbers arescattered megakaryocyte nuclei with a convo-luted outline and condensed chromatin pat-tern, apparently bare of cytoplasm (fig 4: insetB). These are considered to represent senes-cent megakaryocytes.
OTHER CELLS REGULARLY PRESENT IN NORMAL
BONE MARROW
LymphocytesThe distribution and morphology of lympho-cytes within bone marrow biopsy specimensoffer no clues as to whether these cells areundergoing some part of their developmentthere or are simply in transit through thetissue.
Small lymphocytes of B and T phenotypesare present in low to moderate numbersscattered throughout the intertrabecularspaces. Clusters of a few lymphocytes, normal-ly termed lymphoid aggregates, and largercollections termed lymphoid nodules are alsofrequently seen. The larger lymphoid nodulesmay incorporate a few macrophages and smallvascular channels and they occasionally formtrue follicles with germinal centres. Lymphoidaggregates and nodules only rarely lie imme-diately adjacent to trabeculae; collections oflymphoid cells at such sites should raise astrong suspicion of lymphomatous infiltration.Criteria for distinguishing benign from malig-nant lymphoid infiltrates within bone marrowbiopsy specimens have been described in detailby Rywlin and colleagues. 9 However, evenmorphologically benign aggregates may beassociated with subsequent lymphoid malig-nancy, " and they should always be assessedcautiously.
Plasma cellsThese cells are usually present in small num-bers, clustered at the adventitial margins ofsmall blood vessels. They are also foundscattered singly elsewhere in the intertra-becular spaces.
Mast cellsThe relation between mast cells and basophilgranulocytes remains uncertain. It is believedcurrently that both cell types arise by inde-pendent pathways from a common partiallycommitted basophil stem cell.9 Metachromaticand immunohistochemical staining of mast.cells in trephine biopsy specimens shows nospatial relation between developing basophilsand mast cells, nor are cells found whichexhibit transitional morphological, tinctorial,or immunohistochemical appearances."Mast cells can be detected in about 50% of
trephine biopsy specimens by metachromaticstaining. Their number is generally small innormal marrow and they tend to lie imme-diately adjacent to the endosteal surfaces andat the adventitial borders ofblood vessels. Theyare also frequently found at the periphery oflymphoid nodules.821 Morphologically, theyare usually either spindle-shaped or oval with
homogeneous pink cytoplasm on haematoxyand eosin staining and a small, dense rounucleus. They stain metachromatically wGiemsa, but are difficult to discern amclarge numbers of developing granulocytOther metachromatic stains, such as toluidblue or buffered thionine, are more usefultheir demonstration. Immunostaining canperformed using the antibody AAI, reactwith mast cell tryptase,- which does not crcreact with basophils.
ConclusionA great variety of cells, haemopoietic and n(haemopoietic, are present within normal bcmarrow. In keeping with the highly speciali,functions of the tissue, there is a complex Iorderly spatial organisation of cells withinAlthough we do not yet fully understandrelations between bone marrow structure afunction, knowledge in this sphere is advancas in vitro culture systems provide insights iithe roles of cell-cell and cell-stroma intactions in haemopoiesis. Careful histologianalysis of intact bone marrow biopsy spcmens will also contribute to this increaseknowledge of normal haemopoiesis.For haematologists, histopathologists a
any other practitioners engaged in the dinosis ofbone marrow disorders, I hope thatforegoing account will be of practical useclarify current concepts of normal haenpoietic cell organisation and to set a threshiagainst which abnormal haemopoiesis canassessed.
1 Frisch B, Lewis SM, Burkhardt R, Bartl R. IntroductIn: Biopsy pathology of bone and bone marrow. Lon(Chapman and Hall, 1985:1-17.
2 Wickramasinghe SN. Organisation, blood and nerve sulof bone marrow and some properties of non-hae:poietic cells. Human Bone Marrow. Oxford: BlackScientific Publications, 1975:60-81.
3 Campbell AD, Wicha MS. Extracellular matrix andhematopoietic microenvironment. 7 Lab Clin1988;112:140-6.
4 Gordon MY, Riley GP, Watt SM, Greaves MF. C,partmentalisation of a haematopoietic growth fa(GM-CSF) by glycosaminoglycans in the bone marmicroenvironment. Nature 1987;326:403-5.
5 Burgio VL, Pignoloni P, Baroni CD. Immunohistologbone marrow: a modified method of glycol-methacr3embedding. Histopathology 1991;18:37-43.
6 Beckstead JH, Halverson PS, Ries CA, BaintonEnzyme histochemistry and immunohistochemistrybiopsy specimens of pathologic human bone marBlood 1981;57:1088-98.
7 Dilly SA, Jagger CJ. Bone marrow stromal change-haematological malignancies. J Clin Pathol 1990942-6.
8 Frisch B, Bard R. Biology, structure and componentnormal bone marrow. In: Atlas of bone marrow pathoiCurrent Histopatholgy. Vol 15. London: Kluwer AcadePublishers, 1990:9-37.
9 Wickramasinghe SN. Normal Haemopoiesis: cellular c,position ofnormal bone marrow. In: Wickramasingheed. Blood and Bone marrow. Volume 2. Systemic pathoi3rd Edn. Edinburgh: Churchill Livingst(1989:41 -72.
10 Bancroft JD, Stevens A, eds. Enzyme histochemisDiagnostic applications. In: Theory and practice of hlogical techniques. 3rd Edn. Edinburgh: Churchill Livstone, 1990:406-7.
1 1 Pulford KA, ErberWN, Crick JA, et al. Use of monochantibody against human neutrophil elastase in norand leukaemic myeloid cells. J Clin Pc1 988;41 :853-60.
12 DexterTM, Spooncer E. Growth and differentiation inhemopoietic system. Ann Rev Cell Biol 1987;3:423-4
13 WiIkins BS, Jones DB. The use of immunohistocherrtechniques with fixed, decalcified, wax-embedded bmarrow trephine biopsies. Haematol Rev 1989;3:149-
14 Van der Valk P, Mullink H, Huijgens PC, Tadema TM,W, Meier CJLM. Immunohistochemistry in bone mar
wil
on 18 July 2018 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.45.8.645 on 1 A
ugust 1992. Dow
nloaded from

Histology oJ nornmal haemopoiesis: Bone nmarrow histology I
diagnosis. Value of a panel of monoclonal antibodies onroutinely processed bone marrow biopsies. Amz 7 SurgPathol 1989;13:97-106.
15 Pulford KA, Rigney EM, Micklem KJ, et al. KP 1: a newmonoclonal antibody that detects a monocyte/macro-phage associated antigen in routinely processed tissuesections. Clin Pathol 1989;42:414-21.
16 Anstee DJ, Edwards PAW. Monoclonal antibodies to humanerythrocytes. Eur lmmunol 1982;12:228-32.
17 Gatter KC, Cordell JL, Turley H, et al. The immunohisto-logical detection of platelets, megakaryocytes and throm-bi in routinely processed specimens. Histopathology1988;13:257-67.
18 Tavassoli M, Aoki M. Localisation of megakaryocytes in thebone marrow. Blood Cells 1989;15:3-14.
19 Rywlin AM, Ortega RS, Dominguez CJ. Lymphoid nodulesof bone marrow. Blood 1974;43:389-400.
20 Faulkner-Jones BE, Howie AJ, Boughton BJ, Franklin IM.Lymphoid aggregates in bone marrow: study of eventualoutcome. Clin Pathol 1988;41:768-75.
21 Nock ID, WiIkins BS, Jones DB. Bone marrow mast cellsrevisited. Pathol 1991 ;164:352A.
22 Walls AF, Jones DB, Williams JH, Church MK, Holgate STImmunohistochemical identification of mast cells informaldehyde fixed tissue using monoclonal antibodiesspecific for tryptase. 7 Pathol 1990;162:119-26.
649
on 18 July 2018 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.45.8.645 on 1 A
ugust 1992. Dow
nloaded from