Embed Size (px)
Citation preview

Journal of Neurology, Neurosurgery, and Psychiatry, 1975, 38, 1170-1176
Hypertrophic granulomatous cranial pachymeningitiscausing progressive blindness in a chronic
dialysis patientEARL R. FERINGA1 AND LEE WEATHERBEE
From the Departments of Neurology and Pathology, Veterans Administration Hospital, Ann Arbor, Michigani,U.S.A.
SYNOPSIS A patient on chronic haemodialysis because of renal failure developed progressivevisual field loss and eventual blindness. A postmortem examination indicated that the blindness wascaused by granulomatous thickening of the pachymeninges which constricted the optic nerves asthey passed through the optic foramina. Exhaustive bacteriological and histopathological studiesfailed to identify a specific cause for this hypertrophic cranial pachymeningitis.
A variety of unique disease processes in patientswith chronic renal failure whose lives have beenprolonged by haemodialysis have been describedin recent years. In most cases, it is unclearwhether these unusual pathological states arecoincidentally associated with chronic renaldisease and haemodialysis, are caused by supra-end-stage renal disease, or are the result ofhaemodialysis. In this paper we report a patientwho developed progressive visual field loss andeventually became blind. He had been on haemo-dialysis for two years because of chronic renalfailure due to rapidly progressive glomerulone-phritis. At postmortem examination both opticnerves were compressed by hypertrophic changesin the dura mater. The cause of these changes isunknown.
CASE HISTORY
In October 1971, a 50 year old white man first notedmalaise, weakness, nausea, and anorexia. He hadperipheral oedema, an elevated serum potassium(8.1 mmol/l), a blood urea nitrogen of 80.3 mmol/l,and a creatinine of 2376.0 ,umol/l (27 mg/dl). Thecause of his renal disease was not clearly defined.Antinuclear antibody tests, rheumatoid factorstudies, and antistreptolysin 0 titres were all normal.1 Reprint requests: Dr E. R. Feringa, Chief, Neurology ServiceVeterans Administration Hospital, 2215 Fuller Rd., Ann Arbor,Michigan 48105, U.S.A.(Accepted 24 June 1975.)
1170
He was first treated with peritoneal dialysis; then anarteriovenous fistula was placed and he was startedon a programme of haemodialysis.
Haemodialysis was continued three times a weekwith apparently good control of his uraemia. InMarch 1973 he noted the onset of hoarseness, aheadache on the left side, a pressure sensation in hisleft ear, and a decrease in hearing acuity. Directlaryngoscopy demonstrated paralysis of the leftvocal cord. Five days later another examiner feltthat the vocal cords were normal, although thepatient continued to have hoarseness. In May 1973he complained of visual difficulty and was found tohave a visual acuity (corrected) of 20/25 in the righteye and 20/60-1 in the left. Near vision was Jaeger 0in the right eye and Jaeger 13 in the left. Visual fieldexamination demonstrated a superior lateral visualfield defect in the left eye and the suggestion of asimilar defect in the right eye.A complete neurological evaluation was done in
June 1973. His visual fields appeared to be full onconfrontation testing. The disc margin was indis-tinct on the nasal side in the left optic fundus, butwas not considered definitely abnormal. The leftpalate was weak. There was decreased bulk andpower of the left sternocleidomastoid muscle andof the upper fibres of the left trapezius muscle. Thetongue appeared to deviate slightly to the left whenprotruded. Except for minimal evidence of a peri-pheral neuropathy manifest by decreased sensationand decreased deep tendon reflexes distally and sym-metrically, the findings of the rest of the neurological
guest. Protected by copyright.
on February 10, 2021 by
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.38.12.1170 on 1 Decem
ber 1975. Dow
nloaded from

Hypertrophic granulomatous cranial pachymeningitis
i j
examination were normal. A chest radiograph atthis time revealed two small 'coin lesions' in the rightinferior lung field. These were not present on earlierfilms. An electroencephalogram showed excessiveanterior amplitude with bianterior slow activity andbitemporal slow activity but no focal findings.A lumbar puncture in June 1973 showed an openingpressure of 220 to 230 mm of spinal fluid. The fluidcontained three red cells per ml and no white cells.The protein was 0.18 g/l, the glucose 3.55 mmol/lwith a simultaneous blood glucose of 5.72 mmol/l.A Gram stained smear of the spinal fluid showedno bacteria. Fungus cultures, bacterial cultures forpyogens and for tubercle bacilli, an India ink pre-
paration, and the VDRL test were all negative.An extensive evaluation for possible fungal or neo-
plastic disease was begun. Serum for fungal antigenswas negative for Blastomyces dermatitidis, Candidaalbicans, Coccidioides immitis, and Histoplasmacapsulatum (three strains). The sputum was exam-
ined for malignant cells on three occasions and nonewas found. Bronchial washings and bronchial brush-ings from three separate areas were obtained and allwere negative for neoplasia. An upper gastroin-testinal radiographic series was interpreted as show-ing an antral mass lesion with an ulcerated craterand two duodenal diverticulae. Gastric washings andgastric brushings showed no evidence of neoplasia.
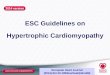
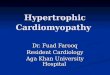
FIG. 1 A gross view of the skull cap atnecropsy showing the thickened duramater. Note the complete occlusion ofthe superior sagittal sinus.
Fibreoptic gastroscopy and biopsy failed to demon-strate tumour. A barium enema showed diverti-culosis without diverticulitis.
Skull radiographs with particular views of thejugular foramina and the optic foramina were normal.A brain isotope scan was read as probably abnormalwith increased uptake bilaterally in the frontal regionand near the sella turcica, but no definite mass couldbe identified. Periodic repeat chest radiographsdemonstrated continued gradual enlargement of the'icoin lesions' in the right lower lung zone.A sigmoidoscopy and a liver scan were normal. A
slide test for antinucleoproteins associated with lupuserythematosus was negative. The antinuclear anti-body test was negative again. A serum fluorescenttreponema antibody test was negative. The sedi-mentation rate of the blood was 64 mm/h. A tuber-culosis skin test with purified protein derivative wasnegative at 48 hours on two occasions.
In June 1973, a re-examination showed the cor-rected visual acuity in the right eye to be 20/30+2,and in the left eye, 20/300. The visual fields wereconstricted, and examination was limited by thepatient's poor cooperation, but it was felt that therewas a bitemporal superior field defect which wasworse in the left eye than in the right. Neurologicalexamination showed a questionable left superiorquadrant defect on confrontation visual fields.
1 171guest. P
rotected by copyright. on F
ebruary 10, 2021 byhttp://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.38.12.1170 on 1 D
ecember 1975. D
ownloaded from

1172~~~~~~Earl R. Feringa and Lee Weatherbee
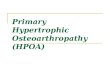
FIG. 2 The optic nerveswere compressed by thegreatly thickened dura mater.Dura mater at the base of theskull was 2 to 3 mm thickand had a lumpy appearanceand a yellowish colour in thefresh state.
444
44*4~~~~~~~~~~~~~~~2
.4444~~~~~~
..~~~~~ ~ ~ ~ ~ ~ ~ ~ ~ ~~~~4.4....
$ 4
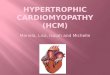
FIG.3 Area of the thickened dura mater showingareas of focal granulomatous inflammation andnecrosis. Note the increased collagen and foci ofchronic inflammatory cellular infiltrates. x SO.
The patient complained of pain in the left jaw andof left ear fullness. His tonsils were enlarged and hadpus-filled crypts. There were decreased bulk andpower of the sternocleidomastoid and the trapeziusmuscles on the left. A subsequent EMG, however,failed to reveal any significant evidence of dener-vation. A second set of skull films was reviewed withthe neuroradiologist, with special attention given tobase views, but no abnormality was found. Thepatientinsisted on being discharged from the hospital andwas allowed to go home with the understanding thatfurther evaluation of his lung nodules and neuro-logical status was imperative just as soon as hewould be willing to return to the hospital.Ten days later, while the patient was at home, he
lost all vision. He refused hospitalization, but for thenext week he claimed that after dialysis he some-times could see for a few minutes; then he wouldbecome blind again. When he was admitted oneweek after the onset of blindness, his pupils werefound to be 'dilated with no reaction to light. Defi-nite optic atrophy was not identified. There was noperception of light.A repeat gastroscopy demonstrated chronic in-
flammation of the stomach lining with no evidenceof tumour. A needle biopsy of the lung revealedacute and chronic inflammatory changes but no evi-dence of tumour. A repeat neurological examinationthree weeks after the onset of blindness revealed anormal mental status, except that the patient wasvery anxious about his condition. No light percep-tion was possible with either eye. The right pupil wasslightly larger and more irregular than the left, butboth pupils were dilated widely. The right pupil
1172guest. P
rotected by copyright. on F
ebruary 10, 2021 byhttp://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.38.12.1170 on 1 D
ecember 1975. D
ownloaded from

Hypertrophic granulomatous cranial pachymeningitis
reacted slightly to direct light stimulation, but therewas no consensual response. The left pupil did notrespond to any light stimulus. The patient's voiceremained hoarse. There was minimal decrease in thenasolabial fold on the right as compared with theleft.
Another lumbar puncture revealed normal pres-sure and crystal clear fluid. Four red cells per mm3and no white cells were seen on microscopic exam-ination. The spinal fluid protein was 0.15 g/l andthe glucose 3.94 mmol/l. The VDRL was negative.India ink preparations, cultures for fungus, andsmears and cultures for bacteria were negative. Fourvessel cerebral angiography was done and no definiteabnormality was found. The patient was dischargedwithout definite diagnosis and continued on hishaemodialysis programme.
In October the patient had a regularly scheduledhaemodialysis. After returning home he developedan extremely severe headache. He became less re-sponsive and lapsed into coma within three hours. Alumbar puncture revealed an opening pressure of500mm of grossly bloody spinal fluid. When the fluidwas centrifuged, the supernatant was mildly xantho-chromic. Despite treatment, he died, two years afterthe onset of haemodialysis for renal disease and threemonths after the onset of blindness.
PATHOLOGICAL FINDINGS
A large recent intracerebral haematoma involved thesurface and extended deeply into the occipital andparietal areas of the right cerebral hemisphere. The
*5 '' ah£ ' a*F Fr.'.~NAt; <<
S ;UA_.5
e b**;_
>,$z.* > v4a_^t.* . _ ,*..F,7
h9s < e 3*§+ S.Ag..'"< a PBN 0o;9~~~~~~~4sp
. >,;.ASw. -w..; P.. W* .-.:..,.. .~~~~.. leptomeninges were otherwise smooth and glistening.
The dura mater was markedly thickened, irreg-ular, and yellow coloured. Over the base of the skullthe dura mater was 2 to 3 mm thick. Over the con-vexities it was 1 to 2 mm thick (Fig. 1). The duramater was particularly thick in the area of the opticforamina and appeared to be constricting the opticnerves bilaterally (Fig. 2). Thickened and irregulardura mater was noted also in the area of the jugularforamen bilaterally, and there was destruction ofbone in that region. In all areas the microscopicchanges of the dura mater were rather uniform andconsisted of confluent granulomas, often with prom-inent areas of necrosis and considerable fibrosis(Figs 3 and 4). Infiltrates of chronic inflammatorycells included lymphocytes, plasma cells, and scat-tered eosinophils. A few giant cells were seen ad-jacent to the necrosis.
There was erosion of the petrous portion of theleft temporal bone which permitted communicationof the left mastoid air cells with the epidural space.No definite aetiology for the destruction of the bonewas determined. The superior sagittal sinus wasobliterated by granulomatous pachymeningitis.A broad based 3 x 1.5 cm anterior lower lobe scar
was seen on the pleural surface of the right lung.Beneath this pleural scar there was a cheesy necroticarea measuring 5 x 4 cm. Microscopically, this lesionconsisted of granulomatous tissue with lymphocytesand eosinophils similar to the granulomatous in-volvement of the dura mater. The necrosis, however,was more extensive and acute inflammatory cellswere more prominent.
FIG. 4 High power view ofan area showing histiocytescharacteristic ofgranulomatousinflammation. Scatteredlymphocytes are also seen andoccasional polymorphonuclearleucocytes are seen at theedges of the picture adjacentto areas of necrosis. x 440.
1173
guest. Protected by copyright.
on February 10, 2021 by
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.38.12.1170 on 1 Decem
ber 1975. Dow
nloaded from

Earl R. Feringa and Lee Weatherbee
The kidneys weighed 75 g each. The capsulesstripped with ease but the cortical surface was finelygranular and pale tan-white. The cortex averaged2 mm in thickness. The cortical medullary junctionswere indistinct and the medulla was poorly striated.The pyramids were blunted and the pelves andcalyces slightly dilated. There was increased peri-pelvic fat and the renal vessels were patent. Nearlyall glomeruli were sclerotic. Arterial and arterio-losclerosis was prominent. Focal chronic inflamma-tory infiltrates, tubular atrophy and dilatation, andvery rare foci of acute inflammatory cells were notedadjacent to small areas of necrosis.No abnormalities were noted in the stomach.The granulomatous areas of the dura mater and
lung were examined further by special stains. Silvermethenamine and PAS stains for fungi were nega-tive. Levaditi stains for spirochaetes and acid faststains for tubercle bacilli were also negative. Brownand Brenn stains did not demonstrate the presence ofbacteria. Cultures of the dura mater for mycobac-teria, fungi, and pyogenic bacteria were negative.
DISCUSSION
The existence of disease states which causehypertrophy of the pachymeninges and neuro-logical abnormalities have been discussed byseveral authors. Gowers (1893) describes pachy-meningitis as either external or internal depend-ing on the direction of insult to the dura mater.In his description 'external pachymeningitis isalmost always secondary to injury or to adjacentdisease...' He describes cases in which localtrauma or infection of the bones of the skullresulted in local inflammation of and somethickening of the dura mater. He does not dis-cuss a more diffuse problem such as is demon-strated by our patient. While our patient didhave ear symptoms of fullness and hearing lossand at postmortem examination showed localdestruction of bone in the area of the leftpetrous pyramid, the involvement of the duramater was not local but rather spread exten-sively over the entire inner table of the skull.Gowers further divides internal pachymen-
ingitis into purulent and haemorrhagic types.The purulent type seems to be associated withpurulent infection of the subarachnoid space, aninfection which our patient clearly did not have.His 'haemorrhagic internal pachymeningitis'seems to correlate best with what would now becalled chronic subdural haematoma. The patho-
logical findings in his cases of much blood andblood pigment and many large capillaries in thehypertrophic dura mater are all very differentfrom the granulomatous tissue in our case.
Patients on chronic haemodialysis have a ten-dency to bleed for several reasons. In our patientthe terminal event was a massive intracerebralhaematoma. However, the clinical course of thispatient was not one of multiple clinical episodescompatible with repeated subdural haemorrhages.When checked at various times the spinal fluidnever showed more than a few red blood cellsand always had low normal CSF proteins. Thefindings at postmortem examination showedonly minimal evidence of haemorrhage. Thishaemorrhage was very acute. It involved onlythe inner surface of the dura mater adjacent tothe area of acute intracerebral haemorrhagewhich was the patient's terminal event. Thelayering of fibrous tissue, excessive blood pig-ments, and multiple large capillary spaces de-scribed by Gowers were all missing in this case.While CSF findings are not described by
Gowers, his description of the involvement ofadjacent arachnoid and pia mater by'. . . peculiarmembranous tissue' would make it unlikely thatsuch patients would have normal CSF. WhileGowers's list of symptoms ascribed to haemorr-hagic internal pachymeningitis resembles a listof the ills which befall mankind's brain, blind-ness is notably absent.Wilson (1940) has also discussed pachymen-
ingitis. His discussion parallels that of Gowers.Again, the external variety of pachymeningitisis most closely associated with local disease pro-cesses and is not described as causing a diffusecranial hypertrophic reaction. His description of'pachymeningitis haemorrhagica interna' againseems to correlate poorly with the history andfindings in our case, and much better withchronic subdural haematoma. Blindness is notdescribed as a sign of this disease by Wilson.
In both Gowers's and Wilson's discussions theaetiology of many cases is ascribed to syphilis,tuberculosis, or perhaps alcohol. Modern neuro-pathologists would probably hold that thesediscussions present inadequate proof to establisha cause and effect relationship, except in the casewhere the infection of the dura mater was assoc-iated with leptomeningitis caused by syphilis ortuberculosis. The more chronic cases without
1174
guest. Protected by copyright.
on February 10, 2021 by
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.38.12.1170 on 1 Decem
ber 1975. Dow
nloaded from

Hypertrophic granulomatous cranial pachymeningitis
involvement of the leptomeninges are probablysimply unexplained.
Better known is hypertrophic cervical pachy-meningitis (Charcot, 1873). This disease is notlimited to the cervical spinal area, nor is itlimited to the dura mater. Rather 'the neigh-bouring leptomeninx always suffers as well, be-coming opaque and thick, and firmly united tothe dura and cord. . .' (Wilson, 1940). But thisdisease is not described as involving the intra-cranial dura mater, and blindness is not a resultof this infection. Hypertrophic pachymeningitisaffecting areas other than the spinal dura materis not described in modern neurology texts.Astrom and Lidholm (1963) described a case
of granulomatous inflammation of the orbitwhich, at postmortem examination, was foundto have spread into the cerebral subarachnoidspace as well as to other adjacent tissues. Thisoccurred in a patient with well-established per-iarteritis nodosa. The authors discuss a possiblerelation to Wegener's granulomatosis. Thelesions described are very different from those ofour case. (1) Grossly, the lesions involved thesubarachnoid space, while our case had a normalsubarachnoid area. (2) Histologically, the lesionswere characterized by vasculitis with associatedchronic and acute infection, while our caseshowed almost no vascular involvement. (3)Clinically, the intracranial lesion was an inci-dental terminal spread of an otherwise obviousorbital granuloma, while in our case the presenceof granuloma intracranially was completelyhidden until postmortem examination.We have also considered that our patient's
disease process might be an example of Wegner'sgranulomatosis. If his kidney disease be con-sidered along with his lung lesions and cerebralsymptoms, this might be a unifying diagnosis. Inthe end, however, we have rejected this diagnosison both clinical and pathological grounds.
Clinically, Wegener's granulomatosis is at besta poorly defined entity (Wolff et al., 1974).Almost all patients with this disease show evi-dence of sinus or nasopharyngeal inflammatorydisease. Symptoms of such were lacking in thispatient, and even a retrospective review of twosets of sinus films taken after his symptoms beganrevealed only minimal thickening of the mucosaof the ethmoid sinuses. No active sinus inflam-mation or infection can be identified on any film.
A variety ofneurological complaints have beenlisted as associated with Wegener's granuloma-tosis (Drachman, 1963). Patients have lesionscaused by vasculitis. Peripheral neuropathies arethe most common neurological manifestation.Ocular signs associated with necrotic granulomasof the orbit, of the eye, and lesions of the third,fourth, and sixth cranial nerves are described(Straatsma, 1957), but visual field loss or blind-ness is notably absent. Although survival up tothree years has been reported in patients withWegener's granulomatosis (Godman and Churg,1954), most cases die in two to five months. Ifthe original kidney disease be considered part ofthe same disease, our patient had a survival oftwo years.One report (Rogers and Roberto, 1956) de-
scribes focal involvement of the dura materadjacent to the left superior orbital fissure withcomplete internal and external ophthalmoplegiaon that side. An exploratory subtemporal crani-ectomy revealed a markedly thickened duramater with yellowish-grey granulations, an in-creased vascularity, and a gelatinous appear-ance. Postoperatively, the patient became blindin that eye. That patient died five months laterafter he developed both extensive local disease inthe eye and orbit and extensive upper and lowerrespiratory disease. The necropsy showed'. . marked fibrosis and inflammation of thedura due to acute vasculitis'. The extent of in-volvement of the dura mater, the leptomeninges,and/or the brain is not described, nor is blindnesson the right side.
Pathologically, Wegener's granulomatosis is anecrotizing granulomatous vasculitis (Godmanand Churg, 1954). In our patient, some bloodvessels were involved in the granulomatous pro-cesses, but this appeared to be quite coincidentalto the diffuse involvement of adjacent tissue. Noevidence of primary granulomatous vasculitiswas found in evaluation of dura mater, kidney,or lung lesions.We report a case of progressive blindness in a
patient on a programme of chronic renaldialysis. At postmortem examination a chroniccerebral granulomatous pachymeningitis of un-certain aetiology was found to have constrictedboth optic nerves. Exhaustive efforts to identifythe cause of this granulomatous thickening ofthe dura mater have been unsuccessful. Because
1175
guest. Protected by copyright.
on February 10, 2021 by
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.38.12.1170 on 1 Decem
ber 1975. Dow
nloaded from

Earl R. Feringa and Lee Weatherbee
of the palisading histiocytes, the character of thenecrosis, and the scattered eosinophils, we haveconcluded that the best pathological descriptionis that of nonspecific allergic granulomatosis. Wecan find no reports of similar cases. We hope our
report will stimulate others to be aware of thisunusual cause of progressive visual field loss andeventual blindness.
This project was supported by institutional researchfunds of the Veterans Administration Hospital at AnnArbor, Michigan.
REFERENCES
Astr6m, K. E., and Lidholm, S. 0. (1963). Extensive intra-cranial lesions in a case of orbital non-specific granulomacombined with polyarteritis nodosa. Journal of ClinicalPathology, 16, 137-143.
Charcot, J. M. (1873). Seance du 13 mai. Conmptes Rendus desSeances de la Societe de Biologie, Serie Se iii, 1871, 32-38.
Drachman, D. A. (1963). Neurological complications ofWegener's granulomatosis. Archives of Neurology, 8,145-155.
Godman, G., and Churg, J. (1954). Wegener's granuloma-tosis. Archives of Pathology, 58, 533-553.
Gowers, W. R. (1893). A Manual of Diseases of the NervousSystem, vol. 2, 2nd edn., pp. 323-328. Hafner: Darien.
Rogers, J. V., and Roberto, A. E. (1956). Circumscribed pul-monary lesions in periarteritis nodosa and Wegener'sgranulomatosis. American Journal of Roentgenology, 76,88-93.
Straatsma, B. R. (1957). Ocular manifestations of Wegener'sgranulomatosis. American Journal of Ophthalmology, 44,789-799.
Wilson, S. A. K. (1940). Pachymeningitis. In Neurology,vol. I, pp. 4-8. Edited by A. N. Bruce. Butterworths:London.
Wolff, S. M., Fauci, A. S., Horn, R. G., and Dale, D. C.(1974). Wegener's granulomatosis. Annals of InternalMedicine, 81, 513-525.
1176
guest. Protected by copyright.
on February 10, 2021 by
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.38.12.1170 on 1 Decem
ber 1975. Dow
nloaded from













![GENETIC BASIS OF HYPERTROPHIC CARDIOMYOPATHYThroughout the years, names such as idiopathic hypertrophic subaortic stenosis[5], muscular subaortic stenosis[6] and hypertrophic obstructive](https://img.pdfslide.net/doc/110x75/60571329c95e4748070a14f6/genetic-basis-of-hypertrophic-cardiomyopathy-throughout-the-years-names-such-as.jpg)