Embed Size (px)
Citation preview

Aging Clin Exp Res 19: 69-74, 2007©2007, Editrice Kurtis
Key words: Age, elderly, critically ill, geriatric, mortality, prognosis.Correspondence: A.Topeli, MD, Department of Internal Medicine, Hacettepe University Faculty of Medicine, Sihhiye, 06100, Ankara, Turkey.E-mail: [email protected] March 11, 2005: accepted in revised form January 17, 2006.
Aging Clin Exp Res, Vol. 19, No. 1 69
ABSTRACT. Background and aims: It is not well-known whether age or the severity of underlying con-ditions affects mortality in critically ill patients. Theaim of this study was therefore to determine whetherage is an independent predictor of hospital survival forcritically ill patients. Methods: Patients consecutivelyadmitted to the intensive care unit from December 11999 to July 31 2001 were included in the study.Patients were stratified into 3 groups (≤65 years old,66-75 years old, >75 years old) and were compared, byboth bivariate and multivariate analyses, to ascertainwhether older critically ill patients had poorer hospitalsurvival than younger patients. Results: Of 331 pa-tients, 178 (53.8%) patients were ≤65 years old, 100(30.2%) were 66-75 years old, and 53 (16%) were>75 years old. Multivariate logistic regression analysisrevealed that older age, presence of fatal comorbidities,mechanical ventilation, central venous catheteriza-tion, and higher acute physiology and chronic healthevaluation score II (excluding the score obtained fromage) were independent predictors of hospital mortali-ty in the study population. Kaplan-Meier survival anal-ysis revealed that patients ≤65 years old had better hos-pital survival than older patients (p=0.02). Conclu-sions: Older critically ill patients have poorer hospitalsurvival than patients ≤65 years old, when other con-founding factors such as disease severity score, invasiveprocedures and comorbidities were controlled for. (Aging Clin Exp Res 2006; 18: 69-74)©2006, Editrice Kurtis
INTRODUCTIONThe number of older people in the population is in-
creasing worldwide, imposing a major share of health-care expenditure. Intensive care of older patients isof particular concern. Acute deterioration of the healthstatus in older patients puts healthcare providers, es-pecially those working in intensive care, in a difficult sit-
Hospital survival of older patients admitted to amedical intensive care unitArzu Topeli1 and Banu Cakir2
1Medical Intensive Care Unit, Department of Internal Medicine, Hacettepe University Faculty of Medicine, Ankara,2Department of Public Health, Hacettepe University Faculty of Medicine, Ankara, Turkey
uation, in which they find themselves in a position ofdecision-making (1). In fact, in one study in whichphysicians were given hypothetical case scenarios andwere asked to decide whether to admit a patient, agewas found to be a factor considered for admission to theintensive care unit (2).
Several studies have investigated whether the follow-upof older patients in intensive care units (ICU) is cost-ef-fective and worth the effort (3-23). However, they wereconducted in populations with high income, and furtherinformation about the outcome of older patients in de-veloping countries is required to develop appropriatehealthcare policies for older people. In Turkey, olderpeople in the population are also increasing. The pro-portion of individuals above 65 years in the total popu-lation rose from 4.6% in the 1980s to 6.3% in 2002 (24).In addition, lack of regulations about approaches to ter-minally ill patients and scarcity of nursing facilities lead toa shortage of ICU beds relative to demand, and alsoraise well-founded concern about whether older patientsreally do benefit from ICU care. Therefore, a prospectivecohort study was conducted in a medical intensive careunit (MICU) to study whether age is an independent pre-dictor of hospital survival in critically ill older patients.
METHODSThe study was performed in the MICU of a university
hospital (Hacettepe University Faculty of Medicine,Ankara, Turkey). Data were prospectively collected for allpatients who were consecutively admitted to the MICUfrom December 1 1999 through July 31 2001, andwho stayed in it for more than 24 hours. Only first ad-missions were included in the analysis. Patients werefollowed untill death or discharge from hospital.
The following information was collected for all pa-tients: age; gender; admission diagnosis (categorized aspulmonary, cardiac, sepsis, gastrointestinal, metabolicand renal, or neurologic conditions, or intoxication);
Aging Clinical and Experimental Research

post-operative status; underlying diseases (grouped ascardiovascular disease, pulmonary disease, malignancies,chronic liver failure, diabetes mellitus, chronic renal fail-ure, neurologic diseases, others, and none), applicationof invasive procedures (mechanical ventilation for >24hours, central venous catheterization, hemodialysis,tracheotomy); length of MICU stay; length of hospitalstay; MICU survival; and hospital survival. Underlyingdiseases were also categorized as absent/not fatal, ul-timately fatal (patients expected to die within 5 years)and rapidly fatal (patients expected to die within 1year), according to McCabe and Jackson’s comorbidi-ty classification system (25). For patients with more thanone underlying disease, the disease with the worstprognosis was used for classification. Acute physiologyand chronic health evaluation (APACHE II score) wascalculated using the worst parameters within the first 24hours of admission, and the “expected” mortality rate,based on the APACHE II score, was calculated ac-cordingly (26). This score consists of points obtained
from age, chronic health status, Glasgow coma scoreand 11 acute physiologic parameters (blood pressure,temperature, heart rate, respiratory rate, oxygenation,arterial blood pH, Na, K, white blood cell count, hema-tocrit, creatinine). After observed hospital mortalitywas obtained, the standardized mortality ratio (SMR),i.e., ratio of observed to expected mortality rate, wascalculated for all groups.
Statistical analysis was performed using the StatisticalPackage for Social Sciences (SPSS), Version 7.5. Analysesincluded frequency distributions, percentages and calcu-lation of means, and standard deviations (SD). Groupswere compared using the Chi-square test or Fisher’s ex-act test, and one-way ANOVA with Bonferroni’s post-hocanalysis or Student’s t-test for categorical, and continuousvariables, respectively. Comparison of survival probabil-ities of groups was performed using Kaplan-Meier curvesand the log-rank test. Logistic regression analysis was per-formed using variables which were found to significantlyinfluence mortality in bivariate analysis, to assess the
A. Topeli and B.Cakir
70 Aging Clin Exp Res, Vol. 19, No. 1
Aging Clin Exp Res 19: 69-74, 2007©2007, Editrice Kurtis
Table 1 - General characteristics of patients by age groupa.
Pts ≤65 years old Pts 66-75 years old Pts >75 years old p-valueb
n=178 n=100 n=53
Average age, years (min-max) 47.0±14.3 (15-65) 70.8±2.7 (66-75)* 81.5±5.1 (76-97)*† <0.001Male patients 91 (51.1) 47 (47.0) 31 (58.5) 0.40APACHE II score (min-max) 19.1±9.2 (2-50) 23.3±7.2 (7-46)* 24.6±7.5 (10-45)* <0.001Admission diagnosis
Pulmonary condition 57 (32.0) 40 (40.0) 19 (35.8) 0.41Cardiac condition 33 (18.5) 27 (27.0) 18 (34.0)* 0.04Sepsis 30 (16.9) 14 (14.0) 7 (13.2) 0.73Gastrointestinal condition 29 (16.3) 6 (6.0)* 3 (5.7) 0.01Metabolic condition 12 (6.7) 8 (8.0) 4 (7.5) 0.92Neurologic condition 11 (6.2) 4 (4.0) 2 (3.8) 0.65Intoxication 6 (3.4) 1 (1.0) 0 0.21
Post-operative admission 19 (10.7) 11 (11.0) 7 (13.2) 0.87Underlying diseases
Cardiovascular disease 34 (19.1) 50 (50.0)* 32 (60.4)* <0.001Pulmonary disease 33 (18.5) 31 (31.0) 13 (24.5) 0.06Malignancies 27 (15.2) 9 (9.0) 4 (7.5) 0.17Chronic liver failure 25 (14.0) 11 (11.0) 2 (3.8) 0.12Diabetes mellitus 22 (12.4) 15 (15.0) 7 (13.2) 0.82Chronic renal failure 22 (12.4) 16 (16.0) 4 (7.5) 0.32Neurologic disease 11 (6.2) 6 (6.0) 8 (15.1) 0.08Others 28 (15.7) 9 (9.0) 5 (9.4) 0.20None 19 (10.7) 4 (4.0) 3 (5.7) 0.11
ComorbiditiesNon-fatal/Absent 110 (61.8) 71 (71.0) 40 (75.5) 0.10Ultimately fatal 52 (29.2) 25 (25.0) 11 (20.8) 0.43Rapidly fatal 16 (9.0) 4 (4.0) 2 (3.8) 0.18
Invasive proceduresMechanical ventilation 103 (57.9) 75 (75.0)* 36 (67.9) 0.01Central venous catheter 79 (44.4) 54 (54.0) 29 (54.7) 0.20Hemodialysis 33 (18.5) 26 (26.0) 10 (18.9) 0.32Tracheotomy 6 (3.4) 8 (8.0) 8 (15.1)* <0.01
aMeans±standard deviations and numbers (percentages in brackets), are presented as appropriate. Percents do not total 100.0 for underlying diseases, as somepatients had multiple underlying diseases. bp-value for Chi-square or Fisher’s exact test, and one-way ANOVA with Bonferroni’s post-hoc analysis for categoricaland continuous variables, respectively. *p<0.05, compared with patients ≤65 years old. †p<0.05, patients aged 66-75 years old as reference group.APACHE: Acute physiology and chronic health evaluation.

significance of age group (≤65, 66-75 and >75 years ofage) as an independent predictor of hospital survival,and to determine other independent predictors of hospitalsurvival. Odds ratios (OR) and 95 % confidence intervals(CI) are also reported. The final model was reached usingthe backward elimination method, at the statistically sig-nificance level of alpha =0.05.
RESULTS The data obtained from 331 patients were analyzed.
There were 178 (53.8%) patients ≤65 years old, 100(30.2%) 66-75 years old, and 53 (16%) >75 years old.
Patients’ general characteristics by age are listed in Table1. The APACHE II scores of patients 66-75 years old and>75 years old were higher than those of patients ≤65years old (p<0.001). However, when the age factor wasexcluded, the APACHE II – age scores of patients ≤65years old, 66-75 years old and >75 years old were simi-lar (17.4±9.1, 18.2±7.2 and 18.6±7.5, respectively;p=0.57). Admission due to cardiac problems was morelikely in those >75 years old than in those ≤65 years old(p<0.05), whereas gastrointestinal problems were morefrequent as admission diagnosis in patients ≤65 years oldcompared to those 66-75 years old (p=0.01). Patients
Survival of older patients in intensive care unit
Aging Clin Exp Res, Vol. 19, No. 1 71
Aging Clin Exp Res 19: 69-74, 2007©2007, Editrice Kurtis
Table 2 - Patient characteristics by hospital mortalitya.
Surviving patients Non-surviving patients p-valueb
n=184 n=147
Average age, years (min-max) 56.9±18.3 (15-97) 63.2±16.4 (17-91) <0.01Age subgroups <0.01
Patients ≤65 years old 115 (62.5) 63 (42.9)Patients 66-75 years old 45 (24.5) 55 (37.4)Patients >75 years old 24 (13.0) 29 (19.7)
Male patients 96 (52.2) 73 (49.7) 0.65APACHE II score (min-max) 17.3±7.0 (2-35) 26.1±8.1 (2-50) <0.001APACHE II - age score (min-max) 14.3±6.3 (1-29) 22.3±8.4 (0-47) <0.001Admission diagnosis
Pulmonary condition 72 (39.1) 44 (29.9) 0.08Cardiac condition 44 (23.9) 34 (23.1) 0.87Sepsis 15 (8.2) 36 (24.5) <0.001Gastrointestinal condition 26 (14.1) 12 (8.2) 0.09Metabolic condition 16 (8.7) 8 (5.4) 0.26Neurologic condition 5 (2.7) 12 (8.2) 0.03Intoxication 6 (3.3) 1 (0.7) 0.14
Post-operative admission 16 (8.7) 21 (14.3) 0.11Underlying diseases
Cardiovascular disease 59 (32.1) 57 (38.8) 0.20Pulmonary disease 56 (30.4) 21 (14.3) <0.01Malignancies 18 (9.8) 22 (15.0) 0.15Chronic liver failure 21 (11.4) 17 (11.6) 0.97Diabetes mellitus 24 (13.0) 20 (13.6) 0.88Chronic renal failure 20 (10.9) 22 (15.0) 0.27Neurologic disease 10 (5.4) 15 (10.2) 0.10Others 20 (10.9) 22 (15.0) 0.27None 18 (9.8) 8 (5.4) 0.15
Comorbidities <0.001Non-fatal/Absent 138 (75.0) 83 (56.5)Ultimately fatal 41 (22.3) 47 (32.0)Rapidly fatal 5 (2.7) 17 (11.6)
Invasive proceduresMechanical ventilation 91 (49.5) 123 (83.7) <0.001Central venous catheter 48 (26.1) 114 (77.6) <0.001Hemodialysis 24 (13.0) 45 (30.6) <0.001Tracheotomy 4 (2.2) 18 (12.2) <0.001
Length of MICU stay <0.001≤14 days 166 (90.2) 105 (71.4)15-30 days 16 (8.7) 32 (21.8)>30 days 2 (1.1) 10 (6.8)
aMeans±standard deviations and numbers (percentages in brackets) are presented, as appropriate. Percents do not total 100.0 for underlying diseases, as somepatients had multiple underlying diseases. bp-value for Chi-square or Fisher’s exact test, and Student’s t-test for categorical and continuous variables, respec-tively. APACHE: Acute physiology and chronic health evaluation; MICU: Medical intensive care unit.

>75 years old and 66-75 years old had more underlyingcardiovascular diseases than patients ≤65 years old(p<0.001 for both). Mechanical ventilation was usedmore commonly in patients 66-75 years old than inthose ≤65 years old (p>0.01) and tracheotomy was per-formed more frequently in patients >75 years old than inthose ≤65 years old (p<0.01).
The expected mortality rate calculated from theAPACHE II score was lower in patients ≤65 years old(33.5%, reference group) than in 66-75 years old (42.3%,p=0.02) and >75 years old (47.1%, p<0.01). The ob-served hospital mortality rate was 35.4% in patients ≤65years old (reference group), 55% in 66-75 years old(p<0.01) and 54.7% in >75 years old (p=0.01). Ac-cordingly, the SMR was 1.06 in patients ≤65 years old,1.30 in 66-75 years old and 1.16 in >75 years old.The MICU mortality rate was 30.9% in patients ≤65years old, 46% in 66-75 years old (p=0.01) and 50.9% in>75 years old (p<0.01) (patients ≤65 years old as the ref-erence group).
The average length of MICU stay was longer in pa-tients >75 years old than in ≤65 years old (15.2±23.7 vs8.4±13.8 days, p=0.02). The average length of MICUstay was 10.6±12.5 days in patients 66-75 years old(p=0.77 compared with patients ≤65 years old). More pa-tients who were >75 years old stayed for >14 days thanthose who were ≤65 years old (30.2% vs 12.4%,p<0.01). Twenty-two percent of patients 66-75 years oldstayed in the MICU for >14 days (p=0.04 compared withpatients ≤65 years old). Length of hospital stay was sim-ilar in all groups (22.5±22.2, 21.7±20.8 and 25.8±25.5days, respectively; p=0.54).
Bivariate analysis of the association between hospitalmortality and various potential risk factors is listed inTable 2. Overall mortality was 44%. Analyses revealed thatolder age, APACHE II score excluding age, sepsis or
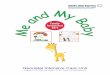
neurologic condition as the admission diagnosis, underly-ing pulmonary disease, fatal comorbidities, mechanicalventilation, central venous catheterization, hemodialysis, tra-cheotomy, and longer MICU length of stay were all sig-nificantly associated with hospital survival. When these fac-tors were examined by multivariate logistic regressionanalysis of hospital survival (i.e., dead vs alive at dis-charge), age 66-75 years and age >75 years (patients aged≤65 years as the reference group), presence of ultimatelyfatal or rapidly fatal diseases, use of mechanical ventilation,performing central venous catheterization and APACHEII – age score were found to be independent predictors ofhospital mortality (Table 3). Pulmonary disease was the on-ly underlying disease predicting discharge from hospital(Table 3). Similarly, Kaplan-Meier survival analysis re-vealed a survival advantage in patients aged ≤65 yearscompared with older patients (Fig. 1). Average survival time(95% CI) was 55.8 (41.7-69.9), 41.0 (30.1-51.9), and46.6 (26.8-66.4) days for patients aged ≤65 years, 66-75,and >75 years, respectively (p=0.02).
DISCUSSION This study demonstrates that critically ill patients aged
66-75 years had 3.1 times odds of dying and patients>75 years old had 2.7 times odds of dying in hospital,both compared with patients ≤65 years old, controlling forpotential confounders like disease severity score, admis-sion diagnosis, comorbidities, invasive procedures, andlength of MICU stayed (Table 3). Survival analysis also re-vealed that critically ill older patients had poorer survivalthan patients aged ≤65 years (Fig. 1).
The outcome of critically ill elderly patients has beenthe focus of interest of healthcare providers for a longtime, mostly because of the high costs of intensive care.
A. Topeli and B.Cakir
72 Aging Clin Exp Res, Vol. 19, No. 1
Aging Clin Exp Res 19: 69-74, 2007©2007, Editrice Kurtis
Table 3 - Independent predictors of hospital mortality.
OR (CI) p
Age subgroups (reference group: patients ≤65 years old) <0.01
Patients 66-75 years old 3.1 (1.5-6.2) <0.01Patients >75 years old 2.7 (1.2-6.3) 0.02
Comorbidities (reference group: <0.01‘non-fatal/absent’)
Ultimately fatal 2.7 (1.3-5.3) <0.01Rapidly fatal 5.2 (1.4-20.0) 0.02
Mechanical ventilation (ref: not used) 4.9 (2.4-10.2) <0.0001Central venous catheter (ref: not performed) 3.8 (2.0-7.3) <0.0001APACHE II - age score 1.08 (1.04-1.13) <0.001Underlying pulmonary disease 0.4 (0.2-1.0) 0.04
APACHE: Acute physiology and chronic health evaluation; OR: Odds ratio;CI: Confidence interval.
Sur
viva
l
0 50 100 150 200Hospital lenght of stay, days
Fig. 1 - Survival curves for patients stratified by age. Patients ≤65years old (thin dotted line) had better hospital outcomes than pa-tients 66-75 years old (thick dotted line) and patients >75 yearsold (straight line) (p=0.02).

Quite a number of studies, most of which are from high-income countries, revealed that age is not related toprognosis (6, 7, 9-16, 18). However, other studies re-vealed that age is a determinant of prognosis (3-5, 8, 17,19, 20, 22, 23), whereas Somme et al. (21) showedthat age was not related to ICU mortality but was, instead,a determinant of long-term outcome.
Different conclusions obtained from different studiesmay be related to differences in study design, some beingdescriptive studies, only involving older patients (4, 11, 12,19), differences in the cut-off value for the definition of“old”, and differences in outcome variable, some studieslooking at short-term outcomes only (6, 7, 9, 13, 19, 20,22). In addition, variations in the selection and control ofpotential confounders in different studies may lead toconflicting results. In most studies performing multivariateanalysis in older critically ill patients, disease severitywas included as a confounding factor (4, 6, 8-10, 12, 13,15, 17-21). However, disease severity is not sufficient initself, because today’s scoring systems such as APACHEII take into consideration only the parameters obtainedwithin the first 24 hours of admission. Various otherconditions or procedures occurring and/or performedduring the course of the ICU stay and even after dis-charge, may influence the final hospital outcome. We ex-amined several parameters such as admission diagnosis,underlying diseases and invasive procedures in our mul-tivariate analysis, in addition to the APACHE II score.Even these parameters were not sufficient, because re-cently some other factors, such as the development ofdelirium, which affects older people more (27), havebeen demonstrated to influence outcomes (28). In addi-tion, nutritional status has been shown to influence out-comes (29). Inability to adjust for such factors may be alimitation of our study and of others.
Examination of mortality patterns of older patientsfor selected diseases may improve the validity of the re-sults. For instance, Ely et al. (20) studied the outcome ofolder patients with acute lung injury or acute respiratorydistress syndrome, and found that patients aged >70years had poor hospital outcomes. Our study was con-ducted in a single MICU and included a limited number ofpatients, hampering our power to perform disease-specificcalculations. Instead, studying mortality in a single unit hadseveral advantages, including a narrowed case-mix. Also,studying mortality in a “closed MICU”, i.e., one with a sin-gle attending physician as the medical director controllingall patient admissions, follow-up and discharge, elimi-nated potential physician bias.
In this study, the observed-to-expected mortality rate wasgreater than 1 in both groups, although the ratio was muchhigher in the older group. Again, the limited resources ofa developing country may influence the ICU care of pa-tients. For instance, the nurse-to-patient ratio was 1 to 3or 4 in our ICU. In addition, “do-not-resuscitate” orders are
not accepted in Turkey, and the mortality rates reported inthis study therefore include terminally ill patients.
Studies about the outcome of critically ill older patientshave been performed in developed countries in which old-er people constitute a major part of the population. Thepresent study, performed in a developing country, showedthat age is a determinant of the hospital survival of criti-cally ill patients. Although we did not use an objectivemeasure for the baseline health status of our older pa-tients, in as much as they were residents of a developingcountry, they may have had different baseline healthstatus and/or quality of life than their counterparts livingin developed countries.
Another limitation of this study is the lack of mea-surement of functional status parameters and quality oflife, which have been found to be predictors of mortalityin the elderly population (10, 30-32). As study participantswere followed untill death or discharge from hospital, wedo not know the long-term outcomes of study population,nor the quality of life after the MICU stay.
Nevertheless, this study may represent a model forother developing countries, from which further studieson larger cohorts with data for several other con-founders are needed.
CONCLUSIONSThis study revealed that older critically ill patients
have a poorer hospital survival than patients aged ≤65years, when other variables which may affect MICU sur-vival were controlled for. Further studies, especially fromdeveloping countries in which health expenditure con-stitutes only a minority of the gross national product, areclearly warranted for conclusive results.
REFERENCES 1. Wood KA, Ely EW. What does it mean to be critically ill and el-
derly? Curr Opin Crit Care 2003; 9: 316-20.2. Nuckton TJ, List ND. Age as a factor in critical care unit admis-
sions. Arch Intern Med 1995; 155: 1087-92.3. Campion EW, Mulley AG, Goldstein RL, Barnett GO, Thibault
GE. Medical intensive care for the elderly. A study of current use,costs and outcomes. JAMA 1981; 246: 2052-56.
4. Le Gall JR, Brun-Buisson C, Trunet P, Latournerie J, ChantereauS, Rapin M. Influence of age, previous health status and severityof acute illness on outcome from intensive care. Crit Care Med1982; 10: 575-7.
5. McLean RF, McIntosh JD, Kung GY, Leung DM, Byrick RJ. Out-come of respiratory intensive care for the elderly. Crit CareMed 1985; 13: 625-9.
6. McClish DK, Powell SH, Montenegro H, Nockomovitz M. The im-pact of age on utilization of intesive care resources. J Am GeriatrSoc 1987; 35: 983-8.
7. Nicolas F, Le Gall JR, Alperovitch A, Loirat P, Villers D. Influenceof patients’ age on survival, level of therapy and length of stay inintensive care units. Intensive Care Med 1987; 13: 9-13.
8. Ridley S, Jackson R, Findlay J, Wallace P. Long-term survival af-ter intensive care. BMJ 1990; 301: 1127-30.
Survival of older patients in intensive care unit
Aging Clin Exp Res, Vol. 19, No. 1 73
Aging Clin Exp Res 19: 69-74, 2007©2007, Editrice Kurtis

9. Wu AW, Rubin HR, Rosen MJ. Are elderly people less responsiveto intensive care? J Am Geriatr Soc 1990; 38: 621-7.
10. Mayer-Oakes SA, Oye RK, Leake B. Predictors of mortality in old-er patients following medical intensive care: the importance offunctional status. J Am Geriatr Soc 1991; 39: 862-8.
11. Chelluri L, Pinsky MR, Grenvik ANA. Outcome of intensivecare of the oldest-old critically ill patients. Crit Care Med 1992;20: 757-61.
12. Kass JE, Castriotta RJ, Malakoff F. Intensive care unit outcomein the very elderly. Crit Care Med 1992; 20: 1666-71.
13. Pesau B, Falger S, Berger E, et al. Influence of age on out-come of mechanically ventilated patients in an intensive care unit.Crit Care Med 1992; 20: 489-92.
14. Chelluri L, Pinsky MR, Donahoe MP, Grenvik A. Long-termoutcome of critically ill elderly patients requiring intensive care. JAMA 1993; 269: 3119-23.
15. Rockwood K, Noseworthy TW, Gibney RTN, et al. One-year out-come of elderly and young patients admitted to intensive careunits. Crit Care Med 1993; 21: 687-91.
16. Chelluri L, Grenvik A, Silverman M. Intensive care for critically illelderly: mortality, costs and quality of life. Arch Intern Med1995; 155: 1013-22.
17. Djaiani G, Ridley S. Outcome of intensive care in the elderly.Anaesthesia 1997; 52: 1130-6.
18. Hamel MB, Davis RB, Teno JM, et al. Older age, aggressivenessof care, and survival for seriously ill, hospitalized adults. Ann In-tern Med 1999; 131: 721-8.
19. Van den Noortgate N, Vogelaers D, Afschrift M, Colardyn F. In-tensive care for very elderly patients: outcome and risk factors forin-hospital mortality. Age Ageing 1999; 28: 253-6.
20. Ely EW, Wheeler AP, Thompson BT, Ancukiewicz M, SteinbergKP, Bernard GR. Recovery rate and prognosis in older personswho develop acute lung injury and the acute respiratory distresssyndrome. Ann Intern Med 2002; 136: 25-36.
21. Somme D, Maillet JM, Gisselbrecht M, Novara A, Ract C, FagonJY. Critically ill old and the oldest-old patients in intensive care:
short- and long-term outcomes. Intensive Care Med 2003; 29:2137-43.
22. Esteban A, Anzueto A, Frutos-Vivar F, et al. Outcome of older pa-tients receiving mechanical ventilation. Intensive Care Med 2004;30: 639-46.
23. Marengoni A, Cossi S, De Martinis M, et al. Adverse outcomes inolder hospitalized patients: the role of multidimensional geri-atric assessment. Aging Clin Exp Res 2003; 15: 32-37.
24. Country information. Available at www.countryreports.org/pre-mium/content/2002/turkey.htm
25. McCabe JR, Jackson GG. Gram-negative bacteraemia I: etiologyand ecology. Arch Intern Med 1962; 110: 847-55.
26. Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHEII: a severity of disease classification system. Crit Care Med1985; 13: 818-29.
27. McNicoll L, Pisani MA, Zhang Y, Ely EW, Siegel MD, Inouye SK.Delirium in the intensive care unit: occurrence and clinical coursein older patients. J Am Geriatr Soc 2003; 51: 591-8.
28. Ely EW, Shintani A, Truman B, et al. Delirium as a predictor ofmortality in mechanically ventilated patients in the intensive careunit. JAMA 2004; 291: 1753-62.
29. Donini LM, De Bernardini L, De Felice MR, Savina C, Coletti C,Cannella C. Effect of nutritional status on clinical outcome in apopulation of geriatric rehabilitation patients. Aging Clin Exp Res2004; 16: 132-8.
30. Inouye SK, Peduzzi PN, Robison JT, Hughes JS, Horwitz RI,Concato J. Importance of functional measures in predictingmortality among older hospitalized patients. JAMA 1998; 279:1187-93.
31. Dominick KL, Ahern FM, Gold CH, Heller DA. Relationship ofhealth-related quality of life to health care utilization and mor-tality among older adults. Aging Clin Exp Res 2002; 14: 499-508.
32. Minicuci N, Maggi S, Noale M, Trabucchi M, Spolaore P, Crepal-di G. Predicting mortality in older patients. The VELCA study. Ag-ing Clin Exp Res 2003; 15: 328-35.
A. Topeli and B.Cakir
74 Aging Clin Exp Res, Vol. 19, No. 1
Aging Clin Exp Res 19: 69-74, 2007©2007, Editrice Kurtis