Embed Size (px)
Citation preview

MINI-SYMPOSIUM: LESS COMMON SHOULDER PROBLEMS
(i) The management ofirreparable rotator cuff tearsJ Charles Talbot
David Limb
AbstractThe management of massive irreparable rotator cuff tears can be chal-
lenging. There are, however, a number of operative and non-operative
options available to the shoulder surgeon.
Non-operative management with simple analgesics, steroid injections
and a deltoid re-education programme may be appropriate for patients
with few symptoms, particularly elderly, lower demand patients with lower
expectations. In more symptomatic patients, especially younger patients
with higher demands, surgical interventionmaybe considered. Arthroscopic
debridement and/or, sub-acromial decompression (with or without biceps
tenotomy) may suffice, but partial or augmented rotator cuff repair or
tendon transfer surgery is available. In the presence of arthrosis, cuff tear
arthroplasty or reverse geometry arthroplasty are valid options.
Treatment should be individualized depending on the patient’s symp-
toms, age, expectations, needs and the presence or absence of associated
glenohumeral joint arthrosis.
Keywords irreparable rotator cuff tear; partial cuff repair; reverse
geometry shoulder arthroplasty; tendon transfer surgery
Introduction
The management options of irreparable rotator cuff tears (IRCT)
are diverse and treatment choice is informed by patient symp-
toms, age, expectations, needs and the presence or absence of
associated glenohumeral joint arthrosis. This review aims to
highlight the alternatives, both operative and non-operative, and
present a treatment algorithm for the management of patients
with irreparable rotator cuff tears.
The rotator cuff
The rotator cuff comprises four muscles arising from the scapula,
which merge to form a confluent tendinous hood or sleeve
around the humeral head. The rotator cuff contributes to
shoulder movements and acts to stabilize the glenohumeral joint.
While the static stabilizers such as the glenohumeral ligaments of
the joint are employed at end ranges of movement, the joint gains
significant mid range stability from the rotator cuff itself. The cuff
J Charles Talbot MBChB MSc(Eng) FRCS(Tr&Orth) SpR., Department of Ortho-
paedics and Trauma, Leeds General Infirmary, Leeds, UK. Conflicts of
interest: none declared.
David Limb BSc FRCSEd(Orth) Consultant Orthopaedic Surgeon, Depart-
ment of Orthopaedics and Trauma, Leeds General Infirmary, Leeds, UK.
Conflicts of interest: none declared.
ORTHOPAEDICS AND TRAUMA 26:6 367
acts to maintain the humeral head centred within the glenoid
concavity and resists upward translation of the humeral head
during abduction caused by activation of the deltoid muscle, in
what is known as the coronal force couple.1 Normal shoulder
kinematics relies on a similar antero-posterior antagonistic force
couple of the subscapularis and infraspinatus/teres minor
tendons. Burkhart et al. developed this line of thinking, which
gave rise to the biomechanical concept of partial rotator cuff
repair, which has been described as anatomically deficient but
biomechanically intact,2,3 and will be discussed later.
The rotator cuff is liable to injury and the intrinsic and extrinsic
theories of rotator cuff tear have been proposed and much
debated. The extrinsic, or impingement, theory relates cuff
damage to repetitive micro trauma of the tendon under the
acromion, resulting in cuff tears. The morphology of the acromion
has been implicated, with more rotator cuff tears seen in patients
with Bigliani type II (curved) and III (hooked) acromions.4 Simi-
larly, the non-operative management of cuff tears is progressively
less effective in type II (curved) and type III (hooked) acromions
respectively in comparison to type I (flat) acromions, supporting
the theory. The intrinsic theory however considers degeneration
of the rotator cuff with age, with relative devascularization of the
tendon, making the cuff more prone to injury.
Massive IRCTs are not common and in most series the inci-
dence of massive tears is about a third of all cuff tears, and even
this may be a result of selection bias. There are two types of
massive rotator cuff tear: antero-superior and, more commonly,
postero-superior. Postero-superior tears involve the supra- and
infra-spinatus but can involve the teres minor. Antero-superior
deficiency is seen with massive retracted subscapularis tears in
combination with supraspinatus tears; these tears inevitably
involve the biceps tendon which often subluxes medially. Signif-
icant tears result in a loss of the normal shoulder kinematics, and
proximalmigration of the humeral headmay result. Arthrosismay
or may not be present at presentation; abnormal shoulder kine-
matics and an adverse biological environment are proposed as the
causative contributors to the development of the arthropathy.
Patients with massive IRCT present with a wide variety of
symptoms from mild pain with little functional deficit to severe
debilitating pain and pseudo-paralysis, and the treatment should
be tailored to symptoms and expectations.
Irreparable rotator cuff tears
Clinical findings, imaging and arthroscopic assessment
Patients with massive IRCT present with variable amounts of
pain and functional loss. In cases with postero-superior tears,
functional loss typically results from weakness in abduction and
external rotation. Loss of active external rotation can occur in
isolation but may be combined with loss of active elevation.
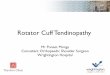
Clinically, wasting of both the supra- and infra-spinatus fossae
may be apparent (Figure 1). An external rotation lag sign may be
elicited and, if the tear involves the teres minor, a Hornblower’s
sign will be identified.5 In antero-superior tears patients report
pain and functional loss that typically stems from poor elevation
and abduction. Clinically an increase in passive external rotation
with a deficiency of internal rotation power is seen. The sub-
scapularis belly press, bear hug and Gerber’s lift-off tests will be
positive.
� 2012 Elsevier Ltd. All rights reserved.
Figure 1 A patient with hollowing of the supraspinatus and infraspinatus
fossae due to wasting of the muscles consequent upon a massive rotator
cuff tear.
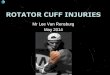
Figure 2 Plain AP radiograph of the shoulder showing rotator cuff
arthropathy, with upward migration of the humeral head, which is
beginning to articulate against the acromion with loss of the normal
acromiohumeral space and sub-acromial sclerosis.
MINI-SYMPOSIUM: LESS COMMON SHOULDER PROBLEMS
Plain radiographs of the shoulder may show proximal
migration of the humerus, with a reduced acromio-humeral
interval (AHI) in massive cuff tears (Figure 2). The normal AHI
measures 7e14 mm in healthy shoulders and is reduced in
massive IRCTs. The AHI has been shown to correlate with the
size of the tear and, with time, the interval has been shown to
reduce further.6 The plain radiograph will also confirm the
presence or absence of associated rotator cuff arthropathy, which
may alter the management options available. Ultrasound scan-
ning can confirm the presence of a massive tear and delineate the
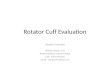
involved tendons, whilst an MRI scan will provide information
regarding the extent and retraction of the tear (classified in the
frontal plane by Patte) and the level of atrophy and fatty infil-
tration of the individual muscles (Figure 3), although Goutallier’s
original four stage classification of fat atrophy was based on
computerized tomography (CT). CT arthrography can therefore
be used successfully to define the outline of the tear, its retraction
and the degree of fatty degeneration, though MRI is more widely
used in the UK.
Direct visualization and manipulation during arthroscopic
evaluation of a rotator cuff tear is the gold standard for deter-
mining its reparability. The tendon and bone quality can be
assessed, as can the quality of the articular surfaces of the
humerus and glenoid. The tendon edges can be assesses for
mobility, before and after any necessary bursal releases or
interval slides (see later), and it will also allow an assessment of
whether a partial rotator cuff repair is viable or not.
Figure 3 MR imaging showing wasting and fatty infiltration of both
Definitionsupraspinatus and infraspinatus (arrows) due to a massive rotator
cuff tear.
Massive rotator cuff tears have been classified as those greater
than 5 cm in size, involving at least two tendons,7 though as yet
ORTHOPAEDICS AND TRAUMA 26:6 368
there is no universally accepted definition of an irreparable cuff
tear. Size and retraction of the tear have been used as indicative
measures,7,8 though Gerber et al9,10 also incorporated the ease
with which the tendon could be mobilized to restore it to its
normal site of insertion in their classification. Tears were deemed
irreparable if the rotator cuff tendon edges could not be reduced
to the tuberosities without excessive tension with the shoulder
abducted to 60�.9,10
� 2012 Elsevier Ltd. All rights reserved.

MINI-SYMPOSIUM: LESS COMMON SHOULDER PROBLEMS
The presence of a symptomatic massive irreparable rotator
cuff tear represents a significant therapeutic challenge. The
management options, both surgical and non-surgical, are plen-
tiful and are shown in Table 1; these will be discussed in more
detail.
Non-operative management
Non-operative management should always be considered as an
option, particularly in the older, lower demand patient with few
symptoms. Regular simple analgesics, possibly intra-articular
steroid injections, and activity adaptations may suffice.
However, strengthening the anterior deltoid and peri-scapular
musculature with movement and proprioception training under
physiotherapy guidance has been shown to be effective in large
rotator cuff tears.11e13 Levy et al13 demonstrated a 37 point
increase in the Constant score (from 26 to 63 points) following
a deltoid re-education programme in elderly patients who were
unsuitable for surgical intervention. This management option
should therefore be the mainstay of initial treatment of elderly
patients with symptomatic massive rotator cuff tears, in the
absence of arthrosis.
Operative management
There are a number of operative interventions in the armamen-
tarium of the shoulder surgeon, and decision making should be
individualized.
Arthroscopic debridement D/L sub-acromial
decompression D/L biceps tenotomy
The least invasive surgical option is an arthroscopic washout,
with rotator cuff, synovial and joint surface debridement.
A limited arthroscopic sub-acromial decompression (ASD),
preserving the coraco-acromial ligament (CAL) by undermining,
can also be performed and biceps tenotomy can also be consid-
ered, particularly if the tendon is degenerate and subluxing. This
option should be reserved for lower demand, elderly patients in
whom pain is the chief complaint, as function will not be
addressed directly though may still improve significantly if pain
is the main inhibitor of muscle function. A post-operative deltoid
rehabilitation programme should be included in the management
of these patients.
Open debridement and sub-acromial decompression of
massive rotator cuff tears has been reported, with successful
Non-operative Operative e no arthrosis
Simple analgesics
Corticosteroid injections
Adaptation of daily living activities
Deltoid re-education programme
Arthroscopic debridement þ/�decompression þ/� biceps ten
Supra-scapular nerve ablation
Tuberoplasty
Partial rotator cuff repair
Augmented rotator cuff repair
Tendon transfer surgery
? Reverse geometry arthroplas
Treatment options for massive, irreparable rotator cuff tears
Table 1
ORTHOPAEDICS AND TRAUMA 26:6 369
outcomes reported for pain relief by Rockwood8 and Gartsman,14
though less favourable outcomes for functional gain were noted.
Arthroscopic techniques are now favoured and the results are
similar, with improved pain scores but again limited gains in
strength are achieved.2
Techniques of limited sub-acromial decompression with
preservation of the CAL have been advocated to reduce the risk
of antero-superior escape. It is worth noting, however, that
Rockwood’s8 original description of his open technique divided
the CAL without there being any reported adverse effects;
however preserving the CAL is recommended on a theoretical
basis in the operative management of these patients.
Biceps tenotomy may be considered controversial in patients
with massive IRCTs due to fears of exacerbating proximal
humeral migration. The biceps tendon has been considered to
be a humeral head depressor, though reports of tenotomy per-
formed with or without arthroscopic decompression have
shown improvement in pain scores and statistically significant
improvements in the Constant and American Shoulder and
Elbow Surgeons (ASES) scores post-operatively.15e17 In
younger, more active patients biceps tenodesis, rather than
tenotomy, has been advocated to reduce muscle weakness and
the associated cosmetic deformity of a long head of biceps
tenotomy.18 However, it is more likely that this group of
patients will undergo more interventional reconstructive
procedures, as described later, rather than opt for debridement
and tenodesis.
Unfortunately, the short term benefits of debridement and
decompression are not maintained with time and there are
reports of deterioration in symptoms in the medium term.19 The
benefits however are shorter operative times, faster rehabilitation
and lower complications rates in comparison to more interven-
tional surgical options.
Tuberoplasty or reverse sub-acromial decompression
Reverse sub-acromial decompression or tuberoplasty has been
advocated on the basis that debridement of the tuberosity, with
or without biceps tenotomy, preserves the integrity of the coraco-
acromial arch (under surface of the acromion, the CAL and the
coracoid), and reduces the risk of antero-superior escape of the
humeral head when compared with classical sub-acromial
decompression. Outcomes are reported to be similar to ASD with
regard to pain relief, function and subjective satisfaction in the
mid-term.20
Operative with arthrosis
sub-acromial
otomy
ty
Arthroscopic debridement þ/� sub-acromial
decompression þ/� biceps tenotomy
Supra-scapular nerve ablation
Cuff tear arthroplasty (CTA)
Reverse geometry arthroplasty
� 2012 Elsevier Ltd. All rights reserved.

MINI-SYMPOSIUM: LESS COMMON SHOULDER PROBLEMS
Supra-scapular nerve ablation
The supra-scapular nerve (SSN) provides around 70% of the
sensory innervation to the shoulder joint via its inferior and
superior articular branches.21 The nerve passes through the
supra-scapular notch, where it underlies the transverse scapula
ligament, to enter the supraspinatus fossa and it goes on to
supply both the supra- and infraspinatus muscles. SSN blocks
have been used successfully to modify shoulder pain from
different pathologies, utilizing many techniques22 and forms the
basis for the rationale that SSN ablation will block the sensori-
neural pathway and improve pain scores. Pulsed radiofrequency
ablation has been shown to be effective in improving shoulder
related pain in rotator cuff disease, with or without glenohumeral
joint arthrosis, though this may be a relatively short-lived
benefit. Kane et al22 reported their findings and showed statisti-
cally significant improvements in pain as assessed by a visual
analogue scale. These improvements were not, however, fully
maintained after 3 months. Nizlan et al23 reported a technique of
arthroscopic neurectomy of the SSN with good levels of pain
relief in patients with various shoulder pathologies, but
predominantly in those with cuff tear arthropathy.
SSN ablation, either via percutaneous radiofrequency or
arthroscopic means, offers a minimally invasive option for pain
management. Additionally, a SSN ablation does not preclude
subsequent reverse geometry shoulder arthroplasty.
Partial rotator cuff repair
The rationale for partial rotator cuff repair when dealing with
massive IRCTs relates to the observation that small rotator cuff
tears rarely result in decompensation of shoulder function, and
that the restoration of the force couples, particularly the antero-
posterior couple, results in a shoulder that is biomechanically
competent while it remains anatomically deficient. Burkhart3
introduced this concept; essentially a “functional” repair of the
posterior rotator cuff is performed, leaving the greater tuberosity
uncovered. A massive tear is thereby converted to a small or
moderate tear with an intact subscapularis and the repaired
infraspinatus providing the competent antero-posterior couple.
There have been a number of studies advocating the benefits
of a partial rotator cuff repair, with reports of improved func-
tional outcome scores.2,3,24,25 Additional benefits of partial repair
over simple debridement have also been shown,26 and Burkhart3
has even challenged the requirement for tendon transfer surgery
on account of the results that can be obtained with a partial
repair. These results appear to be maintained with good reported
outcome scores at a minimum 5 years follow-up.25
The ability to perform partial, or even complete, rotator cuff
repairs may be improved by adequate releases of sub-acromial
bursal adhesions and if necessary interval slide procedures that
facilitate mobilization of the tendon of the rotator cuff footprint.
The anterior interval slide releases the rotator interval and the
coraco-humeral ligament between the subscapularis and supra-
spinatus tendons.27 The posterior interval slide is a release
between the infra- and supra-spinatus up to, though not medial
to, the scapular spine.
Augmented rotator cuff repair
Augmented rotator cuff repairs, or biological bridging, aim to
convert or bridge a partial repair of a massive IRCT into
ORTHOPAEDICS AND TRAUMA 26:6 370
a “complete” repair. Augmentation aims to reinforce the
mechanical properties of a repair and to stimulate and enhance
the biological healing potential of the repair.
There has been significant interest in tissue engineering
techniques to provide scaffolds for tendon augmentation over
recent years and there have been numerous studies, using both
natural and synthetic materials, for the augmentation of massive
IRCTs in animal models. Currently, extracellular matrix derived
from dermis, small intestinal submucosa, fascia lata, and peri-
cardium are commercially available for rotator cuff repair.28
These biological scaffolds of protein-based extracellular
matrices are derived from human or animal connective tissue.
The scaffolds have a 3-dimensional microstructure that allows
cellular infiltration, attachment and proliferation; this induces
quick interaction with the host tissue and new tissue formation.29
Some common examples include GraftJacket�(Wright Medical),
TissueMend� (Stryker), Restore� (DePuy) and CuffPatch�
(Arthrotek). Synthetic materials have been used but biocompat-
ibility has been an issue, with relatively higher rates of infection
and chronic immune response reported.30 The use of animal or
human tissue carries a theoretical risk of disease transmission,
though this has not been reported.29
Wong et al31 published statistically significantly improved
outcome scores in 45 patients treated with arthroscopic
GraftJacket� augmentation of massive IRCTs, followed for
a minimum 2 years post-operatively. Bond et al32 also reported
good outcomes following GraftJacket� augmentation and MRI
scans showed full incorporation of the graft into the native tissue
in the majority of patients.32 Augmentation is an interesting
option for massive IRCTs, though longer term outcomes are
required.
Tendon transfer surgery
Tendon transfers around the shoulder were originally employed
for loss of motor function of the deltoid, rotator cuff and trape-
zius muscles following brachial plexus injuries, most commonly
obstetric brachial plexus injuries. However, in 1988, Gerber et al9
first published a report on the use of a latissimus dorsi transfer
(LDT) for postero-superior rotator cuff deficiency.
Tendon transfer surgery aims to restore function in cuff
deficiency and should be considered in younger, higher demand
patients with pain and functional loss. There are several reports
of the benefits of tendon transfer surgery in IRCTs.33e36 Lat-
issimus dorsi transfer, with or without teres major transfer, has
been shown to benefit patients with postero-superior cuff tears
and likewise pectoralis major transfer is advantageous to patients
with massive irreparable subscapularis tears.
There are a number of techniques published for LDT and
mini-open harvest of the tendon with arthroscopic re-attachment
is gaining popularity. Prerequisites for LDT include an intact
subscapularis tendon, a functioning deltoid, a mobile joint with
no evidence of arthrosis and compliance with the relatively
prolonged rehabilitation.
The results for LDT generally report around a 25% increase in
the functional scores following surgery. LDT does not however
appear to correct for loss of strength,37,38 though the functional
gains patients appear to make, particularly with respect to
improvement of external rotation, do improve patient satisfac-
tion. The major contributory factors to better post-operative
� 2012 Elsevier Ltd. All rights reserved.

MINI-SYMPOSIUM: LESS COMMON SHOULDER PROBLEMS
outcomes scores are improved pain and function rather than
strength. This should be discussed before surgery and patients
can be advised that any strength gain is likely to be modest at
best, but daily activities should subsequently be possible with
little or no pain.38
Pectoralis major transfer for massive irreparable sub-
scapularis tears has been reported with some success. Jost et al36
reported good overall results of 30 transfers of the entire pec-
toralis major tendon to the subscapularis footprint. They re-
ported 23 good or excellent results with reported improvement in
both the Subjective Shoulder Value and the Constant score (from
47 to 70 points). The results of transfer were significantly better
in the absence of a supraspinatus tear, suggesting that a massive
tear involving the superior cuff is a relative contraindication to
the procedure.36 Warner,39 in an attempt to improve the line of
pull of the transfer rerouted the sternal portion of the tendon
under the clavicular head and re-attached the tendon to the
greater tuberosity; all patients experienced improved pain and
stability, but only two patients had “good” improvement.39
Subcoracoid transfer was introduced by Resch et al.40 who
showed improved flexion, abduction and Constant scores
following a split pectoralis transfer under the coracobrachialis
avoiding the musculocutaneous nerve.40 The overall results are
not impressive and, where possible, release of the subscapularis
and early direct repair is recommended.
Reverse geometry arthroplasty (without arthrosis)
Figure 4 Reverse geometry total shoulder arthroplasty used to manage
a patient with intractible shoulder pain with an irreparable massive
rotator cuff tear.
Reverse geometry arthroplasty was developed for patients with
massive rotator cuff deficiency with or without the presence of
arthropathy (Figure 4). More recently, it has gained popularity and
the indications for its use appear to have broadened. The rationale
for reverse arthroplasty relies on medialization of the centre of
rotation of the joint, thereby placing the deltoid at a biomechanical
advantage by increasing its lever arm. This provides prosthetic
joint stability and increases the range of movement of the
shoulder; functional results can therefore be better.
Reverse shoulder replacement is controversial to many for the
treatment of cuff deficiency in the absence of arthrosis. However,
for patients who have failed the options outlined previously and
who have on-going symptoms of pain and pseudo-paralysis of
the affected arm, the options are limited. Shoulder hemi-
arthroplasty (as discussed later) does not offer significant resto-
ration of function but can be useful to moderate the pain asso-
ciated with cuff tear arthrosis. Reverse shoulder replacement
may however be a valid option.
Mulieri et al41 reported the outcomes of reverse arthroplasty
in 69 patients (72 shoulders) without evidence of arthrosis; some
patients had undergone prior surgery but not all. For all patients,
the average American Shoulder and Elbow Surgeons score
improved from 33.3 to 75.4 (p < 0.0001), the average visual
analogue score for pain improved from 6.3 to 1.9 (p < 0.0001),
and the average forward flexion improved from 53� to 134�
(p < 0.0001) at a mean 53 months post-operatively.41
Boileau et al42 have also reported encouraging results with
reverse arthroplasty following failed cuff surgery at a mean 50
months post-operatively. The best results were seen in patients
with pseudo-paralysis with an increase in active anterior eleva-
tion from 56� to 123�, and only 7% of patients were dissatisfied
with the results.
ORTHOPAEDICS AND TRAUMA 26:6 371
However, these encouraging results come at a price and the
complication rate associated with reverse shoulder replacement
is high. The two aforementioned studies reported complication
rates of 20% and 10% respectively, though if scapular notching
is considered a complication this was actually reported in 74% of
cases by Boileau.42 Throughout the literature complication rates
for reverse shoulders are significant, being quoted at rates of up
to 50%. The procedure is technically demanding and complica-
tions include infection, dislocation, scapular notching (though
the true significance of this is not fully understood), and acro-
mion fracture due to the higher forces exerted through the new
lever arm of the deltoid. Reverse shoulder replacement should be
used judiciously and be performed by experienced surgeons.
Operative management with arthrosis
In 1983, Neer43 coined the term “cuff tear arthropathy”: arthrosis
in the presence of a massive rotator cuff tear. As previously
stated, the humeral head migrates proximally due to cuff defi-
ciency under the influence of deltoid, made possible by the
altered kinematics of the shoulder. The humeral head comes to
articulate with the upper portion of the glenoid and the under
surface of the acromion, and the abnormally articulating surfaces
become eroded.
The presence of cuff tear arthropathy is a relative contrain-
dication to partial or augmented rotator cuff repairs, as pain will
� 2012 Elsevier Ltd. All rights reserved.

MINI-SYMPOSIUM: LESS COMMON SHOULDER PROBLEMS
prevail following surgery and outcomes will be poor. The oper-
ative management does include arthroscopic rotator cuff and
joint surface debridement (with or without limited sub-acromial
decompression and biceps tenotomy) and SSN ablation, as
described previously, but if symptoms dictate it, then shoulder
arthroplasty can be offered. Total shoulder replacement is con-
traindicated in cuff deficiency as the tendency for superior
migration of the head results in the “rocking horse” phenom-
enon, with eccentric loading of the glenoid component leading to
early loosing and failure of the glenoid. The options are therefore
a shoulder hemi-arthroplasty, with or without an extended head
for articulation with the acromion, or a reverse geometry
shoulder arthroplasty.
Hemiarthroplasty or cuff tear arthroplasty (CTA)
Stemmed shoulder hemi-arthroplasty or surface replacement
arthroplasty, with or without extended coverage (cuff tear
arthroplasty), have been performed for cuff tear arthropathy with
satisfactory reported clinical outcomes and the risk of glenoid
failure is negated by performing a hemi-arthroplasty alone.
Zuckerman et al44 reported that 87% of patients were satisfied
with their surgery after this procedure, though the average active
forward elevation only increased from 69� to 86�. Patients re-
ported improved pain scores and an improvement in their ability
to perform activities of daily living but, as with other studies,
limited range of shoulder motion was noted. In addition to rela-
tively poor gains in movement, instability of the prostheses in
cuff deficiency remains a concern. The Mayo clinic reported
antero-superior instability in seven of 30 patients treated with
hemi-arthroplasty; this was, however, in association with prior
sub-acromial decompression, and overall a success rate of only
67% at 5 years was documented.45 Goldberg et al46 reported
similar overall results of hemi-arthroplasty but noted that patients
with pre-operative forward elevation of greater than or equal to
90� benefitted the most and overall complication rates were low.
The results of hemi-arthroplasty also appear to deteriorate in the
medium to long term due to glenoid or acromial erosion.
Hemi-arthroplasty should be avoided in patients with
previous shoulder surgery, especially sub-acromial decompres-
sion or if antero-superior instability already exists. However,
hemi-arthroplasty remains a viable option for pain relief without
significant functional gains and may be appropriate for some
patients as a more straightforward procedure with fewer reported
complications than the more invasive reverse shoulder
arthroplasty.
Reverse geometry arthroplasty
The biomechanical rationale of reverse shoulder replacement has
been noted above. Its use in rotator cuff arthropathy has been
well documented and good results have been reported in terms of
functional gains, range of movement and pain relief. However,
despite these encouraging results, the complication rates are
relatively high and judicious use of reverse arthroplasty by
experienced surgeons is recommended.
Summary
The management of massive IRCTs, in the presence or absence of
arthrosis, can be challenging. There are many treatment options
available and management should be tailored to the individual
ORTHOPAEDICS AND TRAUMA 26:6 372
patient. The interventions that have the capability to provide the
best results are also those that are associated with the most
significant and frequent complications therefore shared decision
making with the patient is imperative. A
REFERENCES
1 Sharkey NA, Marder RA. The rotator cuff opposes superior translation
of the humeral head. Am J Sports Med 1995; 23: 270e5.
2 Burkhart SS. Arthroscopic treatment of massive rotator cuff tears:
clinical results and biomechanical rationale. Clin Orthop Relat Res
1991; 267: 45e56.
3 Burkhart SS, Nottage WM, Ogilvie-Harris DJ, et al. Partial repair of
irreparable rotator cuff tears. Arthroscopy 1994; 10: 363.
4 Bigliani LU, Ticker JB, Flatow EL, Soslowsky LJ, Mow VC. The rela-
tionship of acromial architecture to rotator cuff disease. Clin Sports
Med 1991; 10: 823e38.
5 Walch G, Boulahia A, Calderone S, Robinson AH. The ‘dropping’ and
‘hornblower’s’ signs in evaluation of rotator-cuff tears. J Bone Joint
Surg Br 1998; 80: 624e8.
6 Hamada K, Fukuda H, Mikasa M, Kobayashi Y. Roentgenographic
findings in massive rotator cuff tears. A long-term observation. Clin
Orthop Relat Res 1990; 254: 92e6.
7 Cofield RH. Rotator cuff disease of the shoulder. J Bone Joint Surg Am
1985; 67: 974e9.
8 Rockwood Jr CA, Williams Jr GR, Burkhead Jr WZ. D�ebridement of
degenerative irreparable lesions of the rotator cuff. J Bone Joint Surg
Am 1995; 77: 857e66.
9 Gerber C, Vinh TS, Hertel R, et al. Latissimus dorsi transfer for the
treatment of massive tears of the rotator cuff. A preliminary report.
Clin Orthop 1988; 232: 51e61.
10 Gerber C. Latissimus dorsi transfer for the treatment of irreparable
tears of the rotator cuff. Clin Orthop Relat Res 1992; 275: 152e60.
11 Ainsworth R. Physiotherapy rehabilitation in patients with massive,
irreparable rotator cuff tears. Musculoskeletal Care 2006; 4: 140e51.
12 Zingg PO, Jost B, Sukthankar A, Buhler M, Pfirrmann CW, Gerber C.
Clinical and structural outcomes of nonoperative management of
massive rotator cuff tears. J Bone Joint Surg Am 2007; 89: 1928e34.
13 Levy O, Mullett H, Roberts S, Copeland S. The role of anterior deltoid
reeducation in patients with massive irreparable degenerative rotator
cuff tears. J Shoulder Elbow Surg 2008; 17: 863e70.
14 Gartsman GM. Massive, irreparable tears of the rotator cuff. Results
of operative debridement and subacromial decompression. J Bone
Joint Surg Am 1997; 79: 715e21.
15 Klinger HM, Spahn G, Baums MH, Steckel H. Arthroscopic debride-
ment of irreparable massive rotator cuff tears - a comparison of
debridement alone and combined procedure with biceps tenotomy.
Acta Chir Belg 2005; 105: 297e301.
16 Walch G, Edwards TB, Boulahia A, Nove-Josserand L, Neyton L,
Szabo I. Arthroscopic tenotomy of the long head of the biceps in the
treatment of rotator cuff tears: clinical and radiographic results of
307 cases. J Shoulder Elbow Surg 2005; 14: 238e46.
17 Liem D, Lengers N, Dedy N, Poetzl W, Steinbeck J, Marquardt B.
Arthroscopic debridement of massive irreparable rotator cuff tears.
Arthroscopy 2008; 24: 743e8.
18 Kelly AM, Drakos MC, Fealy S, Taylor SA, O’Brien SJ. Arthroscopic
release of the long head of the biceps tendon: functional outcome
and clinical results. Am J Sports Med 2005; 33: 208e13.
� 2012 Elsevier Ltd. All rights reserved.
MINI-SYMPOSIUM: LESS COMMON SHOULDER PROBLEMS
19 Zvijac JE, Levy HJ, Lemak LJ. Arthroscopic subacromial decompression
in the treatment of full thickness rotator cuff tears: a 3- to 6-year
follow-up. Arthroscopy 1994; 10: 518e23.
20 Scheibel M, Lichtenberg S, Habermeyer P. Reversed arthroscopic
subacromial decompression for massive rotator cuff tears. J Shoulder
Elbow Surg 2004; 13: 272e8.
21 Aszmann O, Dellon AL, Birely BT, McFarland EG. Innervation of the
human shoulder joint and its implications for surgery. Clin Orthop
Relat Res 1996; 330: 202e7.
22 Kane TP, Rogers P, Hazelgrove J, Wimsey S, Harper GD. Pulsed radi-
ofrequency applied to the suprascapular nerve in painful cuff tear
arthropathy. J Shoulder Elbow Surg 2008; 17: 436e40.
23 Nizlan NM, Skirving AP, Campbell PT. Arthroscopic suprascapular
neurectomy for the management of severe shoulder pain. J Shoulder
Elbow Surg 2009; 18: 245e50.
24 Duralde XA, Bair B. Massive rotator cuff tears: the result of partial
rotator cuff repair. J Shoulder Elbow Surg 2005; 14: 121e7.
25 Porcellini G, Castagna A, Cesari E, Merolla G, Pellegrini A, Paladini P.
Partial repair of irreparable supraspinatus tendon tears: clinical and
radiographic evaluations at long-term follow-up. J Shoulder Elbow
Surg 2011; 20: 1170e7.
26 Berth A, Neumann W, Awiszus F, Pap G. Massive rotator cuff tears:
functional outcome after debridement or arthroscopic partial repair.
J Orthop Traumatol 2010; 11: 13e20.
27 Tauro JC. Arthroscopic “interval slide” in the repair of large rotator
cuff tears. Arthroscopy 1999; 15: 527e30.
28 Aurora A, McCarron J, Iannotti JP, Derwin K. Commercially available
extracellular matrix materials for rotator cuff repairs: state of the art
and future trends. J Shoulder Elbow Surg 2007; 16: S171e8.
29 Longo UG, Lamberti A, Maffulli N, Denaro V. Tendon augmentation
grafts: a systematic review. Br Med Bull 2010; 94: 165e88.
30 Chen J, Xu J, Wang A, Zheng M. Scaffolds for tendon and ligament
repair: review of the efficacy of commercial products. Expert Rev Med
Devices 2009; 6: 61e73.
31 Wong I, Burns J, Snyder S, et al. Arthroscopic GraftJacket repair of
rotator cuff tears. J Shoulder Elbow Surg 2010; 19: 104e9.
32 Arthroscopic replacement of massive, irreparable rotator cuff tears
using a GraftJacket allograft: technique and preliminary results.
Arthroscopy 2008; 24: 403e9. e1.
ORTHOPAEDICS AND TRAUMA 26:6 373
33 Gerber C, Maquiera G, Espinosa N. Latissimus dorsi transfer for the
treatment of irreparable rotator cuff tears. J Bone Joint Surg 2006;
88: 113e20.
34 Valenti P, Kalouche I, Diaz LC, Kaouar A, Kilinc A. Results of latissimus
dorsi tendon transfer in primary or salvage reconstruction of irrepa-
rable rotator cuff tears. Orthop Traumatol Surg Res 2010; 96: 133e8.
35 Moursy M, Forstner R, Koller H, Resch H, Tauber M. Latissimus dorsi
tendon transfer for irreparable rotator cuff tears: a modified tech-
nique to improve tendon transfer integrity. J Bone Joint Surg Am
2009; 91: 1924e31.
36 Jost B, Puskas GJ, Lustenberger A, et al. Outcome of pectoralis major
transfer for the treatment of irreparable subscapularis tears. J Bone
Joint Surg Am 2003; 85: 1944e51.
37 Nov�e-Josserand L, Costa P, Liotard JP, Safar JF, Walch G, Zilber S.
Results of latissimus dorsi tendon transfer for irreparable cuff tears.
Orthop Traumatol Surg Res 2009; 95: 108e13.
38 Weening AA, Willems WJ. Latissimus dorsi transfer for treatment of
irreparable rotator cuff tears. Int Orthop 2010; 34: 1239e44.
39 Warner JJ. Management of massive irreparable cuff tears: the role of
tendon transfer. Instr Course Lect 2001; 50: 63e71.
40 Resch H, Povacz P, Ritter E, et al. Transfer of the pectoralis major
muscle for the treatment of irreparable rupture of the subscapularis
tendon. J Bone Joint Surg Am 2000; 82: 372e82.
41 Mulieri P, Dunning P, Klein S, Pupello D, Frankle M. Reverse shoulder
arthroplasty for the treatment of irreparable rotator cuff tear without
glenohumeral arthritis. J Bone Joint Surg Am 2010; 92: 2544e56.
42 Boileau P, Gonzalez JF, Chuinard C, Bicknell R, Walch G. Reverse total
shoulder arthroplasty after failed rotator cuff surgery. J Shoulder
Elbow Surg 2009; 18: 600e6.
43 Neer 2nd CS, Craig EV, Fukuda H. Cuff-tear arthropathy. J Bone Joint
Surg Am 1983; 65: 1232e44.
44 Zuckerman JD, Scott AJ, Gallagher MA. Hemiarthroplasty for cuff tear
arthropathy. J Shoulder Elbow Surg 2000; 9: 169e72.
45 Sanchez-Sotelo J, Cofield RH, Rowland CM. Shoulder hemi-
arthroplasty for glenohumeral arthritis associated with severe rotator
cuff deficiency. J Bone Joint Surg Am 2001; 83: 1814e22.
46 Goldberg SS, Bell JE, Kim HJ, Bak SF, Levine WN, Bagliani LU. Hemi-
arthroplasty for the rotator cuff-deficient shoulder. J Bone Joint Surg
Am 2008; 90: 554e9.
� 2012 Elsevier Ltd. All rights reserved.


![Shoulder Arthroplasty Americas 2014 [Read-Only]memorialhermann.org/uploadedfiles/_library_files/ironman/management...Irreparable rotator cuff tear is a contraindication to glenoid](https://img.pdfslide.net/doc/110x75/5afc1a527f8b9a32348fdecb/shoulder-arthroplasty-americas-2014-read-only-rotator-cuff-tear-is-a-contraindication.jpg)