Embed Size (px)
Citation preview
1
Oncothermia for advanced brain gliomas
(Review of ten years experience)
Szasz A.
St.Istvan University, Biotechnics Department, Budapest, Hungary
Introduction None of the established state-of-the-art treatments in malignant primary brain tumors, especially in glioblastoma multiform (GBM), could show effective or commonly accepted curative potential until today, [1]. The earlier well accepted PCV combined chemotherapy (Procarbazine + CCNU (Lomustine) + Vincristine) was shown to be inefficient (n=339 and n=335 in the control- and active-arms, respectively) [2]. In a study where patients did not undergo debulking surgery, survival time was found to be less than 6 months and 2-year survival rate ended up at 0% [3]. The three studies of the Radiation Therapy Oncology Group (RTOG) retrospectively enrolled 1578 patients from 1974-1989, updated in 1991, show overall survival for anaplastic astrocytoma of 49.4 m for patients under the age of 50 years and 21.7 m. for those being older, while for glioblastoma multiforme 13.7 m and 9.7 m were obtained, respectively. The editorial question of JAMA [4] in 2005 is actual even now: “Where to go from here?” Our objective is showing feasible way to go, summarizing the results obtained till now by modulated electro-hyperthermia (oncothermia) in various clinics in EU.
Hyperthermia (HT) combined with conventional therapies seems to be a promising method for glioma treatment by enhancing chemo- and radio-sensitivity [5]. Controlled, randomized, double-armed clinical studies study of Sneed et al. [6], indicated a surprisingly good efficacy of invasive (interstitial) HT treatment for brain-tumors: the median survival had improved from 76 to 85 weeks, and the 2-year survival went up to 31% vs. 15%. In consequence, the FDA certified HT to the brain in its invasive interstitial form.
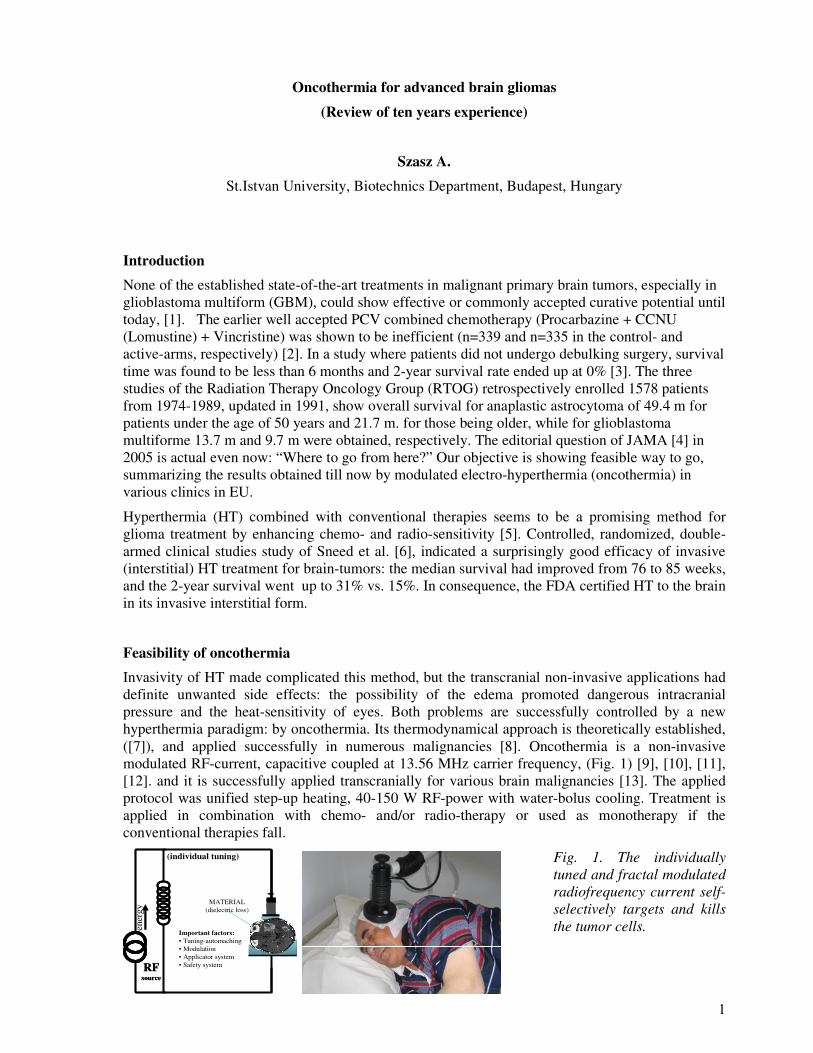
Feasibility of oncothermia Invasivity of HT made complicated this method, but the transcranial non-invasive applications had definite unwanted side effects: the possibility of the edema promoted dangerous intracranial pressure and the heat-sensitivity of eyes. Both problems are successfully controlled by a new hyperthermia paradigm: by oncothermia. Its thermodynamical approach is theoretically established, ([7]), and applied successfully in numerous malignancies [8]. Oncothermia is a non-invasive modulated RF-current, capacitive coupled at 13.56 MHz carrier frequency, (Fig. 1) [9], [10], [11], [12]. and it is successfully applied transcranially for various brain malignancies [13]. The applied protocol was unified step-up heating, 40-150 W RF-power with water-bolus cooling. Treatment is applied in combination with chemo- and/or radio-therapy or used as monotherapy if the conventional therapies fall.
(individual tuning)
Important factors:• Tuning-automaching• Modulation• Applicator system• Safety systemRF
sourceRF
source
MATERIAL(dielectric loss)
ener
gy
Fig. 1. The individually tuned and fractal modulated radiofrequency current self-selectively targets and kills the tumor cells.
2
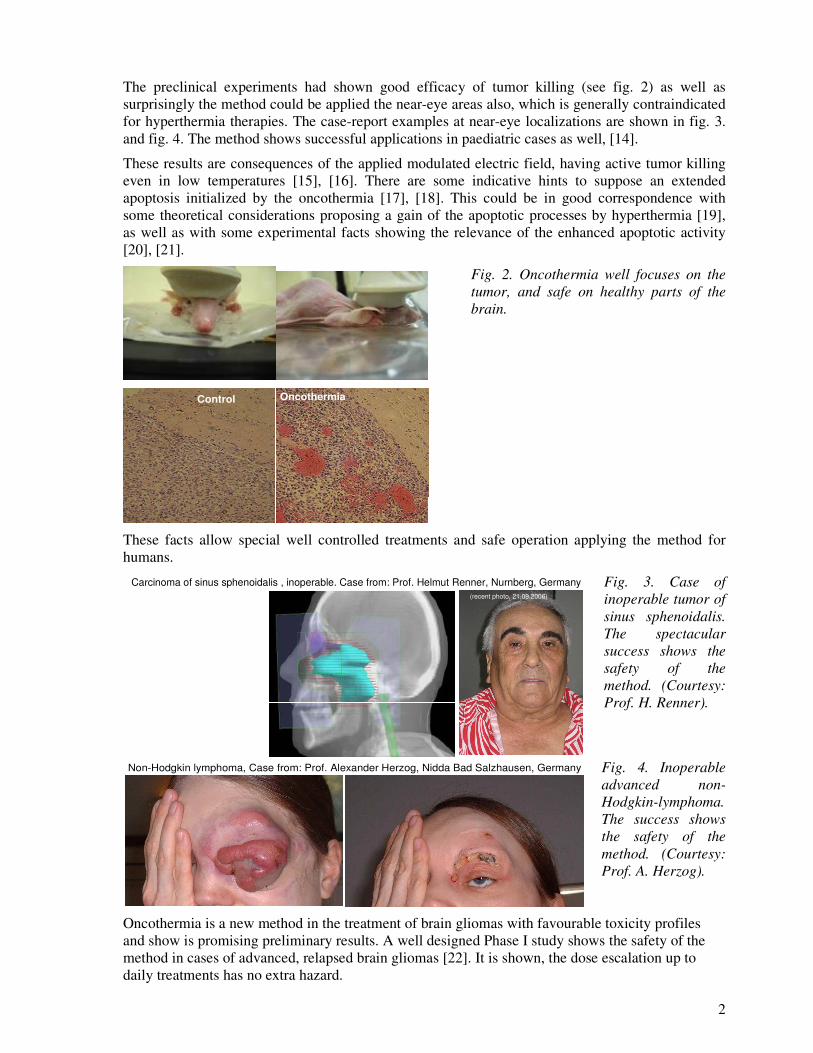
The preclinical experiments had shown good efficacy of tumor killing (see fig. 2) as well as surprisingly the method could be applied the near-eye areas also, which is generally contraindicated for hyperthermia therapies. The case-report examples at near-eye localizations are shown in fig. 3. and fig. 4. The method shows successful applications in paediatric cases as well, [14].
These results are consequences of the applied modulated electric field, having active tumor killing even in low temperatures [15], [16]. There are some indicative hints to suppose an extended apoptosis initialized by the oncothermia [17], [18]. This could be in good correspondence with some theoretical considerations proposing a gain of the apoptotic processes by hyperthermia [19], as well as with some experimental facts showing the relevance of the enhanced apoptotic activity [20], [21].
Control Oncothermia
Fig. 2. Oncothermia well focuses on the tumor, and safe on healthy parts of the brain.
These facts allow special well controlled treatments and safe operation applying the method for humans.
Carcinoma of sinus sphenoidalis , inoperable. Case from: Prof. Helmut Renner, Nurnberg, Germany(recent photo, 21.09.2006)
Fig. 3. Case of inoperable tumor of sinus sphenoidalis. The spectacular success shows the safety of the method. (Courtesy: Prof. H. Renner).
Non-Hodgkin lymphoma, Case from: Prof. Alexander Herzog, Nidda Bad Salzhausen, Germany
Fig. 4. Inoperable advanced non-Hodgkin-lymphoma. The success shows the safety of the method. (Courtesy: Prof. A. Herzog).
Oncothermia is a new method in the treatment of brain gliomas with favourable toxicity profiles and show is promising preliminary results. A well designed Phase I study shows the safety of the method in cases of advanced, relapsed brain gliomas [22]. It is shown, the dose escalation up to daily treatments has no extra hazard.
3
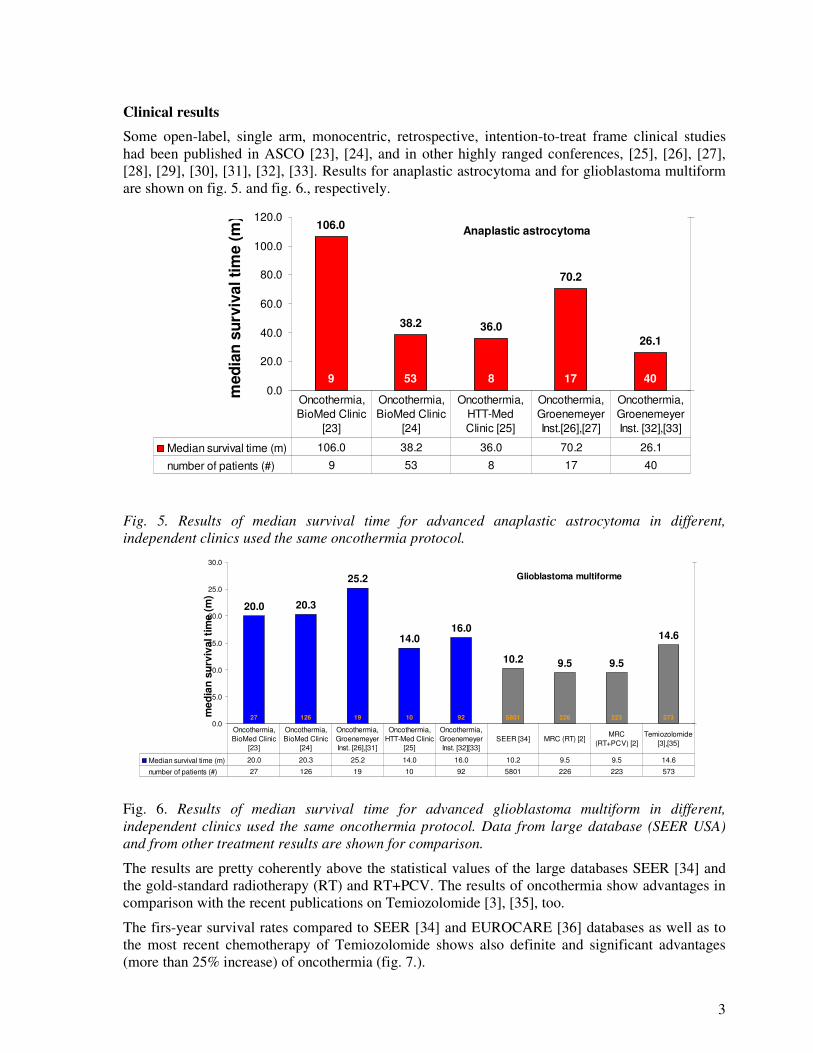
Clinical results Some open-label, single arm, monocentric, retrospective, intention-to-treat frame clinical studies had been published in ASCO [23], [24], and in other highly ranged conferences, [25], [26], [27], [28], [29], [30], [31], [32], [33]. Results for anaplastic astrocytoma and for glioblastoma multiform are shown on fig. 5. and fig. 6., respectively.
Anaplastic astrocytoma106.0
38.2 36.0
70.2
26.1
9 53 8 17 400.0
20.0
40.0
60.0
80.0
100.0
120.0
med
ian
surv
ival
tim
e (m
)
0
120
Median survival time (m) 106.0 38.2 36.0 70.2 26.1
number of patients (#) 9 53 8 17 40
Oncothermia, BioMed Clinic
[23]
Oncothermia, BioMed Clinic
[24]
Oncothermia, HTT-Med Clinic [25]
Oncothermia, Groenemeyer Inst.[26],[27]
Oncothermia, Groenemeyer Inst. [32],[33]
Fig. 5. Results of median survival time for advanced anaplastic astrocytoma in different, independent clinics used the same oncothermia protocol.
Glioblastoma multiforme
20.0 20.3
25.2
14.016.0
10.2 9.5 9.5
14.6
27 126 19 10 92 5801 226 223 5730.0
5.0
10.0
15.0
20.0
25.0
30.0
med
ian
surv
ival
tim
e (m
)
0
10000
Median survival time (m) 20.0 20.3 25.2 14.0 16.0 10.2 9.5 9.5 14.6
number of patients (#) 27 126 19 10 92 5801 226 223 573
Oncothermia, BioMed Clinic
[23]
Oncothermia, BioMed Clinic
[24]
Oncothermia, Groenemeyer Inst. [26],[31]
Oncothermia, HTT-Med Clinic
[25]
Oncothermia, Groenemeyer Inst. [32][33]
SEER [34] MRC (RT) [2]MRC
(RT+PCV) [2]Temiozolomide
[3],[35]
Fig. 6. Results of median survival time for advanced glioblastoma multiform in different, independent clinics used the same oncothermia protocol. Data from large database (SEER USA) and from other treatment results are shown for comparison.
The results are pretty coherently above the statistical values of the large databases SEER [34] and the gold-standard radiotherapy (RT) and RT+PCV. The results of oncothermia show advantages in comparison with the recent publications on Temiozolomide [3], [35], too.
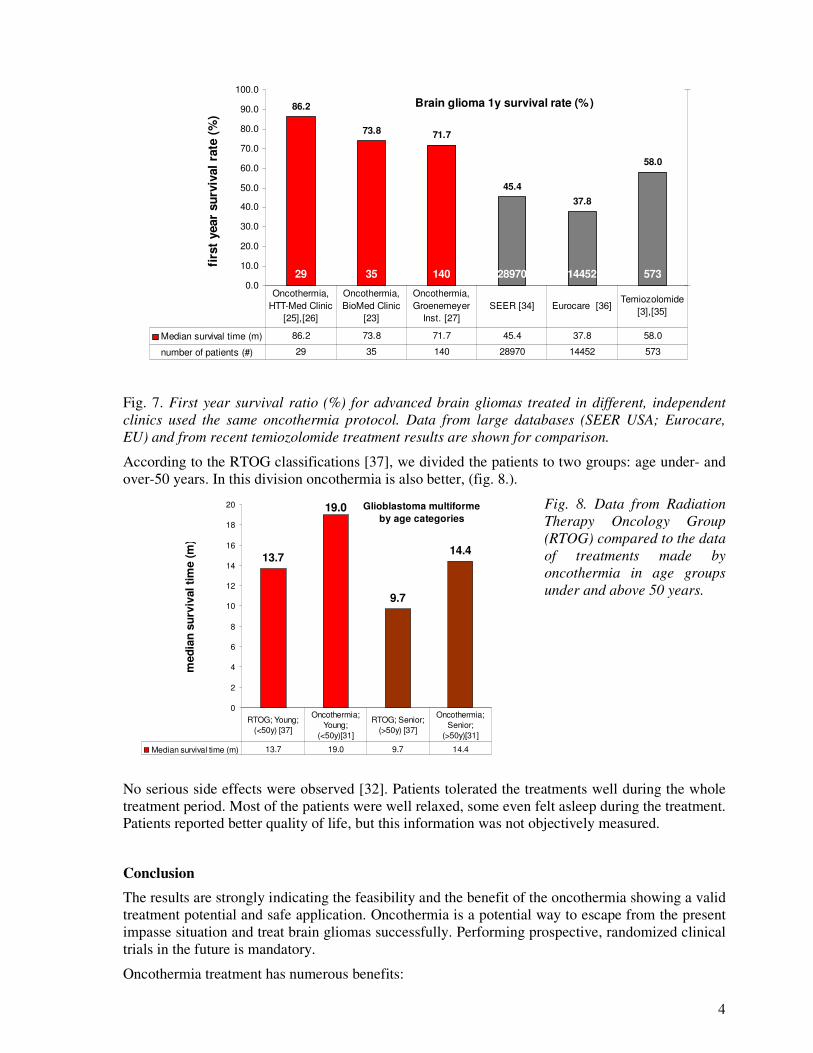
The firs-year survival rates compared to SEER [34] and EUROCARE [36] databases as well as to the most recent chemotherapy of Temiozolomide shows also definite and significant advantages (more than 25% increase) of oncothermia (fig. 7.).
4
Brain glioma 1y survival rate (%)86.2
73.8 71.7
45.437.8
58.0
29 35 140 28970 14452 5730.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
90.0
100.0
firs
t ye
ar s
urvi
val r
ate
(%)
0
40000
Median survival time (m) 86.2 73.8 71.7 45.4 37.8 58.0
number of patients (#) 29 35 140 28970 14452 573
Oncothermia, HTT-Med Clinic
[25],[26]
Oncothermia, BioMed Clinic
[23]
Oncothermia, Groenemeyer
Inst. [27]SEER [34] Eurocare [36]
Temiozolomide [3],[35]
Fig. 7. First year survival ratio (%) for advanced brain gliomas treated in different, independent clinics used the same oncothermia protocol. Data from large databases (SEER USA; Eurocare, EU) and from recent temiozolomide treatment results are shown for comparison.
According to the RTOG classifications [37], we divided the patients to two groups: age under- and over-50 years. In this division oncothermia is also better, (fig. 8.).
Glioblastoma multiformeby age categories
13.7
19.0
9.7
14.4
0
2
4
6
8
10
12
14
16
18
20
med
ian
surv
ival
tim
e (m
)
Median survival time (m) 13.7 19.0 9.7 14.4
RTOG; Young; (<50y) [37]
Oncothermia; Young;
(<50y)[31]
RTOG; Senior; (>50y) [37]
Oncothermia; Senior;
(>50y)[31]
Fig. 8. Data from Radiation Therapy Oncology Group (RTOG) compared to the data of treatments made by oncothermia in age groups under and above 50 years.
No serious side effects were observed [32]. Patients tolerated the treatments well during the whole treatment period. Most of the patients were well relaxed, some even felt asleep during the treatment. Patients reported better quality of life, but this information was not objectively measured.
Conclusion The results are strongly indicating the feasibility and the benefit of the oncothermia showing a valid treatment potential and safe application. Oncothermia is a potential way to escape from the present impasse situation and treat brain gliomas successfully. Performing prospective, randomized clinical trials in the future is mandatory.
Oncothermia treatment has numerous benefits:
5
1. Oncothermia was applied for brain tumors, showing a valid treatment potential and safe application.
2. A transcranially applied non-invasive electric field is able to perform the treatment.
3. No safety or mentionable toxicity problem has occurred. The development of an oedema, which was the general block of hyperthermia applications in the past, is not the case with oncothermia. There was not any eye-damage and/or vision-complication which was also a risk in the radiative hyperthermia methods. The treatment is safe and convenient to use.
4. The survival time, as one of the most important endpoints of the studies, was increased.
5. The quality of life of every patient who was treated with oncothermia was not worsened, even according to their subjective reports.
Ackonowledgement Author is thankful for the diligent and smart physicians dealing with oncothermia and making possible to collect this review. Especial thanks have to be made for Groenemeyer Institute, Witten-Herdecke University, Bochum, Germany; Fachklinik Dr.Herzog, Nidda, Germany; Klinikum Nord-Nurnberg, Nurnberg, Germany; Biomed Clinic, Bad Bergzabern, Germany; HTT-Med Clinic, Budapest, Hungary; Neurology Clinic, Regensburg University, Germany.
References [1] Ries LAG, Eisner MP, Kosary CL, et al (eds): SEER Cancer Statistics, 1973-1998. Bethesda, MD, National Cancer Institute, 2001 [2] Medical Research Council Brain Tumor Working Party: Randomized Trial of Procarbazine, Lomustine, and Vincristine in the Adjuvant treatment
of High-grade Astrocytoma: A Medical Research Council Trial, J. Clin. Oncol. 19:509-518, 2001 [3] Stupp R, Dietrich P-Y, Kraljevic SO, Pica A, Maillard I, Maeder P, Meuli R, Janzer R, Pizzolato G, Mirabell R, Porchet F, Regli L, deTribolet N,
Miramanoff RO, Leyvraz S: Promising survival for patients with newly diagnosed glioblastoma multiforme treated with concomitant radiation plus temiozolomide followed by adjuvant temozolomide, J. Clin. Oncol. 20:1375-1382, 2002
[4] Fisher PG, Buffler PA: Malignant gliomas in 2005. Where to GO from here?, Editorials, JAMA 293:615-617, 2005 [5] Sumiyoshi K, Strebel FR, Rowe RW et al. The effect of whole-body hyperthermia combined with 'metronomic' chemotherapy on rat mammary
adenocarcinoma metastases. Int J Hyperthermia. 2003;19(2):103-18 [6] Sneed PK, Stauffer PR, McDermott MW, Diederich CJ, Lamborn KR, Prados MD, Chang S, Weaver KA, Spry L, Malec MK, Lamb SA, Voss B,
Davis RL, Wara WM, Larson DA, Phillips TL, Gutin PH.: Survival benefit of hyperthermia in a prospective randomized trial of brachytherapy boost +/- hyperthermia for glioblastoma multiforme, Int J Radiat Oncol Biol Phys. 1998 Jan 15;40(2):287-95
[7] Szasz A, Vincze Gy, Szasz O, Szasz N: An energy analysis of extracellular hyperthermia, Magneto- and electro-biology, 22 (2003) 103-115 [8] Szasz A., A. Dani, et.al.: Retrospective analysis of 1180 oncological patients treated by electro-hyperthermia in Hungary, DEGRO 11.
Jahreskongress der Deutschen Gesellschaft für Radioonkologie, 26-29 Mai 2005, Kongresszentrum, Karlsruhe [9] Szasz A, Szasz O, Szasz N: Electrohyperthermia: a new paradigm in cancer therapy, Wissenschaft & Forschung, Deutsche Zeitschrift für
Onkologie, 33:91-99, 2001. [10] Szasz A, Szasz O, Szasz N: Physical background and technical realization of hyperthermia, in: Locoregional Radiofrequency-Perfusional- and
Wholebody- Hyperthermia in Cancer Treatment: New clinical aspects, (Eds: Baronzio GF, Hager ED), Springer Science Eurekah.com, 2005 [11] Szasz, O., Andocs, G., Szasz, A. (2008). Thermally induced effects in oncothermia treatment, In-print Electrom. Bio. Med. 2009 [12] Andocs G., Galfi P., Renner H., Balogh L., Fonyad L., Jakab Cs., Szasz A.: Thermally induced but temperature independent cell-destruction by
modulated electrohyperthermia in nude-mice xenograft model, Expanding the Frontiers of Thermal Biology, Medicine and Physics Annual Meeting of Society of Thermal Medicine, Tucson, AZ, USA, 2009
[13] Szasz A: Brain glioma results by oncothermia, a review, Expanding the Frontiers of Thermal Biology, Medicine and Physics Annual Meeting of Society of Thermal Medicine, Tucson, AZ, USA, 2009
[14] Sahinbas H.: EHT bei Kindern mit Hirntumoren und nicht-invasive Messverfahren am beispiel von Hirntumoren, Symposium Hyperthermie, Cologne, 15-16 Oktober 2004
[15] Andocs G. Renner H.Balogh L, Fonyad L, Jakab Cs, Szasz A: Strong synergy of heat and modulated electromagnetic field in tumor cell killing, Study of HT29 xenograft tumors in a nude mice model, Accepted for publication in Radiology and Oncology [Strahlentherapie und Onkologie], 185:120-126, 2009
[16] Szasz, O., Andocs, G., Szasz, A. (2008). Thermally induced effects in oncothermia treatment, Symposium on Biophysical Aspects of Cancer, Electromagnetic mechanisms, (in memoriam H. Froelich), Prague, 1-3. July, 2008, submitted to Electrom. Bio. Med.
[17] Andocs G, Szasz A: Preliminary results of Oncothermia induced apoptosis in nude-mouse inoculated human-glioblastoma cells, Results of hyperthermia, Seminar, St. Istvan University, Aug. 24., 2005. (in Hungarian)
[18] Andocs G., Galfi P., Szasz O., Szasz A.: Effects of modulated, capacitive coupled electro-hyperthermia (oncothermia) in in vitro Models, Expanding the Frontiers of Thermal Biology, Medicine and Physics Annual Meeting of Society of Thermal Medicine, Tucson, AZ, USA, 2009
[19] Chen JW, Lin J, Madamanchi N, Trier TT, Campbell G: Apoptosis occurs in a new model of thermal brain injury, J. Biomed. Sci. 7:459-465, 2000
[20] Fuse T, Yoon K-W, Kato T, Yamada K: Heat-induced apoptosis in human glioblastoma cell-line A172, Neurosurgery 42:843-849, 1998 [21] Vogel P, Dux E, Wiessner C: Evidence of apoptosis in primary neuronal cultures after heat shock, Brain Res. 764:205-213, 1997 [22] Wismeth C., Hirschmann B., Pascher C., Dudel C., Szasz A., Bogdahn U., Hau P.:Transcranial electro-hyperthermia combined with alkylating
chemotherapy in patients with relapsing high-grade gliomas – Phase I clinical results; Expanding the Frontiers of Thermal Biology, Medicine and Physics Annual Meeting of Society of Thermal Medicine, Tucson, AZ, USA, 2009
[23] Hager ED, Dziambor H, App EM, Popa C, Popa O, Hertlein M: The treatment of patients with high-grade malignant gliomas with RF-hyperthermia. Proc ASCO 2003; 22:118, #470, Proc Am Soc Clin Oncol 22: 2003

6
[24] Hager ED, H Sahinbas, DH Groenemeyer, F Migeod: Prospective phase II trial for recurrent high-grade malignant gliomas with capacitive
coupled low radiofrequency (LRF) deep hyperthermia, ASCO 2008, Journal of Clinical Oncology, 2008 ASCO Annual Meeting Proceedings (Post-Meeting Edition). 26:2047, 2008
[25] Dani A, Varkonyi A: Electro-hyperthermia treatment of malignant brain tumors, Results of hyperthermia, Seminar, St. Istvan University, Aug. 26-27., 2003. (in Hungarian)
[26] Szasz A., Sahinbas H., Dani A.: Electro- hyperthermia for anaplastic astrocytoma and gliobastoma multiforme ICACT 2004, Paris, 9-12. February, 2004
[27] Sahinbas H., Grönemeyer D.H.W., Böcher E., Lange S.: Hyperthermia treatment of advanced relapsed gliomas and astrocytoma, The 9th International Congress on hyperthermic oncology, St. Louis, Missuri, ICHO, April 24-27, 2004
[28] Hager E.D.: Response and survival of patients with gliomas grade III/IV treated with RF capacitive-coupled hyperthermia, ICHO Congress, St. Louis USA 2004
[29] Hager E.D.: Clinical Response and Overall Survival of Patients with Recurrent Gliomas Grade III/IV Treated with RF Deep Hyperthermia – An Update, ICHS Conference, Shenzhen, China, 2004
[30] Fiorentini G, Giovanis P, Rossi S, Dentico P, Paola R, Turrisi G, Bernardeschi P: A phase II clinical study on relapsed malignant gliomas treated with electro-hyperthermia, In Vivo. 20:721-724, 2006
[31] Sahinbas H, Szasz A: Electrohyperthermia in brain tumors, Retrospective clinical study, Annual Meeting of Hungarian Oncology Society, Budapest November 3-5, 2005
[32] Sahinbas H, Groenemeyer DHW, Boecher E, Szasz A: Retrospective clinical study of adjuvant electro-hyperthermia treatment for advanced brain-gliomas, Deutche Zeitschrifts fuer Onkologie, 39:154-160, 2006
[33] Sahinbas H, Baier JE, Groenemeyer DHW, Boecher E, Szasz A: Retrospective clinical study for advanced brain-gliomas by adjuvant oncothermia (electro-hyperthermia) treatment, 2006 www.gimt-online.de/uploads/media/Therapieergebnisse_Giloma_Studie_01.pdf
[34] Surveillance, Epidemiology, and End Results (SEER), National Cancer Institute. www.seer.cancer.gov. April, 2000 [35] Stupp R, Mason WP, van den Bent MJ, Weller M, Fisher B, Taphoorn, MJB, Belanger K, Brandes AA, Marosi C, Bogdahn U, Curschmann J,
Janzer RC, Ludwin SK, Gorlia T, Allgeier A, Lacombe D, Cairncross JG, Eisenhauer E, Mirimanoff RO: Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma, The New England J. of Med., 352:987-996, 2005
[36] EUROCARE-3, European Cancer Database. www.eurocare.org/profiles/index.html [37] Scott CB, Scarantino C, Urtasun R, et al: Validation and predictive power of Radiation Therapy Oncology Group (RTOG) recursive partitioning
analysis classes for malignant glioma patients: A report using RTOG 90-06. Int J Radiat Oncol Biol Phys 40:51-55, 1998











![Malignant hyperthermia [final]](https://img.pdfslide.net/doc/110x75/58ceb1b71a28abb2218b5123/malignant-hyperthermia-final.jpg)