Embed Size (px)
Citation preview

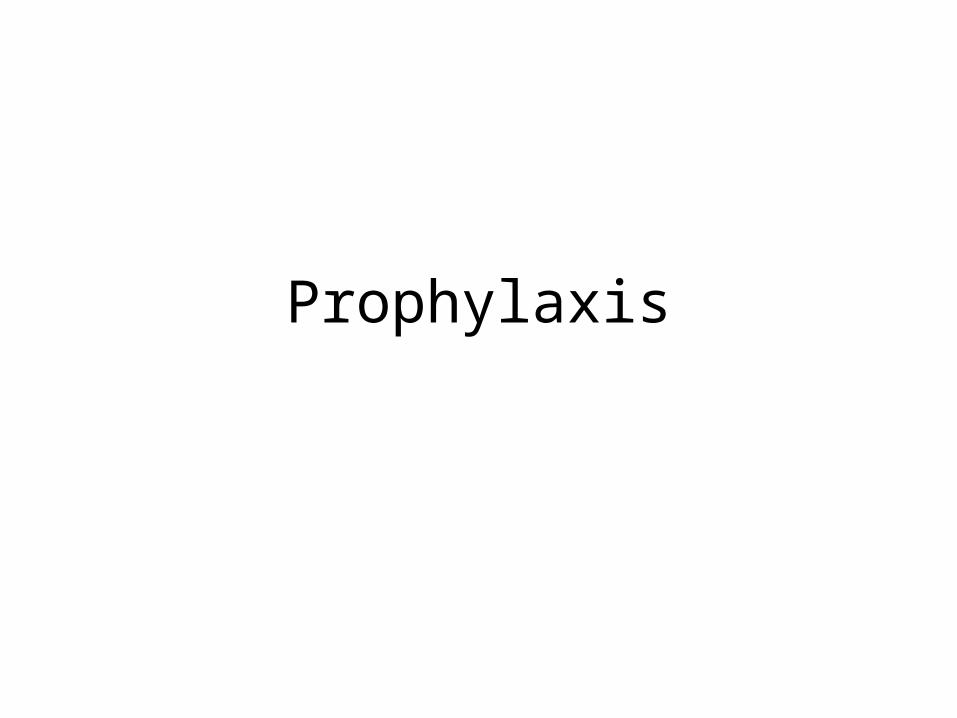
Prophylaxis
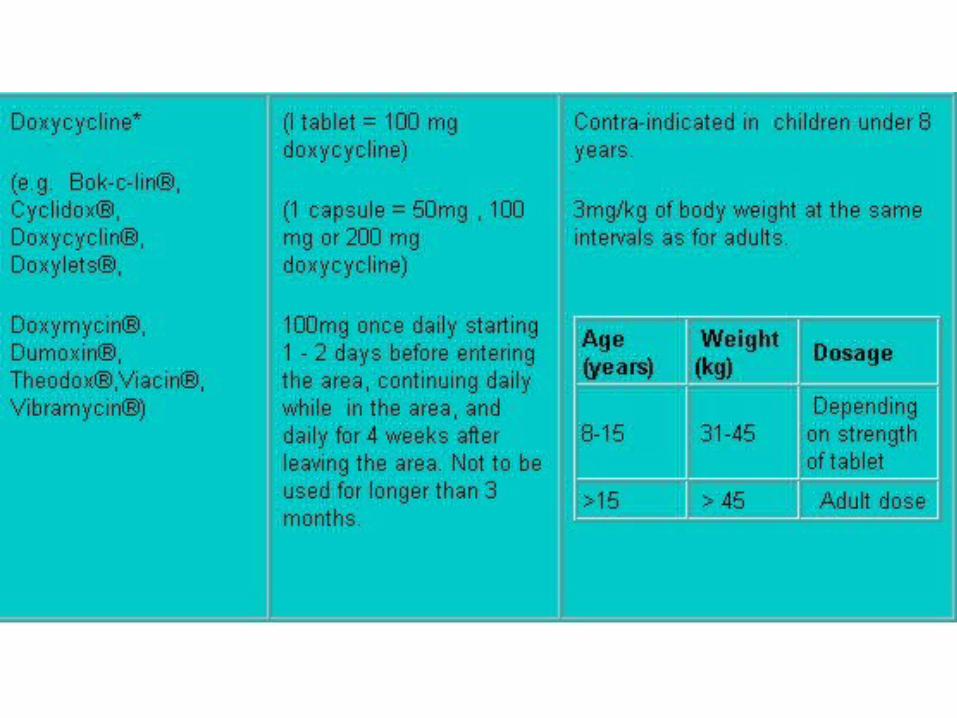

Prevention and Treatment of Malaria
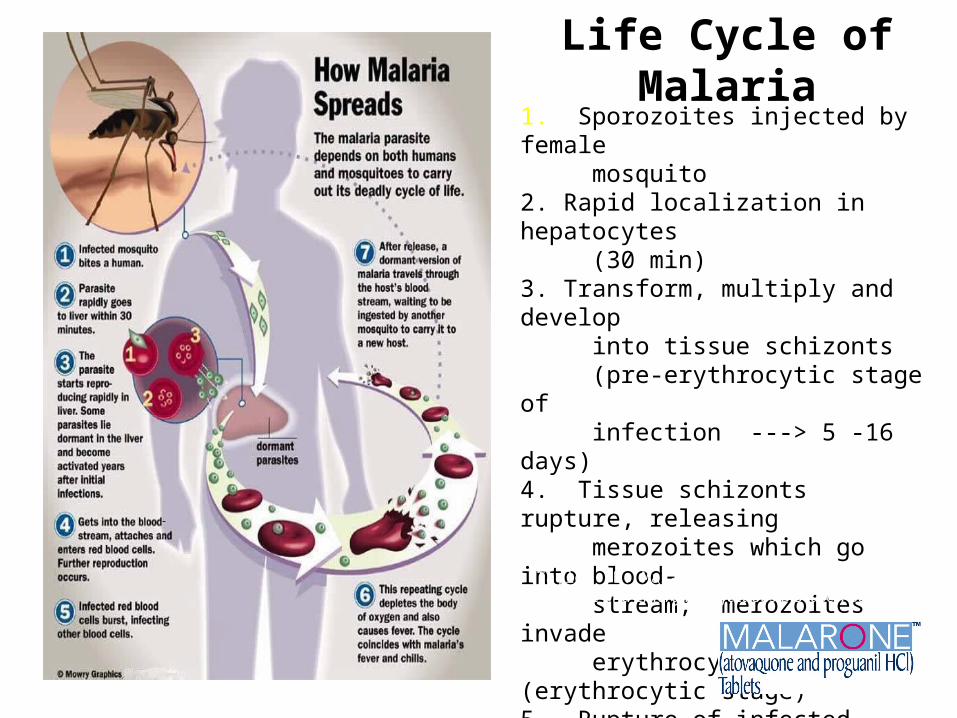
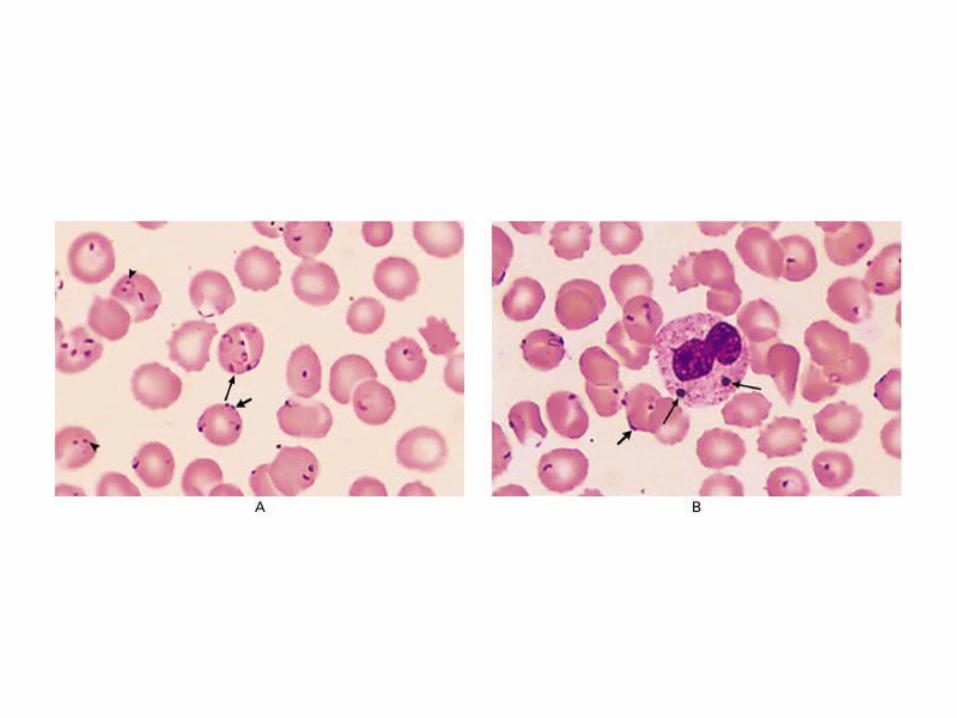
Life Cycle of Malaria1. Sporozoites injected by female mosquito2. Rapid localization in hepatocytes (30 min)3. Transform, multiply and develop into tissue schizonts (pre-erythrocytic stage of infection ---> 5 -16 days)4. Tissue schizonts rupture, releasing merozoites which go into blood- stream; merozoites invade erythrocytes (erythrocytic stage)5. Rupture of infected erythrocytes - febrile attacks every 48 hours6. Repeating cycle7. Continued transmission Taylor TE. Malaria. In: Hunter’s Tropical Medicine and
Emerging Infectious Diseases, 8th ed., 2000.
MALARONETM
Precautions:MALARONE has not been evaluated for the treatment of cerebral malaria or other severe manifestations of complicated malaria, including hyperparasitemia, pulmonary edema, or renal failure. Patients with severe malaria are not candidates for oral therapy.
MALARONETM Dosage and Administration (cont)
• MALARONE should not be used for malaria prophylaxis in patients with severe renal impairment (creatinine clearance <30 mL/min).
• Alternatives to MALARONE should be recommended for treatment of acute P. falciparum malaria whenever possible in patients with severe renal impairment.
• No dosage adjustments are needed in patients with mild to moderate renal impairment.
MALARONETM Dosage in Prevention of Malaria
One dose daily Start 1-2 days before entering endemic area, continue daily during stay & for 7 days after return
Adults: One MALARONE Tablet (adult strength = 250 mg atovaquone/100 mg proguanil hydrochloride) per day.
Pediatric Patients: Pediatric dosage for prevention based on body weight (see pediatric dosing slide)
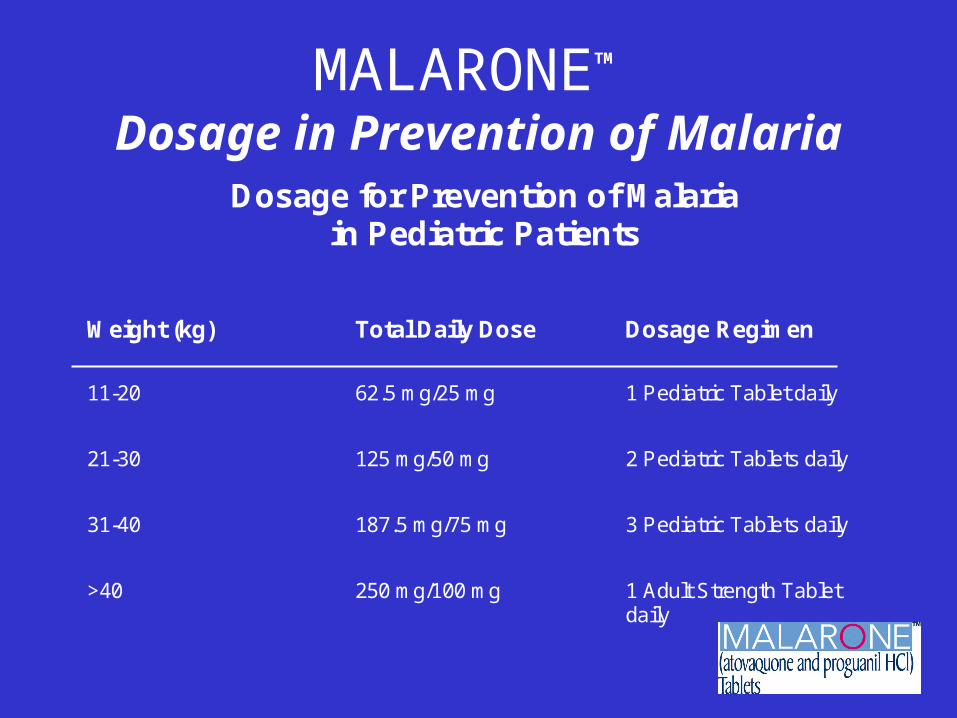
MALARONETM Dosage in Prevention of Malaria
Dosage for Prevention of Malariain Pediatric Patients
Weight (kg) Total Daily Dose Dosage Regimen
11-20 62.5 mg/25 mg 1 Pediatric Tablet daily
21-30 125 mg/50 mg 2 Pediatric Tablets daily
31-40 187.5 mg/75 mg 3 Pediatric Tablets daily
>40 250 mg/100 mg 1 Adult Strength Tabletdaily
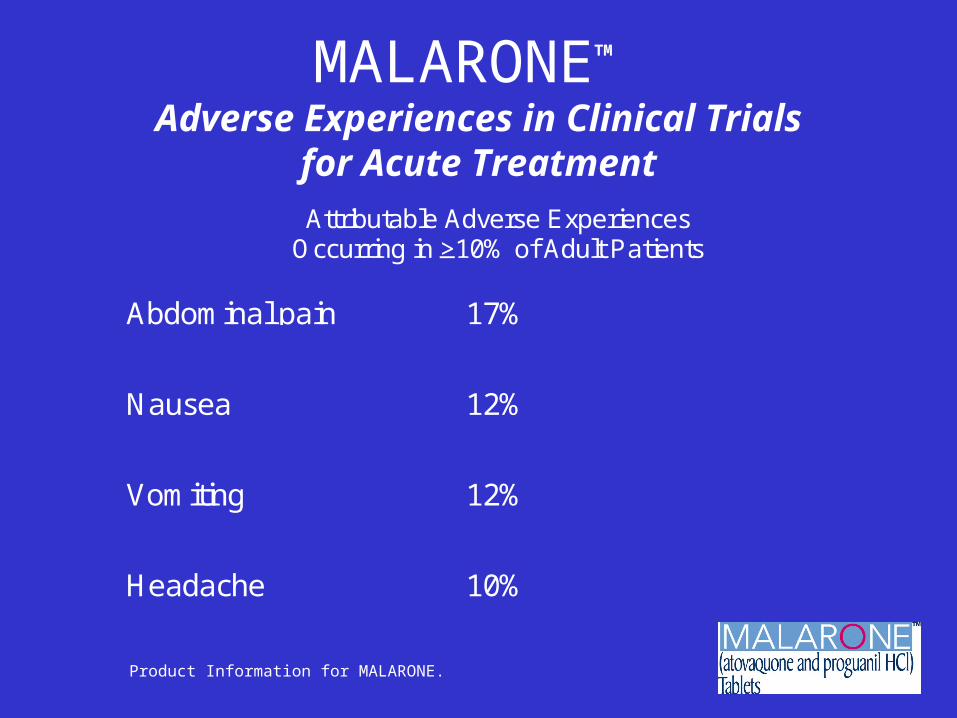
MALARONETM Adverse Experiences in Clinical Trials
for Acute TreatmentAttributable Adverse Experiences
Occurring in >10% of Adult Patients
Abdominal pain 17%
Nausea 12%
Vomiting 12%
Headache 10%
Product Information for MALARONE.
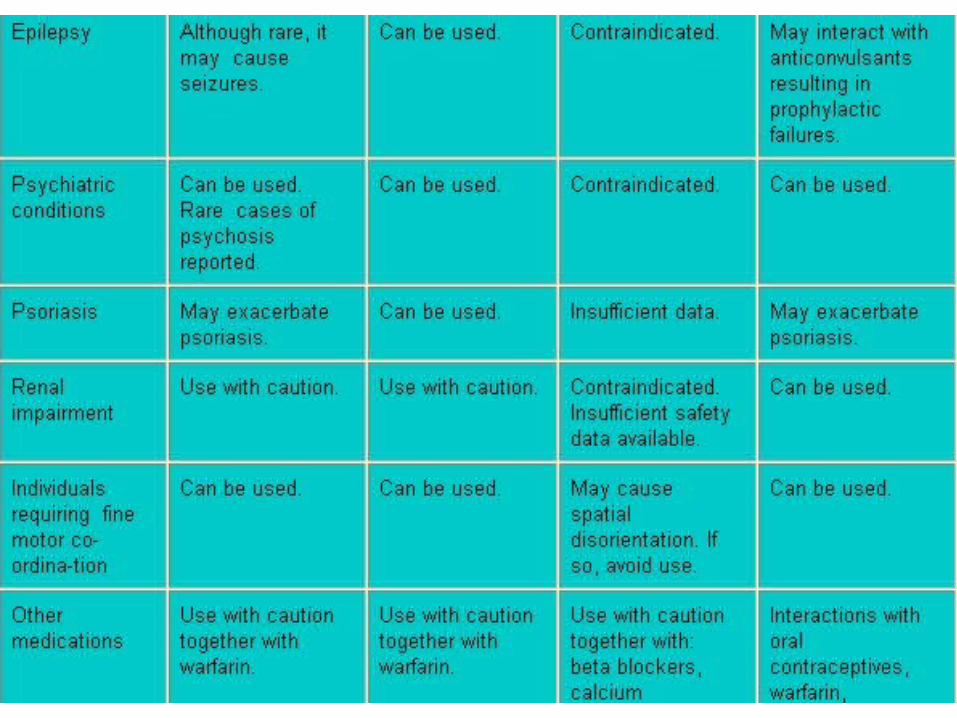
CHOICE OF DRUG(S) ACCORDING TO PATIENT
FACTORS

Symptoms + Treatment
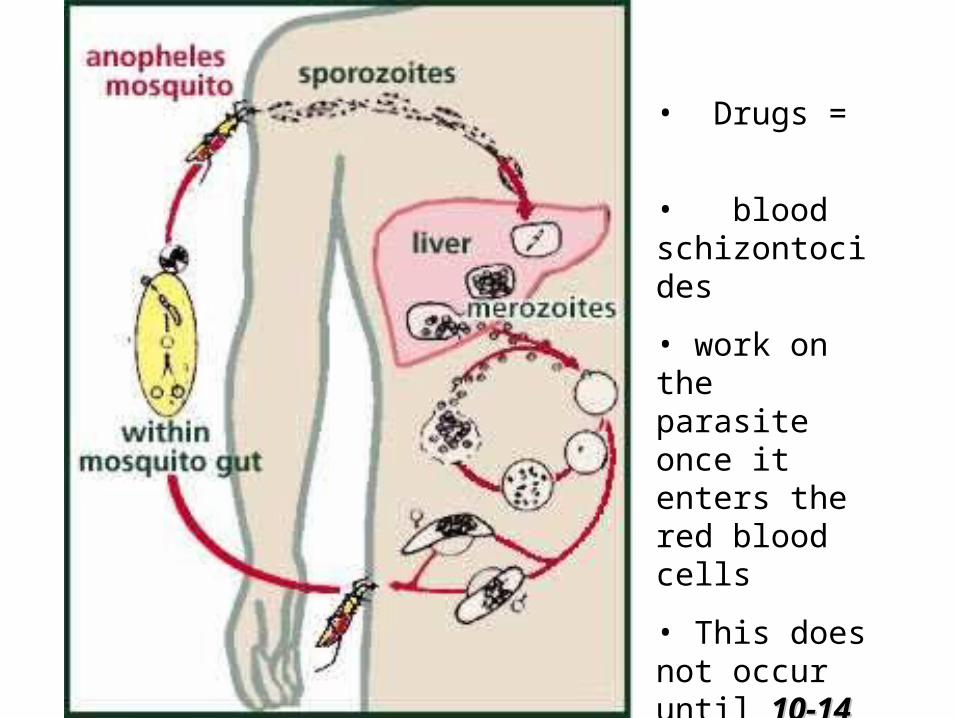
• Drugs =
• blood schizontocides
• work on the parasite once it enters the red blood cells
• This does not occur until 10-10-14 days14 days after being bitten by an infected mosquito
Symptoms of malaria
• Fever is most common, but may be absent in some cases. "Flu-like" symptoms are particularly common presenting symptoms of malaria. Some of the following symptoms may also occur; rigors, headache, sweating, tiredness, myalgia, abdominal pain, diarrhoea, loss of appetite, nausea and vomiting, and cough.
• In young children malaria may present with fever, lethargy, poor feeding, vomiting, diarrhoea and cough.
Presentation of P. falciparum malaria
• is very variable and may mimic many other diseases and (vice versa) including influenza, hepatitis, meningitis, septicaemia, typhoid, tick bite fever, gastroenteritis, viral haemorrhagic fever, trypanosomiasis, HIV seroconversion illness, urinary tract infection and relapsing fever.
SEVERE AND COMPLICATED MALARIA
• Parasitaemia: > 5%
• Hb: <6 g/dl
• spontaneous hypoglycaemia
• major organ dysfunction – particularly cerebral malaria.
Symptoms of severeMALARIA
• impaired consciousness • extreme weakness and jaundice. • cerebral malaria, defined as unrousable coma not
attributable to any other cause • generalised seizures• hyperpyrexia• renal failure• hypoglycaemia• fluid, electrolyte and acid-base disturbance• disseminated intravascular coagulation
Symptoms of severeMALARIA
• pulmonary oedema and adult respiratory distress syndrome
• circulatory collapse and shock ("algid malaria")
• hyperparasitaemia• malarial haemoglobinuria• hepatic impairment• secondary bacterial infections• normocytic anaemia
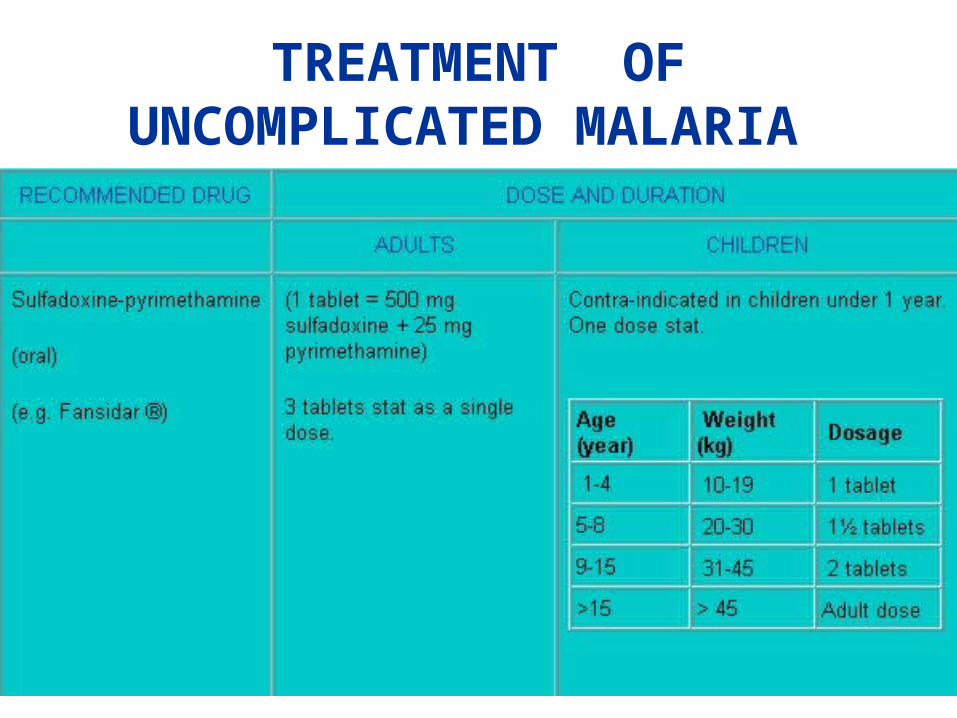
TREATMENT OF UNCOMPLICATED MALARIA
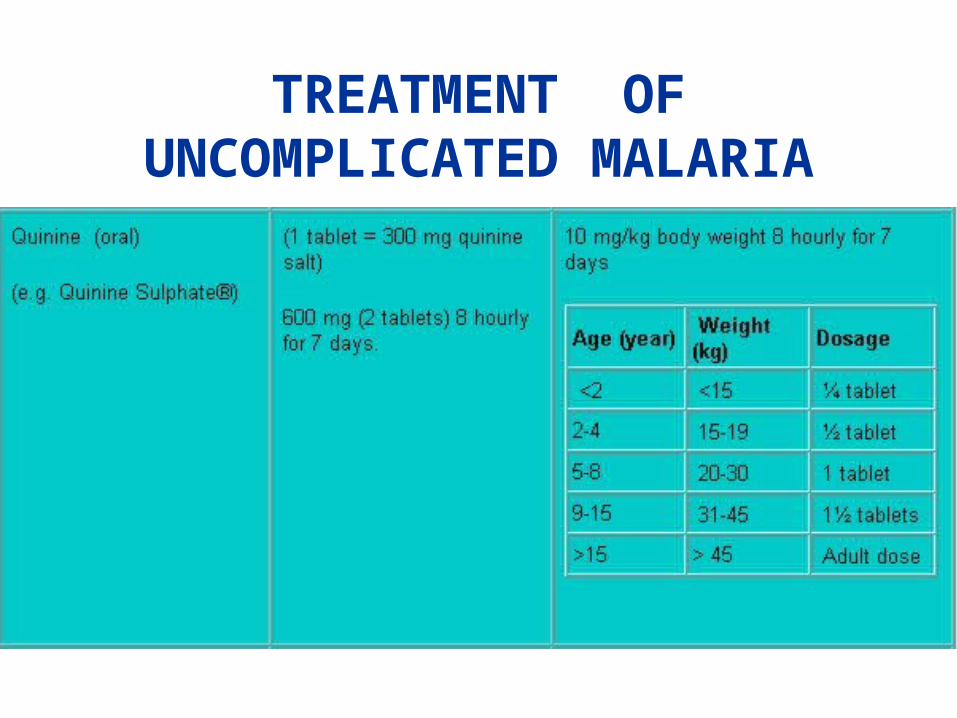
TREATMENT OF UNCOMPLICATED MALARIA
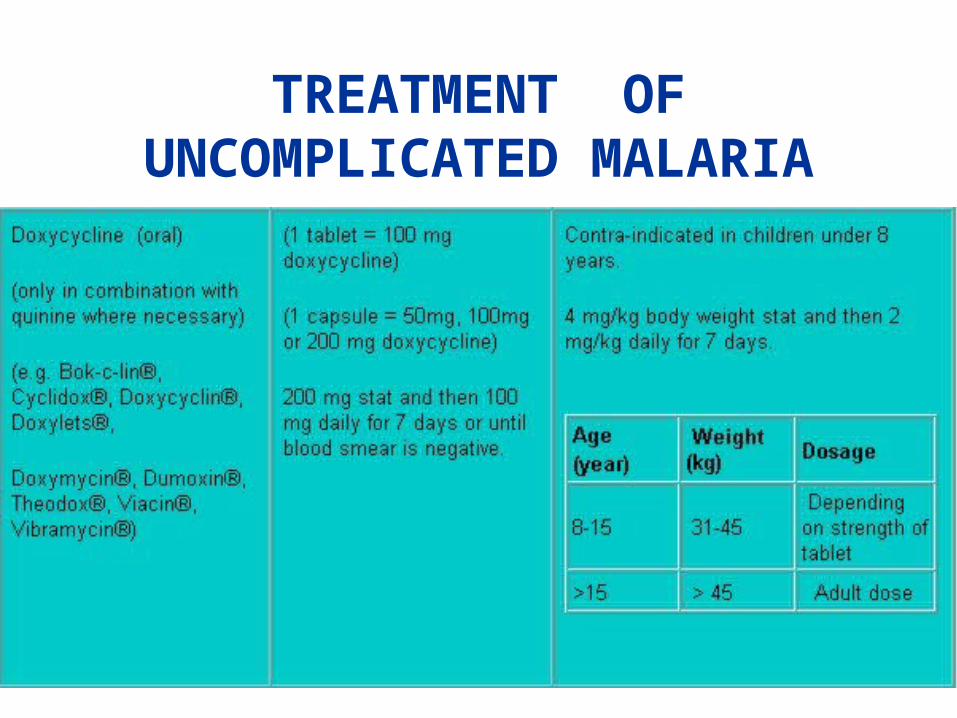
TREATMENT OF UNCOMPLICATED MALARIA
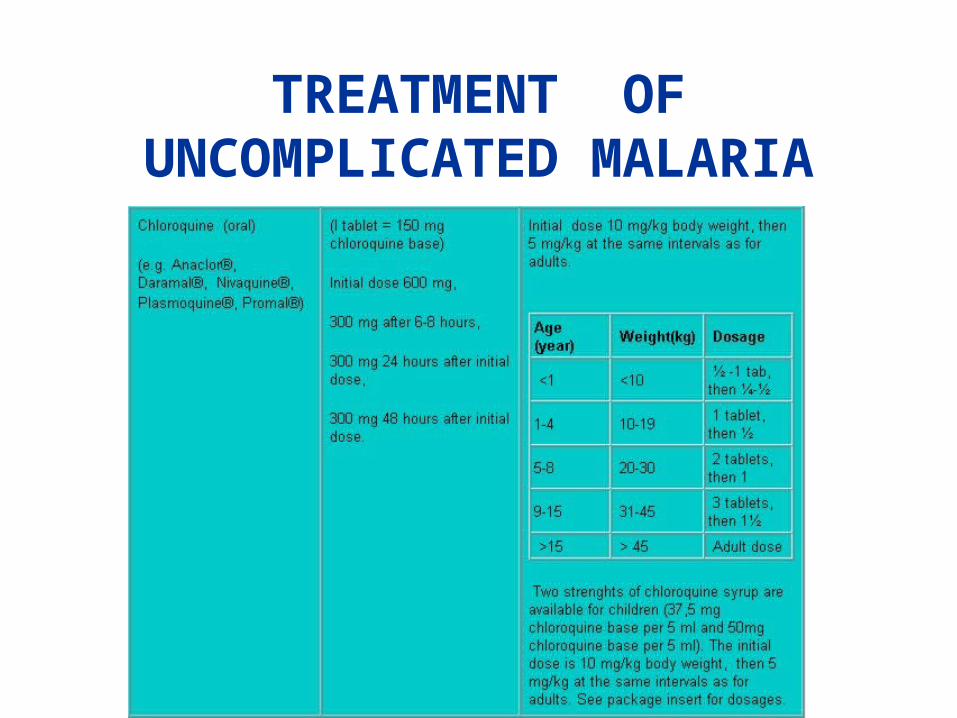
TREATMENT OF UNCOMPLICATED MALARIA
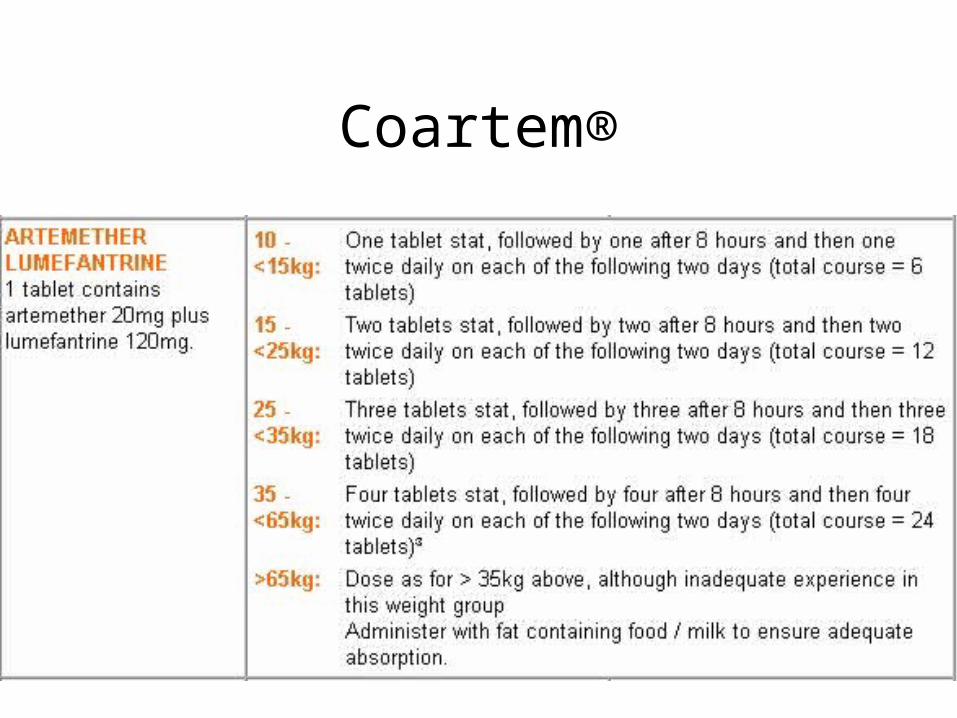
Coartem®
Coartem®
• ** Current artemether-lumefantrine (Coartem®) registration in South Africa indicates use only for treatment of uncomplicated malaria in patients < 65kg body weight, living in malaria endemic areas.
Coartem®
• Artemisinin was originally developed in 1972 in China from the plant Artemisia annua L (sweet wormwood). It is the active ingredient in qinghao, a Chinese herbal tea that have been used for 150 years to treat malaria and haemorrhoids.
Coartem®
• artemether + lumefantrine • traetment of uncomplicated malaria caused
by the P.falciparum strain• Coartem® is the fastest acting anti-malarial
therapy and has demonstrated cure rates of higher than 95%.
• cleared the parasites causing Malaria in less than 48 hours, more rapidly than any other non-artemesinin anti-malarial
Coartem®
• Coartem® has been approved in South Africa as a six-dose course of treatment administered over only 3 days.
• remarkable efficacy and safety profile
• extremely well tolerated
• treatment not prophylaxis
• for emergency standby treatment
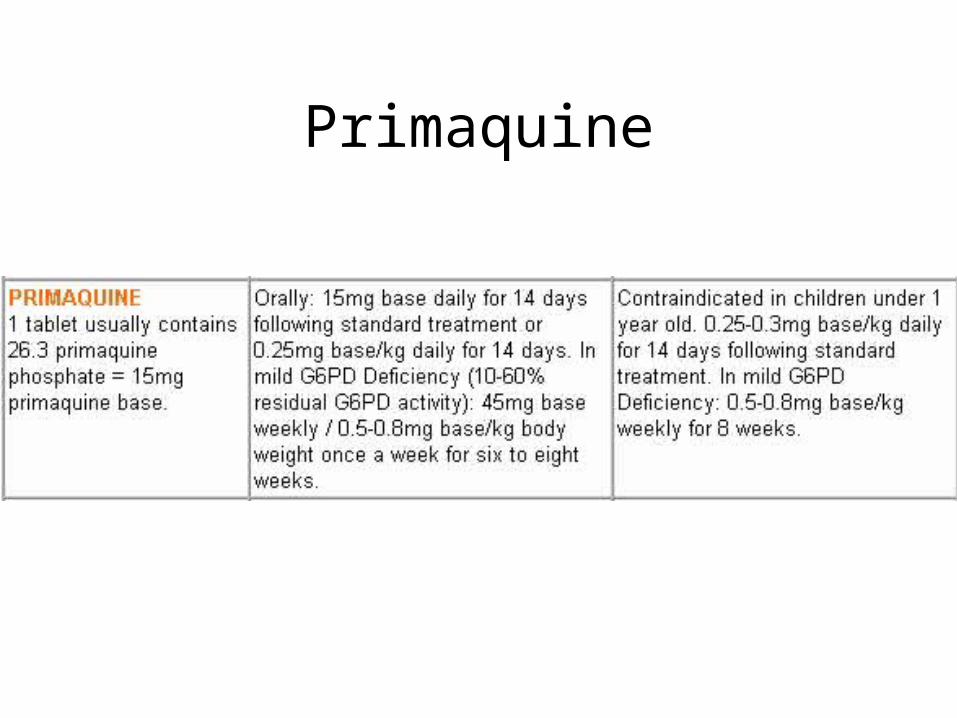
Primaquine
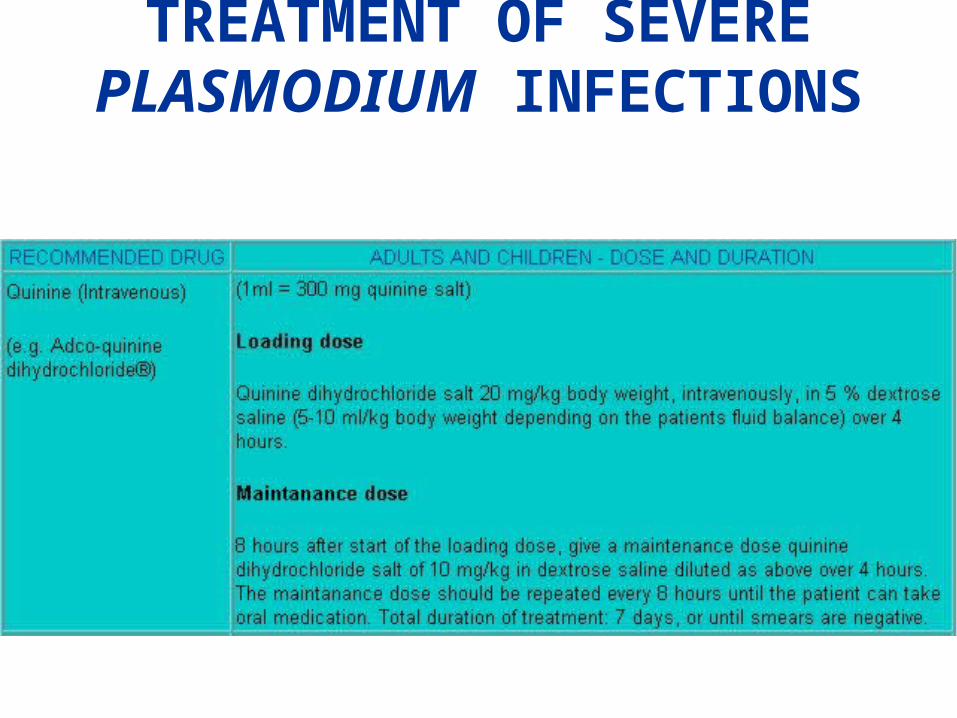
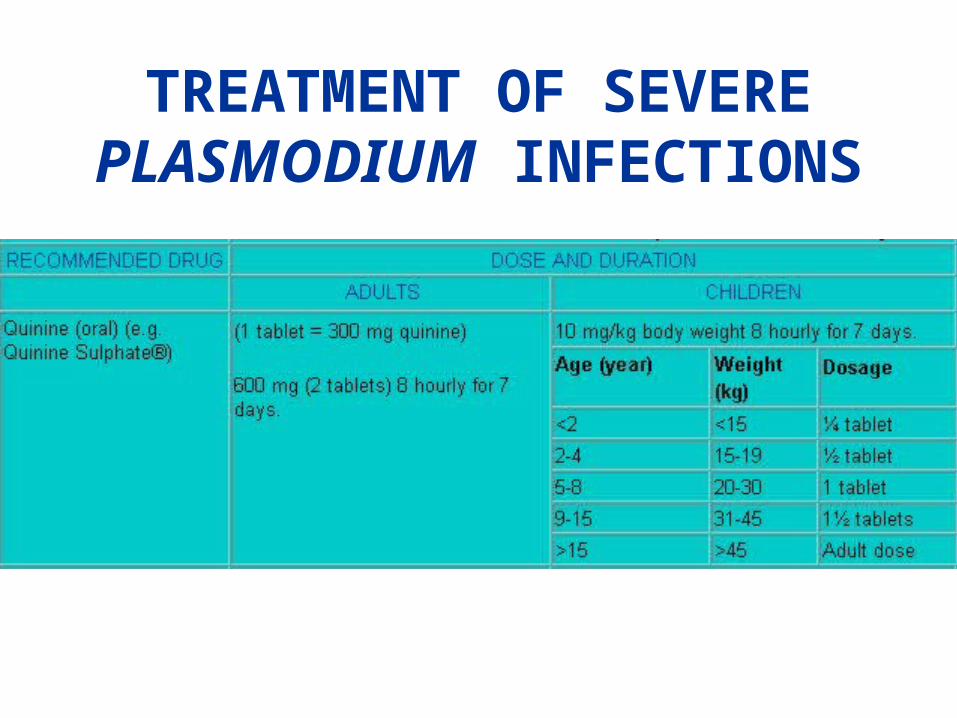
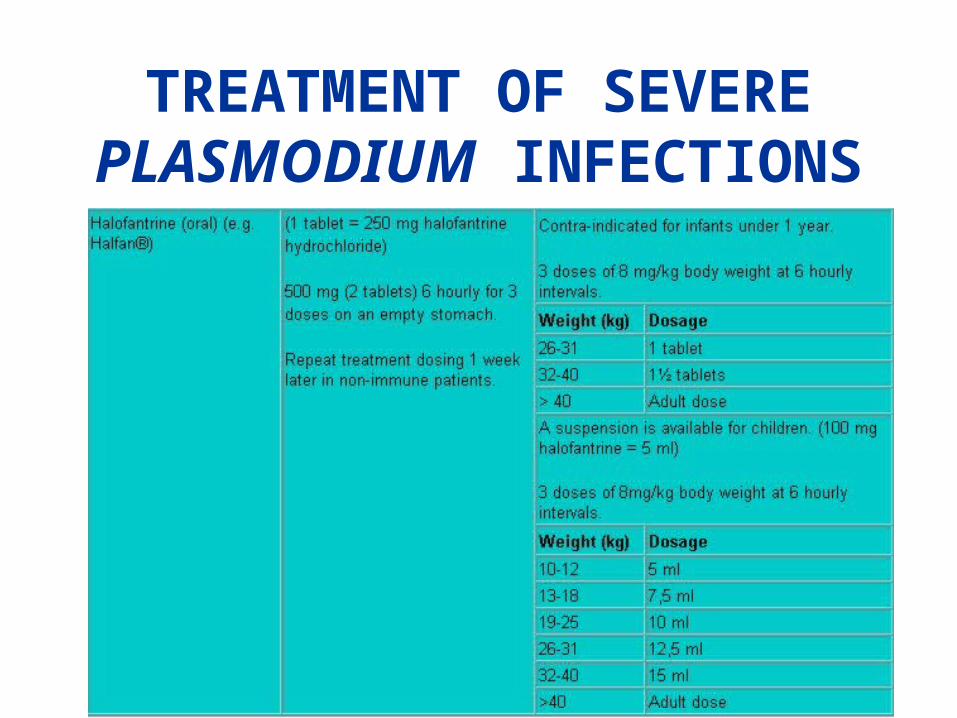
TREATMENT OF SEVERE PLASMODIUM INFECTIONS
TREATMENT OF SEVERE PLASMODIUM INFECTIONS
TREATMENT OF SEVERE PLASMODIUM INFECTIONS
TREATMENT OF SEVERE PLASMODIUM INFECTIONS
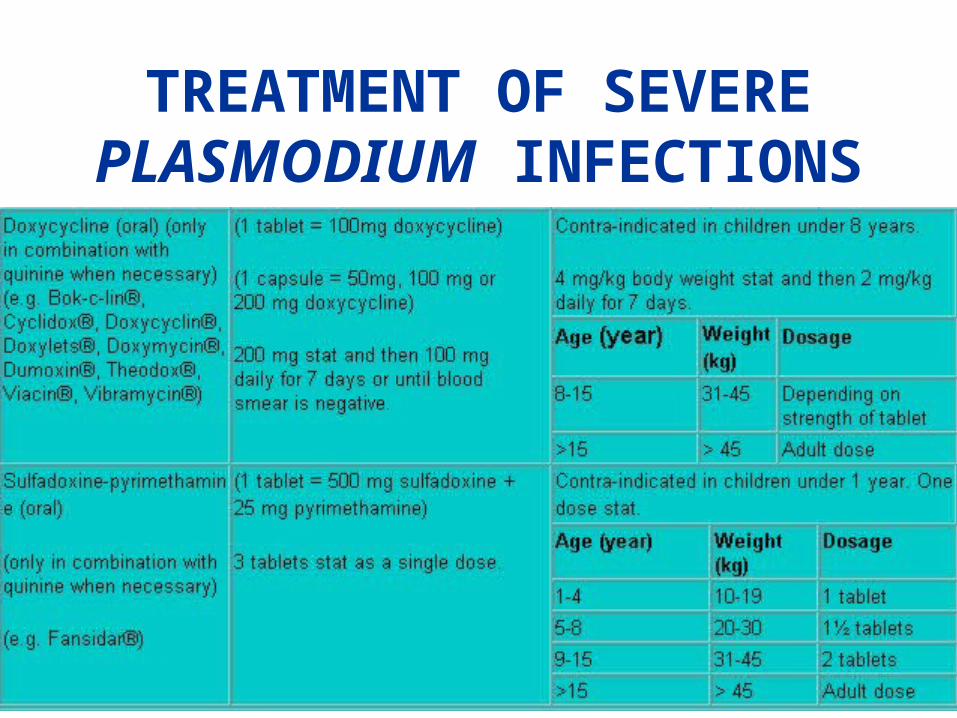
Sulfadoxine-PyrimethamineFANSIDAR
• sulfadoxine-pyrimethamine-resistant parasites
• risk of severe cutaneous adverse effects• for the treatment of mild malaria infections
acquired in South Africa• it is contra-indicated in patients exhibiting
sulphonamide hypersensitivity. • a slow acting schizonticide and should not be
used alone when there is a high risk of severe or complicated malaria.
• *** Sulfadoxine-pyrimethamine (SP) monotherapy is only used for uncomplicated malaria in patients resident in Mpumalanga and Limpopo (Northern) Provinces as the efficacy of SP monotherapy is limited to these areas. Combination therapy that includes an artemisinin derivative is expected to be introduced to these areas as soon as it is available. SP-artesunate combination should then replace all SP monotherapy.
Quinine
• most cases of malaria
• resistance has infrequently been reported in South Africa
• Oral or iv. for at least 7 days or until the blood smear is negative
Treatment of severeMALARIA
• Intensive Care Unit
• Exchange transfusion has gained acceptance as an adjunct to conventional therapy in patients with heavy parasitaemia (more than 10% red blood cells parasitised) and organ dysfunction
Quinine + doxycycline or sulfadoxine- pyrimethamine • * Add clindamycin or doxycycline 2-3 days after
quinine is started. Clindamycin is preferred in children <8 years and pregnant women.
• only indicated if the patient contracted the infection in a country with suspected quinine resistance (e.g. South America and Asia)
• should be added 2-3 days after commencement of the quinine to ensure that possible adverse effects from the quinine are not confused with those of the second agent
Cinchonism
• Mild hearing impairment (notably high tone deafness), tinnitus, headache, nausea and slight visual disturbances are common, occurring in up to 70% of patients during quinine therapy.
• Hypoglycaemia is the most serious frequent adverse side-effect.
• arrhythmias, hypersensitivity