Embed Size (px)
Citation preview

Archives of Disease in Childhood, 1981, 56, 258-263
Hypertrophic cardiomyopathy in infants ofpoor1y-controlled diabetic mothersHENRY L HALLIDAY
Children's Hospital, San Francisco, and Royal Maternity Hospital, Belfast
SUMMARY Twelve newborn infants of poorly-controlled diabetic mothers were transferred fromoutlying maternity hospitals for neonatal intensive care. Respiratory distress and cardiomegaly were
the presenting signs. Ten infants were large for dates (macrosomic) and had echocardiographicevidence of myocardial hypertrophy, reduced ejection time, and systolic anterior movement of themitral valve (in 6 infants). These findings are similar to those of adults with idiopathic hypertrophicsubaortic stenosis. Two infants died. In survivors the myccardial hypertrophy persisted for at least2 weeks but the evidence of functional subaortic stenosis had disappeared by 4-7 days. The 2 infantswho were appropriately grown had cardiomegaly as a result of ventricular dilatation. This was
associated with hypoglycaemia and acidosis, and disappeared when these metabolic disturbanceswere corrected.
Hypertrophic cardiomyopathy is a conditioncharacterised by stiff, hypertrophied ventricularmuscle, predominant thickening of the ventricularseptum, impaired relaxation, and powerful butincoordinate contraction.1 The condition in adults isfamilial, and probably represents an autosomaldominant trait. There is functional subaorticobstruction in severe cases and this is referred to asidiopathic hypertrophic subaortic stenosis (IHSS).Previous reports have suggested that IHSS mayoccur transiently in infants of diabetic mothers.2 4This paper reports echocardiographic findings in 12infants of diabetic mothers who were admitted tohospital for newborn intensive care. Ten of theseinfants appeared to have many echocardiographicfeatures characteristic of IHSS; and in 2 infants thefindings suggested ventricular dilatation rather thanhypertrophy.
Patients
From February 1978 to September 1979, 12 infantsof diabetic mothers were admitted to newbornintensive care units in San Francisco and Belfast.Eight infants were in San Francisco and 4 were inBelfast. The infants had been born in outlyinghospitals where the antenatal care of their mothershad been supervised. Transfer was arranged within4 hours of birth in each case. Poor control ofmaternal diabetes had been a major feature in eachpregnancy; 5 mothers had episodes of ketoacidosis
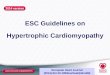
associated with infections, 6 had severe poly-hydramnios, and in addition 5 were hypertensive.Three mothers had class A diabetes, 1 class B, 3class C, 4 class D, and 1 class F (White's classifica-tion).5 Delivery was by caesarean section in 7mothers and per vaginum in 5. Ten infants hadasphyxia with Apgar scores <7 at one minute.There were 9 boys and 3 girls. Mean gestational agewas 37 weeks and mean birthweight 3640 g. Fig. 1shows a growth chart of birthweight against gesta-
5000
4000
0-
.c 3000-
.2'
'C 2000
1000
*0
- 5th0
28 30 32 34 36 38 40 42Gestation ( weeks)
Fig. 1 Growth chart ofgestational age againstbirthweight for UK infants.6 The mean, 5th, and 95thcentiles are shown. Ten infants are on the 90th centileor above and are large for dates (group 1) andthe 2 smaller infants, shown as open circles, formgroup 2.
258
. . . . . .
on Novem
ber 13, 2020 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.56.4.258 on 1 April 1981. D
ownloaded from

Hypertrophic cardiomyopathy in infants ofpoorly-controlled diabetic mothers 259
tional age for babies in the UK;6 9 of the 12 infantsstudied were on or above the 95th centile of weightfor age, one was on the 90th centile, one on the 25thcentile, and one < the 5th centile. The 10 infants onor above the 90th centile were considered to be largefor dates (group 1), and the 2 smaller infants wereconsidered separately (group 2). Two infants ingroup 1 died about 48 hours after birth. There wasno clinical evidence of congenital anomaly ofcardiovascular or other system in any infant.
Methods
M-mode echocardiography (Ekoline 20A in SanFrancisco, and Teknika Echomatic in Belfast) was
.....
0-44
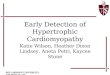
LPEP =left ventricular pre-ejection period, LVET =left ventricularejection time.
Fig. 2 Aortic valve echogram recorded at 100mm/second in an infant of a diabetic mother. In thisinfant LPEPILVET ratio was 0-44 which is abovethe normal mean for newborn infants (O 35) andsuggests disordered left ventricular contractility.
used to assess myocardial thickness and left ventri-cular contractility in all 12 infants within 24 hours ofbirth, and in the 10 surviving infants at both 4-7days and 11-13 days. Septal wall thickness (SWT)and left ventricular posterior wall thickness(LVPWT) were measured as described by Haganet al.7 and Solinger et al.8
Left ventricular contractility was assessed by twodifferent methods; firstly, the percentage shorteningof the internal dimension of the left ventricle(% SID)9 and, secondly, the left ventricular pre-ejection period to ejection time ratio (LPEP/LVETratio).'0 Percentage SID was calculated by theformula9
% SID = LVEDD-LVESD/LVEDD
where LVEDD = left ventricular end-diastolicdimension
and LVESD = left ventricular end-systolicdimension
LPEP/LVET ratio was measured from echograms ofaortic valve recorded at paper speeds of 100mm/second (Fig. 2).10
Results
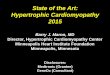
Group 1. Eight of these 10 infants had presented withrespiratory problems after birth which were believedto be due to respiratory distress syndrome. Murmurswere present in 4 of them. On chest x-ray films all10 infants had cardiomegaly (mean cardiothoracicratio 0 72). Nine infants had abnormal electro-cardiographs with either flat T-waves over theanterior chest beats (4 babies), right ventricularhypertrophy of moderate degree (6 babies), orventricular ectopic beats (1 baby) (Fig. 3).Each infant in group 1 had echographic evidence
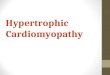
of thickening of interventricular septum and leftventricular posterior wall (Fig. 4). This hypertrophypersisted for at least 2 weeks and was initially
Fig. 3 Lead II of an electrocardiogram from an infant of a diabetic mother taken at half standardisation. Someventricular ectopic beats are shown.
on Novem
ber 13, 2020 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.56.4.258 on 1 April 1981. D
ownloaded from

260 Halliday
Normal
r
RV
SepturWt
~~~~~ ~~~.A Aj
Intant of diabetic mother
!--~~~w$.~~~~~~~~~~~~~N
~PowVVA*R
Fig. 4 Echocardiograms ofnormal infant andofinfant ofdiabetic mother taken to show right ventricle (RV),interventricular septum (IVS), and left ventricle (LV).The mitral valve is marked (MV). There is markedthickening ofIVS (0.6 cm) compared with normal(0.3 cm). Left ventricular posterior wall (PLVW) isalso thickened (0.5 to 0*3 cm). Slight systolicanterior movement of mitral valve can be seen arrowed.
associated with alterations in % SID and LPEP/LVET ratio (Fig. 5). SWT was 0 56 at 24 hours andLVPWT was 0 48 cm, both considerably greaterthan normal (0 3 cm).7 8 SWT/LVPWT ratio was1 -2 which is above the normal range of 0 9 to 10.Mild systolic anterior movement of the mitral valvewas present in 6 infants (Fig. 4). LPEP/LVET ratiowas increased at 24 hours due to a reduction in LVETsince LPEP values were in the normal range1l(Table 1). Although the myocardial hypertrophypersisted for 2 weeks, % SID and LPEP/LVET ratiodecreased with time and were both normal by 4-7days. Indeed, paradoxically there was a directcorrelation between LPEP/LVET ratio and % SID(Fig. 6) which was contrary to what would beexpected in the failing heart.These changes in left ventricular contractility were
not significantly related to the degree of myocardialthickening or to biochemical disturbances (hypo-glycaemia, hypocalcaemia, hypokalaemia or hyper-kalaemia, and acidaemia) (all r<0 3).Two of the infants in group 1 died within 48 hours
of birth from cardiorespiratory failure. One had beengiven a beta-blocker (propranolol) when close todeath without apparent change in clinical condition,and the other had been treated with digoxin, also
Myocardial thickness (cm)
060 SWT
0-50.
0 40. LVPWT
0*30
381 Shortening of internal dimension
340 / w /
30-0 40 LPEP/LVET ratio
0 36- / // / /
0-32
Initial 4-7days 11-13daysFig. 5 Plots ofmean + 1 SD for myocardialthickness, % SID, and LPEP/L VET ratio withpostnatal age of the 10 large for dates infants. Theshaded areas represent the normal range for terminfants.7 8 11 Septal wall thickness (SWT) and leftventricular posterior wall thickness (LVPWT) remainincreased for up to 2 weeks postnatally. The septum ishypertrophied to a greater extent than the LVPWwith SWT/LVPWT ratios of 1-2, 1.2, and 0-9 wherenormal is 0 -9 to 1- 0. % SID = percentage shorteningof internal dimension of left ventricle, LPEP = leftventricle pre-ejection period, and LVET = leftventricular ejection time.
Table 1 Comparison of systolic time intervals(mean ± 1 SD) in infants of diabetic mothers andnormal newborn infants at 24 hours
Normal* Infants of diabeticmothers
LPEP (msecond) 70 + 10 69 ± 8LVET (msecond) 196 + 17 161 + 19LPEP/LVET ratio 0*36 ± 005 0*43 +006
LPEP = left ventricular pre-ejection period, LVET = left ventricularejection time.*Halliday et aI.1
on Novem
ber 13, 2020 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.56.4.258 on 1 April 1981. D
ownloaded from

Hypertrophic cardiomyopathy in infants ofpoorly-controlled diabetic mothers 261
048v
0-44
LPEP0 *0O
LVET036/
032
028
24 28 32 36Shortening of internal dimension %
Fig. 6 Correlation ofLPEP/LVET ratio andin initial echocardiograms. Group 2 infants areas open circles. The relationship is significant(r =0-62,P<0-02).
Table 2 Mean organ sizes of infants of diabeticmothers
Size Weight as Y. of normal*
IHSS Infants of diabetic motherst(n = 2) (n = 21)
Body weight 113 141Body length 109 112Heart weight 200 174Liver weight 139 179Brain weight 83 97Spleen weight 147 127Lung weight 113 127
*Schulz et al.12 tNaeyel3IHSS = idiopathic hypertrophic subaortic stenosis.
without apparent alteration in clinical course. At/ necropsy both had hearts that were about twice the
normal weight12 (Table 2). Shown in the table forcomparison are the findings in 21 large for dateinfants of diabetic mothers studied by Naeye.13 Inboth of our infants SWT was 0-6 cm which corres-
* ponded precisely to that found by echocardiographyduring life. There was no evidence of anatomicalsubvalvular aortic stenosis at necropsy. On histo-logical examination the heart showed some vacuolarand hydropic changes (Fig. 7) but these were non-
40 44 specific and did not amount to any clear cardio-myopathy. There was no disorganisation of
/ SID myocardial fibres or inflammatory cell infiltrate, ande shown special staining failed to show excessive deposition of
glycogen within the cellular cytoplasm.
Group 2. These two smaller infants had cardiomegalydue to ventricular dilatation and myocardialthickness was normal.7 8 They also showed dis-ordered contractility (Fig. 6) but this was related tohypoglycaemia and acidaemia and improved whenthese metabolic disturbances had been corrected.Both infants survived and their condition was normalat follow-up.
Discussion
Pathognomonic echographic findings of IHSS areasymmetrical septal hypertrophy'4 and systolicanterior movement of the mitral valve.15 Additionalfindings are narrow left ventricular outflow tract,
Fig. 7 Histological section of the heart from an infant ofa diabetic mother showing hydropic changes but noevidence of disorganisation of myocardial cells.
on Novem
ber 13, 2020 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.56.4.258 on 1 April 1981. D
ownloaded from

262 Halliday
high ejection fraction, and altered left ventricularejection time (LVET).'617 When outflow obstructionis severe LVET may be lengthened but in patientswithout outflow obstruction the myocardial hyper-trophy tends to be less, systolic anterior movement ofthe mitral valve absent,65 16 and LVET shortened.'8There have been reports of hypertrophic cardio-
myopathy in infancy2-4 19-21 and either a positivefamily history of IHSS21 or the presence of maternaldiabetes-4 21 seems to be a common association.
In our infants there was no family history of IHSSalthough we did not perform echographic studies ontheir 1st-degree relatives. Each mother had eithergestational diabetes mellitus or was a known diabeticrequiring insulin before her pregnancy. In each casethe diabetes had been poorly controlled duringpregnancy. Episodes of ketoacidosis and markedpolyhydramnios were common antecedents. All theinfants had cardiomegaly on radiographic andechographic examination. In the 10 infants (group 1)the cardiomegaly was due to hypertrophy especiallyof the interventricular septum and left ventricularposterior wall, but in the 2 smaller infants there wasdilatation of the heart in association with hypo-glycaemia and acidaemia. Hypoglycaemia has beenassociated with cardiac enlargement and heartfailure in the newborn2223 and I believe that theinfants in group 2 belonged in this category.The 10 large infants (group 1) however, demon-
strated many of the echocardiographic findings ofIHSS:17 myocardial hypertrophy with asymmetricalseptal hypertrophy, vigorous contraction, andincreased ejection fraction or % SID, reduced LVET,and mild systolic anterior movement of the mitralvalve. These findings were not related to hypo-glycaemia, hypocalcaemia, potassium disturbances,or to acidosis. The hypertrophy remained for at least2 weeks but evidence of left ventricular outflowobstruction (increased % SID, reduced LVET, andmild systolic anterior movement of the mitral valve)had disappeared by 4-7 days in the 8 survivinginfants. At necropsy in 2 infants there was noevidence of anatomical subvalvular stenosis althoughthe hypertrophy suggested by echocardiography wasconfirmed. These infants had pathological evidenceof hyaline membrane disease.Whether the presence of hypertrophic cardio-
myopathy could explain the respiratory difficulty ofthese infants and the death of 2 of them is debatable.Eight of the 10 infants had clinical findings that werecompatible with respiratory distress syndrome, andthe presence of hyaline membranes at necropsy in 2of them tends to support this diagnosis as tenable.The absence of anatomical subaortic stenosis atnecropsy does not however, exclude the presence offunctional outflow obstruction.
Beta-blockade with propranolol has been shown tobe effective in one infant with IHSS'9 but thistreatment was used in only one of our infants.Propranolol was given late in the clinical illness ofthis infant without any apparent amelioration in hiscondition. In another infant the hypertrophiccardiomyopathy was associated with a potentiallyserious arrthymia-namely frequent ventricularectopic beats. This infant survived after treatmentdesigned to suppress the arrythmia, but if thisdisturbance of rhythm had occurred in utero thenfetal death may well have occurred. Sudden,unexplained death of the fetus near term is a well-known feature of the diabetic pregnancy. One couldspeculate that cardiac arrythmia might be a cause ofthis phenomenon in the poorly-controlled diabeticpregnancy.The aetiology of the left ventricular outflow
obstruction in these infants is uncertain. It is possiblethat the septal hypertrophy was a part of thegeneralised increase in organ size of the large fordates infant of the diabetic mother.13 In favour of thishypothesis is the tendency for the hypertrophy toresolve during the first year of life in those infantsstudied by Gutgesell et al.4 We feel that our infantsdid not have any structural congenital heart diseasethat could account for the myocardial hypertrophy.It has been reported that left ventricular outflowobstruction occurs in 18% of infants of diabeticmothers whether or not symptoms are present.24
I thank Dr J P Brady and Dr T Hirata of theChildren's Hospital, San Francisco, and Dr GMcClure and Dr M Reid of the Royal MaternityHospital, Belfast, for allowing me to study newbornsadmitted under their care, Mrs Daisy Hogg fortechnical assistance with the echocardiograms,Dr D O'Hara for the pathological studies, Dr H CMulholland for advice on writing the manuscript,and Mrs Lynda Thompson for secretarial assistance.
References
Goodwin J F. A current appraisal of the cardiomyo-pathies. Hosp Update 1979; 5: 665-83.
2 Poland R L, Walther L J, Chang L. Hypertrophiccardiomyopathy in infants of diabetic mothers (abstract).Pediatr Res 1975; 9: 269.
3 Way G L, Ruttenberg H D, Eshaghpour E, Nora J J,Wolfe R E. Hypertrophic obstructive cardiomyopathy ininfants of diabetic mothers (abstract). Circulation 1976;53-54: Supplement II, 105.
4Gutgesell H P, Mullins C E, Gillette P C, Speer M,Rudolph A J, McNamara D G. Transient hypertrophicsubaortic stenosis in infants of diabetic mothers. JPediatr1976; 89: 120-5.White P. Pregnancy and diabetes, medical aspects. MedClin North Am 1965; 49: 1015-24.
on Novem
ber 13, 2020 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.56.4.258 on 1 April 1981. D
ownloaded from

Hypertrophic cardiomyopathy in infants ofpoorly-controlled diabetic mothers 2636 Thomson A M, Billewicz W Z, Hytten F E. The assess-ment of fetal growth. J Obstet Gynaecol Br Commonw1968; 75: 903-16.
7Hagan A D, Deely W J, Sahn D, Friedman W F. Echo-cardiographic criteria for normal newborn infants.Circulation 1973; 48: 1221-6.
8 Solinger R, Elbl F, Minhas K. Echocardiography in thenormal neonate. Circulation 1973; 47: 108-18.
9Lewis R P, Sandler H. Relationship between changes inleft ventricular dimensions and the ejection fraction inman. Circulation 1971 ; 44: 548-57.
10 Hirschfeld S S, Meyer R A, Schwartz D C, Korfhagen J,Kaplan S. Measurement of right and left ventricularsystolic time intervals by echocardiography. Circulation1975; 51: 304-9.Halliday H L, Hirschfeld S S, Riggs T, Liebman J,Fanaroff A A. Echographic ventricular systolic timeintervals in normal term and preterm neonates. Pediatrics1978; 62: 317-21.
12 Schulz D M, Giordano D A, Schulz D H. Weights oforgans of fetuses and infants. Arch Pathol 1962; 74:244-50.
13 Naeye R L. Infants of diabetic mothers: a quantitative,morphological study. Pediatrics 1965; 35: 980-8.
14 Henry W L, Clark C E, Epstein S E. Asymmetric septalhypertrophy; echocardiographic identification of thepathognomonic anatomic abnormality of IHSS. Circula-tion 1973; 47: 225-33.
15 Shah P M, Gramiak R, Adelman A G, Wigle E D. Role ofechocardiography in diagnostic and hemodynamicassessment of hypertrophic subaortic stenosis. Circulation1971; 44: 891-8.
16 Abbasi A S, MacAlpin R N, Eber I M, Pearce M L.Echocardiographic diagnosis of idiopathic hypertrophiccardiomyopathy without outflow obstruction. Circulation1972; 46: 897-904.
17 Boughner D R, Schuld R L, Persaud J A. Hypertrophicobstructive cardiomyopathy. Assessment by echocardio-graphic and Doppler ultrasound techniques. Br Heart J1975; 37:917-23.
18 Meyer R A. Subvalvular aortic stenosis. In: Meyer R A,ed. Pediatric echocardiography. Philadelphia: Lea &Febiger, 1977: 193.
91 Shand D G, Sell C G, Oates J A. Hypertrophic obstructivecardiomyopathy in an infant; propranolol therapy forthree years. NEnglJMed 1971; 285: 843-4.
20 Barr P A, Celermajer J M, Bowdler J D, Cartmill T B.Idiopathic hypertrophic obstructive cardiomyopatjhycausing severe right ventricular outflow tract obstructionin infancy. Br HeartJ 1973; 35: 1109-15.
21 Maron B J, Edwards J E, Henry W L, Clark C E,Bingle G J, Epstein S E. Asymmetric septal hypertrophy(ASH) in infancy. Circulation 1974; 50: 809-20.
22 Reid M McC, Reilly B J, Murdoch A I, Swyer P R.Cardiomegaly in association with neonatal hypo-glycaemia. Acta Paediatr Scand 1971; 60: 295-8.
23 Amatayakul 0, Cumming G R, Haworth J C. Associationof hypoglycaemia with cardiac enlargement and heartfailure in newborn infants. Arch Dis Child 1970; 45:717-20.
24 Mace S E, Hirschfeld S S, Riggs T W, Fanaroff A A,Merkatz I R, Liebman J. Cardiac hypertrophy in infantsof diabetic mothers: an echocardiographic study(abstract). Pediatr Res 1979; 13: 348.
Correspondence to Dr H L Halliday, The Queen'sUniversity of Belfast, Institute of Clinical Science,Grosvenor Road, Belfast BT12 6BJ.
Received 22 January 1980
on Novem
ber 13, 2020 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.56.4.258 on 1 April 1981. D
ownloaded from