Embed Size (px)
Citation preview
ICD-10- CMTHE TRANSITION FROM ICD9
June 2014| Nina Campus
WHY THE CHANGE?
• ICD9-CM is 30 years old• Many of the categories are full• Codes are not descriptive enough• Technology has changed
2
WHEN WILL IT HAPPEN?• ICD9-CM codes will not be accepted for
services provided on or after 10/1/2015.• Claims that do not use ICD10 diagnosis
after 10/1/2015 cannot be processed. • Use ICD9
– Worker’s Compensation & Auto Insurance not required.
• This applies to resubmission or appealed claims.
3
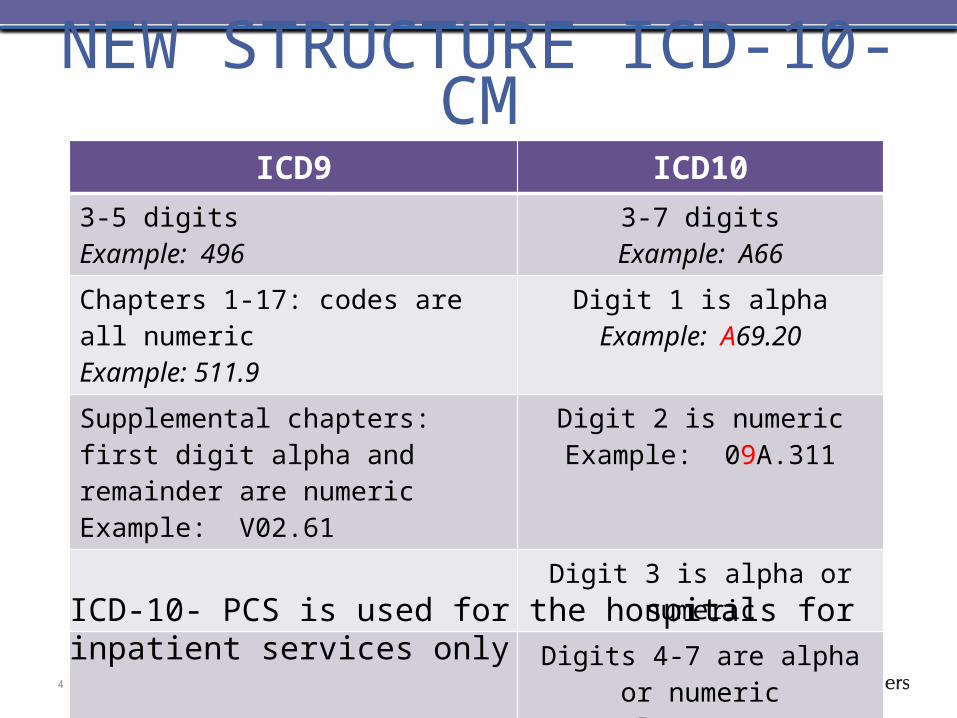
NEW STRUCTURE ICD-10- CMICD9 ICD10
3-5 digitsExample: 496
3-7 digitsExample: A66
Chapters 1-17: codes are all numericExample: 511.9
Digit 1 is alphaExample: A69.20
Supplemental chapters: first digit alpha and remainder are numericExample: V02.61
Digit 2 is numericExample: 09A.311
Digit 3 is alpha or numericDigits 4-7 are alpha or numeric
Example: S42.001A
4
ICD-10- PCS is used for the hospitals for inpatient services only
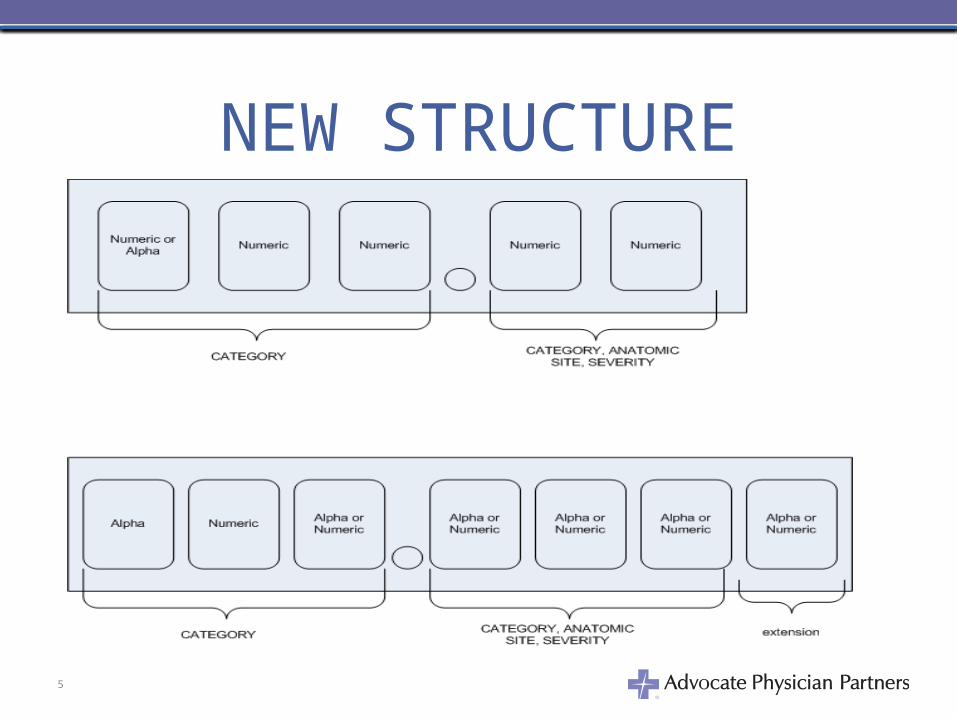
NEW STRUCTURE
5
ICD-10 CHAPTERS• ICD-9-CM has 17 chapters and ICD-10 CM
has 21 chapters– Chapter 18 which are V codes (Classification of Factors
Influencing Health Status and Contact with Health Service)
• Chapter 20 in ICD-10-CM
– Chapter 19 which are E codes (Supplemental Classification of External Causes of Injury and Poisoning
• Chapter 21 in ICD-10-CM
– Eye and ear have their own chapter in ICD-10• Chapter 7 & 8
6
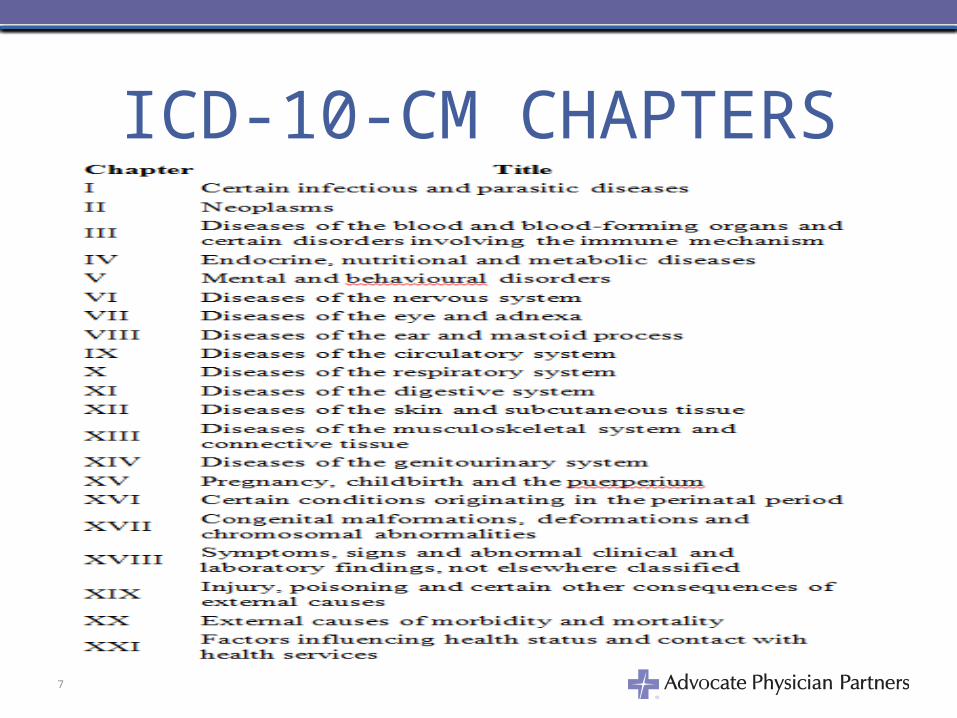
ICD-10-CM CHAPTERS
7
ICD-10-CM CHAPTER CATEGORIES
• Chapters are divided in three alphanumeric character categories.– also called Rubric
• There are no alphanumeric character category that start with letter U.– Use of letter I– Use of letter O
8
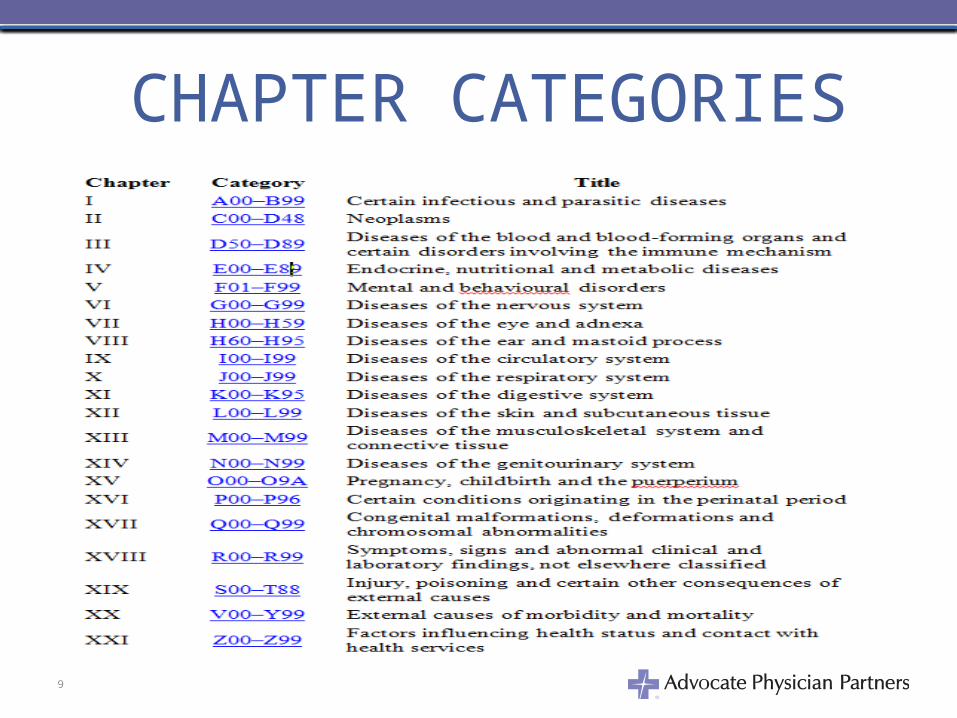
CHAPTER CATEGORIES
9
ALPHABETIC INDEXVolume II
• Arranged in alphabetic order by diseases• Divided into sections and organized by main
terms– Index of Diseases and Injury– Index of External Causes of Injury– Table of Neoplasm– Table of Drugs and Chemicals
• Elimination of Hypertension Table– No more benign or malignant
10
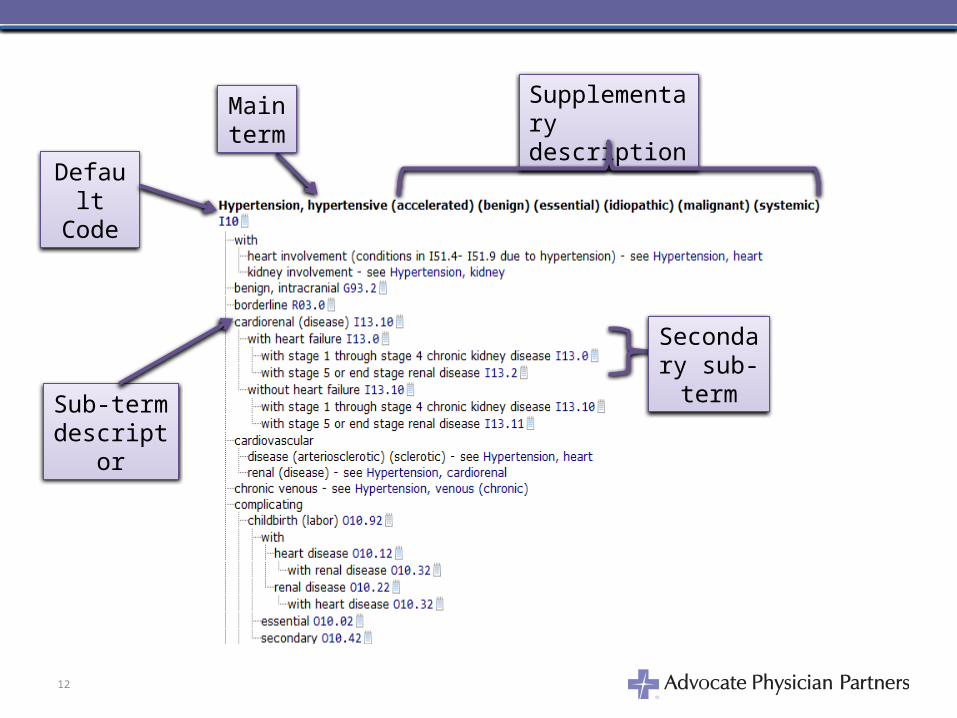
ALPHABETIC INDEX• Main terms describe the disease and/or
condition– Cross reference “see” “see also”
• Sub-terms are under the main term following an indented format.
• Supplemental (nonessential) descriptions are found in parentheses after the main term.
11
12
Supplementary description
Main term
Sub-term descriptor
Default Code
Secondary sub-term
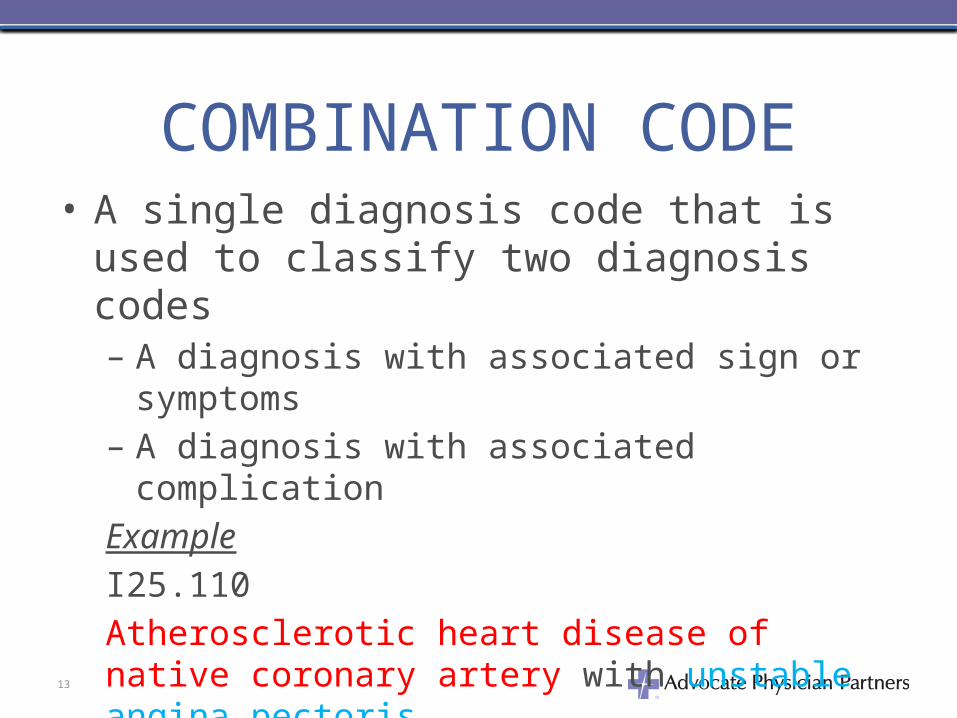
COMBINATION CODE• A single diagnosis code that is used to
classify two diagnosis codes– A diagnosis with associated sign or symptoms – A diagnosis with associated complication
Example
I25.110
Atherosclerotic heart disease of native coronary artery with unstable angina pectoris.
13
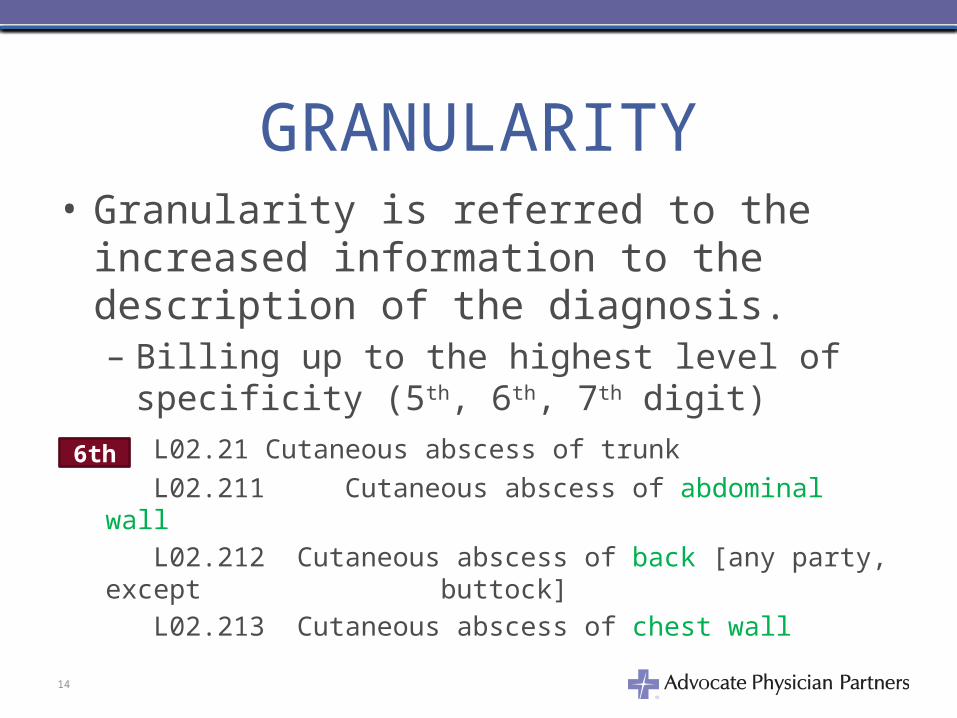
GRANULARITY• Granularity is referred to the increased
information to the description of the diagnosis. – Billing up to the highest level of specificity (5th, 6th,
7th digit)
L02.21 Cutaneous abscess of trunk
L02.211 Cutaneous abscess of abdominal wall
L02.212 Cutaneous abscess of back [any party, except buttock]
L02.213 Cutaneous abscess of chest wall
14
6th
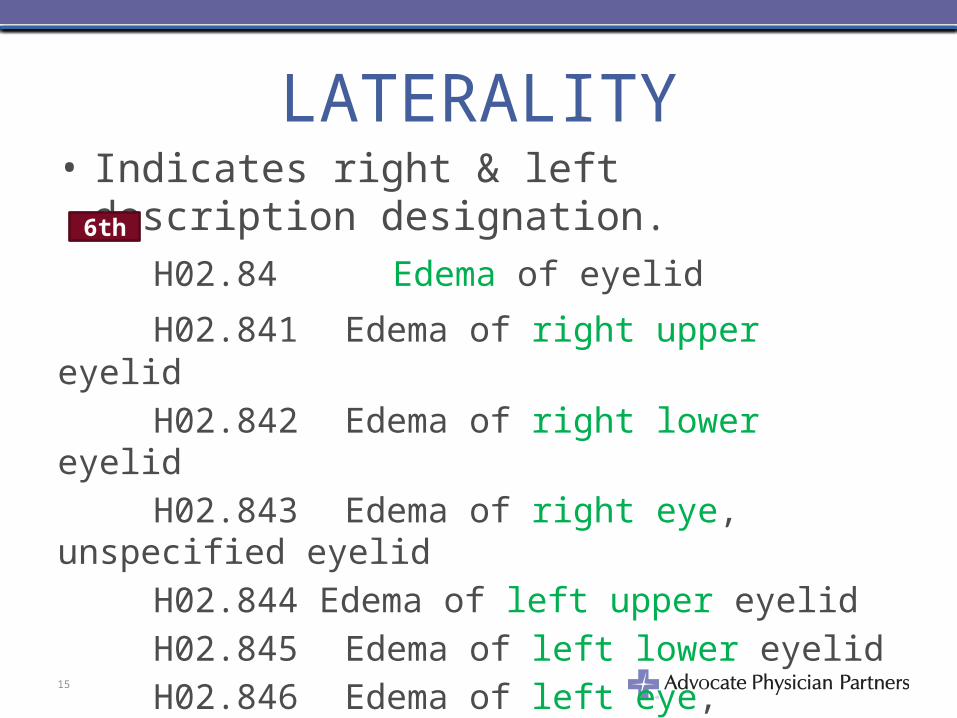
LATERALITY• Indicates right & left description designation.
H02.84 Edema of eyelid
H02.841 Edema of right upper eyelid
H02.842 Edema of right lower eyelid
H02.843 Edema of right eye, unspecified eyelid
H02.844 Edema of left upper eyelid
H02.845 Edema of left lower eyelid
H02.846 Edema of left eye, unspecified eyelid
H02.849 Edema of unspecified eye, unspecified eyelid15
6th
LATERALITY• Right side is usually character 1
– H04.1111 Dacryops of right lacrimal gland
• Left side is usually character 2– H04.1112 Dacryops of left lacrimal gland
• Bilateral is usually character 3– H04.113 Dacryops of bilateral lacrimal glands
• Unspecified side is usually character 0 or 9– H04.129 Dry eye syndrome of unspecified
lacrimal gland
16
TABULAR INDEXVolume I
• CATEGORY– Three-digit character code that represents a single
condition or disease
Example
Chapter 1 A00-B99 Certain Infectious and Parasitic Diseases
A00-A09 Intestinal infectious disease
A15-A19 Tuberculosis
A20-A28 Certain zoonotic bacterial disease
A30-A49 Other bacterial diseases
17
TABULAR INDEX• SUBCATEGORY
– Four-digit character code that provides a higher level of specificity compared category. It defines site, etiology and manifestation of the disease or condition.
Example
C15 Malignant neoplasm of the esophagus
C15.3 Malignant neoplasm of upper third of esophagus
18
TABULAR INDEX• SUBCLASSIFICATION
– A five-digit or sixth character code that adds precise specificity.
Example
J10.82 Influenza due to other identified influenza virus with myocarditis
M88.861 Other juvenile arthritis, right knee
19
TABULAR INDEX• The seventh-digit character code extension is
required if applicable as defined by the tabular index.– Mostly used in injuries and fractures
Example
T65.211A Toxic effect of chewing tobacco, accidental (unintentional), initial encounter
20
TABULAR INDEX• Dummy Placeholder
– Used as a placeholder to allow for future expansion or if you code created for that character.
– When a fifth character code is not created but required to code to the sixth and seventh digit.
Example
T37.5X1 Poisoning by antiviral drugs, accidental
(unintentional)
21
CONVENTIONS• Code first/use additional code notes
– Etiology/manifestation paired codes have a specific index structure.
– Signals that additional codes should be reported to provide a more complete picture of the patient’s diagnosis.
– Etiology code is first followed by the manifestation codes.
22
CODE FIRST/USE ADDITIONAL CODE NOTES
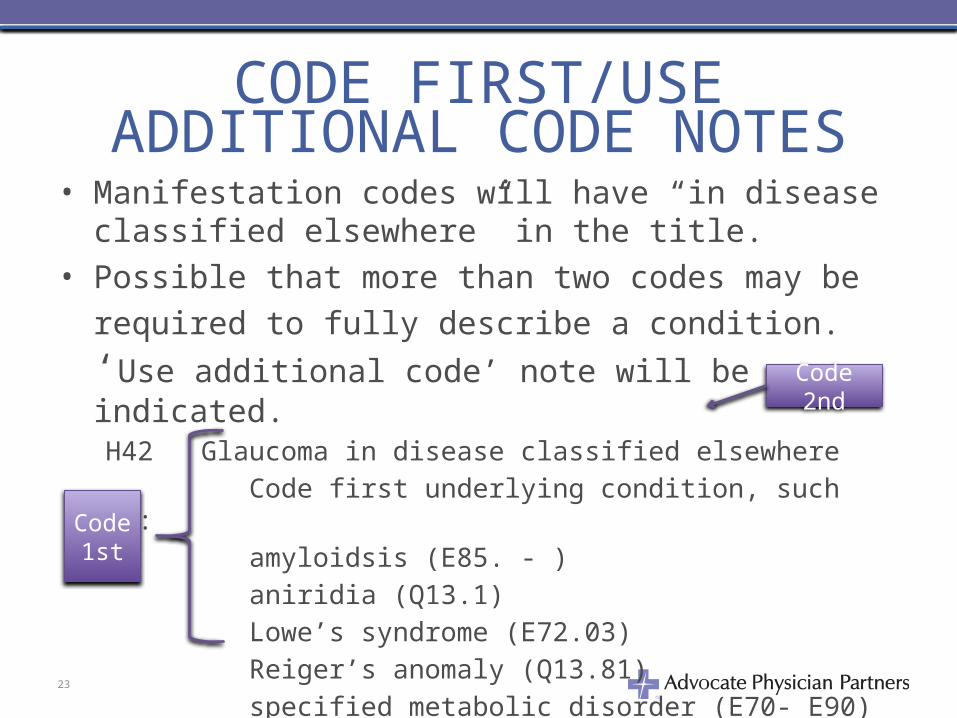
• Manifestation codes will have “in disease classified elsewhere” in the title.
• Possible that more than two codes may be required to
fully describe a condition. ‘Use additional code’ note will be indicated.H42 Glaucoma in disease classified elsewhere
Code first underlying condition, such as:
amyloidsis (E85. - )
aniridia (Q13.1)
Lowe’s syndrome (E72.03)
Reiger’s anomaly (Q13.81)
specified metabolic disorder (E70- E90)
23
Code 1st
Code 2nd
CODE FIRST• ‘Code first’ note and an underlying condition is
present, the underlying condition should be sequenced first.
• ‘Code, if applicable, any causal condition first,’ notes indicates that this code may be assigned as a principal diagnosis when the causal condition is unknown or not applicable.
• If the causal condition is know, then the code for the condition should be sequenced as principal or first-listed diagnosis.
24
CONVENTION – ‘NEC’ ‘NOS’
• NEC directed to an ‘other specified’ code in the Tabular List. Reference the inclusion term under the subheading.– No codes defined for the documentation
• NOS is the equivalent of unspecified.– More codes defined that was is documented.
25
PUNCTUATION[ ]- used in tabular list to enclose synonyms, alternative wording or explanatory wording. Brackets are used to identify manifestation codes.
( )- used in the alphabetic index and tabular list and referred to as supplementary descriptions (nonessential modifiers)
:- Used after an incomplete term that needs one or more supplementary descriptions.
26
PUNCTUATION• } – series of terms which is modified by the
statement appearing at the right of the brace.• , - words that are essential descriptors. The
terms in the inclusion note must be present in the diagnostic statement to assign for this code.
Example
C50.31 Malignant neoplasm of lower-inner quadrant of breast, female27
‘CODE ALSO’, ‘SEE’, ‘SEE ALSO’• Code Also – instructs that two codes may be
required to fully describe a condition.– Sequencing of the two codes depends on the severity
of the condition and the reason for the encounter.
• See- instructions following a main term indicates another term should be referenced.
• See Also – instructions following a main term that another main term may also be referenced.Amentia – see also Disability, intellectual
28
DEFAULT CODES• A code next to the main term• Most commonly associated with the main
term• Unspecified code for the condition• If condition documented in medical record
does not provide the additional information, the default code should be assigned.
K37 Appendicitis - not indicated as chronic
or acute29
EXCLUDES NOTES• Two types of EXCLUDES NOTES
– Type I Excludes notes indicates the codes should never be used at the same time as the above the Excludes1 note.
• Two conditions cannot occur together and are mutually exclusive.
• A Type I Excludes note means NOT CODED HERE!Example
E11 Type 2 diabetes
Excludes1: gestational diabetes (Q24.4 -)
Type 1 diabetes (E10. - )
30
EXCLUDES NOTES• Type II Excludes note represents ‘Not included
here’. The condition excluded is not part of the condition represented by the code.– It is acceptable to use both the code and the excluded
code together. Example
I10 Essential (primary) Hypertension Includes:
high blood pressure hypertension (arterial) (benign) (essential) (malignant) (primary) (systemic)
Excludes2: essential (primary) hypertension involving vessels of brain (I60-I69)
essential (primary) hypertension involving vessels of eye (H35.0)
31
INCLUSION TERM• List of codes included under some codes.
Additional terms found only in the index may also be assigned to a code.
ExampleChapter 1 Certain Infectious and Parasitic DiseasesUse additional code to identify resistance to antimicrobial drugs (Z16.-)
Excludes2: carrier or suspected carrier of infectious disease (Z22.-)
B95-B97 Bacterial and viral infectious agents
32
USE OF ‘AND’, WITH/WITHOUT• When the term ‘and’ is used in a narrative
statement, it represents and/or. • When ‘with’ and ‘without’ are the two options
for the final character of a set of codes, the default is always ‘without’.– For five character codes, the 0 (zero) represents
‘without’ and 1 represents ‘with’. – For six character codes, the 1 represents ‘with’
and 9 represents ‘without’
33
GENERAL CODING GUIDELINES• There are general coding guidelines outlined
in each chapter of the ICD-10-CM.• To find a code, first locate the term in the
alphabetic index and then verify code in the tabular list.
• Diagnosis codes are to be used and reported at their highest number of characters available.
34
GENERAL CODING GUIDELINES• Three character code is only used if it is not
further subdivided. • The appropriate codes from A00.0 – T88.9,
Z00-Z99.8 must be used to identify diagnoses, symptoms, conditions, problems, complaints, or other reasons for the encounter/visit.
35
GENERAL CODING GUIDELINES• Codes that describe symptoms and signs, as
opposed to diagnoses, are acceptable for reporting purposes when the relating definitive diagnosis has not be established by the provider. (Reference Chapter 18 of the ICD-10 CM book.)
Abnormal Liver Function Test would be coded R94.5
36
GENERAL CODING GUIDELINES– Signs or symptoms should not be reported with a
confirmed diagnosis if the symptom is integral to the diagnosis.
Patient is experiencing ear pain and the diagnosis is otitis media. the ear pan would be integral to the otitis media and
would not be reported.
– Symptom code is used with a confirmed diagnosis only when the symptom is not associated with the confirmed diagnosis.
A patient is diagnosed with epigastric pan and referred the patient to a gastroenterologist to rule out ulcer.
ICD9-CM 789.06 Abdominal pan, epigastric
ICD10- CM R10.13 Epigastric pain37
GENERAL CODING GUIDELINES• Signs and symptoms that are associated
routinely with a disease process should not be assigned as additional codes, unless otherwise instructed by the classifications.
• Additional signs and symptoms that may not be associated routinely with a disease process should be coded when present.
38
GENERAL CODING GUIDELINES• A physician diagnosed a patient with rheumatoid arthritis
of the right ankle and foot who also has rheumatoid polyneuropathy. The condition is coded in ICD-10-CM using the combination code.
ICD-9-CM 714.0 Rheumatoid arthritis
357.1 Polyneuropathy in collagen vascular disease
In ICD9, we do not have a combination code to fully describe the condition and must use two codes when reporting this diagnosis.
ICD-10-CM a combination code is available:
M05.571 Rheumatoid polyneuropathy with rheumatoid arthritis of right ankle and foot39
GENERAL CODING GUIDELINESAcute and Chronic Conditions• If the same condition is described as both
acute (sub-acute) and chronic, and separate subentries exist in the Alphabetic Index at the same indentation level, code both and sequence the acute (sub-acute) code first.
Patient was diagnosed with acute maxillary sinusitis that is chronic report ICD-10 CM codes J01 (Acute sinusitis) and J32.0 (Chronic maxillary sinusitis)
40
GENERAL CODING GUIDELINES• Late Effects (Sequela)• Sequela is a condition produced after the
acute phase of an illness or injury has terminated.
• Not time limit on when sequela can be used.• Coding sequela generally requires two codes
sequenced as follows:– Condition or nature of the sequela is first– Sequela is sequenced second
41
Principal Diagnosis Code• Reported in medical record as the primary
reason or the determination at the end of the encounter.
• Providers should only be reporting the diagnosis codes for the conditions they treated in the encounter.
• Not all diagnosis codes can be listed as the primary diagnosis code for an encounter.– Reference ICD-10-CM Draft Official Guidelines for Coding and
Reporting 2014
42
Guidelines for Principal DX• Sign or symptom is not used when a definitive
diagnosis for the sign/symptom has been established.
• If anticipated treatment is not carried out due to unforeseen circumstances, the principal code remains the diagnosis that the provider planned to treat.
• When the admission is for treatment of a complication resulting from surgery or other medical care, the complication code is sequenced as the principal diagnosis/first-listed code.
43
Secondary Diagnosis Code• Although a patient has an encounter for the principal
diagnosis, the additional conditions or reasons for the encounter also need to be coded.
• Other diagnosis codes are additional codes that affects patient care in terms of requiring clinical evaluation or therapeutic treatment or diagnostic procedure or extended length of hospital stay or increase nursing care and/or monitoring.
• Diagnoses that relate to an earlier episode that have no bearing on the current hospital stay are to be excluded.
44
Abnormal Test Findings• Laboratory, x-ray, pathologic and other
diagnostic results are not coded or reported unless the physician indicates their clinical significance.
• If the findings are outside the normal range and the physician has ordered other tests to evaluate the condition or prescribe treatment, it is appropriate to ask the physician whether the abnormal finding should be added.
45
Abnormal Test Findings• If the abnormal finding corresponds to a
confirmed diagnosis, it should be coded in addition to the confirmed diagnosis.
• If the diagnosis is confirmed (eg, an X-ray, pathology or laboratory report confirms DX), prior to coding the encounter, the confirmed DX code should be used.
46
RESOURCES• CMS ICD10 Website
– www.cms.gov/Medicare/Coding/ICD10
• ICD-10-CM Draft Official Guidelines for Coding and Reporting 2014– http://www.cdc.gov/nchs/data/icd/icd10cm_guidelines_2014.pdf
• Center for Disease Control (CDC)– http://www.cdc.gov/nchs/icd/icd10cm.htm
• World Health Organization (WHO)– http://www.who.int/classifications/icd/en/
• AAPC Website– http://www.aapc.com/icd-10
47