Embed Size (px)
Citation preview
1140
6. Wnght CA, Southgate VR, Knowles RJ. What is Schistosoma intercalatum Fisher1934?. Trans R Soc Trop Med Hyg 1982; 66: 28-56.
7. Muller RL, Taylor MG. On the use of the Ziehl-Neelsen technique for specificidentification of schistosoma eggs. J Helmintol 1972; 42: 139-42.
8. Burchard GD, Kern P. Probable hybridization between S intercalatum andS haematobium in Western Gabon. Trop Geogr Med 1985; 37: 119-23.
HYPNOSIS FOR INTRACTABLE VOMITING
SIR,-A 57-year-old woman was admitted to hospital in
November, 1986, for malignant ascites 8 years after surgery andradiotherapy for bilateral breast cancer. Severe emesis (six to tenepisodes a day) was noted for 9 months. Endoscopy, a barium meal,and an abdominal scan suggested gastric and jejunal compression byperitoneal tumours. Neither parenteral drugs (methylprednisolone20 mg, metoclopramide 60 mg, chlorpromazine 50 mg, alizapride100 mg) or ranitidine (300 mg daily) were very effective in
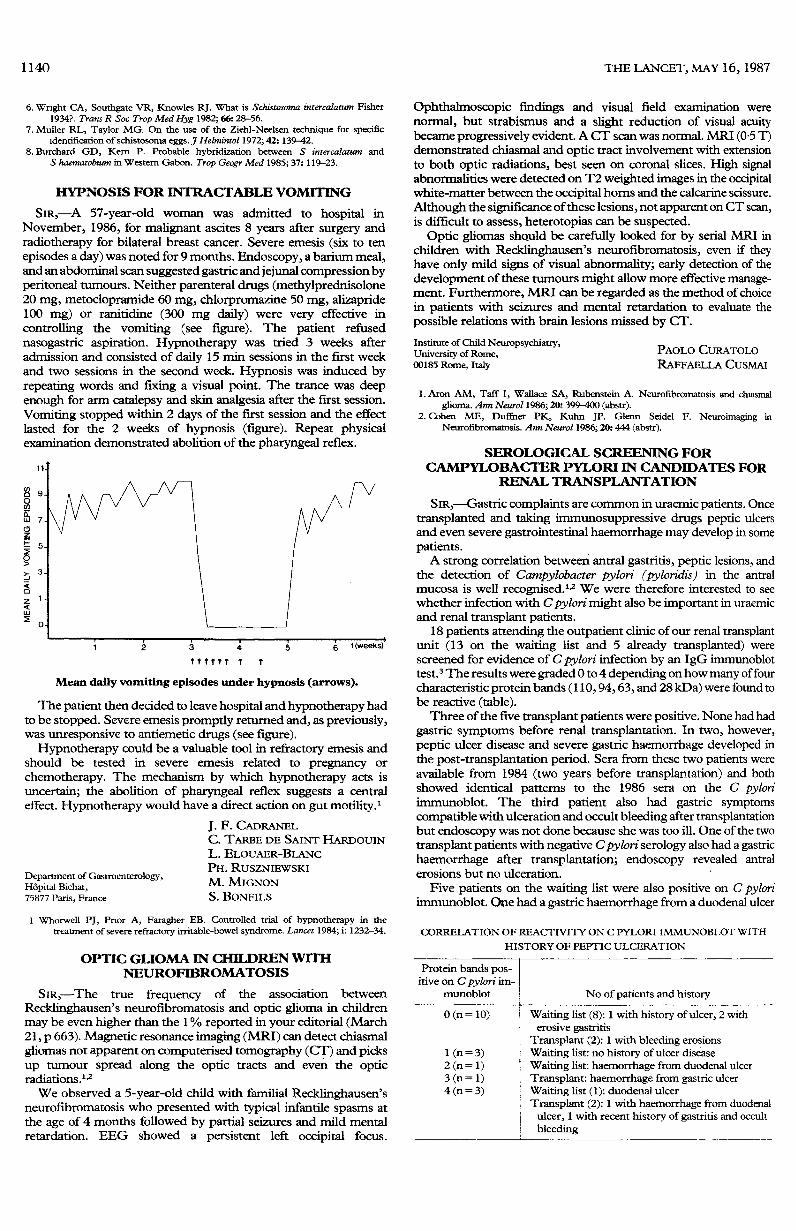
controlling the vomiting (see figure). The patient refused
nasogastric aspiration. Hypnotherapy was tried 3 weeks afteradmission and consisted of daily 15 min sessions in the first weekand two sessions in the second week. Hypnosis was induced byrepeating words and fixing a visual point. The trance was deepenough for arm catalepsy and skin analgesia after the first session.Vomiting stopped within 2 days of the first session and the effectlasted for the 2 weeks of hypnosis (figure). Repeat physicalexamination demonstrated abolition of the pharyngeal reflex.
Mean daily vomiting episodes under hypnosis (arrows).
The patient then decided to leave hospital and hypnotherapy hadto be stopped. Severe emesis promptly returned and, as previously,was unresponsive to antiemetic drugs (see figure).Hypnotherapy could be a valuable tool in refractory emesis and
should be tested in severe emesis related to pregnancy or
chemotherapy. The mechanism by which hypnotherapy acts isuncertain; the abolition of pharyngeal reflex suggests a centraleffect. Hypnotherapy would have a direct action on gut motility. 1
Department of Gastroenterology,Hôpital Bichat,75877 Paris, France
J. F. CADRANELC. TARBE DE SAINT HARDOUINL. ELOUAER-BLANCPH. RUSZNIEWSKIM. MIGNONS. BONFILS
1 Whorwell PJ, Pnor A, Faragher EB. Controlled trial of hypnotherapy in thetreatment of severe refractory irritable-bowel syndrome. Lancet 1984; i: 1232-34.
OPTIC GLIOMA IN CHILDREN WITHNEUROFIBROMATOSIS
S!R,—The true frequency of the association between
Recklinghausen’s neurofibromatosis and optic glioma in childrenmay be even higher than the 1 % reported in your editorial (March21, p 663). Magnetic resonance imaging (MRI) can detect chiasmalgliomas not apparent on computerised tomography (CT) and picksup tumour spread along the optic tracts and even the opticradiations. 1.2We observed a 5-year-old child with familial Recklinghausen’s
neurofibromatosis who presented with typical infantile spasms atthe age of 4 months followed by partial seizures and mild mentalretardation. EEG showed a persistent left occipital focus.
Ophthalmoscopic findings and visual field examination werenormal, but strabismus and a slight reduction of visual acuitybecame progressively evident. A CT scan was normal. MRI (0-5 T)demonstrated chiasmal and optic tract involvement with extensionto both optic radiations, best seen on coronal slices. High signalabnormalities were detected on T2 weighted images in the occipitalwhite-matter between the occipital horns and the calcarine scissure.Although the significance of these lesions, not apparent on CT scan,is difficult to assess, heterotopias can be suspected.
Optic gliomas should be carefully looked for by serial MRI inchildren with Recklinghausen’s neurofibromatosis, even if theyhave only mild signs of visual abnormality; early detection of thedevelopment of these tumours might allow more effective manage-ment. Furthermore, MRI can be regarded as the method of choicein patients with seizures and mental retardation to evaluate thepossible relations with brain lesions missed by CT.
Institute of Child Neuropsychiatry,University of Rome,00185 Rome, Italy
PAOLO CURATOLORAFFAELLA CUSMAI
1. Aron AM, Taff I, Wallace SA, Rubenstein A. Neurofibromatosis and chiasmalglioma. Ann Neurol 1986; 20: 399-400 (abstr).
2.Cohen ME, Duffner PK, Kuhn JP. Glenn Seidel F. Neuroimaging inNeurofibromatosis. Ann Neurol 1986; 20: 444 (abstr).
SEROLOGICAL SCREENING FORCAMPYLOBACTER PYLORI IN CANDIDATES FOR
RENAL TRANSPLANTATION
SIR,--Gastric complaints are common in uraemic patients. Oncetransplanted and taking immunosuppressive drugs peptic ulcersand even severe gastrointestinal haemorrhage may develop in somepatients.A strong correlation between antral gastritis, peptic lesions, and
the detection of Campylobacter pylori (pyloridis) in the antralmucosa is well recognised. 1,2 We were therefore interested to seewhether infection with C pylori might also be important in uraemicand renal transplant patients.
18 patients attending the outpatient clinic of our renal transplantunit (13 on the waiting list and 5 already transplanted) werescreened for evidence of C pylori infection by an IgG immunoblottest.3 The results were graded 0 to 4 depending on how many of fourcharacteristic protein bands (110, 94, 63, and 28 kDa) were found tobe reactive (table).Three of the five transplant patients were positive. None had had
gastric symptoms before renal transplantation. In two, however,peptic ulcer disease and severe gastric haemorrhage developed inthe post-transplantation period. Sera from these two patients wereavailable from 1984 (two years before transplantation) and bothshowed identical patterns to the 1986 sera on the C pyloriimmunoblot. The third patient also had gastric symptomscompatible with ulceration and occult bleeding after transplantationbut endoscopy was not done because she was too ill. One of the twotransplant patients with negative C pylori serology also had a gastrichaemorrhage after transplantation; endoscopy revealed antralerosions but no ulceration. ’
Five patients on the waiting list were also positive on C pyloriimmunoblot. One had a gastric haemorrhage from a duodenal ulcer
CORRELATION OF REACTIVITY ON C PYLORI IMMUNOBLOT WITH
HISTORY OF PEPTIC ULCERATION



















![Hypnosis William Hewitt - Hypnosis for Beginners[2003]](https://img.pdfslide.net/doc/110x75/552115f3497959734d8b4612/hypnosis-william-hewitt-hypnosis-for-beginners2003.jpg)