Embed Size (px)
Citation preview
How to Perform a Transrectal UltrasoundExamination of the Lumbosacral and SacroiliacJoints
Erik H.J. Bergman, DVM, Diplomate ECAR, Associate Member LA-ECVDI*;Sarah M. Puchalski, DVM, Diplomate ACVR; andJean-Marie Denoix, DVM, PhD, Agrege, Associate Member LA-ECVDI
Authors’ addresses: Lingehoeve Veldstraat 3 Lienden 4033 AK, The Netherlands (Bergman); Uni-versity of California, Davis, One Shields Avenue, School of Veterinary Medicine, Davis, CA 95616(Puchalski); Ecole Nationale Veterinaire d’Alfort, 7 Avenue du General de Gaulle, 94700 Maisons-Alfort, France (Denoix); e-mail: [email protected]. *Corresponding and presenting author. © 2013AAEP.
1. Introduction
There is increasing interest in pathology of thelumbosacral and sacroiliac joints giving rise to stiff-ness and/or lameness and decreased performancein equine sports medicine.1–3 Pain arising fromthese regions can be problematic alone or in con-junction with lameness arising from other sites(thoracolumbar spine, hind limbs, or forelimbs).4
Localization of pain to this region is critically impor-tant through clinical assessment, diagnostic anes-thesia, and imaging.
In general, diagnostic imaging of the axial skele-ton and pelvis is difficult to perform and to interpret.Radiography is infrequently performed. To obtaingood-quality diagnostic radiographs, general anes-thesia, a high-output radiographic generator, andspecial techniques must be performed.5,6 Variationin the size and shape of the sacroiliac joints andsacral wings and caudal sacral osteophytes are com-mon7,8; special techniques for taking radiographs
have allowed for identification of these structuresand the inter-transverse joints.5 These authors urgecaution in the interpretation of lesions identified onradiography in the absence of other diagnostic im-aging and clinical examination. Nuclear scintigra-phy is an important component of work-up forsacroiliac region pain, but limitations exist. Sev-eral reports9,10 exist detailing the anatomy and tech-nique findings in normal horses11,12 and findings inlame horses.13 Patient motion, camera positioning,and muscle asymmetry can cause errors in interpre-tation. In normal horses, the appearance of thesacroiliac region varies with age but is generallysymmetric. In horses with sacroiliac problems, it ismore difficult to distinguish the tubera sacrale fromthe sacroiliac joint than in normal horses, and, inhorses with lameness, there is more asymmetrydetected.12,13
Techniques for percutaneous and transrectal ul-trasound examination have been described, and
AAEP PROCEEDINGS � Vol. 59 � 2013 229
DIAGNOSTIC IMAGING
NOTES
their use is increasingly common.2,14–19 Ultra-sound is very useful for the evaluation of the jointmargins and lumbosacral intervertebral disc.14
Similar to the radiographic anatomy of the region,variability exists in the appearance of the tuberasacrale, dorsal sacroiliac ligaments, thoracolumbarfasciae, and the lumbosacral joint.3,19 Artifacts ofacquisition and interpretation can occur with im-proper technique in the ultrasound examination,and knowledge of reference images and the regionalanatomy is paramount in accurate interpretation ofdiagnostic imaging studies of this region. All diag-nostic imaging techniques should also be interpretedin light of the anamnesis and the static and dynamicclinical examination.
The purpose of this “How-to” presentation is toprovide a review of the technique for transrectalultrasound with reference images and ultrasoundimages of examples of pathology of the lumbosacraljunction, lumbosacral intertransverse joints, andsacroiliac joints. This presentation will review im-aging findings in 231 horses presenting to Linge-hoeve Diergeneeskunde, Equine Referral Hospital,The Netherlands, for evaluation of stiffness or poorperformance in 2012.
2. Materials and Methods
The diagnostic imaging picture archiving and com-munications system (PACS) of Lingehoeve Dierge-neeskunde was searched for all horses undergoingtransrectal ultrasound during 2012. Age and breeddata were collected. All horses had a completeclinical evaluation for poor performance. After an-amnesis and static and dynamic examination, a per-cutaneous examination of the lumbar spine anda transrectal examination of the sacroiliac and lum-bosacral junction were performed.
Transrectal ultrasound examination was per-formed with the use of the technique described byDenoix.20 and illustrated in Fig. 1. A 5- to 10-MHzmicro-convex intra-operative ultrasound probe wasused per rectum. All horses were sedated with an�-2 agonist and restrained in stocks. The rectumwas cleaned, and copious lubricant was introducedinto the rectum. A stand-off pad was not used.Anti-spasmodic agents were used infrequently (ninehorses). The ultrasound images are oriented sothat ventral is to the bottom of the image displayscreen, and, when appropriate, cranial is to the left.
Technique
Step 1: Lumbosacral DiscTransrectally, the aorta and its bifurcation (nor-mally at the level of the fifth lumbar vertebra) canbe palpated. Place the ultrasound probe in a me-dian plane, caudal to the aorta and vena cava (bi-furcation normally at the level of L5). The L6 andS1 vertebrae can be recognized by the well-definedhyperechoic shadowing ventral margins, meetingat approximately a 140° to 150° angle. At this site,
the lumbosacral (LS) disc, the ventral longitudinalligament, and, occasionally, the dorsal longitudinalligament, can be identified (Fig. 2). At this loca-tion, scan the entire disc by moving the probe leftand right, maintaining a paramedian orientation ofthe probe.
Step 2: Intervertebral Disc and Vertebral Bodies ofL5–6 and L4–5From the LS disc, move the ultrasound probe ina cranial direction while maintaining the medianplane orientation. As the probe is moved forward,maintain visualization of the ventral vertebralmargin. The L5–6 disc is just dorsal and is usuallycaudal to the aortic bifurcation. The probe ismoved cranially to identify the L4–5 disc space dor-sal to the aorta.
Step 3: Lumbosacral Intervertebral ForamenIdentify the LS disc space. Move the probe in alateral direction, maintaining a paramedian imag-ing plane. As the probe is moved laterally, lookfor a smoothly demarcated defect in the bone surfacethat represents the intervertebral foramen. Once
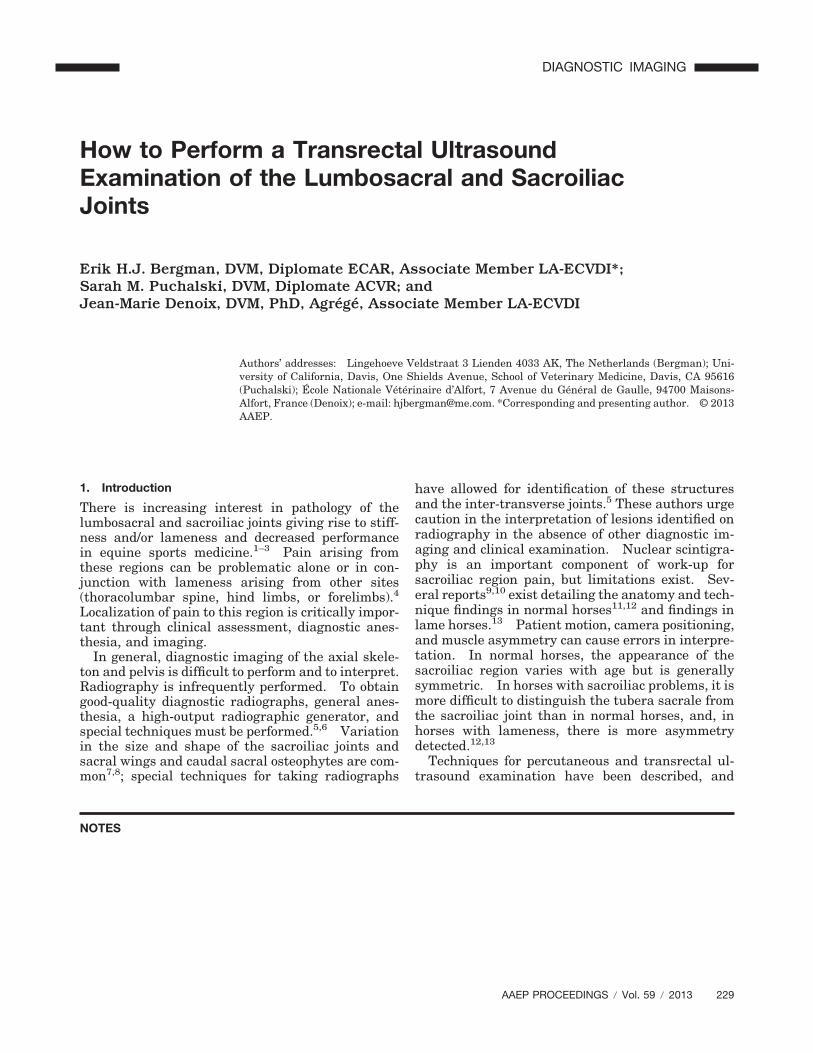
Fig. 1. Schematic drawing by Denoix of the ventral aspect of thelumbosacral region illustrates the stepwise procedure of trans-rectal evaluation of the lumbosacral and sacroiliac joints. Redlines indicate probe orientation. A, Sixth lumbar vertebra;B, sacrum; C, sciatic nerve; a, L6 nerve root; b, S1 nerveroot; 1, lumbosacral intervertebral joint; 2, L5–6 intervertebraljoint; 3, lumbosacral intervertebral foramen; 4, lumbosacral in-tertransverse joint; 5, S1–2 intervertebral foramen; 6, sacroiliacjoint; 7, direction of imaging the psoas minor tendon.
230 2013 � Vol. 59 � AAEP PROCEEDINGS
DIAGNOSTIC IMAGING
the defect is identified, look for the L6 nerve rootthat can be identified as a bundle of long, parallel,hyperechoic fibers. When the foramen is first iden-
tified, the imaging plane will be oblique to the nerve,and probe manipulation is needed to orient the ul-trasound probe parallel to the nerve root to char-
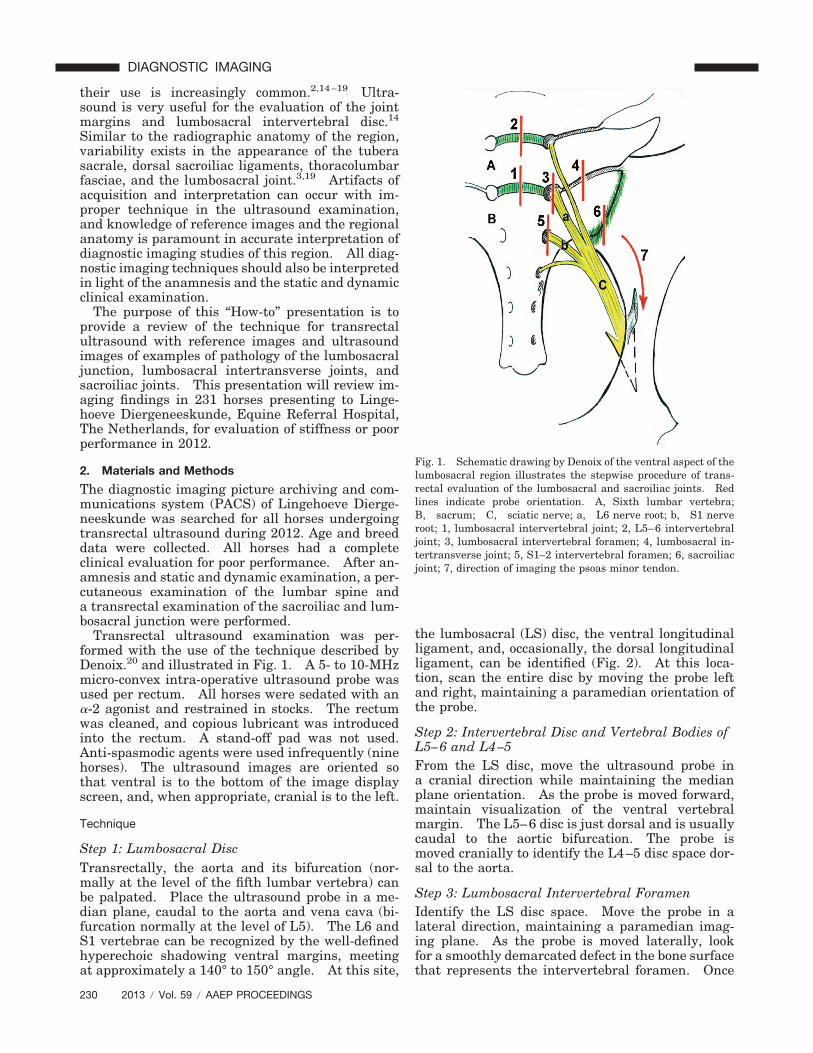
Fig. 2. These images depict the desired ultrasound image and probe position for evaluation of the lumbosacral joint, including the LSdisc, in a median plane (A1 and A2) and a transverse plane (B1 and B2). This represents Step 1 of the examination. Stars mark thespinal cord; X marks the ventral longitudinal ligament.
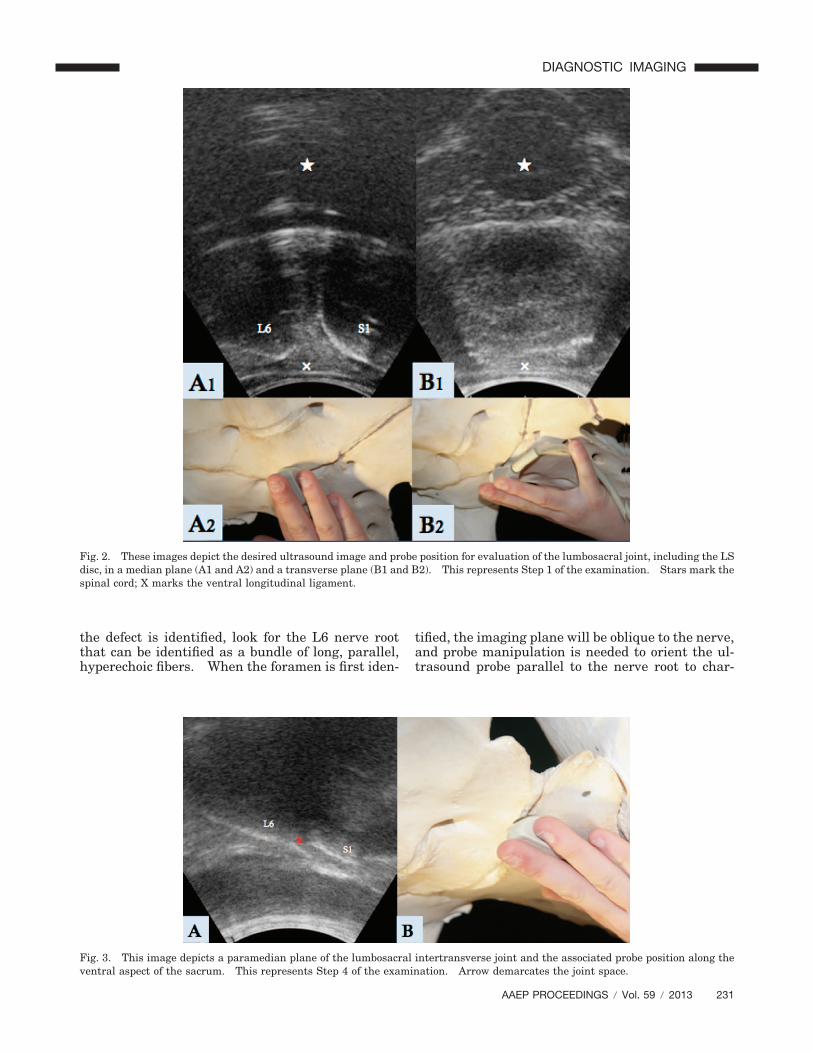
Fig. 3. This image depicts a paramedian plane of the lumbosacral intertransverse joint and the associated probe position along theventral aspect of the sacrum. This represents Step 4 of the examination. Arrow demarcates the joint space.
AAEP PROCEEDINGS � Vol. 59 � 2013 231
DIAGNOSTIC IMAGING
acterize this structure as it passes through theforamen.
Step 4: Lumbosacral Intervertebral IntertransverseJointsFrom the LS intervertebral foramen, continue tomove in a lateral direction to cross the LS inter-transverse joint. The joint is identified as a smalldefect in the bone surface (Fig. 3). Center the sur-face defect (joint space) in the ultrasound image andmove the probe in a medial to lateral direction whilemaintaining a paramedian probe orientation. Thisallows for evaluation of the joint margins.
Step 5: S1–2 Intervertebral ForamenReturn to the L6 nerve root at the LS intervertebralforamen (see Step 3). Move the entire probe in acaudal direction, maintaining the same probe orien-tation to identify the S1–2 intervertebral foramenand the S1 nerve root. The imaging characteristicsare similar to the LS intervertebral foramen and the
L6 nerve root. The operator must maintain aware-ness of their orientation and location relative tothe described landmarks in order to insure accurateidentification of these structures.
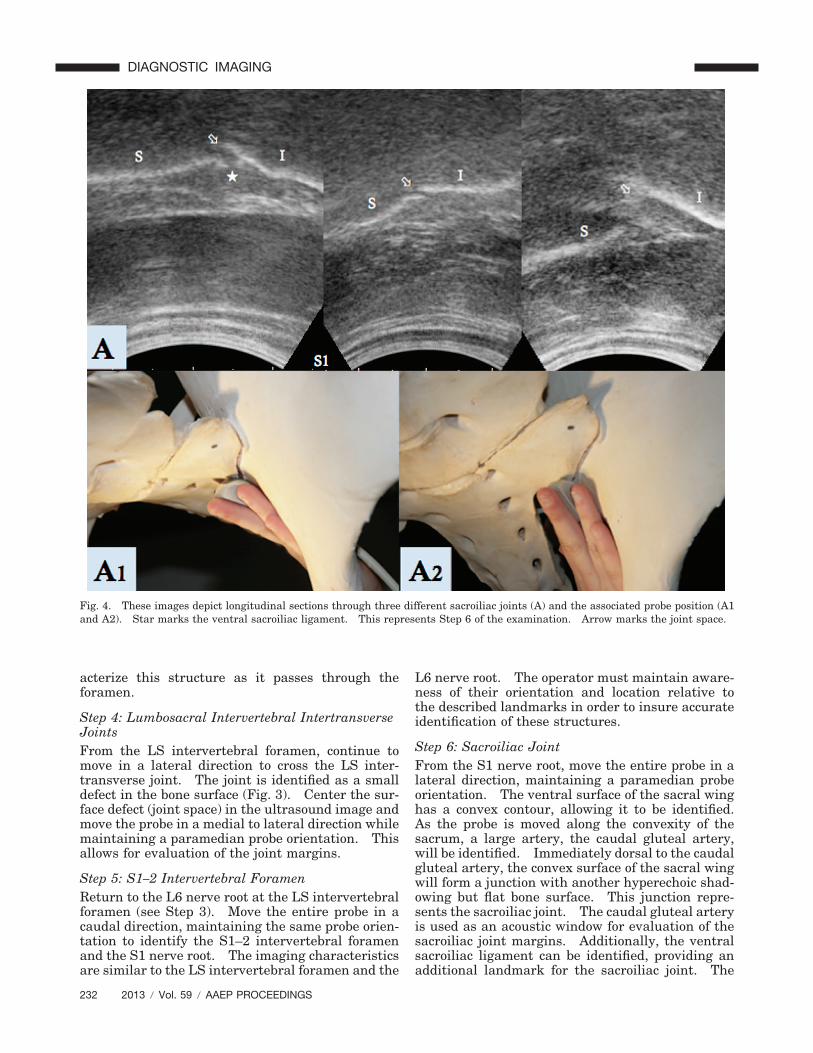
Step 6: Sacroiliac JointFrom the S1 nerve root, move the entire probe in alateral direction, maintaining a paramedian probeorientation. The ventral surface of the sacral winghas a convex contour, allowing it to be identified.As the probe is moved along the convexity of thesacrum, a large artery, the caudal gluteal artery,will be identified. Immediately dorsal to the caudalgluteal artery, the convex surface of the sacral wingwill form a junction with another hyperechoic shad-owing but flat bone surface. This junction repre-sents the sacroiliac joint. The caudal gluteal arteryis used as an acoustic window for evaluation of thesacroiliac joint margins. Additionally, the ventralsacroiliac ligament can be identified, providing anadditional landmark for the sacroiliac joint. The
Fig. 4. These images depict longitudinal sections through three different sacroiliac joints (A) and the associated probe position (A1and A2). Star marks the ventral sacroiliac ligament. This represents Step 6 of the examination. Arrow marks the joint space.
232 2013 � Vol. 59 � AAEP PROCEEDINGS
DIAGNOSTIC IMAGING
ventral sacroiliac ligament long axis is oblique to theparamedian imaging plane and perpendicular to thejoint margin; therefore, probe manipulation is re-quired to optimize images of this ligament.
Make longitudinal images of the caudomedialmargin of the sacroiliac joint including the ventralsacroiliac ligament (Fig. 4).
Optional: Step 7: Psoas Minor TendonMove the entire probe in a lateral and ventral direc-tion along the ventral concavity of the ilium. Thepsoas minor tendon is encountered and can beidentified by the typical imaging characteristics ofa tendon (long, parallel hyperechoic fibers). This
structure can be tracked by means of ultrasound toits attachment on the ilium.
Step 8Repeat for the contralateral side. Using the sameimaging landmarks identify the contralateral in-tervertebral forminae, lumbosacral intertransversejoint, sacroiliac joint, and ventral sacroiliac liga-ment. The psoas minor tendon and its insertion onthe ilium can also be visualized at this site.
Ultrasound images were reviewed on a dedicatedworkstation with DICOM viewing software (eFilm,Merge Healthcare), including digital calipers. Oneauthor reviewed the images of the lumbosacral disc,
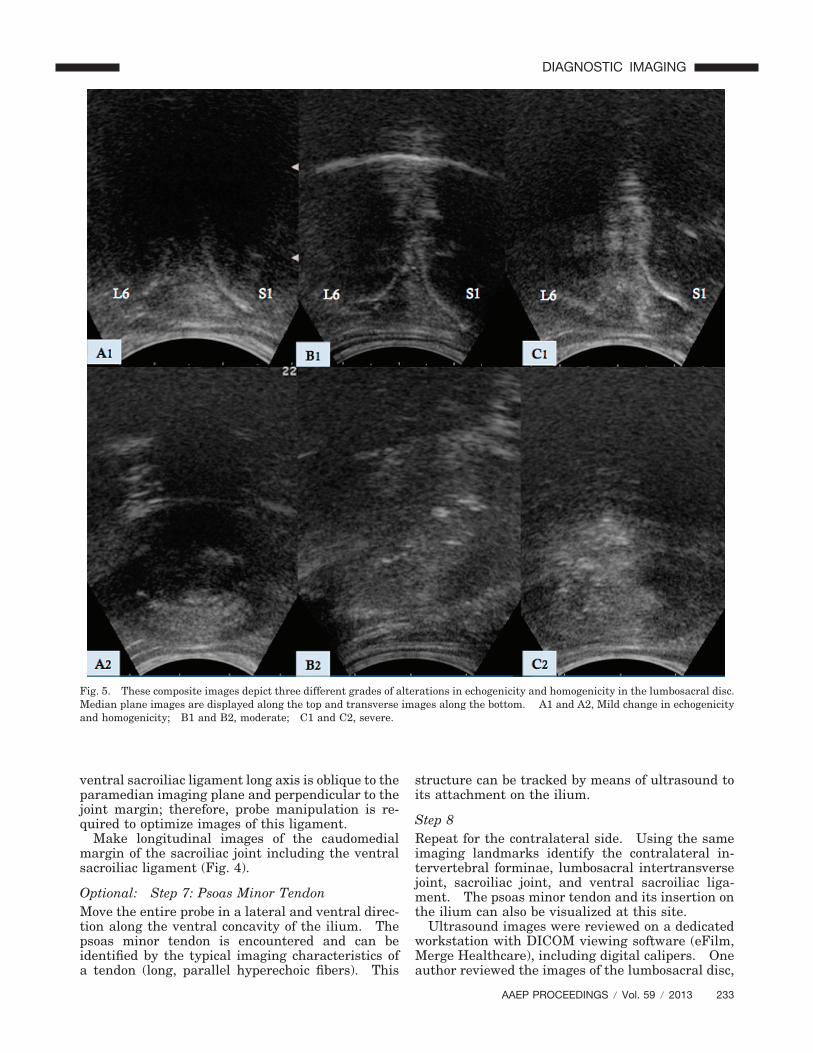
Fig. 5. These composite images depict three different grades of alterations in echogenicity and homogenicity in the lumbosacral disc.Median plane images are displayed along the top and transverse images along the bottom. A1 and A2, Mild change in echogenicityand homogenicity; B1 and B2, moderate; C1 and C2, severe.
AAEP PROCEEDINGS � Vol. 59 � 2013 233
DIAGNOSTIC IMAGING
intertransverse joint, and sacroiliac joint, retrospec-tively (H.J.B.). To grade the following structures,a subset of reference images were identified andgraded as normal, mild, moderate, or severe by twoauthors (H.J.B. and S.M.P.). On the basis of thesubset of reference images, the grading of the re-maining images was performed. The LS disc echo-genicity and homogeneity were considered together,and the disc was graded (normal, mild, moderate,severe). The LS disc grading was mild if the dischas localized regions of increased echogenicity orchanges from homogenous to mildly heterogeneous,moderate if there was increased echogenicity andthe disc appeared heterogeneous, and severe if thedisc was hyperechoic and heterogeneous (Fig. 5).The vertebral margins at the LS intervertebralspace were characterized for changes in shape andmargination (normal, mild, moderate, severe).They were considered mildly abnormal if there wasfocal irregularity or shape change, moderate if theirregular margination involved most but not all ofthe vertebral border, and severe if the margin wasirregular and there was shape change indicatingbone modeling (Fig. 6). The intervertebral spacewas measured from the caudoventral margin of L6to the cranioventral margin of S1. The degree ofventral bulging of the LS disc was measured in thefashion described by Nagy et al3 (Fig. 7). The leftand right sacroiliac joints were considered sepa-rately. Bone proliferation as identified by in-creased size and irregular margination at the jointmargin was characterized for the ilium and the sa-crum (normal, mild, moderate, and severe) (Fig. 8and Fig. 9). The ventral sacroiliac ligament wasnoted as normal or abnormal if it was thickened andheterogeneous). The lumbosacral intertransversejoints were also characterized as normal or abnor-
mal if proliferation was identified. Descriptive sta-tistics were calculated.
3. Results
Two hundred thirty-one horses were identified.The breed distribution included 199 Warmbloodhorses and 32 other breeds. The mean age was 8.8years (standard deviation � 3.7). The median age
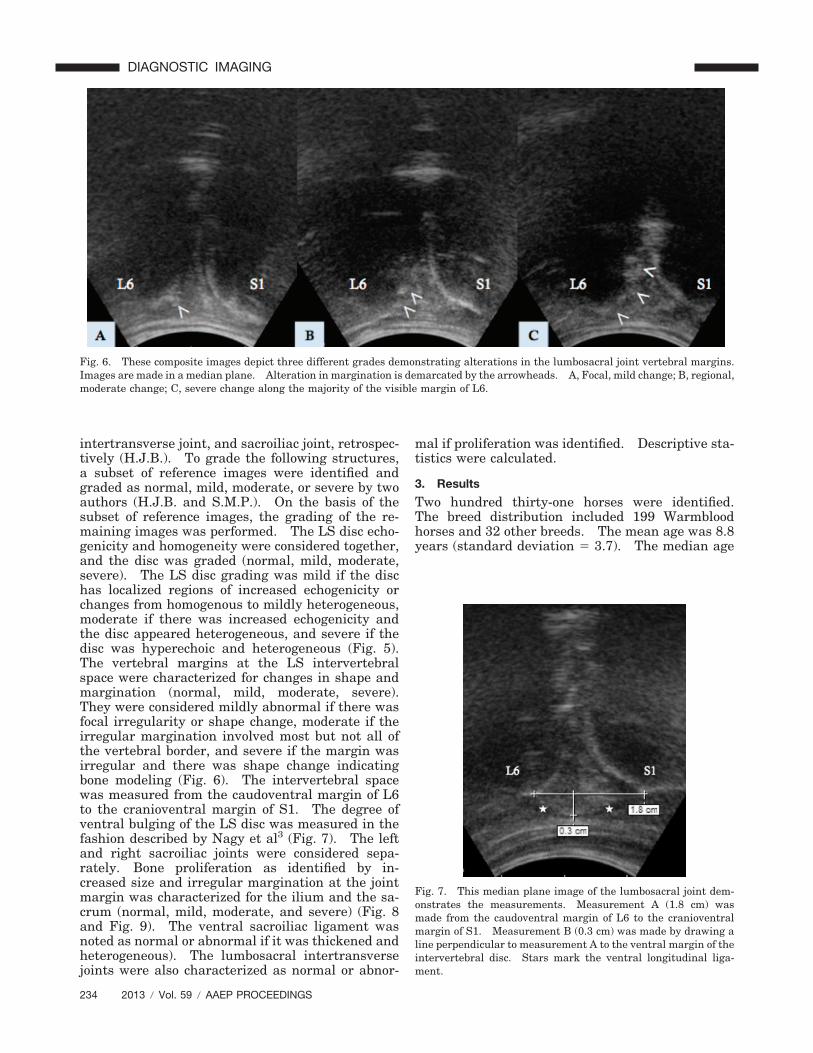
Fig. 6. These composite images depict three different grades demonstrating alterations in the lumbosacral joint vertebral margins.Images are made in a median plane. Alteration in margination is demarcated by the arrowheads. A, Focal, mild change; B, regional,moderate change; C, severe change along the majority of the visible margin of L6.
Fig. 7. This median plane image of the lumbosacral joint dem-onstrates the measurements. Measurement A (1.8 cm) wasmade from the caudoventral margin of L6 to the cranioventralmargin of S1. Measurement B (0.3 cm) was made by drawing aline perpendicular to measurement A to the ventral margin of theintervertebral disc. Stars mark the ventral longitudinal liga-ment.
234 2013 � Vol. 59 � AAEP PROCEEDINGS
DIAGNOSTIC IMAGING
was 8, with a range of 3 to 22 years. In 227 horses,poor performance was attributed at least in part toabnormalities of the lumbosacral or sacroiliac joints.Four horses were asymptomatic, and transrectal ul-trasound was performed as a part of pre-purchaseexamination.
Images of 228 lumbosacral disc spaces were re-viewed. There was sacralization of the LS spacein three horses (�1%). Three horses were excludedbecause diagnostic images were not saved to thePACS. Because of data presented previously byNagy and Dyson, normal and mild were considered
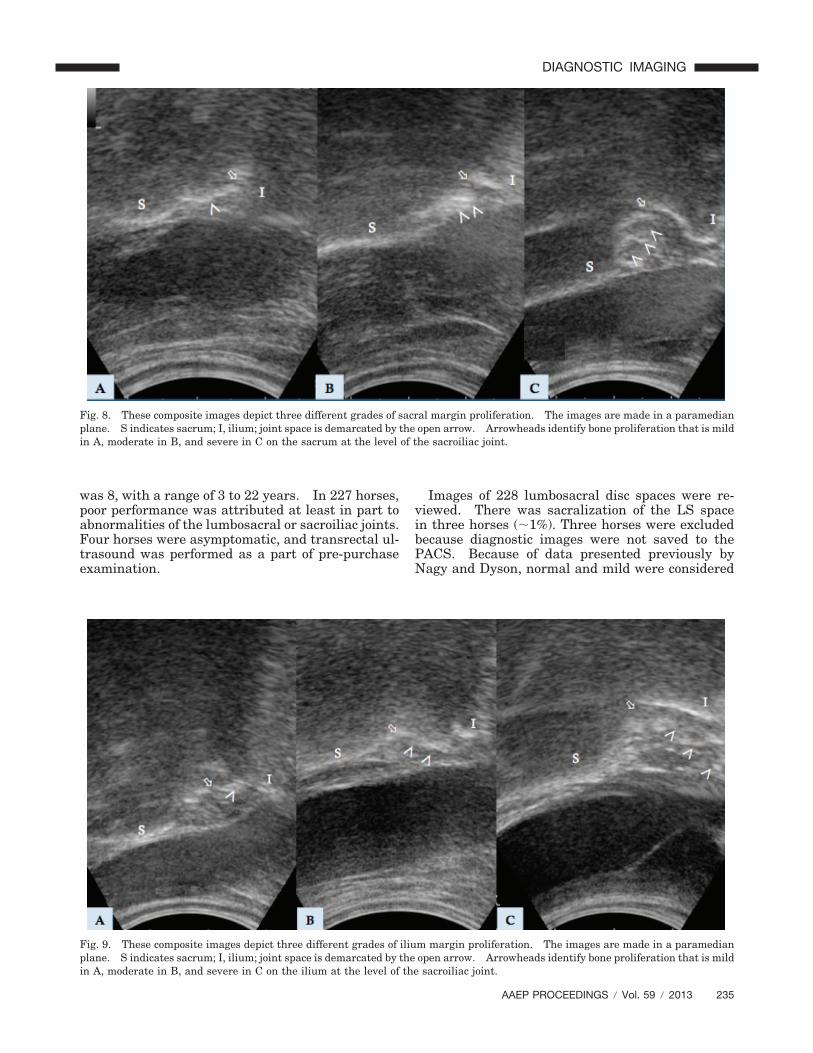
Fig. 8. These composite images depict three different grades of sacral margin proliferation. The images are made in a paramedianplane. S indicates sacrum; I, ilium; joint space is demarcated by the open arrow. Arrowheads identify bone proliferation that is mildin A, moderate in B, and severe in C on the sacrum at the level of the sacroiliac joint.
Fig. 9. These composite images depict three different grades of ilium margin proliferation. The images are made in a paramedianplane. S indicates sacrum; I, ilium; joint space is demarcated by the open arrow. Arrowheads identify bone proliferation that is mildin A, moderate in B, and severe in C on the ilium at the level of the sacroiliac joint.
AAEP PROCEEDINGS � Vol. 59 � 2013 235
DIAGNOSTIC IMAGING

together for the lumbosacral disc space descriptivecharacteristics. The results for ultrasound findingsof the lumbosacral disc and vertebral margins arepresented in Table 1 and Table 2, respectively.Measurements of the lumbosacral disc space andLS disc bulging are presented in Table 3. Abnor-malities of the lumbosacral intertransverse jointswere infrequent, with 38 of 462 (8%) identified.
Sacroiliac joint abnormalities were separated intojoint margin abnormalities on the ilium and on thesacrum; the results are presented in Table 4. Leftand right were considered separately, and, of thetotal abnormal sacroiliac joints (n � 173), abnormal-ities of the left were identified in 71 and abnormal-ities of the right were identified in 102. The ventralsacroiliac ligament was characterized as abnormal(thickened and heterogeneous) in 113 of 461 (24%)joints. Similar to the intertransverse joints, whenconsidering moderate and severe abnormalities ofthe sacroiliac joints, abnormalities of higher severitywere more frequently identified on the right 71 of113 than the 42 of 113.
4. Discussion
The objective of this report was to provide a reviewof the procedure for transrectal ultrasound evalua-tion technique of the lumbosacral and sacroiliacjoints and to provide reference images from a popu-lation of horses with clinical signs of lumbosacraland/or sacroiliac dysfunction. For each of the ana-tomic sites evaluated, this population of horses hadvariability in the severity of the abnormal findings.
It remains difficult to determine the clinical sig-nificance of alterations in echogenicity and margin-ation at the lumbosacral joint. In this group ofhorses, there was variability in the echogenicityof the LS disc and the margination of the endplatesof L6 and S1, but the majority of horses were cate-gorized as normal or mildly abnormal. A moderateproportion of horses were described as moderateto severely abnormal. Previous reports detailingthe ultrasound evaluation of this region in horses
without clinical signs of lumbosacral disease dem-onstrated that there can be variability in the echo-genicity and margination at this site, but markedchange was not present.3 Although it is impossibleto make a direct comparison of the two studies, itis likely that horses in this population with moder-ate or severe ultrasound changes have clinically sig-nificant imaging findings. Moderate to severechanges at the lumbosacral junction are identified inclinically abnormal horses. It must be underlinedthat subclinical manifestations with incidence onthe horse behavior, locomotion, or performance doexist.
Anomalous anatomy was rare in this population.Historic literature has discussed variability in theanatomic configuration of the pelvis and lumbosa-cral region,5 and sacralization of the lumbar verte-bra has been reported previously.2,5 Ultrasoundevaluation is limited to the ventral aspect of theosseous structures, and the identification of anoma-lies is dependent on the anomaly causing overallshape change of the vertebra or loss of the interver-tebral disc space, visible from the ventral surface.
Lumbosacral intertransverse joint pathology wasalso very uncommon in this population. Ultra-sound evaluation of these joints is limited to theventral joint margin. Postmortem evaluation ofThoroughbred racehorses showed that the entirepopulation had degenerative changes of the inter-transverse joints.21 The low incidence of inter-transverse joint pathology relative to this previousreport may be caused by the differences in patientpopulation or possibly the limitations of transrectalultrasound as compared with ex vivo postmortemevaluation. Lumbosacral intertransverse joint pa-thology has been observed with a higher prevalencein racing Standardbred trotters.
The sacroiliac joint abnormalities of the majorityof horses in this study showed normal or mildchanges. Nevertheless, slightly greater than one
Table 1. Lumbosacral Disc
Echogenicity Number (n � 225) Percentage
Normal 120186 82
Mild 66Moderate 35 16Severe 4 2
Table 2. Lumbosacral Disc Space Vertebral Margins
Vertebral Margin Number (n � 225) Percentage
Normal 146207 92
Mild 61Moderate 12 5Severe 6 3
Table 3. Lumbosacral Disc Space Measurements
LS Disc Measurement A Measurement B
Mean (SD) 15.4 mm (2.5) 1.7 mm (0.95)Median (range) 15 (8–22) 2 (0–3)
Table 4. Sacroiliac Joint Margin Bone Proliferation
Number Percentage
Sacrum (n � 462) Normal 187289 63
Mild 102Moderate 120 26Severe 53 11
Ilium (n � 462) Normal 136311 67
Mild 175Moderate 119 26Severe 32 7
236 2013 � Vol. 59 � AAEP PROCEEDINGS
DIAGNOSTIC IMAGING

third of horses in this group with clinical signs hadmoderate to severe sacroiliac changes. Ultrasoundevaluation of the joint margins allows for the iden-tification of periarticular proliferative new bone(osteophytes), as expected in this or any other jointwith joint disease. Variability in the appearanceof the sacroiliac joint is expected in normal popula-tions; however, many publications agree that abnor-malities of increasing severity are increasinglylikely to be clinically significant.6,10,12,18,20 Scinti-graphic abnormalities are often identified in horseswith hind limb lameness; however, care should betaken in the interpretation of these findings becauseoverlap exists between horses with sacroiliac dis-ease confirmed by diagnostic anesthesia and horseswith other causes of hind limb lameness.4,12,13
It is likely that a similar corollary exists for ultra-sound evaluation of the same region, whereby over-lap exists between clinically significant andclinically silent pathologic change. However, sac-roiliac pathologic change has been a common findingin postmortem studies, which may indicate that thistruly represents a common pathology.7,8,21 By con-trast, it is also important to recall that ultrasound ofthe caudomedial margin of the sacroiliac joint mayrepresent a small window relative to overall size ofthe joint and associated soft tissue structures.
In summary, transrectal ultrasound of the sacro-iliac and lumbosacral joints is a key component theevaluation of horses with lumbosacral and sacroiliacstiffness or poor performance. The technique re-quires a knowledge of the anatomy, the ability toperform ultrasound, good equipment, and knowl-edge surrounding the identification and interpre-tation of abnormalities. Transrectal ultrasoundshould be used in conjunction with anamnesis, com-plete clinical examination, and percutaneous ultra-sound evaluation of the lumbar facet joints. Thistechnique can be used to guide diagnostic and treat-ment decisions. Although it is a potentially usefultechnique for prepurchase examination evaluation,caution should be exercised in image interpretationuntil a broader body of knowledge exists.
References1. Jeffcott LB, Dalin G, et al. Sacroiliac lesions as a cause of
chronic poor performance in competitive horses. Equine Vet J1985;17:111–118.
2. Denoix JM. Diagnosis of Sacroiliac Lesions in Horses. Essen,Germany: Equitana XVI-Tagung; 2005.
3. Nagy A, Dyson S, et al. Ultrasonographic findings in thelumbosacral joint of 43 horses with no clinical signs of backpain or hindlimb lameness. Vet Radiol Ultrasound 2010;51:533–539.
4. Dyson S, Murray R. Pain associated with the sacroiliac jointregion: a clinical study of 74 horses. Equine Vet J 2003;35:240–245.
5. Gorgas D, Kircher P, et al. Radiographic technique andanatomy of the equine sacroiliac region. Vet Radiol Ultra-sound 2007;48:501–506.
6. Gorgas D, Luder P, et al. Scintigraphic and radiographicappearance of the sacroiliac region in horses with gait abnor-malities or poor performance. Vet Radiol Ultrasound 2009;50:208–214.
7. Dalin G, Jeffcott LB. Sacroiliac joint of the horse, 1: grossmorphology. Anat Histol Embryol 1986;15:80–94.
8. Dalin G, Jeffcott LB. Sacroiliac joint of the horse, 2: mor-phometric features. Anat Histol Embryol 1986;15:97–107.
9. Erichsen C, Berger M, et al. The scintigraphic anatomy ofthe equine sacroiliac joint. Vet Radiol Ultrasound 2002;43:287–292.
10. Erichsen C, Eksell P, et al. Scintigraphy of the sacroiliacjoint region in asymptomatic riding horses: scintigraphicappearance and evaluation of method. Vet Radiol Ultrasound2003;44:699–706.
11. Feige K, Schwarzwald C, et al. Esophageal obstruction inhorses: a retrospective study of 34 cases. Can Vet J 2000;41:207–210.
12. Dyson S, Murray R, et al. The sacroiliac joints: evaluationusing nuclear scintigraphy, part 2: lame horses. Equine Vet J2003;35:233–239.
13. Dyson S, Murray R, et al. The sacroiliac joints: evaluationusing nuclear scintigraphy, part 1: the normal horse. EquineVet J 2003;35:226–232.
14. Denoix JM. Spinal biomechanics and functional anatomy:back problems. Vet Clin North Am Equine Pract 1999;15:27–60.
15. Tomlinson JE, Sage AM, et al. Detailed ultrasonographicmapping of the pelvis in clinically normal horses and ponies.Am J Vet Res 2001;62:1768–1775.
16. Tomlinson JE, Sage AM, et al. Ultrasonographic abnormal-ities detected in the sacroiliac area in twenty cases of upperhindlimb lameness. Equine Vet J 2003;35:48–54.
17. Kersten AA, Edinger J. Ultrasonographic examination ofthe equine sacroiliac region. Equine Vet J 2004;36:602–608.
18. Denoix JM, Coudry V. Diagnosis and Treatment of Lumbo-sacral and Sacroiliac Pain in Horses. Essen, Germany: XVITagung uber Pferdekrankheiten; 2005.
19. Engeli E, Yeager AE, et al. Ultrasonographic technique andnormal anatomic features of the sacroiliac region in horses.Vet Radiol Ultrasound 2006;47:391–403.
20. Denoix JM, Audigie F, et al. Review of Diagnosis and Treat-ment of Lumbosacral Pain in Sport and Race Horses, inProceedings. Am Assoc Equine Pract 2005;51:366–373.
21. Haussler KK, Stover SM, et al. Pathologic changes in thelumbosacral vertebrae and pelvis in Thoroughbred race-horses. Am J Vet Res 1999;60:143–153.
AAEP PROCEEDINGS � Vol. 59 � 2013 237
DIAGNOSTIC IMAGING