Embed Size (px)
Citation preview
Hormone Receptors in Rapidly Progressing Breast Cancer
PAUL H. LEVINE," FRANCOISE TABBANE,? LARRY R. MUENZ,' LAKSHMI S. KAMARAJU,* SAROJ DAS,+ SEENA POLIVY,+ SLIM BELHASSEN,t SUSY M. SCHOLL,* J. GEORGE BEKESI,§ AND NEJIB MOURALlt
Biopsy specimens from 85 Tunisian breast cancer patients were compared with those of 95 American breast cancer patients for estrogen receptor (ER) and progesterone receptor (PR) levels. Tunisian patients with rapidly progressing breast cancer (RPBC) had lower ER levels than American patients or Tunisian patients without evidence of RPBC. Lower ER levels in the earliest stage of RPBC, which presents without inflammatory signs, supported epidemiologic and pathologic studies indicating that rapid growth as reported by the patient is an important aspect of RPBC. Low ER levels were generally found in young, premenopausal Tunisian women with advanced RPBC; multivariate analyses suggest that age was the most important correlating factor. In the Tunisian patients, ER levels showed a direct correlation with response to therapy. No consistent relationship between American and Tunisian patients or subgroups was observed for PR levels. These results indicate the need for reevaluating the routine use of oophorectomy in RPBC.
Cancer 54:3012-3016, 1984.
N AGGRESSIVE FORM of breast cancer, generally A designated Pousee Evolutive (PEV) or Rapidly Progressing Breast Cancer (RPBC) in French and Tuni- sian publication^'-^ shares many clinical and pathologic features with inflammatory breast cancer (IBC) in the United state^.^.^ Previously performed epidemiologic studies suggested a possible hormonal influence; late menarche, multiparity, and an association with preg- nancy were more common in Tunisian patients with RPBC than in other Tunisian breast cancer patients. To further investigate the possible hormonal relationship to RPBC, we studied a series of Tunisian breast cancer patients for hormone receptor levels and compared the results with a series of American breast cancer patients studied simultaneously in the same laboratory.
Materials and Methods
Biopsy specimens for this study were obtained at the time of diagnosis from all breast cancer patients seen at
Supported in part by DHEW, NIH, Research Project Agreement
* National Cancer Institute, National Institute of Health, Bethesda,
f Institute Salah Azaiz, Tunis, Tunisia. $ Litton Bionetics, Kensington, Maryland. 4 Mt. Sinai Medical School, New York, New York. Address for reprints: Paul H. Levine, Clinical Epidemiology Branch,
5A2 1 Landow Building, National Cancer Institute-NIH, Bethesda, MD 20205.
The authors thank Mary Ann Abraham and Barbara Salins for their help in preparation of the manuscript.
Accepted for publication November 7, 1983.
NO. 07-002- 1.
Maryland.
the Institute Salah Azaiz (ISA) in Tunisia between May, 1977 and May, 1980 whose tumors were sufficiently large to allow hormone receptor studies. Portions of each biopsy specimen were placed in formalin for patho- logic evaluation and adjacent portions were frozen at -70°C immediately after collection in Tunisia. Ship- ments of specimens were sent in dry ice and the tumors were kept frozen at -70°C until testing for hormone receptors. Patients were categorized according to their PEV or RPBC status at the time of their first visit to the ISA. As previously reviewed: the diagnosis of RPBC was made as follows: PEV-0 is the designation given to breast tumors without evidence of rapid growth: the diagnosis of PEV-1 is based on the report of the patient that there has been rapid growth; PEV-2 is associated with redness, warmth, and edema involving less than 50% of the breast; and patients with PEV-3 have redness, warmth, and edema involving more than 50% of the breast.
Treatment of the patients in this study was as described in our earlier report^.^*^-^ Surgical therapy formed the basis of management of patients with PEV-0, MO turn or^.^ Patients with limited disease (Tl, T2, T3 < 7 cm) subsequently had radiotherapy if lymph nodes were involved. Radiotherapy preceded surgery in T3 patients with tumors greater than 7 cm and in T4 patients, as well as in any patients with N2 or N3 disease. For patients classified as having PEV-1, PEV-2, or PEV-3 disease, the initial treatment after biopsy was surgical castration if they were still ovulating or had entered menopause within the past 3 years. Forty-five PEV
3012
No. 12 HORMONE RECEPTORS IN BREAST CANCER - Levine et al. 3013
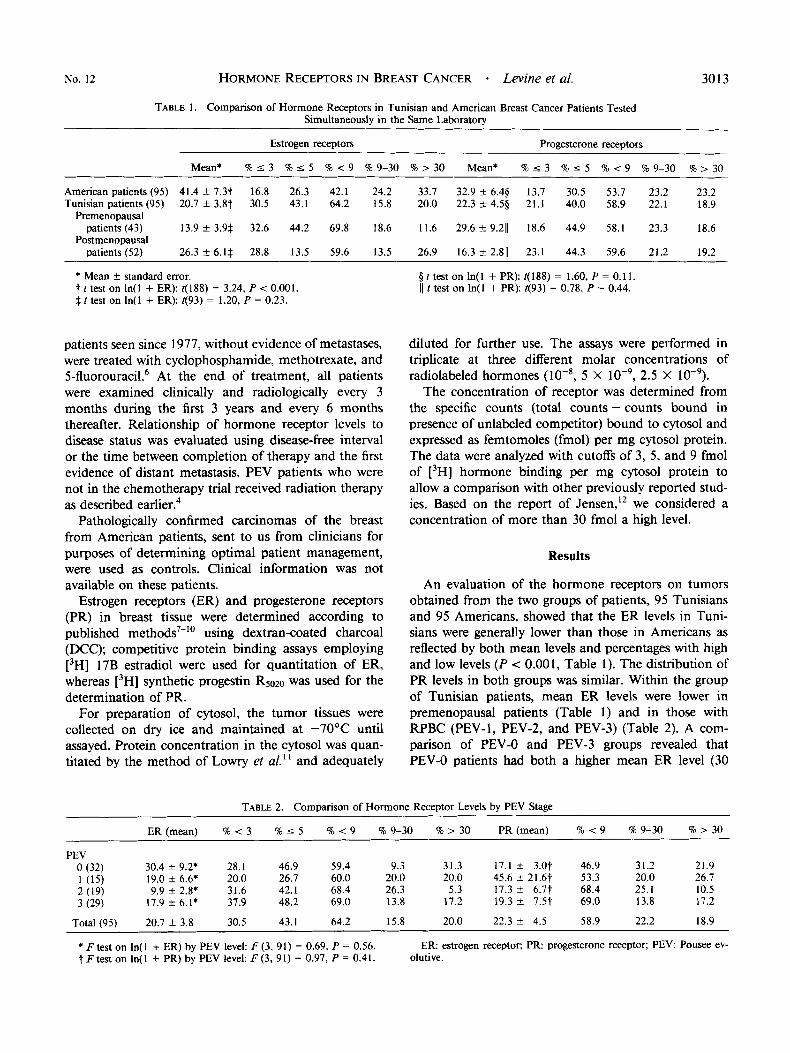
TABLE 1. Comparison of Hormone Receptors in Tunisian and American Breast Cancer Patients Tested Simultaneously in the Same Laboratory
Estrogen receptors Progesterone receptors
Mean* % 5 3 %I 5 % < 9 % 9-30 % > 30 Mean* % 5 3 90 I 5 % < 9 % 9-30 % > 30
American patients (95) 41.4 f 7.3t 16.8 26.3 42.1 24.2 33.7 32.9 ? 6.49 13.7 30.5 53.7 23.2 23.2 Tunisian patients (95) 20.7 f 3.8t 30.5 43.1 64.2 15.8 20.0 22.3 k 4.59 21.1 40.0 58.9 22.1 18.9
patients (43) 13.9 f 3.94 32.6 44.2 69.8 18.6 11.6 29.6 k 9.211 18.6 44.9 58.1 23.3 18.6
patients (52) 26.3 f 6.14 28.8 13.5 59.6 13.5 26.9 16.3 k 2.811 23.1 44.3 59.6 21.2 19.2
Premenopausal
Postmenopausal
* Mean f standard error. t t test on ln(l + ER): t(188) = 3.24, P < 0.001. 4 t test on In( 1 + ER): t(93) = 1.20, P = 0.23.
patients seen since 1977, without evidence of metastases, were treated with cyclophosphamide, methotrexate, and 5-fluor0uracil.~ At the end of treatment, all patients were examined clinically and radiologically every 3 months during the first 3 years and every 6 months thereafter. Relationship of hormone receptor levels to disease status was evaluated using disease-free interval or the time between completion of therapy and the first evidence of distant metastasis. PEV patients who were not in the chemotherapy trial received radiation therapy as described earlier.4
Pathologically confirmed carcinomas of the breast from American patients, sent to us from clinicians for purposes of determining optimal patient management, were used as controls. Clinical information was not available on these patients.
Estrogen receptors (ER) and progesterone receptors (PR) in breast tissue were determined according to published methods7-" using dextran-coated charcoal (DCC); competitive protein binding assays employing [3H] 17B estradiol were used for quantitation of ER, whereas [3H] synthetic progestin Rsozo was used for the determination of PR.
For preparation of cytosol, the tumor tissues were collected on dry ice and maintained at -70°C until assayed. Protein concentration in the cytosol was quan- titated by the method of Lowry et al." and adequately
gttestonln(1 +PR):t(188)= 1.60,P=0.11. (1 t test on In( 1 + PR): t(93) = 0.78, P = 0.44.
diluted for further use. The assays were performed in triplicate at three different molar concentrations of radiolabeled hormones 5 X lo-', 2.5 X lo-').
The concentration of receptor was determined from the specific counts (total counts - counts bound in presence of unlabeled competitor) bound to cytosol and expressed as femtomoles (fmol) per mg cytosol protein. The data were analyzed with cutoffs of 3, 5 , and 9 fmol of [3H] hormone binding per mg cytosol protein to allow a comparison with other previously reported stud- ies. Based on the report of Jensen," we considered a concentration of more than 30 fmol a high level.
Results
An evaluation of the hormone receptors on tumors obtained from the two groups of patients, 95 Tunisians and 95 Americans, showed that the ER levels in Tuni- sians were generally lower than those in Americans as reflected by both mean levels and percentages with high and low levels (P -= 0.001, Table 1). The distribution of PR levels in both groups was similar. Within the group of Tunisian patients, mean ER levels were lower in premenopausal patients (Table 1) and in those with RPBC (PEV-1, PEV-2, and PEV-3) (Table 2). A com- parison of PEV-0 and PEV-3 groups revealed that PEV-0 patients had both a higher mean ER level (30
TABLE 2. Comparison of Hormone Receptor Levels by PEV Stage
ER (mean) % < 3 %I 5 % < 9 % 9-30 I > 30 PR (mean) % < 9 % 9-30 % > 30
PEV 30.4 f 9.2; 28.1 46.9 59.4 9.3 31.3 17.1 f 3.0t 46.9 31.2 21.9 19.0 f 6.6; 20.0 26.7 60.0 20.0 20.0 45.6 f 21.6t 53.3 20.0 26.7 9.9 f 2.8; 31.6 42.1 68.4 26.3 5.3 17.3 f 6.7t 68.4 25.1 10.5
1 ( 1 5 )
3 (29) 17.9 f 6.1; 37.9 48.2 69.0 13.8 17.2 19.3 f 7.5t 69.0 13.8 17.2 2 (19)
Total (95) 20.7 f 3.8 30.5 43. I 64.2 15.8 20.0 22.3 f 4.5 58.9 22.2 18.9
o (32)
* F test on In( 1 + ER) by PEV level: F (3, 91) = 0.69, P = 0.56. t F test on In( 1 + PR) by PEV level F (3, 9 I ) = 0.97, P = 0.41.
ER: estrogen receptor; P R progesterone receptor; PEV: Pousee ev- olutive.
3014 CANCER December 15 1984 VOl. 54
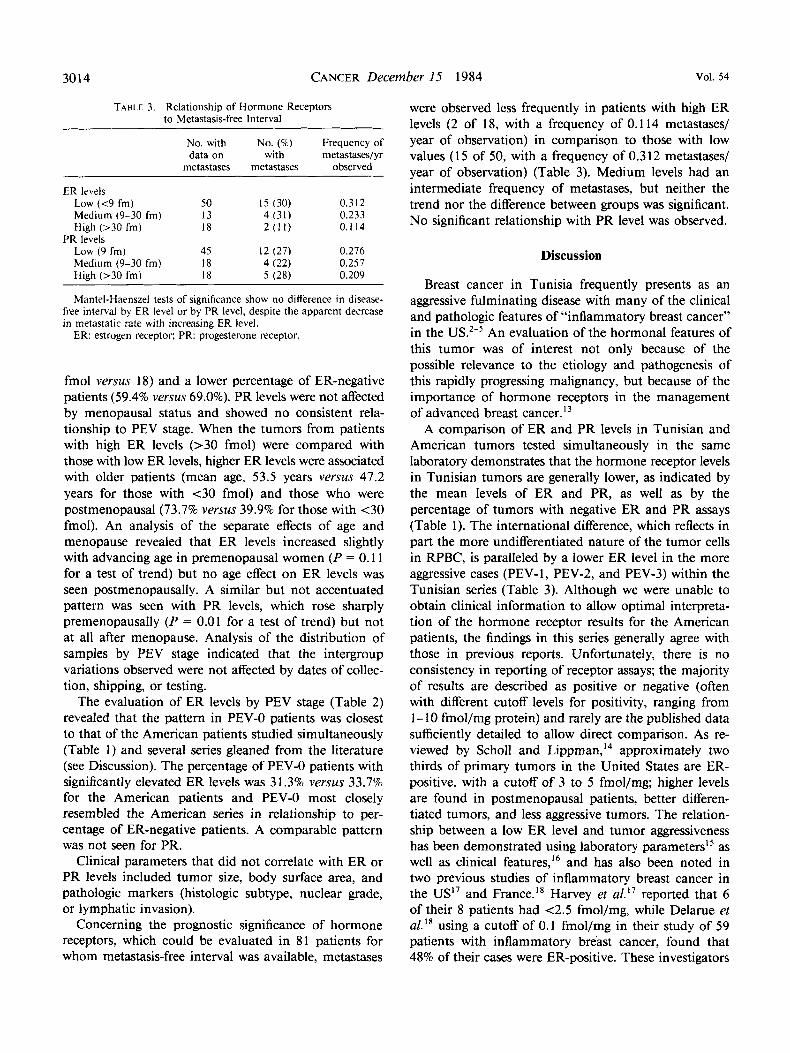
TABLE 3. Relationship of Hormone Receptors to Metastasis-free Interval
No. with No. (%) Frequency of data on with metastases/yr
metastases metastases observed
ER levels Low (<9 fm) 50 15 (30) 0.312 Medium (9-30 fm) 13 4 (31) 0.233 High (>30 fm) 18 2(11) 0.114
Low (9 fm) 45 12 (27) 0.276 Medium (9-30 fm) 18 4 (22) 0.257 High (>30 frn) 18 5 (28) 0.209
PR levels
Mantel-Haenszel tests of significance show no difference in disease- free interval by ER level or by PR level, despite the apparent decrease in metastatic rate with increasing ER level.
ER: estrogen receptor: PR: progesterone receptor.
fmol versus 18) and a lower percentage of ER-negative patients (59.4% versus 69.0%). PR levels were not affected by menopausal status and showed no consistent rela- tionship to PEV stage. When the tumors from patients with high ER levels (>30 fmol) were compared with those with low ER levels, higher ER levels were associated with older patients (mean age, 53.5 years versus 47.2 years for those with <30 fmol) and those who were postmenopausal (73.7% versus 39.9% for those with <30 fmol). An analysis of the separate effects of age and menopause revealed that ER levels increased slightly with advancing age in premenopausal women ( P = 0.1 1 for a test of trend) but no age effect on ER levels was seen postmenopausally. A similar but not accentuated pattern was seen with PR levels, which rose sharply premenopausally ( P = 0.01 for a test of trend) but not at all after menopause. Analysis of the distribution of samples by PEV stage indicated that the intergroup variations observed were not affected by dates of collec- tion, shipping, or testing.
The evaluation of ER levels by PEV stage (Table 2) revealed that the pattern in PEV-0 patients was closest to that of the American patients studied simultaneously (Table 1) and several series gleaned from the literature (see Discussion). The percentage of PEV-0 patients with significantly elevated ER levels was 3 1.3% versus 33.7% for the American patients and PEV-0 most closely resembled the American series in relationship to per- centage of ER-negative patients. A comparable pattern was not seen for PR.
Clinical parameters that did not correlate with ER or PR levels included tumor size, body surface area, and pathologic markers (histologic subtype, nuclear grade, or lymphatic invasion).
Concerning the prognostic significance of hormone receptors, which could be evaluated in 81 patients for whom metastasis-free interval was available, metastases
were observed less frequently in patients with high ER levels (2 of 18, with a frequency of 0.1 14 metastases/ year of observation) in comparison to those with low values (15 of 50, with a frequency of 0.312 metastases/ year of observation) (Table 3). Medium levels had an intermediate frequency of metastases, but neither the trend nor the difference between groups was significant. No significant relationship with PR level was observed.
Discussion
Breast cancer in Tunisia frequently presents as an aggressive fulminating disease with many of the clinical and pathologic features of “inflammatory breast cancer” in the An evaluation of the hormonal features of this tumor was of interest not only because of the possible relevance to the etiology and pathogenesis of this rapidly progressing malignancy, but because of the importance of hormone receptors in the management of advanced breast cancer. l 3
A comparison of ER and PR levels in Tunisian and American tumors tested simultaneously in the same laboratory demonstrates that the hormone receptor levels in Tunisian tumors are generally lower, as indicated by the mean levels of ER and PR, as well as by the percentage of tumors with negative ER and PR assays (Table 1). The international difference, which reflects in part the more undifferentiated nature of the tumor cells in RPBC, is paralleled by a lower ER level in the more aggressive cases (PEV-1, PEV-2, and PEV-3) within the Tunisian series (Table 3). Although we were unable to obtain clinical information to allow optimal interpreta- tion of the hormone receptor results for the American patients, the findings in this series generally agree with those in previous reports. Unfortunately, there is no consistency in reporting of receptor assays; the majority of results are described as positive or negative (often with different cutoff levels for positivity, ranging from 1-10 fmol/mg protein) and rarely are the published data sufficiently detailed to allow direct comparison. As re- viewed by Scholl and Lippman,I4 approximately two thirds of primary tumors in the United States are ER- positive, with a cutoff of 3 to 5 fmol/mg; higher levels are found in postmenopausal patients, better differen- tiated tumors, and less aggressive tumors. The relation- ship between a low ER level and tumor aggressiveness has been demonstrated using laboratory parametersi5 as well as clinical features,I6 and has also been noted in two previous studies of inflammatory breast cancer in the US” and France.I8 Harvey er a1.I’ reported that 6 of their 8 patients had <2.5 fmol/mg, while Delarue et
using a cutoff of 0.1 fmol/mg in their study of 59 patients with inflammatory breast cancer, found that 48% of their cases were ER-positive. These investigators

No. 12 HORMONE RECEPTORS IN BREAST CANCER Levine et al. 3015
noted a better response to therapy in the ER-positive patients with inflammatory breast cancer than the ER- negative patients, but did not report specific receptor values or means.
Of great importance to the understanding of the pathogenesis of RPBC is our observation that PEV-1 patients have lower ER levels than PEV-0 patients, thus providing further evidence that PEV- 1, which has no clinical signs of inflammation and is based on the patient’s report of rapid tumor growth, is a biologic entity closely related to IBC. Our previous ~ t u d i e s ~ - ~ suggesting the importance of the history of rapid growth in the pathogenesis and treatment of breast cancer received support from a pathologic evaluation of 94 biopsy specimens from Tunisian cancer patients, which demonstrated that poor nuclear grade was significantly more common in PEV-1, PEV-2, and PEV-3 patients than in PEV-0.5 Although RPBC without inflammation is recognized in the Institut Gustav Roussy, where it was initially described by Denoix,’ this group was not included in the French study.
Although low ER levels were generally found in young, premenopausal, and PEV-3 patients, interrelated features that could not be readily isolated, a multivariate analysis suggested that age was the most important correlating factor. As in most other series, we also found a correlation between ER level and response to treatment, which was standardized to the extent that all PEV-0 patients received radical mastectomy and all PEV-posi- tive patients were entered into a therapeutic trial with cyclophosphamide, methotrexate, and 5-fluorouracil ac- cording to a standard protocol, with premenopausal patients receiving oopherectomy.6 A trend relating the ER levels to disease-free interval was observed. A lower incidence of metastases (2 of 18 patients, 0.1 14 metas- tases/year of exposure) was seen in those with high ER levels, an intermediate incidence (4 of 13, 0.233 metas- tases/year) was seen in those with medium ER levels, and the highest recurrence rate (15 of 50, 0.312 metas- tases/year) was observed in those having the lowest ER levels. However, these differences were not significant (P = 0.27 by Mantel-Haenszel test).
Rapidly growing malignancies of the breast have been observed to have pathologic markers of their growth rate and a very unfavorable o ~ t c o m e . ~ ~ ~ ” ~ Such rapidly proliferating tumors are known to undergo dedifferen- tiation and become independent of any control measures. Hence, one would expect lack of hormone receptors in those tumors, as was reported by Meyer et aL2’ Our finding of low receptors in PEV and in more advanced tumors is in accordance with these earlier findings.
In a previous comm~nication,~ we observed that risk factors were different for pre- and postmenopausal women. Premenopausal women, particularly during
pregnancy or lactation, were at the greatest risk of developing RPBC (1 8 of 19 women with breast cancer during this period had PEV tumors), whereas for post- menopausal women late menarche was associated with RPBC. This hormone receptor study, which indicated that younger premenopausal women are more often receptor-negative than older postmenopausal women, is in agreement with the findings of other investiga- t o r ~ . ’ ~ , ’ ~ , ~ ’ The low ER receptor levels in young women observed in these studies cannot be interpreted as show- ing the lack of relationship between hormones and RPBC, however. The assay we used measures only the unbound receptor protein, and since it is possible that high levels of endogenous estrogen could be binding receptors in young patients with RPBC, the evaluation of the hormone influence requires the use of an assay measuring total (bound and unbound) receptor levels, such as the hydroxylapatite ejlchange assay.22
There are conflicting reports in the literature on the usefulness of receptor analysis as a prognostic tool, with some investigators considering it a useful prognostic marker23124 and others noting no significant ~orrelation.~~ This study on 95 patients demonstrates that patients with receptor-positive tumors responded better to treat- ment than those with receptor-negative tumors.
Our comparison of 95 American cases with our Tunisian series showed a similarity of ER pattern between the American patients and Tunisian PEV-0 patients rather than with the PEV-1, PEV-2, and PEV-3 stages. Clinically, the response to therapy in PEV-0 is compa- rable to that in American tumors, but in other ways, particularly in immune response, there are great differ- ences.26
Younger age, pregnancy, and lack of receptors with progression of disease clearly support the importance of understanding hormonal influence in the pathogenesis of the disease. The apparent value of hormone receptors in guiding therapy and the wide variation in receptor levels among breast cancer patients emphasize the im- portance of individualization of treatment for patients with RPBC. The routine use of oophorectomy in the management of RPBC is a particular practice that now requires reevaluation.
REFERENCES
1. Denoix P. Treatment of malignant breast tumors. In: Allfrey VG, ed. Recent Results in Cancer Research, vol. 31. Berlin: Springer/ Verlag, 1970; 92.
2. Mourali N, Tabbane F, Djazizi M, Cammoun M, Belhassen S. Fulminating breast cancer: Clinical features. In: Nieburgs HE, ed. Prevention and Detection of Cancer, Part 1 , vol. 1. New York: Marcel Dekker, 1977; 545-554.
3. Tabbane F, Muenz LR, Jaziri M, Cammoun M, Belhassen S, Mourali N. Clinical and prognostic features of a rapidly progressing breast cancer in Tunisia. Cancer 1977; 40376-382.
4. Mourali N, Muenz LR, Tabbane F, Belhassen S, Bahi J, Levine
3016 CANCER December 15 1984 VOl. 54
PH. Epidemiologic features of rapidly progressing breast cancer in Tunisia. Cancer 1980; 46:274 1-2746.
5 . Costa J, Webber BL, Levine PH et al. Histopathological features of rapidly progressing breast carcinoma in Tunisia: A study of 94 cases. Int J Cancer 1982; 30:35-37.
6. Mourali N, Tabbane F, Muenz LR ef a/. Preliminary results of primary systemic chemotherapy with cyclophosphamide, methotrexate and 5-fluorouracil (CMF) in association with local/regional treatment in rapidly progressing breast cancer. Er J Cancer 1982; 45:367-370.
7. Horwitz KB, McGuire WL. Progesterone and progesterone recep- tors in experimental breast cancer. Cancer Res 1977; 37:1733-1738.
8. Korenman SG, Dukes BA. Specific estrogen binding by the cytoplasm of human breast carcinoma. J Clin Endocrinol 1970;
9. McGuire WL, De La Garza M. Improved sensitivity of the measurement of estrogen receptor in human breast cancer. J Clin Endocrinol Metab 1973; 37:986-989.
10. McGuire WL, Horowitz KB, Pearson OH, Segaloff A. Current status of estrogen and progesterone receptors in breast cancer. Cancer
11. Lowry OH, Rosenbrough NJ, Farr AL, Randall RJ. Protein measurement with Fohn reagent. J Biol Chem 1961; 193:265-275.
12. Jensen EV. Estrogen receptors in hormone-dependent breast cancer. Cancer Res 1975; 35:3362-3364.
13. McCuire WL. Horwitz KB, Zava DT, Garola RE, Chamness GC. Hormones in breast cancer: Update 1978. Melabo/rsm 1978;
14. Scholl SM. Lippman ME. Methods and clinical use of receptor assay. In: Bonnadonna G, ed. Breast Cancer: Diagnosis and Manage- ment. England: John Wiley and Sons, 1984; 75-107.
15. Meyer JS, Rao BR, Stevens SC, White WL. Low incidence of estrogen receptor in breast carcinomas with rapid rates of cellular replication. Cancer 1977; 40:2290-2298.
16. Antoniades K, Spector H. Quantitative estrogen receptor values
30~639-645.
1977; 39:2934-2947.
27:487-50 I .
and growth of carcinoma of the breast before surgical intervention. Cancer 1982; 50793-796.
17. Harvey HA, Lipton A, Lusch CJ et a/. Estrogen receptor status in inflammatory breast carcinoma. Proc Am Soc Clin Oncol 1979; 20:43 1.
18. Delarue JC, May-Levin F, Mouriesse H, Contesso G, Sancho- Gamier H. Estrogen and progesterone cytosolic receptors in clinically inflammatory tumors of the human breast. Br J Cancer 198 1; 44:9 I 1- 916.
19. Boyd NF, Meakin JW, Hayward JL, Brown TC. Clinical esti- mation of the growth rate of breast cancer. Cancer 1981; 48:1037- 1042.
20. Meyer JS, Rao BR, Stevens SC, White WL. Low incidence of estrogen receptor in breast carcinomas with rapid rates of cellular replication. Cancer 1977; 40:2290-2298.
21. Knight WA, Livingston RB, Gregory U, McGuire WL. Estrogen receptor as an independent prognostic factor for early recurrence in breast cancer. Cancer Res 1977; 37:4669-4671.
22. Garola RE, McGuire WL. An improved assay for nuclear estrogen receptor in experimental and human breast cancer. Cancer Res 1977; 37:3333-3337.
23. Bloom ND, Tobin EH, Schreibman B. Degenshein GA. The role of progesterone receptors in the management of advanced breast cancer. Cuncer 1980: 4512992-2997.
24. Cooke T, George D, Shields R, Maynard P, Griffiths K. estrogen receptors and prognosis in early breast cancer. Lancet 1979; 1:995- 997.
25. Hilf R, Feldstein ML, Gibson SL, Savlov ED. The relative importance of estrogen receptor analysis as a prognostic factor for recurrence or response to chemotherapy in women with breast cancer. Cancer 1980 45:1993-2000.
26. Levine PH, Mourali N, Tabbane F ef al. Studies on the role of cellular immunity and genetics in the etiology of rapidly progressing breast cancer in Tunisia. Int J Cancer 198 1; 27:6 1 1-6 15.