Embed Size (px)
Citation preview

This article was downloaded by: [The UC Irvine Libraries]On: 08 November 2014, At: 23:12Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Psychology & HealthPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/gpsh20
Hostility, oral contraceptive use,and cardiovascular reactivity inwomenKathryn Graff Low a , Gillian Casey a , Alison Megroz a ,Kathleen Leonard a , Kmberly McGuffee a & Lisa Briand aa Department of Psychology , Bates College , Lewiston,Maine, 04240Published online: 19 Dec 2007.
To cite this article: Kathryn Graff Low , Gillian Casey , Alison Megroz , Kathleen Leonard ,Kmberly McGuffee & Lisa Briand (2001) Hostility, oral contraceptive use, and cardiovascularreactivity in women, Psychology & Health, 16:6, 675-687, DOI: 10.1080/08870440108405866
To link to this article: http://dx.doi.org/10.1080/08870440108405866
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information(the “Content”) contained in the publications on our platform. However, Taylor& Francis, our agents, and our licensors make no representations or warrantieswhatsoever as to the accuracy, completeness, or suitability for any purpose of theContent. Any opinions and views expressed in this publication are the opinions andviews of the authors, and are not the views of or endorsed by Taylor & Francis. Theaccuracy of the Content should not be relied upon and should be independentlyverified with primary sources of information. Taylor and Francis shall not be liablefor any losses, actions, claims, proceedings, demands, costs, expenses, damages,and other liabilities whatsoever or howsoever caused arising directly or indirectly inconnection with, in relation to or arising out of the use of the Content.
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden.

Terms & Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions
Dow
nloa
ded
by [
The
UC
Irv
ine
Lib
rari
es]
at 2
3:12
08
Nov
embe
r 20
14

Psychologyand Health, 2001, Vol. 16, pp. 675687 Reprints available directly from the Publisher Photocopying permitted by license only
0 2001 OPA (Overseas Publishers Association) N.V. Published by license under
the Hanvood Academic Publishers imprint, part of Gordon and Breach Publishing,
a member of the Taylor & Francis Group. Printed in Malaysia.
HOSTILITY, ORAL CONTRACEPTIVE USE, AND CARDIOVASCULAR REACTIVITY IN WOMEN
KATHRYN GRAFF LOW*, GILLIAN CASEY, ALISON MEGROZ, KATHLEEN LEONARD, KIMBERLY McGUFFIE and LISA BRIAND
Department of Psychology, Bates College, Lewiston, Maine 04240
(Received 7 September, 1999; in$final form 17 August, 2000)
Hostility, task instructions, social desirability and cardiovascular reactivity were investigated in a exploratory study of 70 female college students and employees. Women were administered the Videotaped Clinical Interview (VCI), the Marlowe-Crowne Social Desirability Scale (MC), the Cook-Medley Hostility Scale (CM), the Buss- Durkee Hostility Index (BD) and the Personal Attributes Questionnaire (PAQ) before undergoing a stressful discussion. Oral contraceptive users had significantly higher DBP at baseline. Based on PAQ scores, women were given instructions for the discussion task consistent or inconsistent with their gender-relevant styles. Instruction type predicted heart rate changes, and interacted with hostility to predict DBP reactivity. Interview-based hostility (VCI-H) was associated with increased DBP during the discussion task, as was being high hostile (low MChigh VCI-H). The CM and the BD had less association with heart rate and blood pressure changes. Oral contraceptive (OC) use was associated with higher SBP reactivity under stress, with highest SBP increases in the OC users con- cerned with social desirability. The complex interaction between trait dimensions like hostility, social desirability, and oral contraceptive use requires further investigation.
KEY WORDS: Reactivity, hostility, oral contraceptives.
HOSTILITY, ORAL CONTRACEPTIVE USE, AND CARDIOVASCULAR REACTIVITY IN WOMEN
Heart disease is the leading cause of death in women in the United States (U.S. Bureau of Census, 1994), and there is accumulating evidence that the pathogenesis of coronary artery disease (CAD) may differ in the two sexes (Arnstein er al., 1996). Several traditional risk factors, such as diabetes mellitus, appear to be more salient in women (Evanoski, 1997), and risk factors related to menstrual hormones and timing of menopause (Evanoski, 1997) are uniquely female. A variety of psychosocial risk factors for CAD have also been explored in women, including Type A behavior, hostility, and marital discord (Barefoot et al., 1995; Case et al., 1992; Low et al., 1994). It is believed that the stress-induced neuroendocrine and cardiovascular reactivity resulting from these negative emotions may be associated with CAD over the long term (Dimsdale, 1993; Manuck, 1994; Helmers et al., 1994). In recent research, hostility has had the strongest associations with cardiovascular disease endpoints and reactivity in both men and women (Hardy and Smith, 1988; Manuck, 1994; Powch and Houston, 1996).
* Corresponding author. Tel.: 207-786-6186; E-mail: [email protected]
675
Dow
nloa
ded
by [
The
UC
Irv
ine
Lib
rari
es]
at 2
3:12
08
Nov
embe
r 20
14

676 K.G. LOW ETAL.
A variety of variables related to the expression of anger, such as hostility, defensive hostility, cynicism, and anger expression, have been correlated with cardiovascular react- ivity in laboratory studies with predominantly male participants (Carroll et al., 1997; Hardy and Smith, 1988; Smith and Allred, 1989; Suarez and Williams, 1989). More recent research on ambulatory blood pressure in naturalistic settings has confirmed the link between hostility and cardiovascular arousal in such samples (Ewart and Kolodner, 1994; Jamner et al., 1991; Linden et al., 1993). In short, the accumulating literature on hostility suggests that it is indeed a correlate of both coronary disease endpoints and reactivity in males.
Research on hostility continues to be beset with methodological problems, however. Definitions of hostility and its components vary in their emphases, making research on cardiovascular reactivity difficult to integrate. For example, the Cook and Medley Ho Scale ( 1 954) assesses cognitive components of hostility such as cynicism, while the Buss- Durkee Hostility Index (1 957) targets .aggressive attitudes and behaviors (Barefoot and Lipkus, 1994). Further, the Ho may have different meaning depending on the gender of the respondent (Steinberg and Jorgensen, 1996). Despite the fact that studies on cardiovascular disease endpoints report that interview-based measures of hostility or Type A pattern are better predictors of disease status in coronary patients (Rosenhan et al., 1988; Raikkonen et al., 1999), most of the reactivity research has used self-report measures of hostility. Finally, many studies of hostility and cardiovascular reactivity have included only male participants (Burns et al., 1992; Carroll et al., 1997; Jamner et al., 1991; Siegman et al., 1992). Some have suggested that women may inhibit hostility and aggression (Lerner, 1985; Powch and Houston, 1996); such variables may therefore predict reactivity better in men than in women (Linden et al., 1993; Smith et al., 1996) because of social desirability and resultant underreporting of anger and hostility.
Recent research has explored the degree to which social desirability and its interaction with hostility affect cardiovascular endpoints (Helmers and Krantz, 1996; Helmers et af., 1995; Larson and Langer, 1997). Studies have found that high defensive (high MC) high hostile (CM) males have the greatest blood pressure reactivity (Helmers and Krantz, 1996) and more ischemic episodes (Helmers et al., 1995). Findings were mixed in women, with low hostile (low MC/low Ho) women having the lowest SBP and DBP levels. Such research suggests the need to explore anger suppression and social desirability in combination with hostility measures in both men and women.
In addition, previous research indicates that men and women respond differently to stressors in both laboratory and naturalistic settings (Allen et al., 1996; Dimsdale, 1993; Ewart and Kolodner, 1994; Smith and Gallo, 1999): for example, men are more likely to respond to stressors with larger increases in systolic blood pressure than women (Davis and Matthews, 1996; Dimsdale, 1993; Ewart and Kolodner, 1994; Fichera and Andreassi, 1998). In contrast, women may have greater heart rate increases compared to men (Stoney et al., 1987). The menstrual cycle may partially explain such gender differences, given some evidence that reactivity may increase during the luteal phase (e.g. Hastrup and Light, 1984; Stoney et al., 1987; Fontana and McLaughlin, 1998) and with oral contraceptive use (Suarez et al., 1995; Davis, 1999). f
Interpretation of laboratory-based data is further complicated by the fact that there are few studies examining the effectiveness of traditional laboratory stressors such as mental arithmetic or puzzles in cardiovascular research on women (Frankenhauser, 1983; Linden et al., 1998; Waldstein and Neumann, 1998). Specifically, women may have greater responses to challenges that are female-relevant or consistent with gender-socialization
Dow
nloa
ded
by [
The
UC
Irv
ine
Lib
rari
es]
at 2
3:12
08
Nov
embe
r 20
14

HOSTILITY, GENDER AND REACTIVITY 617
(Davis and Matthews, 1996). A growing number of studies support the hypothesis that social stress (interpersonal interactions, cooperative role tasks, discussions) elicits more reactivity in both men and women than traditional laboratory tasks (mirror tracing, math problems) (Ewart et al., 1991; Lassner et al., 1994; Smith et al., 1996; Suarez et al., 1993; Waldstein et al., 1998). Gender differences in cardiovascular reactivity in studies employ- ing traditional stressors therefore may also be the result of using stress inductions that are less effective in women because of gender-socialization.
To explore the interaction between gender and task, Davis and Matthews assessed the contribution of gender-attributes and gender-relevant instructions on cardiovascular react- ivity (1996). Specifically, men and women were assessed for instrumental or expressive style, and were asked to engage in interpersonal tasks that were either consistent or consist- ent with style as assessed by the Personal Attributes Questionnaire (PAQ, Spence et al., 1975). Contrary to the authors’ hypothesis, participants in the inconsistent conditions had the greatest reactivity in response to an interpersonal challenge. Like Ewart, these authors found that interactions between a stressful task and personal attributes (sociotropy or gender-relevant style, respectively) were associated with reactivity. The relationship between hostility and person-task interactions remains unexplored.
The present pilot study assessed hostility in women using both self report (Cook and Medley Ho, Buss-Durkee Hostility Inventory) and interview based measures (Videotaped Clinical Interview). Participants were also tested for gender-linked attributes using the PAQ, and were given instructions during a stressful task consistent or inconsistent with attributes. Heart rate and blood pressure were assessed at baseline, which included a low-stress conversation, and during the stressful discussion task. It was hypothesized that an interview-based measure of hostility would be the best predictor of cardiovascular react- ivity. Based on previous research, it was also hypothesized that women in the inconsistent instruction condition would have more blood pressure reactivity, and that hostility and con- dition would interact, with hostile women assigned the most demanding task (inconsistent instruction) having the highest reactivity. The roles of social desirability and oral contra- ceptives in combination with hostility were also explored.
METHOD
Overview
Participants gave informed consent, and were asked to complete a variety of ques- tionnaires. The PAQ was scored before the low-stress interview and task portion of the research began. Women were then given instructions that were consistent or inconsistent with their PAQ-defined style (see Davis and Matthews, 1996). For example, women high in the expressive dimension of the PAQ were asked to be assertive during the conversation, to refute differing opinions, and to persuade the confederate of their point of view. Similar- ly, women higher on the instrumental sub-scale were instructed to be particularly receptive, empathic, and sensitive to the confederate’s arguments. In women whose PAQ-I and PAQ- E scores were identical, instructions were alternately assigned instrumental or expressive instructions.
Effects of oral contraceptive use, hostility, and social desirability on reactivity were explored through stepwise hierarchical multiple regression. Analyses controlled for age,
Dow
nloa
ded
by [
The
UC
Irv
ine
Lib
rari
es]
at 2
3:12
08
Nov
embe
r 20
14

678 K.G. LOW ETAL.
body mass index, and oral contraceptives (dummy coded O/l) in a first step, psychosocial variables (social desirability, hostility, PAQ instruction (dummy coded 0/1)) in a second step, and interaction terms in a last block.
Participants
Seventy women between the ages of 18 and 38 were recruited on a college campus. The women were 96 percent Caucasian, and were predominantly middle class. Participants were instructed to avoid cigarettes and caffeine on the day of the assessment. Based on self- report, it was determined that the participants were in good health, were normal weight based on BMI, did not take prescription medication other than oral contraceptives, and menstruated regularly. Date of last menstrual period was used to estimate phase of the menstrual cycle. Thirty-one percent of participants were taking oral contraceptives. The women were reimbursed $5.00 for participation.
Procedure
Four readings of heart rate and blood pressure were taken before and during a low-stress interview, at the culmination of the interview, and after a five-minute rest period. Readings were averaged to determine baseline measures. Participants were then informed that they would participate in a discussion of gun control, and were asked to formulate an opinion on the topic and state it to open the discussion. The confederate was instructed to disagree regardless of the participant’s position, but to maintain a neutral demeanor (for similar discussion tasks see Davis and Matthews, 1996; Powch and Houston, 1996). Instructions were either consistent (N=40) or inconsistent ( N = 3 0 ) with PAQ scores (see Davis and Matthews, 1996). Heart rate and blood pressure readings were taken five minutes into the stressful task. Changes in heart rate for statistical analyses were these readings subtracted from baseline. Participants were debriefed at the conclusion of the study.
Self-report Measures
Self-report measures of hostility included the Cook and Medley Ho Scale (Ho; Cook and Medley, 1954) and the Buss-Durkee Hostility Index (BD; 1957). The CM is a 50-item measure with acceptable consistency and validity (Houston and Vavak, 1991). The Buss- Durkee consists of a variety of sub-scales (aggression, suspicion, resentment, irritability and assaultiveness were used in the present study) with adequate reliability and validity (Powch and Houston, 1996). The Personal Attributes Questionnaire (PAQ) (Spence et al., 1975) is a 24-item self-report measure which assesses gender-related dimensions like assertiveness and empathy. The PAQ generates scores on expressiveness and instrumental- ity, and these can be used to identify individuals as favoring one or the other interpersonal approach. The reliability and validity of the PAQ are well-documented (Spence et al., 1975). The Marlowe-Crowne Social Desirability Scale (MC; Crowne and Marlowe, 1964) is a 33-item questionnaire which assesses social desirability or concerns about social representation. The MC has acceptable test-retest reliability (I-= .86) and internal consistency (a= .70), and adequate validity (Crowne and Marlowe, 1964).
Dow
nloa
ded
by [
The
UC
Irv
ine
Lib
rari
es]
at 2
3:12
08
Nov
embe
r 20
14

HOSTILITY, GENDER AND REACTIVITY 679
Videotaped Clinical Interview
The VCI is an interview protocol consisting of 35 items assessing Type A behavior based on both content and behavior during the interview. The VCI has adequate reliability and validity (Friedman and Powell, 1984), and has been shown to predict degree of atheroscler- osis in women with CAD (Low et al., 1998). Inter-rater reliablity for VCI-Hostility scores for this and a related project (ratings were done by the VCI-trained first author) was r = .8 1. In the present study, the hostility sub-scale of the VCI was used in analyses.
Physiological Measures
A Marshall-97 oscillometric sphygmomanometer was attached to the non-dominant arm of participants. Blood pressure and heart rate readings were taken before during and after a low-stress discussion to establish baselines, and five minutes into a stressful discussion on gun control.
RESULTS
Descriptive statistics for the psychosocial measures are summarized in Table 1. The present sample was slightly less hostile than women in previous studies (CM; X = 16.9(5.1) vs. 19.6 (6.9) in Powch and Houston, 1996; mean BD subscales all lower, than Lawler et al., 1993 or Suarez et al., 1993; VCI-H lower than Low et al., 1994). In addition, the average social desirability scores (MC) were somewhat lower than those reported in previous research (Helmers et al., 1994).
One-way analysis of variance of menstrual phase by reactivity for each of the three physiological variables was non-significant. Use of oral contraceptives was significantly correlated with baseline measures of blood pressure, and was therefore included in analysis of variance and multiple regression models. There were no significant differences between oral contraceptive users and non-users on any of the psychosocial measures (see Table 1). Similarly, hostility measures were not associated with baseline measures of heart rate or blood pressure.
Table 1 Means and standard deviations of psychosocial variables by oral contraceptive use
Variable ~ ~ ~ ~ ~~
Grand Mean OC Users Non-OC Users (N = 70) (N = 19) (N=51)
~ ~~ ~
Body Mass Index Age VCI-Total
VCI-Hostility CM Total
CM Hostility BD Hostility Index
Resentment Assaultiveness
MCIndex PAQ-Expressive PAQ-Instrumental
~
23.4 (3.8) 20.9 (4.7) 25.4 (8.8) 6.2 (4.0)
16.8 (5.2) 3.8 (2.1)
17.2 (6.9) 2.2 (1.7) 2.3 (2.2)
14.3 (4.8) 30.7 (4.2) 26.0(5.1)
~~
23.6 (3.8) 20.2 (2.2) 24.6 (8.9) 5.4 (4.1)
15.6 (4.3) 3.4 (2.2)
17.7 (6.9) 2.2 ( I .7) 2.0 (2.2)
14.4 (5.0) 32.1 (5.2) 27.2 (4.4)
23.3 (3.9) 21.3 (5.3) 25.6 (8.9) 6.5 (4.0)
17.3 (5.4) 3.6 (2.2)
16.1 (1.7) 2.1 (1.6) 2.4 (2.1)
14.3 (4.8) 30.2 (3.8) 25.6 (5.4)
VCI = Videotaped Clinical Interview: CM = Cook-Medley; BD = Buss-Durkee; MC = Marlowe-Crowne Social Desirability Index; PAQ = Personal Attributes Questionnaire.
Dow
nloa
ded
by [
The
UC
Irv
ine
Lib
rari
es]
at 2
3:12
08
Nov
embe
r 20
14

680 K.G. LOW ETAL.
Table 2 Correlations of hostility measures and sub-scales with changes in heart rate and blood pressure (N = 70)
Variubles 2 3 4 5 6 7
1. VCI-Hostility .33** .53** -.068 .30** .02 .24* 2. Cook-Medley Ho - .64** -.04 .I4 -.04 -.09 3. Buss-Durkee - - -.02 .21* -.02 .03 4. Marlowe-Crowne - - - -.06 .35** .06 5. Change in HR - - - - .09 .I0 6. Change in SBP - - - - - . I3 7. Change in DBP
**p < .01: * p c .05.
Preliminary univariate correlations (Table 2) were used to identify the measure of hostility or its sub-scales most highly correlated with changes in heart rate or blood pressure during the stressful task, and to explore the relationships between measures of hostility. The VCI-H was correlated with both change in heart rate and change in diastolic blood pressure ( r = .30, p c .01 and r= .24, p c .05 respectively), and therefore appeared to be the best predictor of reactivity. The Ho was not associated with reactivity during the discussion task, and the BD was only correlated with HR changes (r=.27, p < .05). Correlations between the hostility measures were modest, suggesting ap- proximately 9-38% of variance in common. The lowest correlation was between the VCI- H and the Ho ( r = .33, p c .05), despite the fact that both purport to measure attitudinal aspects of hostility. The VCI-H, Marlowe-Crowne and PAQ scores were independent ( r < . 1 , p > .05).
Stepwise multiple regression was used to test the effects of age, BMI, oral contraceptive use, social desirability, consistent or inconsistent instruction, hostility (VCI-H), and their interactions on change in cardiovascular measures (see Table 3). For all dependent vari- ables, baseline descriptive variables were stepped in first, followed by a dummy coded (0 / 1) contraceptive variable, hostility (VCI), defensiveness (MC), PAQ instruction type and the interaction terms.
In predicting HR, hostility was marginally significant, with hostile individuals having the greatest HR reactivity. PAQ instruction was significant (t= -2.6, p = .Ol), with women given instructions inconsistent with their personality style having the greatest heart rate reactivity during the stressful task (p c .05). Finally, hostility interacted with contraceptive use to predict heart rate increases, with high hostile non-OC users having the greatest change (p < .05). On the whole, however, the model did not account for a significant pro- portion of the variance (R2 =. 19, F = 1.2, p = .3 1).
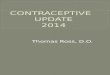
For DBP, age accounted for a significant portion of the variance ( t= -2.6, p = .009). Hostility made an additional significant contribution ( t= 3.7, p = .0006). The two-way interaction between hostility and social desirability was significant ( t = -2.1, p = .04); low social desirability and high hostility (e.g. high hostile) women had greater DBP reactivity under stress than the low hostile women (p c .05) (see Figure 1). Similarly, the interaction between instruction type and hostility was marginally significant, with hostile women given instructions inconsistent with their PAQ score having the greatest reactivity. The three-way interaction between OC use, hostility and social desirability did not add to the model. The final model, including marginal interactions, accounted for 41% (p = .002) of the variance in DBP reactivity.
Dow
nloa
ded
by [
The
UC
Irv
ine
Lib
rari
es]
at 2
3:12
08
Nov
embe
r 20
14

HOSTILITY, GENDER AND REACTIVITY 68 1
Table 3 pressure from interview-based measure of hostility (N= 70)
Multiple regession models predicting change in heart rate, systolic blood pressure, and diastolic blood
Step Variable entered ARz P t P
Heart rate I . Age
BMI Oral Contraceptives
2. Marlowe-Crowne VCI-Host PAQ Instruction
VCI-H x Marlowe- Crowne
OC x Marlowe-Crowne VCI-H x OC x Marlowe Crowne
3. VCI-H x PAQ Instruction
VCI-H x OC
4. Total R2 = .19, F = 1 . 2 , ~ = .3 1 Systolic Blood Pressure 1. Age
BMI Oral Contraceptives
2. Marlowe-Crowne VCI-Host PAQ Instruction
VCI-H x Marlowe- Crowne
OC x Marlowe Crowne VCI-H x OC x Marlowe Crowne
3. VCI-H x PAQ Instruction
VCI-H x OC
4. Total R2 = .42, F = 3.4, p = .0015 Diastolic Blood Pressure 1. Age
BMI Oral Contraceptives
2. Marlowe-Crowne VCI-Host PAQ-Instruction
VCI-H x Marlowe-Crowne VCI-H x OC OC x Marlowe-Crowne VCI-H x OC x Marlowe-Crowne
3. VCI-H x PAQ Instruction
4. Total R2= .41, F =3.2,p= ,002
,027 .03 .17 .oo
.073 .33 1 .oo -.33 -.52
,035 -.54 -1.5 -1.2
.045 1.3
.04 - . I 1 -.07 -1.2
.I4 .05 .38 .06
.22 -.44 .07
-.04 1 .5
.03 NS
.I3 -.32 .I4 .I6 .36
. I 1 1.70 -.13
.I5 -.81 -.71 -.01
.I9 -.01 NS
.25 1.30 1.71 1.2 1.8
-2.6 - 1.02 -1.30 -2.2 -1.6
1.9
-.94 -.54 -3.1
.2 1
.81
.5 1 -1.0
.19 -. 19 4. I
-2.6 1.2 .4
1 .5 3.7
-1.1 -1.9 -2.1 -.05
.53
.79
.20
.09
.2 1
.07
.o 1
.3 I
.17
.02
.06
.06
.35
.58 ,004 .84 .42 .61 .30 .85 .85 ,0001
,009 .25 .68 .13 .0006 .26 .06 .04 .95 .34
VCI-H = Videotaped Clinical Interview (hostility); PAQ Instruction = dummy coded variable indicating instructions consistent or inconsistent with PAQ score; OC = oral contraceptive use.
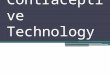
For SBP, contraceptive use accounted for a significant portion of the variance ( t = -3.1, p = .004), and OCs interacted with social desirability ( t = 4.1, p = .0001) such that there was marginally greater reactivity in OC users, and greatest reactivity in the OC users high in social desirability (see Figure 2). The three-way interaction (OC x VCI-H x MC) was not significant. The total RZ for the model was .42 ( F = 3.4, p < .0015).
Dow
nloa
ded
by [
The
UC
Irv
ine
Lib
rari
es]
at 2
3:12
08
Nov
embe
r 20
14

682 K.G. LOW ETAL.
4 -
3 .
2 = 2. 8 2 n 1 .
a a - l * VCI-Hostility
3 0 .
C
t3) c
.- -
- 2 . Low if __
2 - 4 , Hlsh c - 3 '
.oo 1 .oo
Marlowe Crowne (Dichotomized)
Figure 1 Interaction between hostility and social desirability to predict change in diastolic blood pressure.
0
0 0 .- - c
($ -10
r C
a, .-
.I=
0 -20
Status
.oo 1 .oo
Marlowe Crowne Social Desirability Index (Low/High)
Figure 2 Interaction between Marlowe-Crowne and OC use predicting change in systolic blood pressure.
DISCUSSION
In general, women in the present study were somewhat less hostile than comparable samples regardless of the type of measure. Although interview-based ratings of hostility reportedly vary with gender of coder (Davidson et al., 1996), the relatively low scores on the
Dow
nloa
ded
by [
The
UC
Irv
ine
Lib
rari
es]
at 2
3:12
08
Nov
embe
r 20
14

HOSTILITY. GENDER AND REACTIVITY 683
Table 4 Three-way Analysis of Variance Predicting Reactivity from VCI-Hostility
ss DF F Significance
Heart Rate Main Effects
VCI-Ho Marlowe-Crowne Contraceptives
2-way Interactions VCI x MC VCI x Contra MC x Contra
3-way Interactions Systolic Blood Pressure Main Effects
VCI-HO Marlowe-Crowne Contraceptives
2-way Interactions VCI-HO x MC VCI-Ho x Contra MC x Contra
3-way Interactions Diastolic Blood Pressure Main Effects
VCI-HO Marlowe-Crowne Contraceptives
2-way Interactions VCI-Ho x MC VCI-Ho x Contra MC x Contra
3-way Interactions
100.0 7.4 2.9
2.2 .16 .07
.14
.68
.80
4.7 3.8
180.0
. I 1
.09 4.02
.74
.77
.05 NS
.23 629.4 30.7
.oo 10.20 SO
.95 ,002 .488
1.9 174.3 903.2
.03 2.80
14.70
.86
.09 .0001 NS
303.5 . I 1
388.5
8.2 I .oo
10.53
,006 .96
,002
186.8 79.5 .036
5.0 2.1
,001
,029 .I5 .98
451.1 12.1 ,001 1
VCI are consistent with self-report measures, and suggest a low-hostility sample. Correla- tions between the measures of hostility were modest, underscoring the difficulties with ac- curate assessment of multi-dimensional hostility (Steinberg and Jorgensen, 1996). Further, there were no significant correlations between the CM and changes in reactivity.
In contrast, the interview-based measure of hostility (VCI-H) was associated with both change in heart rate and change in diastolic blood pressure in univariate analyses and mul- tiple regression models. The VCI-H assesses both responses to questions and a variety of behaviors during the interview, including interruptions, facial expression, use of obscenity, and gestures. Because the VCI-H does not rely on self-report, it may avoid response biases that affect pencil and paper assessment of hostile affect in women, such as social desirabil- ity. For example, the correlation between VCI-H and MC scores is non-significant in the pre- sent sample, in contrast to the strong negative correlation between social desirability and the Cook-Medley scales in previous research (-.46 < r<-.58; Powch and Houston, 1996).
As predicted, hostility as assessed by VCI-H scores was positively associated with blood pressure reactivity during a stressful interview. This is consistent with Powch and Houston’s (1996) finding that high hostile women (CM) had greater blood pressure react- ivity during a similar discussion task, and supports the hypothesis that hostility and reactivity
Dow
nloa
ded
by [
The
UC
Irv
ine
Lib
rari
es]
at 2
3:12
08
Nov
embe
r 20
14

684 K.G. LOW ETAL.
are linked in women. In addition, however, the hostility-reactivity relationship appears to be affected by both social desirability and personality-task interactions in the case of dia- stolic blood pressure. Like Helmers and Krantz (1997), we found that true high hostile women (low in social desirability/high in hostility) had significantly greater reactivity than other women, and that true low hostile women (low social desirability/low hostility) were the least reactive. This differs from research on men, which suggests that defensive hos- tility (high MC/high Cooke-Medley) is associated with greatest reactivity (Helmers et al., 1995; Helmers and Krantz, 1997).
In contrast to previous research, our data suggest that hostility is associated with HR reactivity and DBP in women, but not with SBP. Although many studies report changes in both DBP and SBP based on hostility or anger, almost all report greater associations with SBP reactivity. However, those studies which sample women appear to have somewhat different outcomes. In general, women appear to be greater heart rate and lower blood pres- sure responders than men (Stoney et al., 1988). Further, studies of women (Stone ef al., 1990; Suarez et al., 1995; Davis and Matthews, 1996; Helmers and Krantz, 1996; Powch and Houston, 1996; Davis, 1999) tend to report greater diastolic changes under stressful conditions. This may be the result of the fact that blood pressure reactivity is connected to female hormones both indirectly and directly. Studies report that exogenous administration of estrogens is associated with increased stroke volume due to direct effects on the myocar- dium (Walters and Lim, 1970), as well as indirect effects related to peripheral responses to catecholamines (Davis, 1999). Female hormones may therefore affect the hemodynamic responses to stress in studies such as ours (e.g. high HR, DBP responding).
Finally, some research has suggested that hemodynamic responses may vary depending on the subjective experience of the participant. Waldstein, Neumann, Burns and Maier report that threat appraisal, such as that done by hostile individuals, may be associated with greater negative affect and corresponding increased vascular resistance (with less cardiac output) (1998). In contrast, challenge appraisal (perceiving a task as demanding, but with- out negative affect) is associated with greater cardiac output. These authors assert that a controversial discussion such as the one in the present study is more likely to elicit threat appraisal, with associated vascular resistance (Waldstein et al., 1998). In a sample of women, the likelihood of interpersonal conflict resulting in threat appraisal seems particularly high. Future research should explore the differential hemodynamic effects (elevated DBP relative to SBP, for example) of different appraisals of stressors.
Consistent with our hypotheses, PAQ instruction type predicted reactivity, but only in the case of heart rate. In the case of DBP, PAQ instruction interacted with hostility such that only high hostile individuals responded with greater reactivity to the PAQ-inconsistent condition. This finding is consistent with and extends the findings of Davis and Matthews ( 1 996) in which instrumental individuals engaging in an expressive interaction had higher DBP reactivity. Interestingly, Davis and Matthews noted that women had greater DBP reactivity than men when instructions were mismatched. Similarly, the present study suggests that high hostile women who receive mismatched instructions have the greatest DBP changes.
Menstrual cycle was not associated with reactivity in this sample. This may be related to the fact that many women were on OCs, and that menstrual cycle phase was assessed by retrospective self-report. OCs, however, both independently and in combination with high social desirability, appear to have effects on systolic blood pressure in the present study. OC use has been associated with increased DBP and SBP in previous studies (Powch and Houston, 1996; Davis, 1999; Masson and Gilbert, 1999) and differences may be enhanced
Dow
nloa
ded
by [
The
UC
Irv
ine
Lib
rari
es]
at 2
3:12
08
Nov
embe
r 20
14

HOSTILITY. GENDER AND REACTIVITY 685
in high stress situations (Suarez et al., 1996). The present study suggests that OC users who have social evaluation concerns in a high stress situations are most reactive. It may be that concerns about social evaluation in socially stressful tasks are particularly salient pre- dictors of cardiovascular endpoints in women, and that OC use somehow potentiates the stress reaction through increased neuroendocrine responses.
There are a number of limitations to this preliminary research worth noting. First, the sample was relatively small, and although the statistical power was sufficient to detect a number of important effects, there may have been insufficient power to detect smaller effect sizes. Similarly, a number of analyses were run on a relatively small sample, increas- ing the possibility of Type I errors. In addition, the participants were largely white and middle-class, limiting the generalizability of the findings. Finally, there was only one physiological assessment during the stressful task and the interviewer and confederates were all women, and the interview ratings were done by the first author, a woman. Coder gender has affected hostility interview ratings in previous studies (e.g. Davidson et al., 1996), and may be a factor in the research reported here.
Finally, recent research has suggested that cigarette smoking, OC use and personality variables such as hostility may interact in stressful situations to produce greater reactivity (Davis, 1999; Masson and Gilbert, 1999). Although women in this study were instructed to refrain from smoking on the day of the testing, effects of smoking and OC use together have been found in smokers who are abstinent during testing. Future research should both control for smoking status, and confirm abstinence or non-smoking status through cotinine levels.
In sum, interview-based assessment of hostility appeared to be correlated with blood pressure reactivity during a social stressor in this sample of women. Person-task interaction as measured by instructions inconsistent or consistent with personality (PAQ) affected heart rate, and interacted with hostility to predict diastolic blood pressure changes. Further, oral contraceptive use increased reactivity both independently, and in combination with social desirability and hostility on a number of fronts. The role of the menstrual cycle and hormones use or replacement in combination with personality variables are important considerations for future research on cardiovascular reactivity in women.
Acknowledgements
The authors gratefully acknowledge the support of a Howard Hughes Medical Foundation Faculty Development grant from Bates College, and the comments of two anonymous reviewers.
References
Allen, M., Stoney, C. and Matthews, K. (1993) Hemodynamic adjustments to laboratory stress: Influence of
Arnstein, P., Buselli, E. and Rankin, S. (1996) Women and heart attacks: Prevention, diagnosis and care. Nurse
Barefoot, J., Larsen, S., von der Leith, L. and Schroll, M. (1995) Hostility and incidence of acute MI and mortality
Barefoot, J. and Lipkus, I. (1994) The assessment of anger and hostility. In: A.W. Siegman and T.W. Smith
Bums, J. , Friedman, R. and Katkin, E. (1992) Anger expression, hostility, anxiety and patterns of cardiac reactivity
gender and personality. Psychosomatic Medicine, 55,505-5 17.
Practitioner, 5,57-70.
in a sample of older Danish men and women. American Journal ofEpidemiology, 142,477484.
(Eds.), Anger, Hostility and the Hear? (pp. 4 3 6 6 ) . Hillsdale, NJ: Erlbaum.
to stress. Behavioral Medicine, 18, 7 1-78.
Dow
nloa
ded
by [
The
UC
Irv
ine
Lib
rari
es]
at 2
3:12
08
Nov
embe
r 20
14

686 K.G. LOW ETAL.
Buss, A. and Durkee, A. (1957) An inventory for assessing different kinds of hostility. Journal of Consulring
Carroll, D.. Davey Smith, G., Sheffield, D., Shipley, J. and Marmot, M. (1997) The relationship between socio- economic status, hostility, and blood pressure reactions to mental stress in men: Data from the Whitehall 11 study. Health Psychology, 16. 131-136.
Case, R.. Moss, A. and Case, N. (1989) Living alone after myocardial infarction. Journal of the American Medical Association, 267,515.
Cook, W. and Medley, D. (1954) Proposed hostility and pharisaic-virtue scales for the MMPI. Journal ofApplied Psychology. 38.414418.
Davidson, K., MacGregor, M., McDermott, N., Fquharson, J. and Chaplin, W. (1996) Coder gender and poten- tial for hostility ratings. Health Psychology, 15,298-302.
Davis, M. (1999) Oral contraceptive use and hemodynamic, lipid, and fibrinogen responses to smoking and stress in women. Health Psychology, 18, 122-130.
Davis, M. and Matthews, K. (1996) Do gender relevant characteristics determine cardiovascular reactivity? Match versus mismatch of traits and situations. Journal of Personality and Social Psychology, 71,527-535.
Dimsdale, J. (1993) Coronary heart disease in women: stress-induced biological responses. Annals of Behavioral Medicine, 15, 119-123.
Evanovski, C. (1997) Myocardial infarction. The number one killer of women. Critical Care Nursing Clinics of Nonh America, 9,489496.
Ewart, C., Jorgensen, R. and Kolodner, K. (1998) Sociotropic cognition moderates blood pressure response to interpersonal stress in high risk adolescent girls. International Journal of Psychophysiology, 28, 13 1-142.
Ewart, C. and Kolodner, K. (1994) Negative affect, gender, and expressive style predict elevated ambulatory blood pressure in adolescents. Journal of Personality and Social Psychology, 66,596405.
Ewart. C., Taylor, C., Kraemer, H. and Agras, S. (1991) High blood pressure and martial discord: Not being nasty matters more than being nice. Health Psychology, 10, 155-163.
Fichera, L. and Andreassi, J. (1998) Stress and personality as factors in women’s cardiovascular reactivity. International Journal of Psychophysiology, 28, 143-155.
Fontana, A. and McLaughlin, M. (1998) Coping and appraisal of daily stressors predict heart rate and blood pressure levels in young women. Behavioral Medicine, 24.5-16.
Frankenhauser, M. (1983) The sympathetic-adrenal and pituitary-adrenal response to challenge: Comparison between the sexes. In: T. Dembroski, T. Schmidt and G. Blumchen (Eds.), Biobehavioral Bases of Heart Disease (pp. 91-105). Basel, Switzerland: Karger.
Friedman, H.S. and Powell, L. (1994) The diagnosis and quantitative assessment of Type A behavior: Introduc- tion and description of the Videotaped Structured Interview. Integrative Psychiatry, 2, 122-136.
Hardy, J. and Smith, T. (1988) Cynical hostility and vulnerability to disease: Social support, life stress, and physiological response to conflict. Health Psychology, 7,447-459.
Hastrup, J. and Light, K. (1984) Sex differences in cardiovascular stress responses and modulation as a function of menstrual cycle phases. Journal of Psychosomatic Research, 28,475483.
Helmers, K. and Krantz, D. (1997) Defensive hostility, gender and cardiovascular levels and responses to stress. Annals of Behavioral Medicine, 18,246254.
Helmers, K., Krantz, D., Merz, C., Bairey, N., Klein, J., Kop, W., Gottdiener and Rozanski, A. (1995) Defensive hostility: Relationship to multiple markers of cardiac ischemia in patients with coronary disease. Healrh Psychology, 14,202-209.
Helmers, K., Posluszny, D. and Krantz, D. (1993) Associations of hostility and coronary artery disease: A review of studies. In: A. Siegman and T. Smith (as . ) , Anger, Hostility and the Heart (pp. 67-96). Hillsdale, NJ: Erlbaum.
Houston, B.K. and Vavak, C.R. (1991) Hostility: Developmental factors, psychosocial correlates and health behaviors. Health Psychology, 10.9-17.
Jamner, L., Shapiro, D., Goldstein, I. and Hug, R. (1991) Ambulatory blood pressure and heart rate in paramedics: Effects of cynical hostility and defensiveness. Psychosomatic Medicine, 53,393-406.
Lassner, J., Matthews, K. and Stoney, C. (1994) Are cardiovascular reactors to asocial stress also reactors to so- cial stress? Journal of Personality and Social Psychology, 6,69-77.
Larson, M. and Langer, A. (1997) Defensive hostility and anger expression: Relationship to additional heart rate reactivity during active coping. Psychophysiology, 34, 177-1 84.
Lawler, K., Harralson, T., Armstead, C. and Schmied, L. (1993) Gender and cardiovascular responses: What is the role of hostility? Journal of Psychosomatic Research, 37,603413.
Lemer. H. (1985) The dance of anger. NY: Harper and Row. Linden, W., Chambers, I., Maurice, J. and Lenz, J. (1993) Sex differences in social support. self-deception,
hostility, and ambulatory cardiovascular activity. Health Psychology, 12. 376380. Linden, W., Rutledge, T. and Con, A. (1998) A case for the usefulness of laboratory social stressors. Annals of
Behavioral Medicine, 20,3 10-3 16. Low, K.G., Fleisher, C., Colman, R., Dionne, A,, Case, G. and Legendre, S. (1998) Psychosocial variables, age. and
angiographically-determined coronary artery disease in women. Annals of Behavioral Medicine, 20,221-226. Low, K.G., Thoresen, C., Pattillo, J. and Fleischmann, N. (1993) Causal attributions and coronary heart disease in
women. Psychological Reports, 73,627436.
P~chology , 21,343-349.
Dow
nloa
ded
by [
The
UC
Irv
ine
Lib
rari
es]
at 2
3:12
08
Nov
embe
r 20
14

HOSTILITY. GENDER AND REACTlVITY 687
Low, K.G., Thoresen, C., Pattillo, C., King, A. and Jenkins, C. (1994) Anxiety, depression and heart disease in women. International Journal of Behavioral Medicine, 1,305-3 19.
Manuck, S. (1994) Cardiovascular reactivity in cardiovascular disease: “Once more unto the breach. fnterna- tional Journal of Behavioral Medicine, 1 , 6 3 1.
Masson, C. and Gilbert, G. (1999) Cardiovascular and mood responses to quantified doses of cigarette smoke in oral contraceptive users and nonusers. Journal of Behavioral Medicine, 22,589-605.
Powch, I.G. and Houston, B.K. (1996) Hostility, anger-in, and cardiovascular reactivity in white women. Health Psychology, 15,200-208.
Raikkonen, K., Matthews, K., Flory, J. and Owens, J. (1999) Effect of hostility on ambulatory blood pressure and mood during daily living in health adults. Health Psychology, 1 8 , 4 6 5 3 .
Rosenhan, R., Swann, G. and Carmelli, D. (1988) Definition, assessment, and evaluation of the Type A behavior pattern. In: B.K. Houston and C.R. Snyder (Eds.), Type A Behavior Pattern: Research, Theory and Interven- tion. NY: Wiley.
Siegman, A,, Anderson, R., Herbst, J., Boyle and Wilkinson, J.I. (1992) Dimensions of anger and hostility and cardiovascular reactivity in provoked and angered men. Journal of Behaviorul Medicine, 15, 257-272.
Smith, T. and Allred, K. (1989) Blood pressure responses during social interaction in high and low cynically hostile males. Journal of Behuvioral Medicine, 12, 135-143.
Smith, T., Limon, J., Gallo, L. and Ngu, L. (1996) Interpersonal control and cardiovascular reactivity: Goals, behavioral expression, and the moderating effects of sex. Journal of Personality and Social Psychology, 70, 1012-1024.
Spence, J., Helmreich, R. and Stapp. J. (1975) Ratings of self and peers on sex-role attributes and their relation to self-esteem and conceptions of masculinity and femininity. Journal of Personality and Social Psychology,
Steinberg, L. and Jorgensen, R. (1996) Assessing the MMPI-based CM Ho Scale: The implications of dimen- sionality. Journal of Personality and Social Psychology, 70, 1281-1287.
Stone, S., Dembroski, T., Costa, P. and MacDougall, J. (1990) Gender differences in cardiovascular reactivity. Journal of Behavioral Medicine. 13, 137-156.
Stoney, C., Davis, M. and Matthews, K. (1987) Sex differences in physiological responses to stress and in coronary heart disease: A causal link? Psychophysiology, 24, 127-1 3 1.
Stoney, C., Matthews, K., McDonald, R. and Johnson, C. (1988) Sex differences in lipid, lipoprotein, cardiovascular and neuroendocrine responses to acute stress. Psychophysiology, 25,645-65.
Suarez, E., Bates, M., Harralson, T., Tyrey, M. and McNeer, T. (1995) The joint effect ofhostility and oral contra- ceptives on cardiovascular responses in women. Society of Behavioral Medicine Annual Meeting, San Diego, CA, March.
Suarez, E., Harlan, E., Peoples, M. and Williams, R. (1993) Cardiovascular and emotional responses in women: The role of hostility and harassment. Health Psychology, 12,459468.
Suarez, E. and Williams, R. (1989) Situational determinants of cardiovascular and emotional reactivity in high and low hostile men. Psychosomatic Medicine, 51,404-418.
US. Bureau of Census, Statistical Abstracts of the U.S. (1994) ( 1 14th ed.). Washington, D.C. Waldstein, S., Neumann, S., Burns, H. and Maier, K. (1998) Role played interpersonal interaction: Ecological
Walters, W. and Lim, Y. (1970) Hernodynamic changes in women taking oral contraceptives. Journal of
32,29-39.
validity and cardiovascular reactivity. Annals of Behavioral Medicine, 20,302-309.
Obstetrics and Gynaecology, 77,1007-1012.
Dow
nloa
ded
by [
The
UC
Irv
ine
Lib
rari
es]
at 2
3:12
08
Nov
embe
r 20
14