Embed Size (px)
Citation preview

ICD-9-CM ICD-10-CM
Implementing ICD-10-CM
Preparing for the Conversion
Long Term and Post Acute Care Practice Council
1

BackgroundICD-9-CM
Current coding classification system Introduced 30 years ago No longer fits with 21st century health system
ICD-10-CM International standard Track, report & compare morbidity & mortality Transition to ICD-10 required by federal
regulations (HIPAA standards)
2

BackgroundICD-10
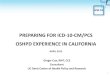
Available since 1992 Approximately 100 countries use ICD-10
including Canada, Australia, and the United Kingdom
United States: Only industrialized nation not using ICD-10
United States: ICD-10 go-live date was October 1, 2013 NOW revised to be implemented October 1, 2014 3

Global Use of ICD-10
4

The WHO - What – Why ???
ICD-9-CM Overview
• ICD-9 Developed by the WHO
(World Health Organization)
• 1979 U.S. developed the Clinical Modification to ICD-9-CM
• 2000 HIPAA transaction and code set:
ICD-9 -CM for electronic transactions
Now updated for ICD-10-CM
5

Where - How – When ???
• ICD-10-CM All health care settings as well as other industries which utilize the ICD system, e.g. Insurance Providers
ICD-10-PCS for inpatient hospital)• A single implementation date for all providers
• Current Implementation Date: October 1, 2014
6

Code Freeze
• Last regular, annual updates to both ICD-9 and ICD-10 was Oct. 1, 2011
• Oct. 1, 2012 - 2013 there will be only limited code updates to both code sets
• Oct. 1, 2014 there will be only limited updates to ICD 10 code set• Limited updates will capture new technology
or new diseases only
• Oct. 1, 2015 regular annual updates to ICD-10 will begin, ending the freeze 7

ICD-10-CM Significant improvement
for reporting clinical data
• Measuring the quality, safety, and efficacy of care
• Conducting clinical trials, epidemiological studies, research
• Setting health policy• Tracking public health and risks
8

ICD-10-CMSignificant Improvements
• Strategic planning and designing healthcare delivery systems
• Monitoring resource utilization• Improving clinical, financial, and administrative performance
• Detecting and preventing healthcare fraud and abuse 9

ICD-10-CMSignificant Improvements
• Fewer miscoded, rejected & improperly reimbursed claims
• Improved disease management• Increased Specificity• Data comparability internationally
10

What remains the same?
• Use of code books or encoder • Tabular List Chapters similar to
ICD-9-CM with some exceptions• Main Term, indented sub term• Alphabetic Index of External Causes• Table of Neoplasms• Table of Drugs and Chemicals
11

What remains the same?
• Conventions – abbreviations, punctuation, symbols, code first, use additional code, includes, excludes
• Code to highest level of specificity• Adherence to HIPAA and official guidelines (ICD-10-CM)
• Nonspecific codes still available 12

What remains the same?
Inconsistent, missing, conflicting, documentation must still be resolved by the Provider—both today under ICD-9-CM, as well as in the
future with ICD-10-CM 13

• The goal is always to work toward better documentation for the following reasons:• Avoid misinterpretation by third parties (such
as auditors, payers, attorneys)• Justify medical necessity• Provide a more accurate clinical picture of the
quality of care provided• Support current & future initiatives aimed at
improving quality and reducing costs, such as value-based purchasing
Coding and Documentation
14

ICD-10-CM Differences
• Increase codes: 14,000 to 68,000 • Flexible – Incorporate emerging diagnoses, advances in medicine and medical technology
• Uses current medical terminology• Codes are Alphanumeric
• all codes begin with a letter
• Uses all letters of the alphabet except the letter U
15

ICD-10-CM Differences
• Expanded length 3-7 characters vs. 3-5• Increased precision in diagnosis code• Full diagnostic titles for each code• Added Laterality (right/left, bilateral)• Code extensions for injuries and
external causes of injuries• Combination codes for etiology &
manifestations• Episode of Care designation
16

ICD-10 Differences
EXCLUDE NOTES• Excludes 1: not coded here
• The 2 conditions contradict each other• Acquired condition vs. congenital• Codes cannot be reported together
• Excludes 2: not included here• The condition excluded is not a part of the
condition represented by the code• Both codes can be reported together
17

ICD-10 Difference
• Acute MI – Time Frame Change
ICD – 9 8 weeks or less
ICD – 10 4 weeks or less• Hemiplegia / Monoplegia
Dominant vs. Nondominant• Example:
• G81.91 Hemiplegia, unspecified affecting right dominant side
18

Difference & Similarities
• Hypertension Table eliminated
• Only 1 hypertension code in ICD-10
• Same rules apply in ICD-10 as in ICD-9 for combining Hypertension codes with heart disease and chronic kidney disease.
19

HypertensionICD-9-CM
• 401.0 Essential Hypertension, Malignant
• 401.1 Essential Hypertension Benign
• 401.9 Essential Hypertension Unspecified
ICD-10-CM
• I10 Essential
Primary
Hypertension
20

Asthma with Acute ExacerbationICD-9-CM
• 493.92 – Asthma, unspecified with acute exacerbation
ICD-10-CM
•J45.21 - Mild intermittent asthma with acute
exacerbation•J45.31 - Mild persistent asthma with acute exacerbation•J45.41 - Moderate persistent asthma with acute exacerbation•J45.51 - Severe persistent
asthma with acute exacerbation
21

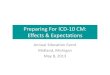
ICD-10-CM Code Format
X X X X X X X
Category
.
Etiology, anatomic site, severity
Extension 22

ICD-10 Placeholder “X”
• Addition of dummy placeholder “X” is used in certain codes to:• Allow for future expansion• Fill out empty characters when a code
contains fewer than 6 characters and a 7th character is required
• When placeholder character applies, it must be used in order for the code to be considered valid
• Example: S32.9XXD Fx Pelvis d/t fall, routine healing, subsequent episode of care
23

SIGNIFICANT DIFFERENCE
Coding Fractures• No longer will we use Aftercare codes for healing fractures• V54.13 Aftercare for healing traumatic
fracture of hip
• Will use the acute fracture code followed by an appropriate 7th character extension to indicate subsequent episode of care
24

Closed Fracture 7th character extensions:
• A – Initial encounter for closed fracture hospital, ER, clinic
• D – Subsequent encounter for fracture routine healing
• G – Subsequent encounter for fracture delayed healing
• K – Subsequent encounter for fracture nonunion
• P – Subsequent encounter for fracture malunion
25

CODING GUIDELINES
26

Coding Guidelines
• A Fracture not indicated as displaced or nondisplaced should be coded to displaced.
• A fracture not indicated whether open or closed should be coded to closed
27

Coding Guidelines
Initial vs. subsequent encounter for fractures:
• Initial care involves active treatment• Subsequent care occurs after active
treatment and receiving routine care during the healing or recovery phase
• Sequela – complications or conditions that arise as a direct result of an injury
(previously called ‘late effect’)28

ICD 10 Structure
FRACTURES• S72 Fracture Femur• S72.1 Pertrochanteric fx femur• S72.14 Intertrochanteric fx femur• S72.141 Displaced Intertrochanteric
fracture of right femur• S72.141D Displaced Intertrochanteric Fx
of right femur, subsequent encounter for closed fx with
routine healing29

Closed fracture of the greater trochanter of the right femur (hip fracture)
• S72.111A - Initial encounter for closed fracture: Patient admitted for initial treatment in ER and hospital with resulting surgical repair
• S72.111D - Subsequent encounter for closed fracture with routine healing: Admission to long-term care (LTC) for rehabilitation after hip replacement
30

Examples: Subsequent Encounter
• S72.111D, Subsequent encounter for closed fracture with routine healing: Discharged from LTC Home Health for continued PT
• S72.111D, Subsequent encounter for closed fracture with routine healing: Patient visits hospital radiology department for X-ray
• S72.111D, Subsequent encounter for closed fracture with routine healing: Patient to physician office for follow-up visit 31

ICD-10-CM ‘Snapshot’
• Diabetes mellitus 59 to ~ 200+ • Pressure ulcer 9 to ~ 125• Path. fracture 8 to ~ 150• Under dosing NEW section
32

ICD-10-CM ‘Snapshot’
• Z43.1 Attention to gastrostomy• Z48.815 Aftercare following surgery
on digestive system (cholecystectomy)
• F03.90 Unspecified Dementia, w/o behavior
• L89.613 Pressure ulcer right heel, stage III
33

ICD-10-CM ‘Snapshot’
• E11.40 Type II DM with neuropathy
• Z79.4 Long Term use of insulin• J44.9 COPD• Z99.81 Oxygen dependent• Z79.52 Prednisone dependent
34

MI – Myocardial Infarction
• Time frame for coding acute myocardial infarctions changes with ICD-10• ICD-9 8 weeks• ICD-10 4 weeks
• As long as treatment is required, regardless of care setting
35

MI – Myocardial Infarction
• I21.4 Non-ST elevation (NSTEMI) myocardial infarction• Use acute code for 4 weeks regardless of treatment facility
• I25.2 Old myocardial infarction• After initial episode of 4 weeks, then use “healed / old MI” code
36

Residual Effects of Cerebrovascular Disease
ICD-10-CM
• Hemiplegia following nontraumatic subarachnoid hemorrhage
• Hemiplegia following nontramatic intracerebral hemorrhage
• Hemiplegia following other intracranial hemorrhage
37

Residual Effects of Cerebrovascular Disease
ICD-10-CM• Hemiplegia following cerebral infarction
• Hemiplegia following other cerebrovascular disease
• Hemiplegia following unspecified cerebrovascular disease
38

Hemiparesis following CVA
ICD-9-CM ICD-10-CM
438.21 Hemiplegia following CVA affecting dominant side
I69.051 Hemiplegia and hemiparesis following nontraumatic subarachnoid hemorrhage affecting right dominant side
I69.052 Hemiplegia and hemiparesis following nontraumatic subarachnoid hemorrhage affecting left dominant side 39

CVAs
• Terminology “Late Effects” is eliminated from ICD-10
• Sequela is the new term for Late Effects• Sequela of cerebral hemorrhage• Sequela of cerebral infarct• Sequela of cerebrovascular disease
40

CVAs
• I69.0 – I69.298 • Sequela of hemorrhages
• I69.3 – I69.398• Sequel of cerebral infarction
• Occlusion of artery• Default for “stroke”
• I69.8 – I69.998• Sequela of cerebrovascular disease 41

CVAs
• Coder will have to pay close attention to the type of CVA which occurred to obtain the correct code
• No more flipping to the 438 section and looking for your code! • Flipping to I69 will only confuse you
more!• Use alphabetic index to look up what
is documented in the record.42

ICD-10-CM Project Planning
•Resources:•Coding Manuals•Coding Instruction Resources•Training costs (Biomedical science & ICD-10)
43

ICD-10-CM Transition Budget $$$ Considerations
• Hardware/software system upgrade, maintenance fees
• Data Conversion• Clinical & financial
• Forms redesign & reprinting• Consultant Fees • Outsourcing 44

ICD-10-CM Transition Budget Considerations
• Temporary staff needed to assist during transition period
• Lost productivity during training & implementation phase
• Increased coding time
with ICD-1045

ICD-10 Project Planning
• Clearinghouses, outside billing service, health Insurance payers• When will upgrades be completed?• When can claims with ICD-10-CM
codes be transmitted for testing?• Re-negotiate provider contracts or
electronic data interchange agreements (EDI)
46

ICD-10-CM Project Planning• Who Assigns or Uses ICD-9-CM Codes:• Health Information Management (Medical Record Staff)
• Nursing, MDS Coordinators• Admissions• Billing • Therapy • Lab, X-ray
47

Early Preparation
• A well-planned, well-managed implementation process will increase the changes of a smooth, successful transition
• Experience in other countries has shown that early preparation is the key to success & earlier realization of benefits
• An early start allows for resource allocation, such as costs for systems changes and education, process evaluation and change, as well as staff time devoted to implementation processes to be spread over several years
48

Inadequate Preparation
Potential Consequences• Decreased coding accuracy• Decreased coding productivity• Increased compliance risks• Increased claims rejection• An adverse impact on patient care and
administrative decision-making• Decrease in key staff morale 49

Preparation – When to Start
.
Don’t Delay! Get Started Today!
50

51

Methods of Training
• Current in-house SNF on-line Education System
• Online self-study courses including AHIMA
• Webinars/WebEx
52

Methods of Training
• Videos on specific body systems• Seminars/workshops • Local Educational Institutions• ICD-10-CM Workbooks (self learn)
53

Methods of Training
• Local hospital educational
programs ICD-10-CM ONLY
NOT ICD-10-PCS)• Qualified HIM Professionals / HIM Consultants (e.g. AHIMA Approved)
54

Coder Preparation
• Intensive Training: Not until 6 – 9 months prior to implementation 10/1/2014
• LTC Coders: 16 hours (ICD-10-CM only for current trained coders)
• (Check with our timeline for consistency)
55

Coder Preparation2013-2014
•Obtain ‘refresher’ training for biomedical sciences
•Anatomy and Physiology•Medical Terminology•Pathophysiology•Pharmacology
56

Transitioning from ICD-9 to ICD-10 LTC
1st Quarter 2014 (January – March)
• Formal training for staff followed by “hands-on practice”
• Determine if coders have been using ICD-9-CM code lists (e.g. ‘cheat’ sheets). These will require updating if processes are appropriate. (e.g. list of codes for unit clerks for lab requisitions)
• Determine if there are any forms which will need to be revised to allow for 7 characters
• Determine whether software is compatible with ICD-10-CM
57

Transitioning from ICD-9 to ICD-10 LTC
• 2nd Quarter 2014 (April – June)
• Begin using ICD 9 codes with clear diagnostic descriptions, similar to those used in ICD 10 for ease in re-coding.
• Print diagnosis lists of current residents and code diagnoses with ICD-10-CM (Take sample number each week) for practice
• Maintain ICD-10-CM coded diagnosis lists (in case resident remains in facility)
• Continue to practice, practice, practice!! 58

Transitioning ICD-9 to ICD-10 LTC
3rd Quarter 2014 (July – September)
• Dual code using both ICD-9 & ICD-10• By July 1, 2014
• Determine if your software will be available and capable of dual coding
• All new admissions, • hospital returns, and • continued stayPLEASE NOTE: ICD-10-CM CONVERSION DOES NOT APPLY IN
WORKMEN’S COMP CASES
• Continue updating diagnosis lists and codes according to MDS schedule until all residents’ diagnosis lists have been updated.
59

Transitioning from ICD-9 to ICD-10 LTC
4th Quarter 2014 (Oct. – December)
• Apply ICD-10-CM codes for all diagnoses for all admissions and MDSs starting October 1, 2014.
• Maintain Legacy ICD-9-CM Coding System
• Monitor claims & denials for coding errors and vendor problems 60

Billing Claims
• CMS working to address claims that overlap from September 30, 2014 into October 2014 (SNFs)
• All Claims submitted for services on or before September 30, 2014 will use ICD-9 codes
• ICD-10 codes will not be recognized/accepted on claims BEFORE 10-1-2014 61

Billing Claims
• All claims submitted for services provided on or after October 1, 2014 will use ICD 10 codes
• Claims cannot contain BOTH ICD-9 codes and ICD-10 codes
• Claims using ICD-9-CM after 10/1/14 will be rejected
62

Billing Claims
• Facilities behind in billing Medicare?• Use added transition time to get
caught up with billing.• Be current on go-live date
63

RESOURCES
• American Health Information Management Association http://www.ahima.org
• American Association of Professional Coders http://www.aapc.com
• Centers for Medicare and Medicaid Services http://www.cms.gov/Medicare/Coding/ICD10/index.html
• http://www.cms.gov/Medicare/Coding/ICD10/CMSImplementationPlanning.html
• http://www.cms.gov/Medicare/Coding/ICD10/ProviderResources.html
• Centers for Disease Control http://www.cdc.gov/nchs/icd/icd10cm.htm
64

65

66

67

68

Special Thanks to the AHIMA 2012 LTPAC Practice Council
Coding & Reimbursement Strategy Team
Nancy Benson, RHIA
Molly Cahill, RHIA
Michelle Dick, RHIA
Deborah Johnson, RHIT, CHP
Leslie Joyner, RHIT
Kathie McClary, RHIT
Tamela McQuiston, RHIT, RAC-CT
Renae Spohn, RHIA
Monica Tormey, RHIA
Carol Young, RHIT
69