Embed Size (px)
Citation preview
HOSPICE COMPLIANCE/REGULATORYREQUIREMENTS, WITH MEDICARE
REIMBURSEMENT CHANGES
2009 - 2016
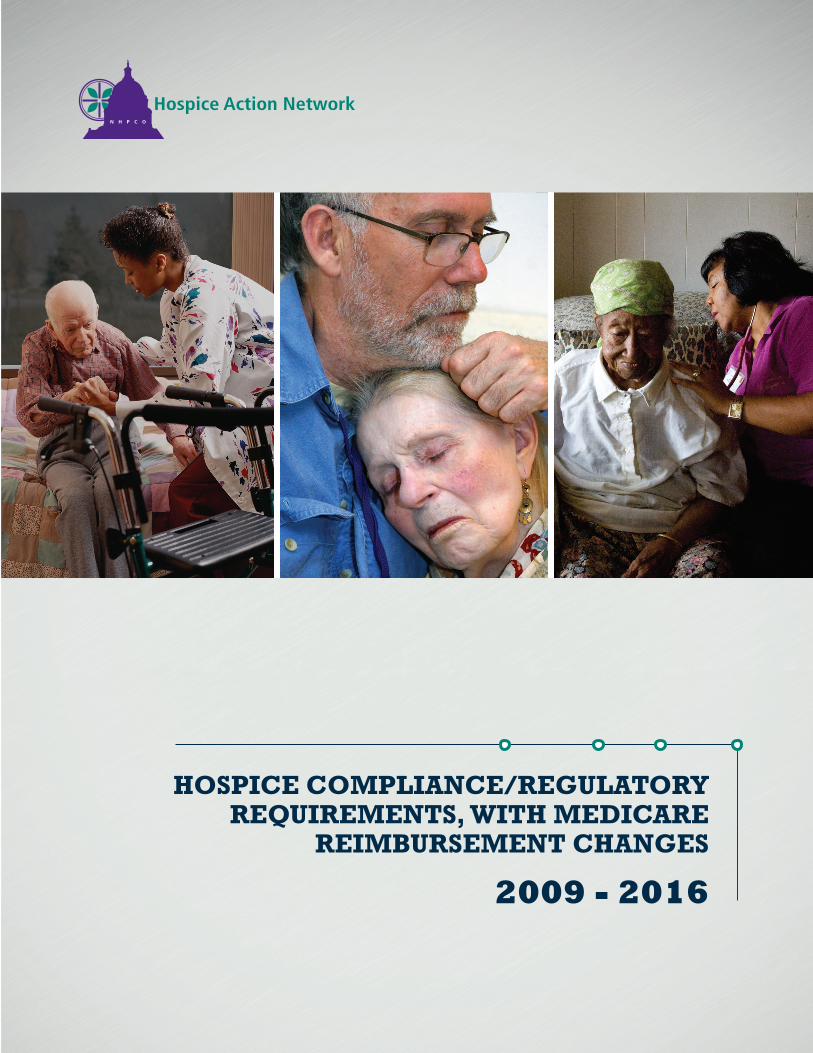
Budget Neutrality Adjustment Factor (BNAF) October 1, 2009A 1997 change in the calculation of the hospice wage index results in stabilizing hospice payments. The BNAF, implemented to ease hospices’ transition to a new payment methodology, phases out from 2009 through 2016 resulting in an estimated 4.2 percent reduction in reimbursement.
Brief Physician Narrative October 1, 2009CMS requires hospice physicians to compose a brief narrative explanation of the clinical findings that support a life expectancy of six months or less as part of or addendum to the certification and recertification forms.
CR6440: Reporting Visit Intensity on Claim Form January 1, 2010CMS requires hospices to record the length of nurse, social worker, and hospice aide visits in 15-minute increments. CR6440 adds physical therapists, occupational therapists, and speech language pathologists to this requirement.
Concurrent Care for Children March 23, 2010Section 2302 of the Patient Protection and Affordable Care Act (ACA) requires states to allow children enrolled in Medicaid or CHIP programs, and who are eligible for hospice services, to receive hospice services without foregoing curative treatment.
CR7337: Face-to-Face Encounter January 1, 2011; delayed until April 1, 2011CMS requires that a hospice physician or hospice nurse practitioner have a face-to-face encounter with each hospice patient before the patient’s third benefit period (after 180 days of care) and before each subsequent benefit period. The patient loses Medicare hospice eligibility if the face-to-face encounter requirements are not met.
CR7473: Report Revocations as Separate Code on Claim Form July 1, 2012For CMS tracking, hospices must differentiate patient-initiated revocation and hospice-initiated discharges on claim forms.
ACA Productivity Adjustment October 1, 2012The ACA imposes a “productivity adjustment” on the calculation of annual payment updates for hospice. In FY 2013, Medicare providers experience a productivity adjustment of -0.7 percent. Hospices receive an additional -0.3 percent productivity adjustment, for a total payment reduction of 1.0 percent. The productivity adjustment will cut hospice payments by approximately 11.8 percent over ten years.
Quality Reporting for Hospice Programs October 1, 2012CMS requires hospices to report on two measures: a structural measure on patient-focused performance improvement projects, and a pain score that measures pain on admission and pain after 48 hours.
Sequestration January 2013All Medicare providers, including hospice, experience a non-compounding two percent reduction in payments each year through 2024.
Long Term Care Facilities: Hospice Services Final Rule August 23, 2013 Long‐term care facilities (nursing facilities and skilled nursing facilities) arrange for hospice care through an agreement with one or more Medicare‐certified hospice providers. CMS requires SNFs, NFs, and hospices to maintain written agreements specifying the roles and responsibilities of each party.
ACA Productivity Adjustment October 1, 2013In FY2014, Medicare providers receive a productivity adjustment of -0.5 percent. Hospices experienced a hospice-specific productivity adjustment of -0.3 percent, for a total payment reduction of 0.8 percent.
CR8371: Demand Billing of Hospice General In patient Level of Care January 6, 2014 CMS requires hospice providers to issue an advance beneficiary notice (ABN) notifying beneficiaries that general inpatient (GIP) will not be covered by Medicare if the hospice determines that GIP care is not medically necessary.
CR8358: Additional Data Collection on Claim Form April 1, 2014CMS requires hospices to collect the following information: • GIP visits by hospice staff in a contract facility; • inpatient facility national provider identifiers (NPIs); • post-mortem visits; and• prescription drugs (injectable and non-injectable) by fill and charges,infusion pumps, and cassettes.
Hospice Item Set (HIS) July 1, 2014CMS requires data collection for seven new quality measures through a patient-level data-collection tool developed by CMS. The hospice item set (HIS) includes two parts: HIS-Admission and HIS-Discharge. CMS collects the data from hospice records and uses the data to calculate six National Quality Forum (NQF) approved measures and one modified NQF measure.
CMS Revised Guidance on Hospice and Part D July 18, 2014CMS issues revised guidance regarding the prior authorization (PA) requirement for medications unrelated to the terminal illness and submitted for payment under a patient’s Part D plan. The PA now applies ONLY to four classes of drugs: analgesics, anti-emetics, laxatives, and anti-anxiety medications. The hospice remains responsible for all medications related to the terminal prognosis, whether or not they are included in the four classes.
The HIPAA Omnibus Rule September 22, 2014CMS requires all healthcare providers, including hospices, to review and revise business associate agreements, revise HIPAA policies and procedures to address possible breaches of unsecured protected health information, update notices of privacy practice, and train employees on updated obligations.
Hospice Self-Reporting the Aggregate Cap March 31, 2015CMS requires hospices to complete and self-report their aggregate cap determination within 5 months after the cap year ends. If a provider fails to file the cap report with the Medicare contractor, payments to theprovider are suspended until the cap report is filed.
Hospice Consumer Assessment of Healthcare Providers and Systems (CAHPS®) Survey Mandatory Implementation April 1, 2015CMS implements Hospice CAHPS, a post-death family caregiver survey designed to assess patient and family experiences with hospice care. Survey vendors administer Hospice CAHPS on behalf of hospices.
Hospice Survey Requirement April 6, 2015Medicare certified hospices are subject to mandatory surveys every 36 months, through 2025. CMS contracts with organizations in each state. Surveys may also be performed by accrediting agencies with deemed status, such as The Joint Commission, the Community Health Accreditation Partner (CHAP), and the Accreditation Commission for Health Care (ACHC).
Penalty for Non-Participation in Quality Reporting in FY2014 October 1, 2015Hospices that fail to participate in FY2014 Quality Reporting receive a two percent FY2016 market basket reduction.
ACA Productivity Adjustment October 1, 2015Hospices receive a -0.3 percent productivity adjustment on top of the productivity adjustment applied to all Medicare providers.
ICD – 10 Implementation October 1, 2015ICD-10 code sets replace the ICD-9-CM code sets used by medical coders and billers to report health care diagnoses and procedures.
Implementation of 2010 Census CBSA or State Designations October 1, 2015FY2016 wage index rates reflect changes in urban and rural areas based on the 2010 census. For FY2016 only, a blended wage index value is used: 50 percent of the prior CBSA/rural designation and 50 percent of the new designation. In FY2017, all wage index values are calculated based on the current designation.
Reporting All Diagnoses on the Claim Form October 1, 2015Hospices must report all diagnoses identified in the initial and comprehensive assessments on the hospice claim, whether related or unrelated to the terminal prognosis. The list of diagnoses includes any mental health disorders or conditions that affect the plan of care. Hospices do not identify which diagnoses they have determined to be related versus unrelated.
2009
2009-2016
2010 2011 2012 2013 2014
Penalties for Failure to Participate in FY2013 Quality Reporting October 1, 2014Hospices that do not submit quality reporting data receive a two percent hospital market basket reduction for payment year FY2015.
Claims Returned to Provider (RTP) October 1, 2014 CMS disallows claims that use a manifestation code as a primary diagnosis (including debility and adult failure to thrive). Claims with these codes are no longer paid. These codes may be used as a secondary/other diagnosis.
Hospice Cost Report October 1, 2014 CMS implements a new cost report for free-standing hospice providers for reporting periods beginning October 1, 2014, or later. Hospice providers must change their charts of accounts to collect additional data to accurately complete the new cost report.
Filing of Notice of Election (NOE) and Notice of Termination/Revocation (NOTR) October 1, 2014CMS requires hospices to submit the NOE and/or NOTR, and have the form(s) accepted by their Medicare contractor, within five days of a patient’s hospice election or revocation. If a hospice is late filing the NOE, the hospice remains responsible for all care and services detailed in the plan of care but will not be reimbursed until the NOE is submitted and accepted. Further, Medicare will not retroactively pay the hospice for days of care provided before the contractor accepts the NOE.
Patient Designation of Attending Physician October 1, 2014CMS requires the name of each patient’s attending physician to appear on the NOE, along with an acknowledgement that the identified physician is the patient’s choice. To change the attending physician, the patient or legal representative must provide the hospice with a signed document designating a new attending physician. CMS intends that this new requirement will act as a safeguard and preserve the patient’s choice of attending physician.
ACA Productivity Adjustment October 1, 2014Medicare providers received a productivity adjustment of -0.4 percent. Hospices experience an additional hospice-specific productivity adjustment of -0.3 percent, for a total payment reduction of 0.7 percent.
2015
Hospice Payment Reform Section 3132 of the ACA directs the Secretary of HHS to revise the hospice payment methodology no sooner than October 1, 2013. Revisions should result in the same estimated amount of aggregate expenditures for hospice care as if the revisions were not implemented.
• Two-Tiered Routine Home Care Rate (January 1, 2016) CMS introduces a two-tiered routine home care rate (RHC). Hospices receive a higher rate for the first 60 days of a patient’s care, and a lower rate for days 61 and after. This change also applies to state Medicaid fee-for-service hospice benefits.
• Service Intensity Add-On (January 1, 2016) CMS develops the service intensity add-on (SIA) payment for visits conducted by an RN and/or social worker up to 4 hours a day (combined) during the last 7 days of a hospice patient’s life. The patient must be receiving routine home care, and the RN and/or social worker provide direct patient care. The SIA payment equals the continuous home care hourly rate, and is disbursed in addition to the RHC rate for the dates of the RN and social worker visits.
• Service Intensity Budget Neutrality Factor (January 1, 2016) RHC rates are adjusted by budget neutrality factors to account for spending on the SIA payment. The first budget adjustment factor applies to days one through 60 of a patient’s care. A separate factor affects payments for days 61 and beyond. SIA utilization determines the exact adjustment factors.
ACA Productivity Adjustment (October 1, 2016)In FY2017, hospices will continue to receive a -0.3 percent productivity adjustment in addition to the productivity adjustment applied to all Medicare providers.
Update to Hospice Aggregate Cap (October 1, 2016)The IMPACT Act realigns the inflation adjustment of the hospice aggregate cap so that it is based on the same increase as hospice rates, the hospital marketbasket. In addition, the cap year changes to align with the fiscal year of October 1, beginning in 2016. with hospice reimbursement for ten years (through cap year ending September 30, 2025).
Medical Review (Pending)The ACA incorporates a 2009 recommendation of the Medicare Payment Advisory Commission (MedPAC) that hospice programs with a high percentage of patients qualifying as long lengths of service (more than 180 days) receive oversight through focused medical review. This provision is now ready for CMS to set the threshold, or percentage, which will trigger medical review.
2016
As of July 1, 2016

91%
Of Hospice Patients Rely on Medicare/Medicaid Reimbursements
Hospices are facing a perfect storm -
- multiple Medicare reimbursement reductions, a series of costly regulatory changes, and hospice payment reform.
With the confluence of reimbursement cuts, increased regulatory and administrative burdens, and the prospect of significant additional changes to the Medicare Hospice Benefit in the near future, the health of the hospice community, and access to it, is in danger.
Hospice care relies more heavily on Medicare and Medicaid reimbursements(91% of patients) than other types of providers. This poses a challenge for hospice providers, allowing little room for shifting costs in response to the financial, administrative, and regulatory challenges.
According to recent MedPAC data...the projected hospice margin for 2016 is 7.7%. Once other mandatory butnon-reimbursable costs are included (bereavement services and volunteerprograms), the aggregate margin drops to 6.0%.
7.7% - Projected 2016 Hospice Margin
6.0% - Hospice Margin After Non-reimbursable Costs
Hospice Action Network and National Hospice and Palliative Care Organization
1731 King Street, Alexandria, VA 22314www.hospiceactionnetwork.org x www.nhpco.org
Tel: 703-837-1500 x Fax: 703-837-1233