Embed Size (px)
DESCRIPTION
Il rischio Cardiovascolare : aspetti patogenetici e diagnostici Il ruolo del Sodio Carmine Zoccali. What really defined the decade was the rise of China. By Fareed Zakaria. Huang Ti, 2698–2598 BC (the Yellow Emperor). ‘Hence if too much salt is used for food, the pulse hardens ...’. - PowerPoint PPT Presentation
Citation preview
Il rischio Cardiovascolare : aspetti patogenetici Il rischio Cardiovascolare : aspetti patogenetici e diagnosticie diagnostici
Il ruolo del SodioIl ruolo del Sodio
Carmine Zoccali Carmine Zoccali
Huang Ti, 2698–2598 BC (the Yellow Emperor)
What really defined the decade was What really defined the decade was the rise of China.the rise of China. By Fareed ZakariaBy Fareed Zakaria
‘Hence if too much salt is used for food, the pulse hardens ...’
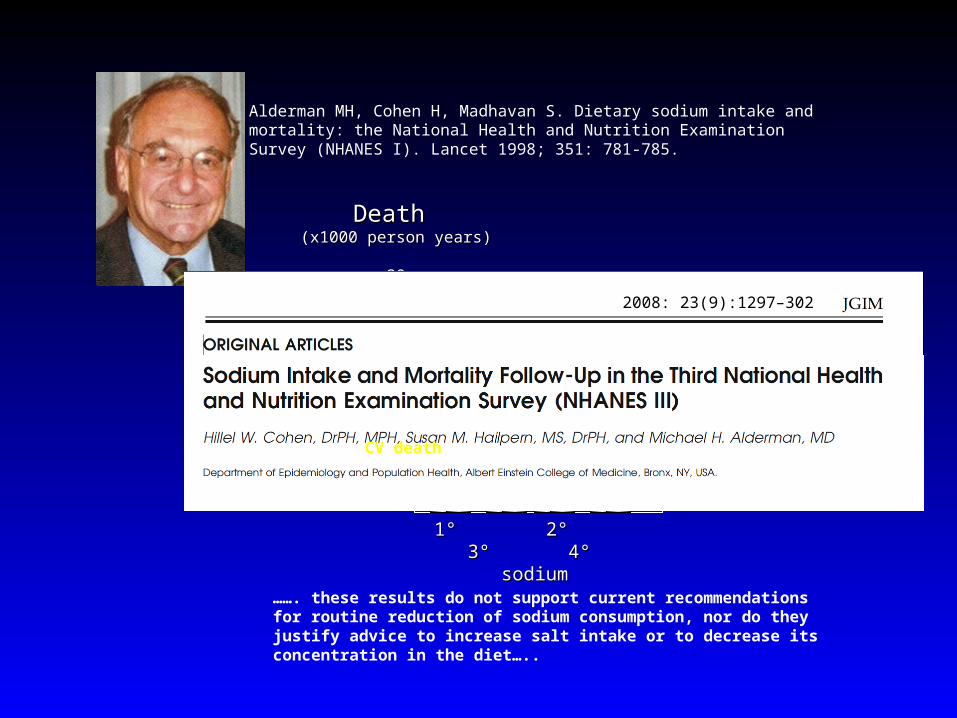
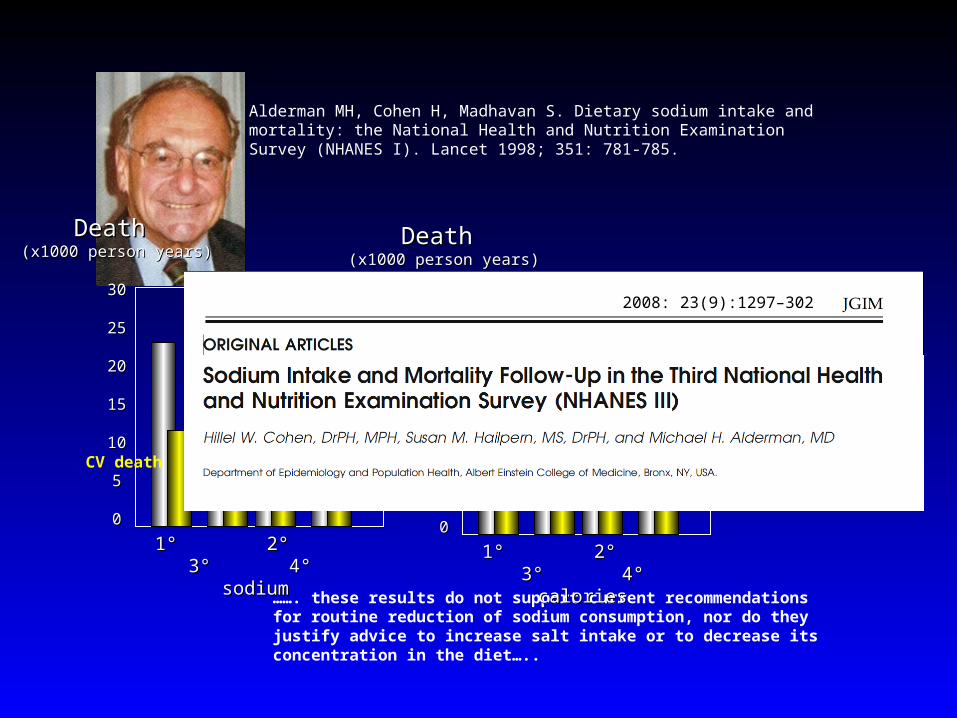
Alderman MH, Cohen H, Madhavan S. Dietary sodium intake and mortality: the National Health and Nutrition Examination Survey (NHANES I). Lancet 1998; 351: 781-785.
Death Death (x1000 person years)(x1000 person years)
3030
2525
2020
1515
1010
55
00
1° 2° 3° 4° 1° 2° 3° 4° sodiumsodium
……. these results do not support current recommendations for routine reduction of sodium consumption, nor do they justify advice to increase salt intake or to decrease its concentration in the diet…..
2008: 23(9):1297–302
CV death
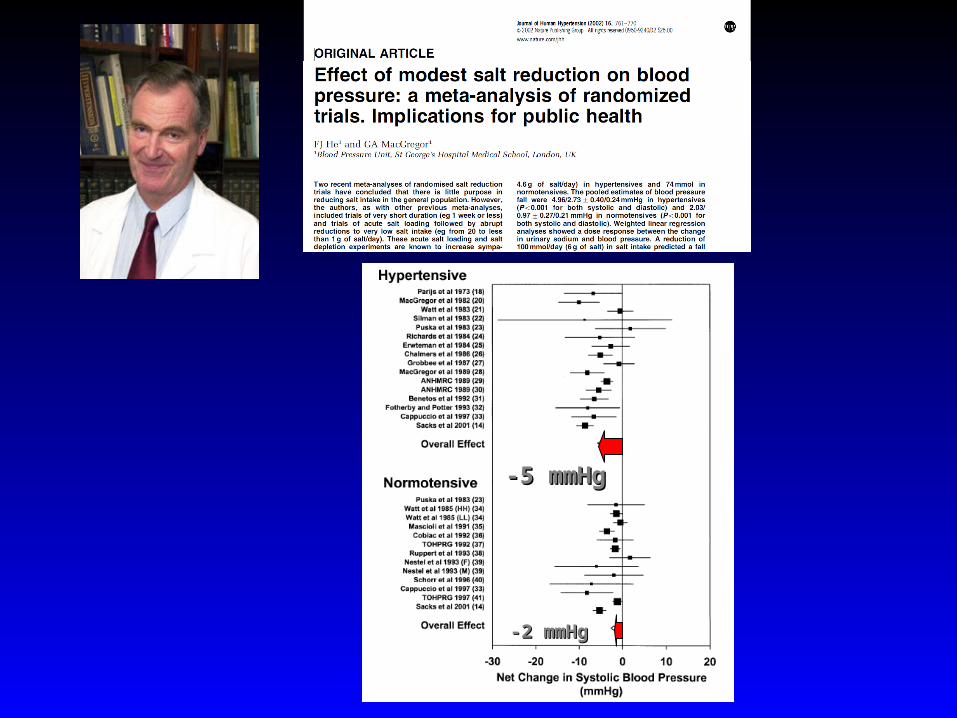
-5 mmHg-5 mmHg
-2 mmHg-2 mmHg
.......Absent convincing scientific evidence of a benefit to eating less .......Absent convincing scientific evidence of a benefit to eating less salt, much less an assurance of safety, it might be wiser for the NY dpt. salt, much less an assurance of safety, it might be wiser for the NY dpt. of Health to press for the research that could provide a solid scientific of Health to press for the research that could provide a solid scientific basis for action……basis for action……
The New York TimesThe New York Times
A Pinch of ScienceA Pinch of Science
by Michael Aldermanby Michael Alderman9 February 20099 February 2009
New York City Health Department.New York City Health Department.
20082008Salt reduction (-40%) in processed foodSalt reduction (-40%) in processed food
& Carmine Zoccali
End Stage Renal DiseaseEnd Stage Renal Disease
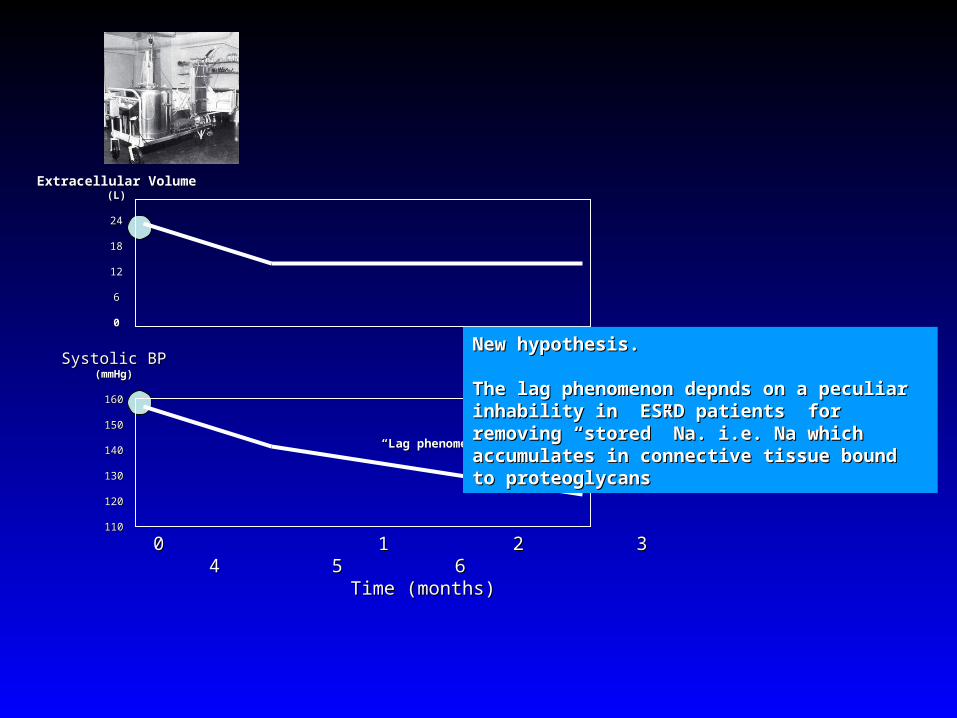
Systolic BPSystolic BP(mmHg)(mmHg)
160160
150150
140140
130130
120120
110110
0 1 2 3 4 5 60 1 2 3 4 5 6Time (months)Time (months)
Extracellular VolumeExtracellular Volume(L)(L)
2424
1818
1212
66
00
““Lag phenomenon” Lag phenomenon”
New hypothesis.New hypothesis.
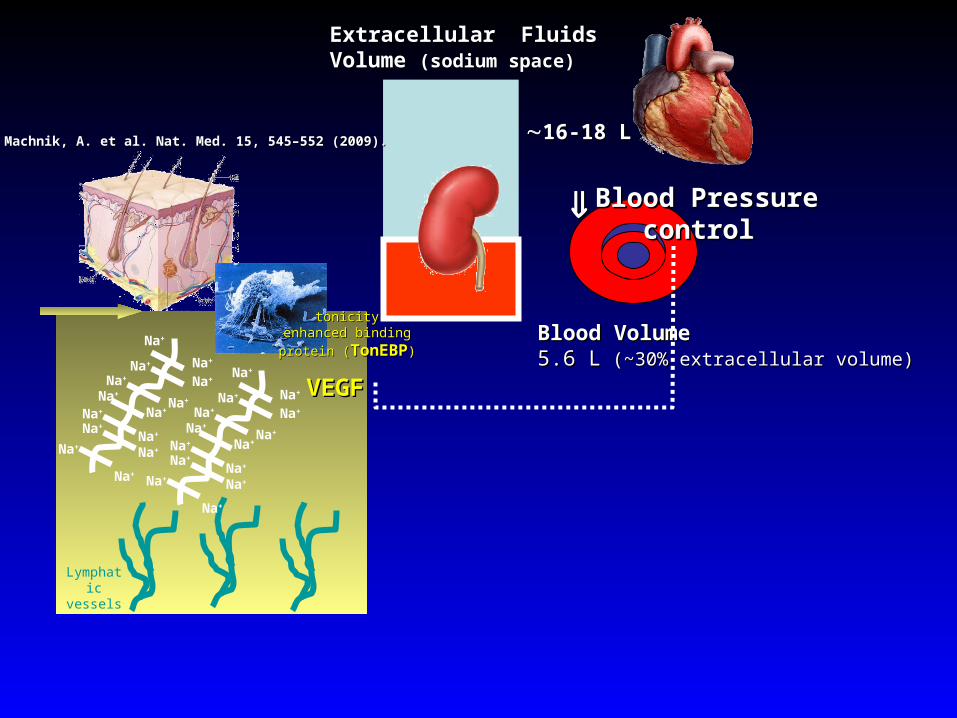
The lag phenomenon depnds on a peculiar The lag phenomenon depnds on a peculiar inhability in ESRD patients for removing “stored” inhability in ESRD patients for removing “stored” Na. i.e. Na which accumulates in connective tissue Na. i.e. Na which accumulates in connective tissue bound to proteoglycansbound to proteoglycans
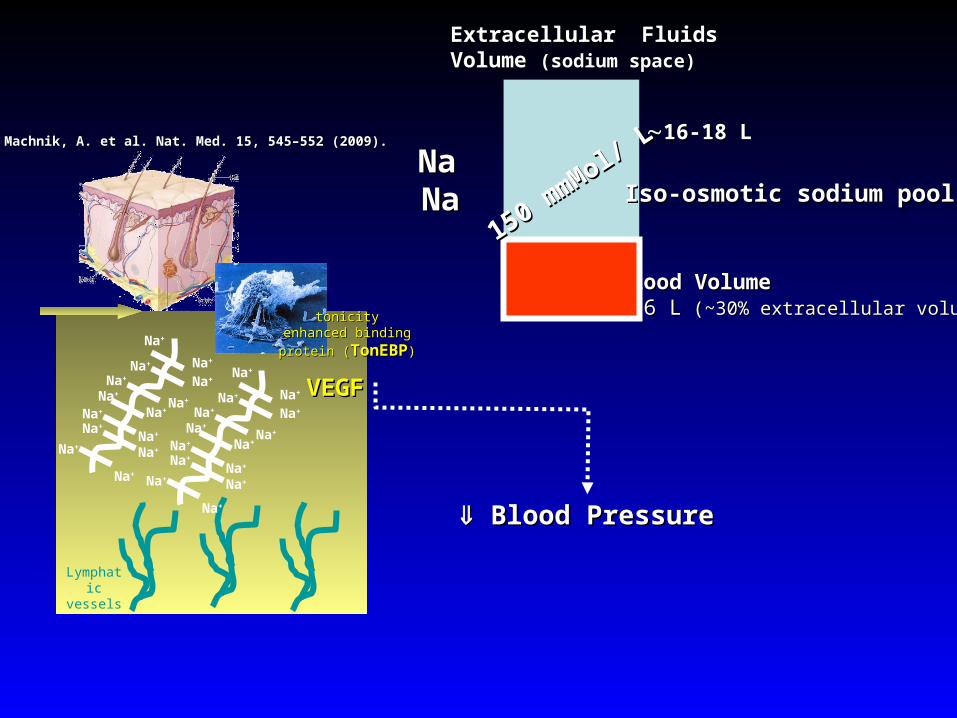
16-18 L16-18 L
Blood Volume Blood Volume 5.6 L5.6 L ( (~30% extracellular volume)~30% extracellular volume)
Extracellular Fluids Extracellular Fluids Volume Volume (sodium space)(sodium space)
Blood Pressure Blood Pressure
Na+
Na+
Na+
Na+
Na+
Na+
Na+
Na+Na+
Na+
Na+
Na+
Na+
Na+
Lymphatic vessels
tonicitytonicityenhanced binding protein enhanced binding protein
((TonEBPTonEBP))
VEGFVEGFNa+
Na+
Na+
Na+
Na+
Na+
Na+
Na+Na+
Na+
Na+
Na+
Na+
Na+
Machnik, A. et al. Nat. Med. 15, 545–552 (2009).Machnik, A. et al. Nat. Med. 15, 545–552 (2009).
150 mmMol/ L
150 mmMol/ L
Iso-osmotic sodium poolIso-osmotic sodium poolNaNaNaNa
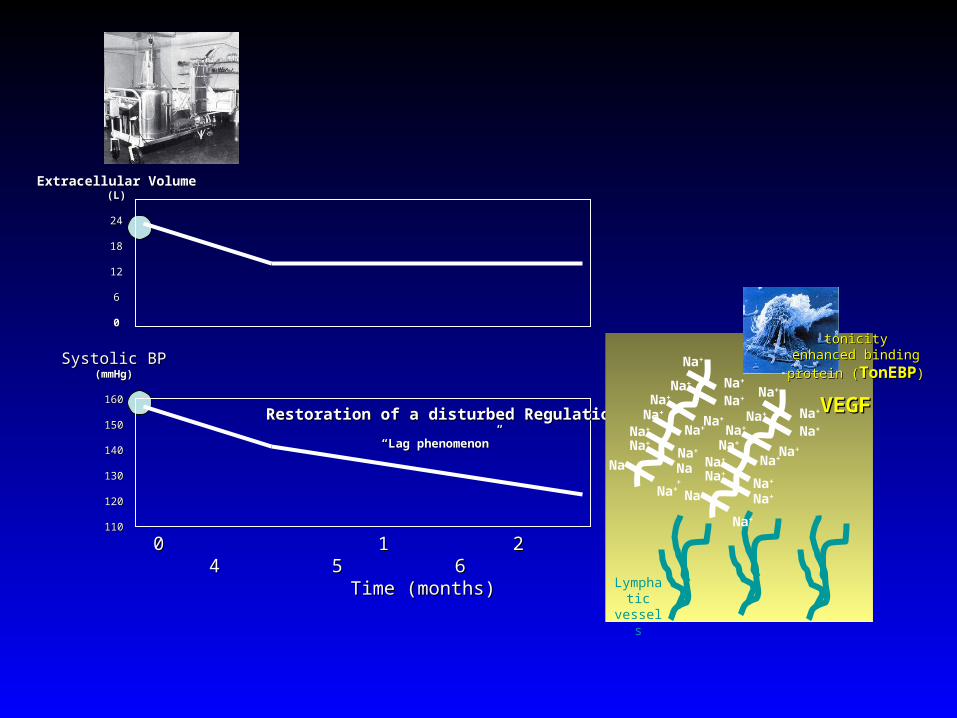
Systolic BPSystolic BP(mmHg)(mmHg)
160160
150150
140140
130130
120120
110110
0 1 2 3 4 5 60 1 2 3 4 5 6Time (months)Time (months)
Extracellular VolumeExtracellular Volume(L)(L)
2424
1818
1212
66
00
““Lag phenomenon” Lag phenomenon”
Restoration of a disturbed Regulation? Restoration of a disturbed Regulation?
Na+
Na+
Na+
Na+
Na+
Na+
Na+
Na+Na+
Na+
Na+
Na+
Na+
Na+
Lymphatic
vessels
tonicitytonicityenhanced binding protein enhanced binding protein
((TonEBPTonEBP))
VEGFVEGFNa+
Na+
Na+
Na+
Na+
Na+
Na+
Na+Na+
Na+
Na+
Na+
Na+
Na+
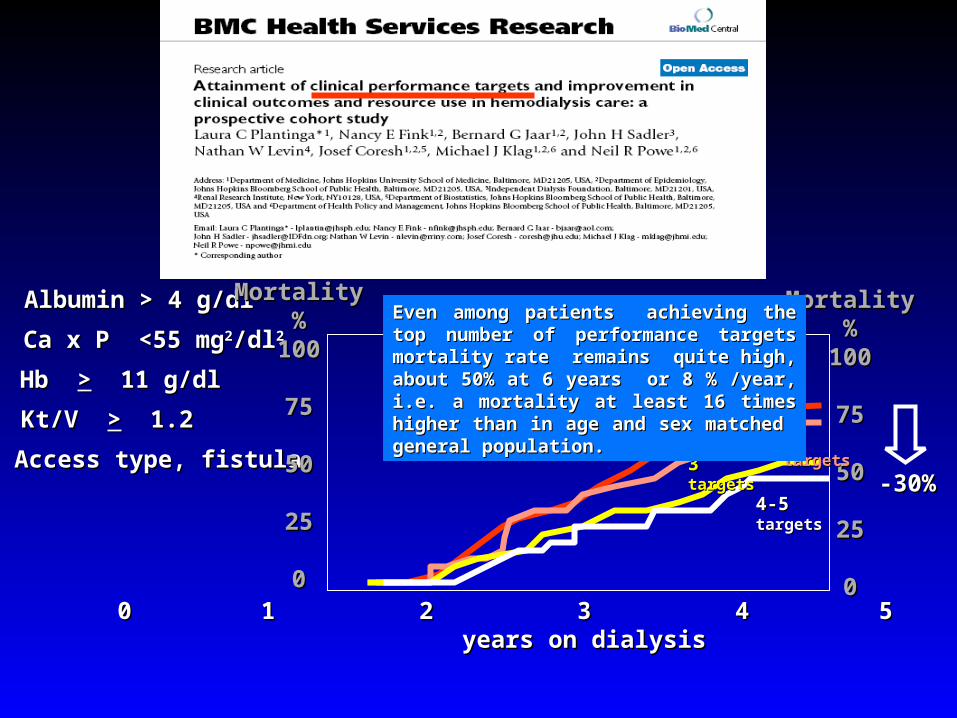
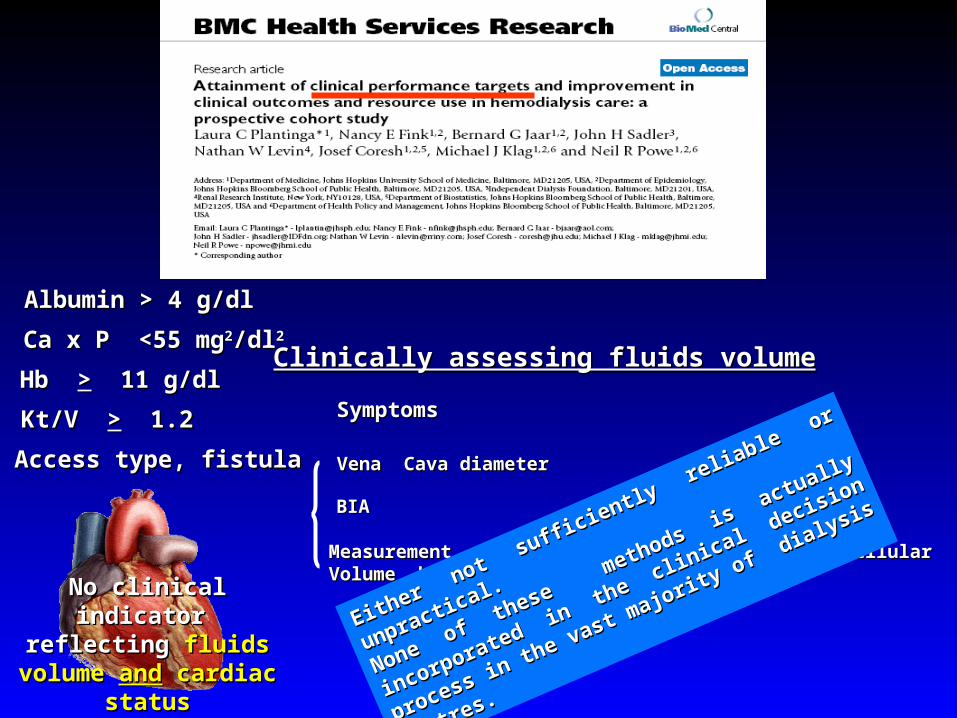
Albumin > 4 g/dlAlbumin > 4 g/dl
Ca x P <55 mgCa x P <55 mg22/dl/dl22
Kt/V Kt/V >> 1.2 1.2
Hb Hb >> 11 g/dl 11 g/dl
Access type, fistulaAccess type, fistula
MortalityMortality%%
100100
7575
5050
2525
000 1 2 3 4 5 60 1 2 3 4 5 6
years on dialysisyears on dialysis
MortalityMortality%%
100100
7575
5050
2525
00
0-10-1 targets targets
22 targets targets
33 targets targets
4-5 4-5 targets targets-30%-30%
Even among patients achieving the top Even among patients achieving the top number of performance targets mortality rate number of performance targets mortality rate remains quite high, about 50% at 6 years or remains quite high, about 50% at 6 years or 8 % /year, i.e. a mortality at least 16 times 8 % /year, i.e. a mortality at least 16 times higher than in age and sex matched general higher than in age and sex matched general population. population.
Albumin > 4 g/dlAlbumin > 4 g/dl
Ca x P <55 mgCa x P <55 mg22/dl/dl22
Kt/V Kt/V >> 1.2 1.2
Hb Hb >> 11 g/dl 11 g/dl
Access type, fistulaAccess type, fistula
No clinical indicator No clinical indicator reflecting reflecting fluids volume fluids volume
andand cardiac status cardiac status
Clinically assessing fluids volumeClinically assessing fluids volume
BIABIA
Measurement of Plasma or Blood Volume orExtracellular Volume Measurement of Plasma or Blood Volume orExtracellular Volume by radio-isotopic methods.by radio-isotopic methods.
Vena Cava diameter Vena Cava diameter
Either not sufficiently reliable or unpractical.
Either not sufficiently reliable or unpractical.
None of these m
ethods is actually incorporated in
None of these m
ethods is actually incorporated in
the clinical decision process in the vast majority
of
the clinical decision process in the vast majority
of
dialysis centres.
dialysis centres.
SymptomsSymptoms
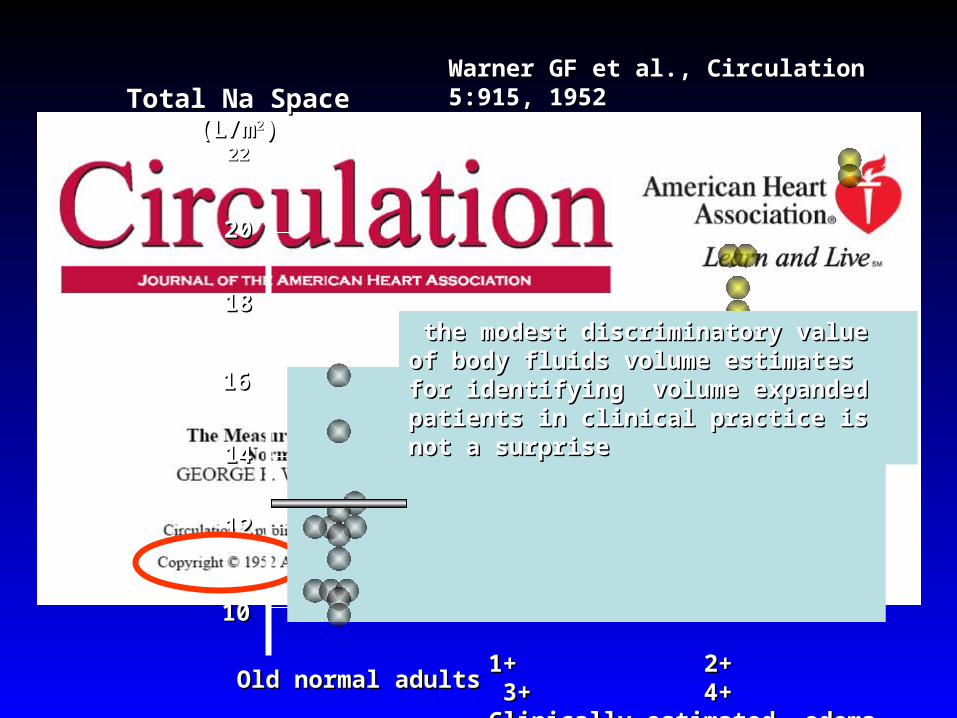
Poor discriminatory Poor discriminatory power of body fluids power of body fluids
volume measurements volume measurements for guiding therapy for guiding therapy
1+ 2+ 3+ 4+1+ 2+ 3+ 4+Clinically estimated edemaClinically estimated edema
Total Na SpaceTotal Na Space(L/m(L/m22))
2222
2020
1818
1616
1414
1212
1010
Old normal adultsOld normal adults
Warner GF et al., Circulation 5:915, 1952Warner GF et al., Circulation 5:915, 1952
the modest discriminatory value of body the modest discriminatory value of body fluids volume estimates for identifying fluids volume estimates for identifying volume expanded patients in clinical volume expanded patients in clinical practice is not a surprisepractice is not a surprise
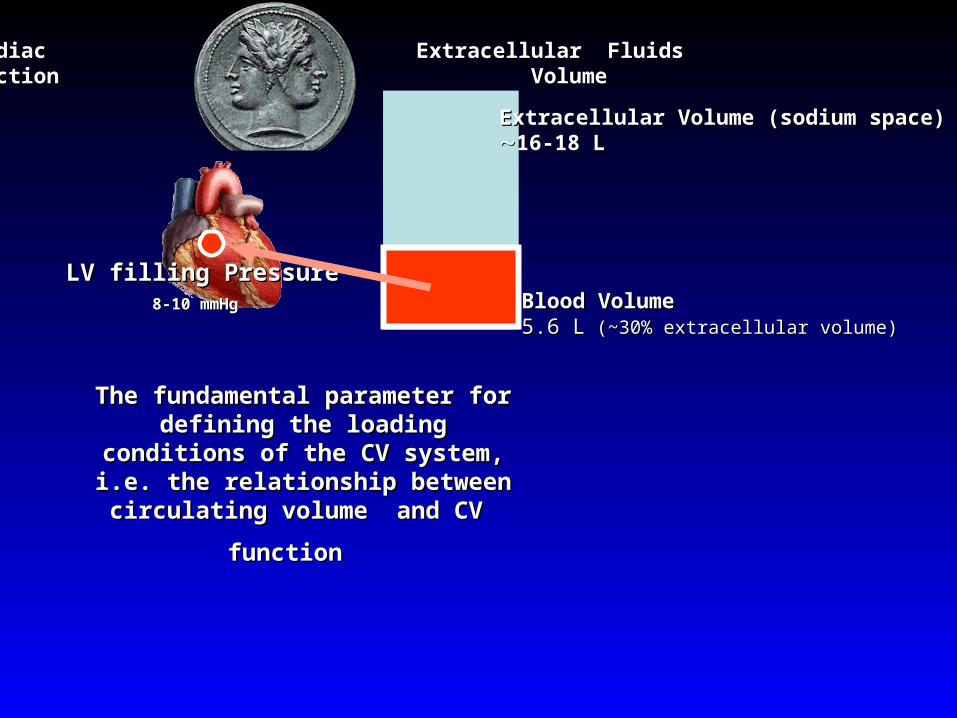
Extracellular Volume (sodium space)Extracellular Volume (sodium space)16-18 L16-18 L
Blood Volume Blood Volume 5.6 L5.6 L ( (~30% extracellular volume)~30% extracellular volume)
LV filling PressureLV filling Pressure8-10 mmHg8-10 mmHg
Cardiac Extracellular Fluids Cardiac Extracellular Fluids function Volumefunction Volume
The fundamental parameter for The fundamental parameter for defining the loading conditions of defining the loading conditions of the CV system, i.e. the relationship the CV system, i.e. the relationship
between circulating volume and CV between circulating volume and CV
function function
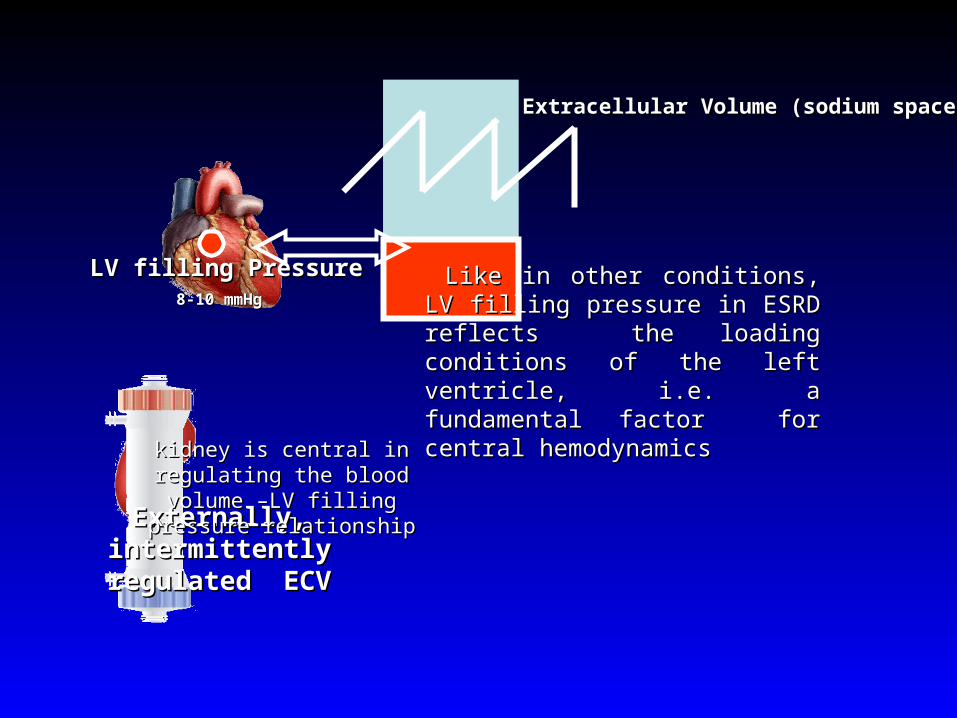
Extracellular Volume (sodium space)Extracellular Volume (sodium space)
LV filling PressureLV filling Pressure8-10 mmHg8-10 mmHg
Externally, intermittently Externally, intermittently regulated ECVregulated ECV
Like in other conditions, LV filling Like in other conditions, LV filling pressure in ESRD reflects the pressure in ESRD reflects the loading conditions of the left loading conditions of the left ventricle, i.e. a fundamental factor ventricle, i.e. a fundamental factor for central hemodynamicsfor central hemodynamics
kidney is central in regulating the kidney is central in regulating the blood volume –LV filling pressure blood volume –LV filling pressure
relationshiprelationship
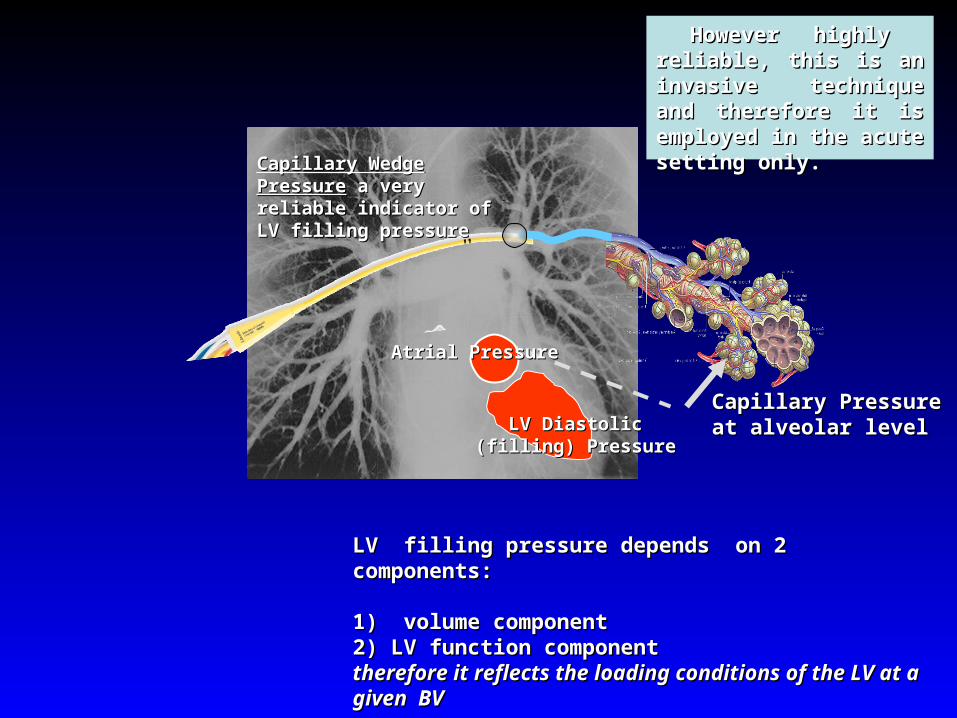
Capillary Pressure at Capillary Pressure at alveolar levelalveolar level
Atrial PressureAtrial Pressure
LV Diastolic (filling) LV Diastolic (filling) PressurePressure
LV filling pressure depends on 2 components:LV filling pressure depends on 2 components:
1) volume component 1) volume component 2) LV function component2) LV function componenttherefore it reflects the loading conditions of the LV at a therefore it reflects the loading conditions of the LV at a given BVgiven BV
Capillary Wedge PressureCapillary Wedge Pressure a very reliable indicator of a very reliable indicator of LV filling pressureLV filling pressure
However highly reliable, However highly reliable, this is an invasive this is an invasive technique and therefore it technique and therefore it is employed in the acute is employed in the acute setting only.setting only.
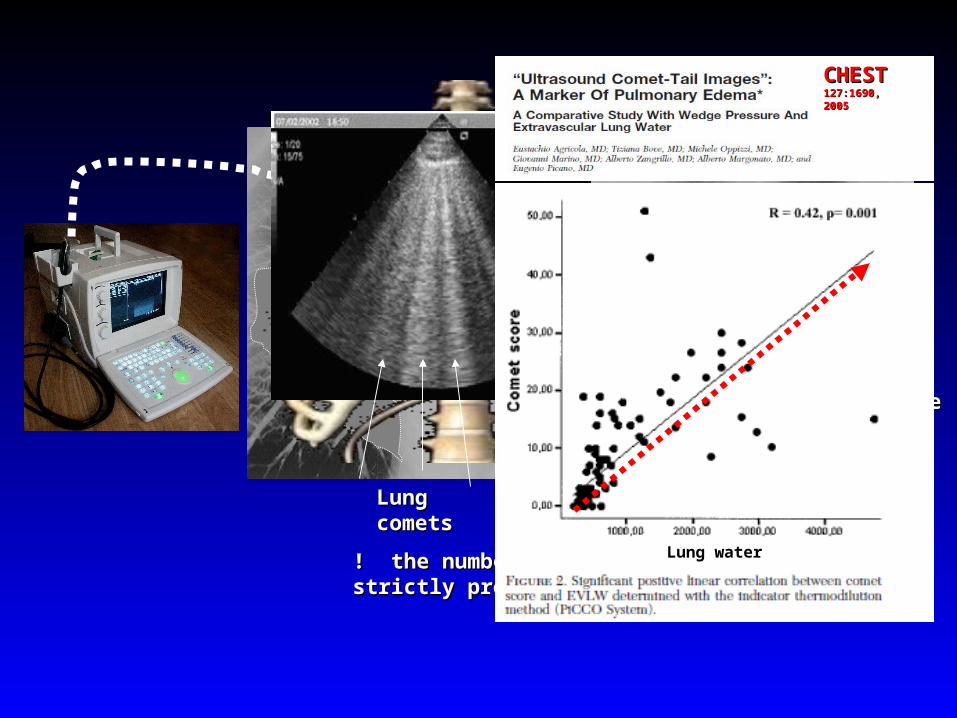
Capillary Pressure at Capillary Pressure at alveolar levelalveolar level
Pulmonary WaterPulmonary Water
normalnormal
Pulmonary edemaPulmonary edema
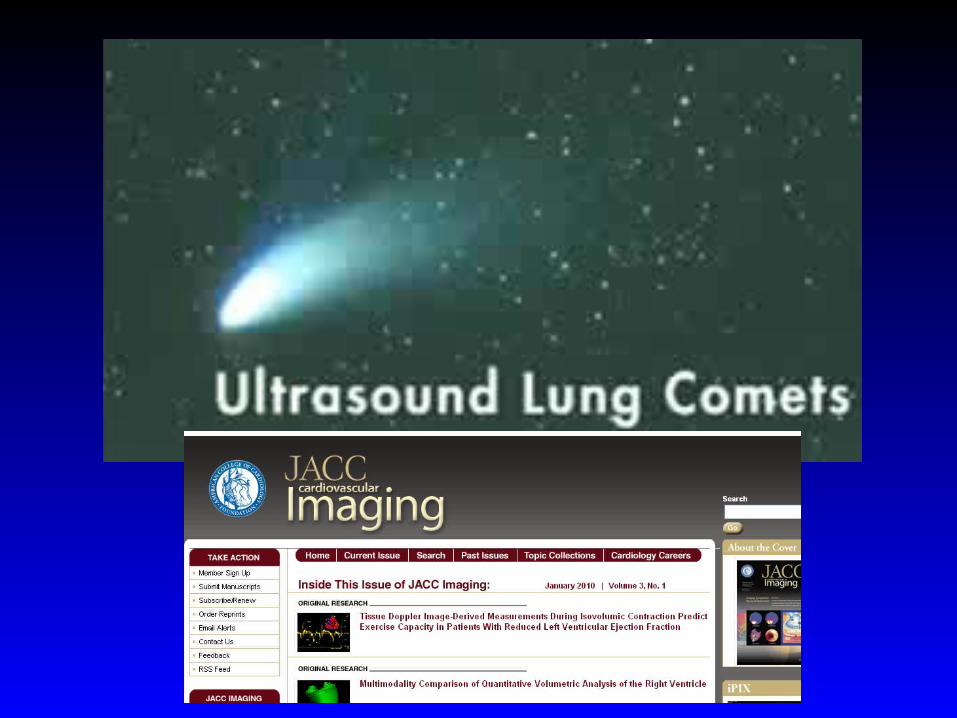
Lung cometsLung comets
! the number of lung comets is strictly ! the number of lung comets is strictly proportional to lung waterproportional to lung water
Lung water
CHESTCHEST127:1690, 2005127:1690, 2005
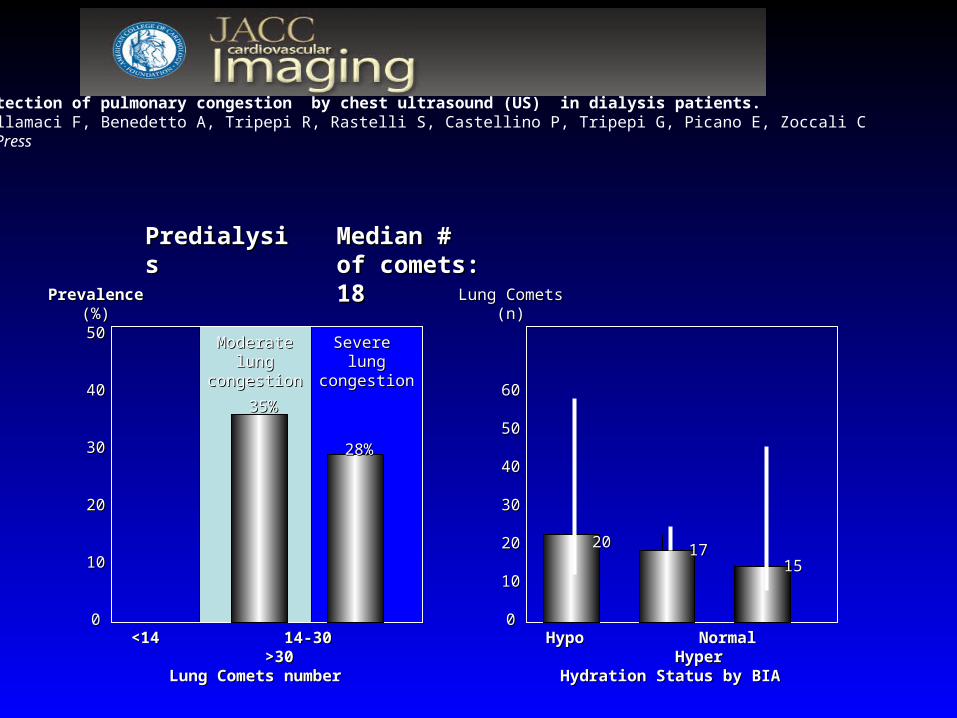
Severe lung Severe lung congestioncongestion
Moderate lung Moderate lung congestioncongestion
<14 14-30 >30<14 14-30 >30Lung Comets numberLung Comets number
PrevalencePrevalence(%)(%)5050
4040
3030
2020
1010
00
35%35%
28%28%
Hypo Normal HyperHypo Normal HyperHydration Status by BIAHydration Status by BIA
Lung CometsLung Comets(n)(n)
6060
5050
4040
3030
2020
1010
00
17172020
1515
PredialysisPredialysis
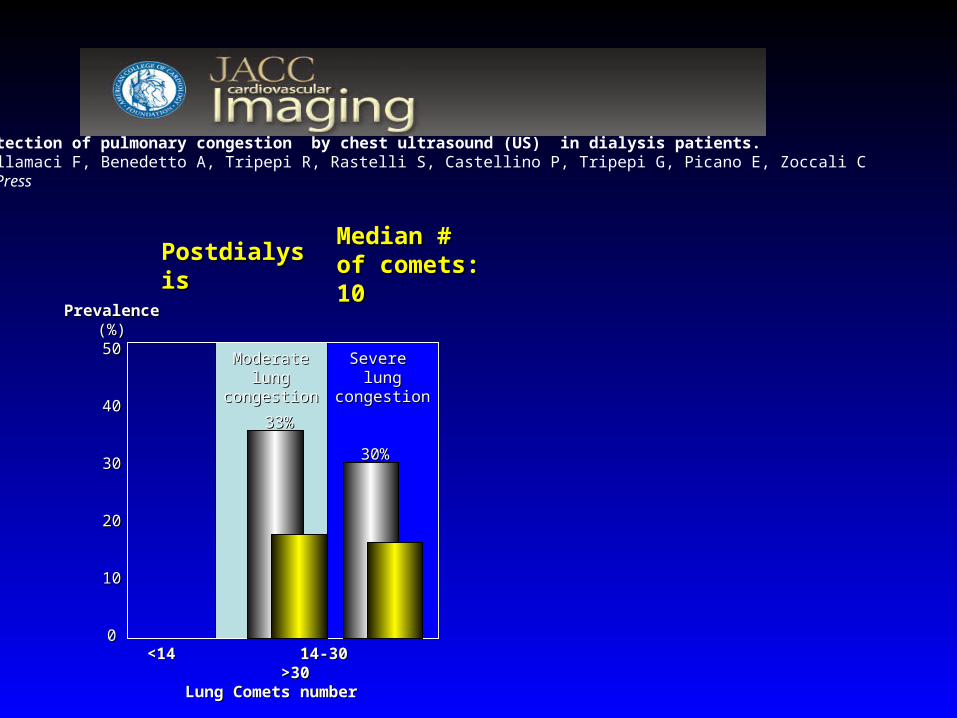
Detection of pulmonary congestion by chest ultrasound (US) in dialysis patients.Mallamaci F, Benedetto A, Tripepi R, Rastelli S, Castellino P, Tripepi G, Picano E, Zoccali CIn Press
Median # of Median # of comets: 18comets: 18
Detection of pulmonary congestion by chest ultrasound (US) in dialysis patients.Mallamaci F, Benedetto A, Tripepi R, Rastelli S, Castellino P, Tripepi G, Picano E, Zoccali CIn Press
Severe lung Severe lung congestioncongestion
Moderate lung Moderate lung congestioncongestion
<14 14-30 >30<14 14-30 >30Lung Comets numberLung Comets number
PrevalencePrevalence(%)(%)5050
4040
3030
2020
1010
00
33%33%
30%30%
PostdialysisPostdialysisMedian # of Median # of comets: 10comets: 10
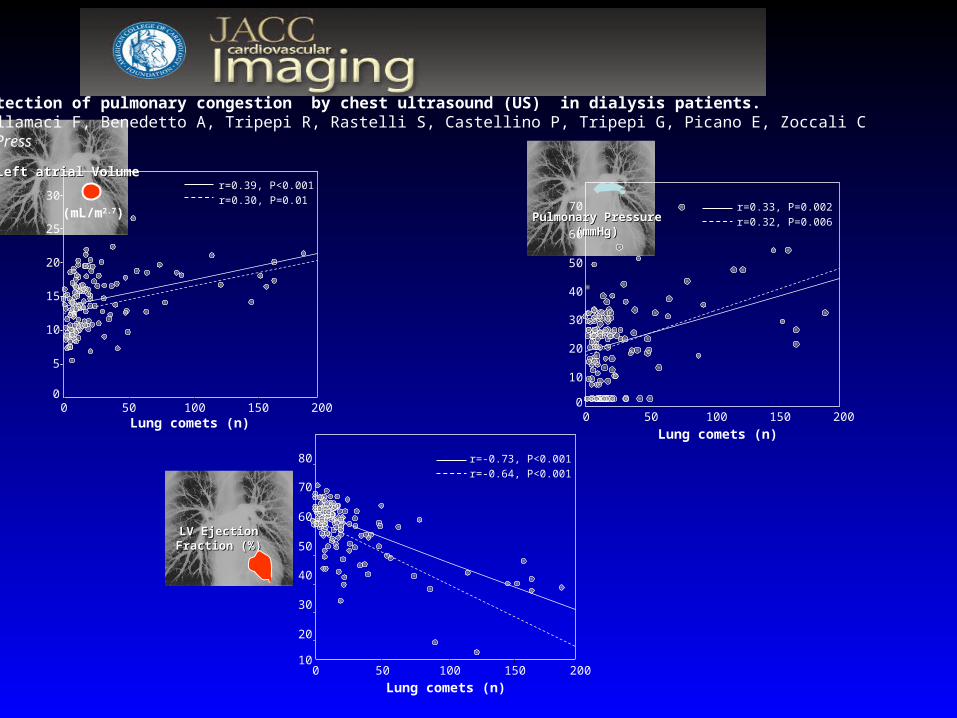
Pulmonary PressurePulmonary Pressure(mmHg)(mmHg)
Left atrial VolumeLeft atrial Volume
r=0.33, P=0.002
r=0.32, P=0.006
70
60
50
40
30
20
10
0200150100500
Lung comets (n)
r=0.39, P<0.001
r=0.30, P=0.0130
25
20
15
10
5
0
(mL/m2.7)
200150100500Lung comets (n)
r=-0.73, P<0.001
r=-0.64, P<0.001
80
70
60
50
40
30
20
10200150100500
Lung comets (n)
Detection of pulmonary congestion by chest ultrasound (US) in dialysis patients.Mallamaci F, Benedetto A, Tripepi R, Rastelli S, Castellino P, Tripepi G, Picano E, Zoccali CIn Press
LV Ejection LV Ejection Fraction (%)Fraction (%)
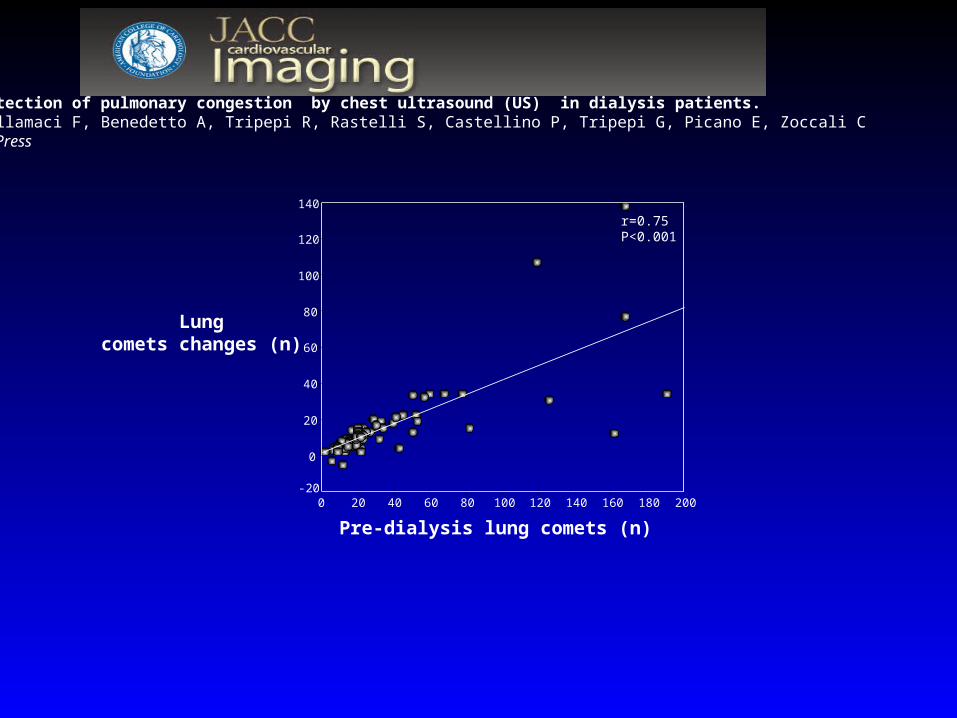
200180160140120100806040200
Pre-dialysis lung comets (n)
140
120
100
80
60
40
20
0
-20
Lungcomets changes (n)
r=0.75P<0.001
Detection of pulmonary congestion by chest ultrasound (US) in dialysis patients.Mallamaci F, Benedetto A, Tripepi R, Rastelli S, Castellino P, Tripepi G, Picano E, Zoccali CIn Press
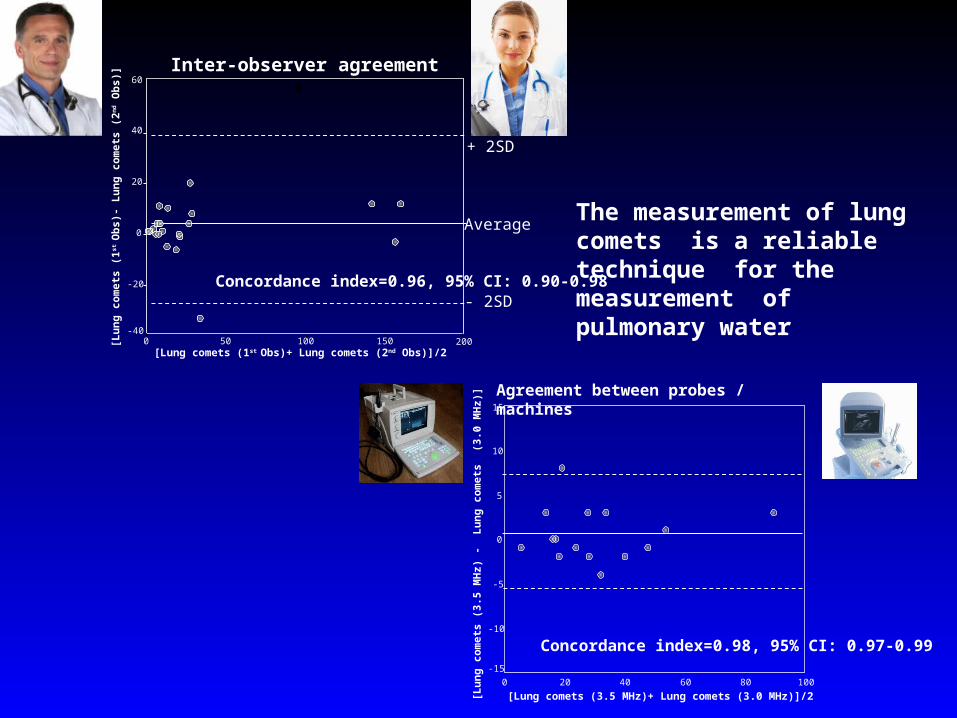
+ 2SD
- 2SD
Average
Concordance index=0.96, 95% CI: 0.90-0.98
Inter-observer agreement60
40
20
0
-20
-40
[Lu
ng
co
met
s (1
st O
bs)
- L
un
g c
om
ets
(2n
d O
bs)
]
200150100500[Lung comets (1st Obs)+ Lung comets (2nd Obs)]/2
Concordance index=0.98, 95% CI: 0.97-0.99
[Lung comets (3.5 MHz)+ Lung comets (3.0 MHz)]/210080604020
[Lu
ng
co
met
s (3
.5 M
Hz)
-
Lu
ng
co
met
s (
3.0
MH
z)]
0
15
10
5
0
-5
-10
-15
Agreement between probes / machines
The measurement of lung comets is a reliable technique for the measurement of pulmonary water
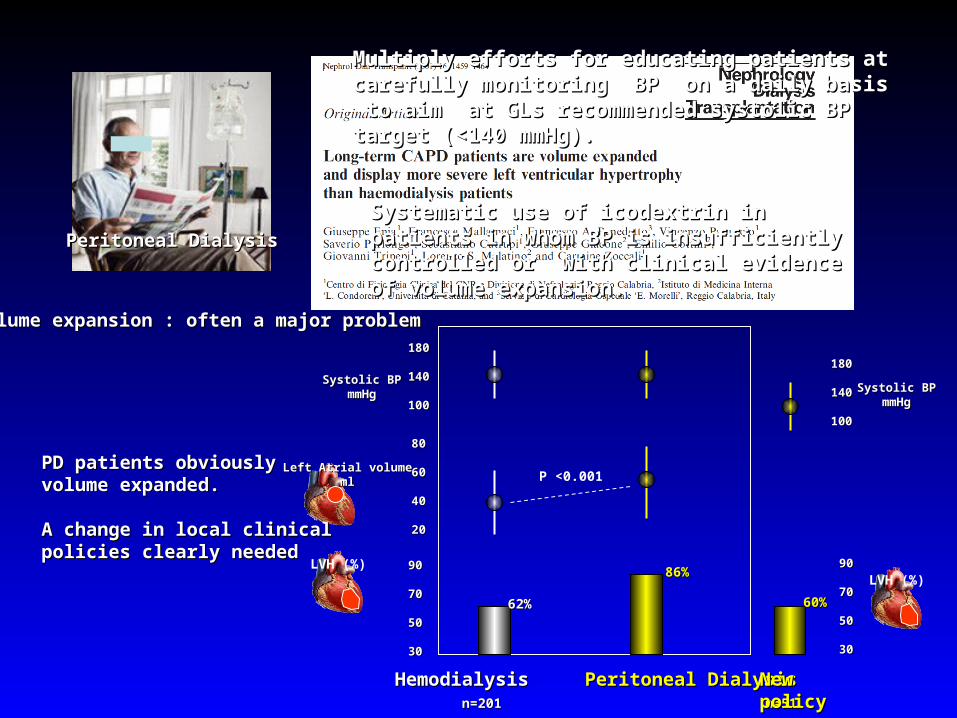
Peritoneal DialysisPeritoneal Dialysis
Volume expansion : often a major problemVolume expansion : often a major problem
Hemodialysis Hemodialysis Peritoneal DialysisPeritoneal Dialysis n=201 n=201 n=51n=51
Systolic BPSystolic BPmmHgmmHg
180180
140140
100100
Left Atrial volumeLeft Atrial volumemlml
8080
6060
4040
2020
9090
7070
5050
3030
LVH (%)
62%62%
86%86%
P <0.001PD patients obviously volume PD patients obviously volume expanded.expanded.
A change in local clinical policies A change in local clinical policies clearly needed clearly needed
60%60%
Systolic BPSystolic BPmmHgmmHg
180180
140140
100100
9090
7070
5050
3030
LVH (%)
New New policypolicy
Multiply efforts for educating patients at carefully Multiply efforts for educating patients at carefully monitoring BP on a daily basis to aim at GLs monitoring BP on a daily basis to aim at GLs recommended systolic BP target (<140 mmHg).recommended systolic BP target (<140 mmHg).
Systematic use of icodextrin in patients in Systematic use of icodextrin in patients in whom BP is insufficiently controlled or with whom BP is insufficiently controlled or with clinical evidence of volume expansion.clinical evidence of volume expansion.
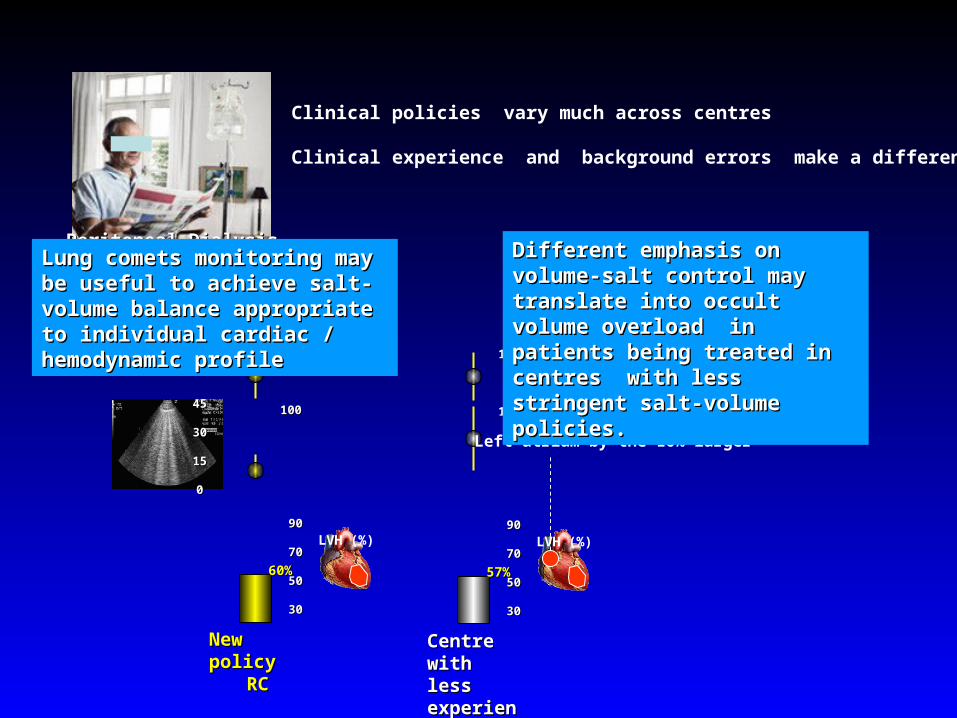
Clinical policies vary much across centres
Clinical experience and background errors make a difference
Peritoneal DialysisPeritoneal Dialysis
Systolic BPSystolic BPmmHgmmHg
140140
100100
9090
7070
5050
3030
LVH (%)
New New policypolicy
RCRC
60%60%
4545
3030
1515
00
Systolic BPSystolic BPmmHgmmHg
140140
100100
9090
7070
5050
3030
LVH (%)
Centre Centre with less with less experiencexperiencee
57%57%
Left atrium by the 10% larger
Different emphasis on volume-Different emphasis on volume-salt control may translate into salt control may translate into occult volume overload in occult volume overload in patients being treated in centres patients being treated in centres with less stringent salt-volume with less stringent salt-volume policies.policies.
Lung comets monitoring may be Lung comets monitoring may be useful to achieve salt-volume useful to achieve salt-volume balance appropriate to individual balance appropriate to individual cardiac / hemodynamic profilecardiac / hemodynamic profile
Lung comets monitoring may be Lung comets monitoring may be useful to achieve salt-volume useful to achieve salt-volume balance appropriate to individual balance appropriate to individual cardiac / hemodynamic profilecardiac / hemodynamic profile
late eightieslate eighties
BIA bielectrical impedance analysisBIA bielectrical impedance analysis
enthusiasmenthusiasm
disappointementdisappointement
controversycontroversy
NO APPROPRIATE CLINICAL TRIAL NO APPROPRIATE CLINICAL TRIAL TESTING THE USEFULNESS OF TESTING THE USEFULNESS OF THIS TECHNIQUE OVER 20 YEARS THIS TECHNIQUE OVER 20 YEARS OF CLINICAL APPLICATION.OF CLINICAL APPLICATION.
A clinical trial based on a A clinical trial based on a management strategy guided by management strategy guided by lung comets neededlung comets needed
S S & & C C
La storia dei rapporti tra sale e rischio cardiovascolare a livello di La storia dei rapporti tra sale e rischio cardiovascolare a livello di popolazione è lunga e controversa ma è assodato che un eccesso di sale / popolazione è lunga e controversa ma è assodato che un eccesso di sale / volume pone alti rischi nell’insufficienza renale. volume pone alti rischi nell’insufficienza renale.
L’eccesso di volume innescato dal sale è difficilmente quantificabile nei L’eccesso di volume innescato dal sale è difficilmente quantificabile nei pazienti in dialisi. D’altra parte, per l’alta frequenza di disfunzione pazienti in dialisi. D’altra parte, per l’alta frequenza di disfunzione ventricolare sinistra, la sola misura del volume è insufficiente per guidare ventricolare sinistra, la sola misura del volume è insufficiente per guidare l’ultrafiltrazione in questi pazienti. l’ultrafiltrazione in questi pazienti.
La misura dell’acqua polmonare con gli US è una tecnica promettente in La misura dell’acqua polmonare con gli US è una tecnica promettente in quanto fornisce informazioni affidabili sul grado di congestione polmonare, quanto fornisce informazioni affidabili sul grado di congestione polmonare, cioè su un fenomeno da prevenire o correggere tempestivamente nei cioè su un fenomeno da prevenire o correggere tempestivamente nei pazienti in dialisi.pazienti in dialisi.
L’utilità di questa tecnica deve essere testata in uno specifico trial clinico. L’utilità di questa tecnica deve essere testata in uno specifico trial clinico.
16-18 L16-18 L
Blood Volume Blood Volume 5.6 L5.6 L ( (~30% extracellular volume)~30% extracellular volume)
Extracellular Fluids Extracellular Fluids Volume Volume (sodium space)(sodium space)
Blood PressureBlood Pressurecontrol control
Na+
Na+
Na+
Na+
Na+
Na+
Na+
Na+Na+
Na+
Na+
Na+
Na+
Na+
Lymphatic vessels
tonicitytonicityenhanced binding protein enhanced binding protein
((TonEBPTonEBP))
VEGFVEGF
Na+
Na+
Na+
Na+
Na+
Na+
Na+
Na+Na+
Na+
Na+
Na+
Na+
Na+
Machnik, A. et al. Nat. Med. 15, 545–552 (2009).Machnik, A. et al. Nat. Med. 15, 545–552 (2009).
& Carmine Zoccali
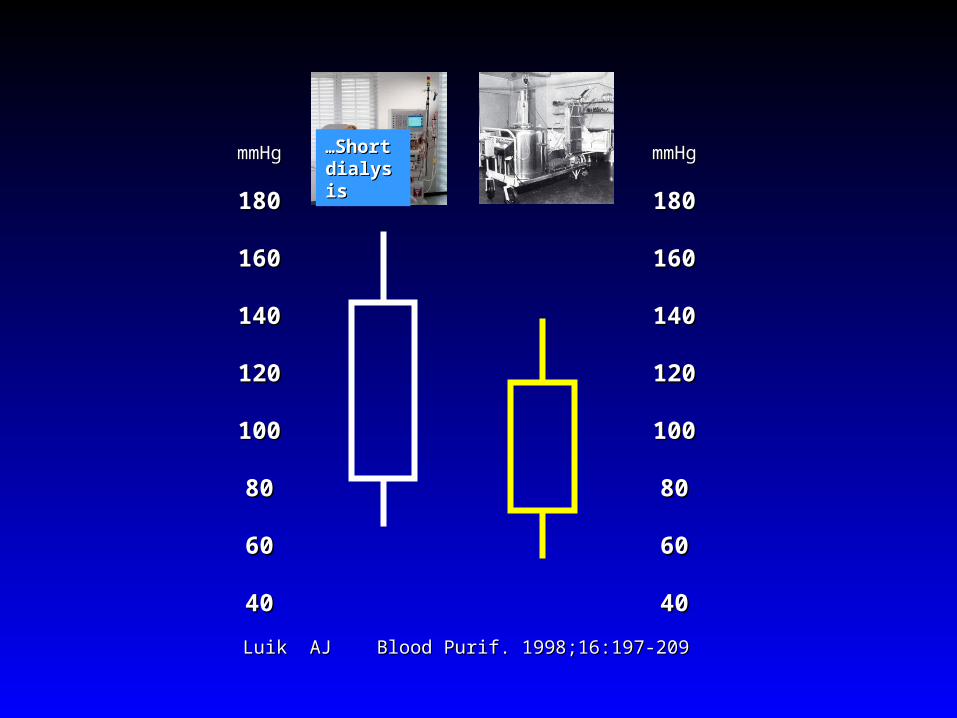
Luik AJ Blood Purif. 1998;16:197-209 Luik AJ Blood Purif. 1998;16:197-209
mmHgmmHg
180180
160160
140140
120120
100100
8080
6060
4040
mmHgmmHg
180180
160160
140140
120120
100100
8080
6060
4040
……Short Short dialysisdialysis
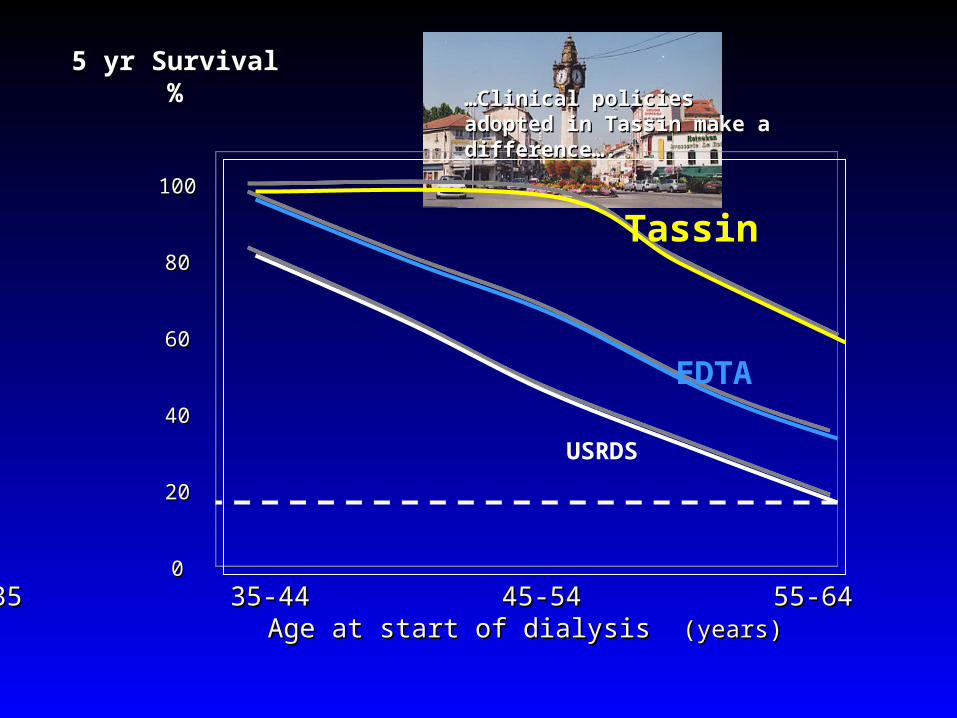
5 yr Survival5 yr Survival%%
<35 35-44 45-54 55-64 >64<35 35-44 45-54 55-64 >64Age at start of dialysis Age at start of dialysis (years)(years)
100100
8080
6060
4040
2020
00
Tassin
EDTA
USRDS
……Clinical policies adopted in Clinical policies adopted in Tassin make a difference…. Tassin make a difference….
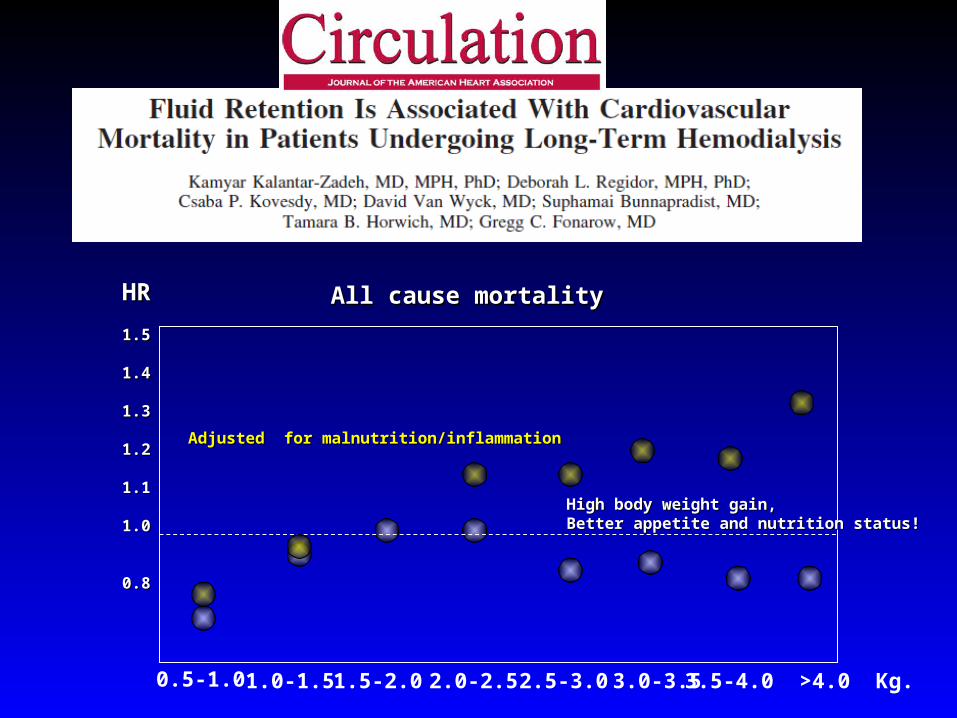
All cause mortalityAll cause mortalityHRHR
1.51.5
1.41.4
1.31.3
1.21.2
1.11.1
1.01.0
0.80.8
0.5-1.0 1.0-1.5 1.5-2.0 2.5-3.0 3.0-3.5 3.5-4.0 >4.0 Kg.2.0-2.5
High body weight gain, High body weight gain, Better appetite and nutrition status!Better appetite and nutrition status!
Adjusted for malnutrition/inflammationAdjusted for malnutrition/inflammation
Alderman MH, Cohen H, Madhavan S. Dietary sodium intake and mortality: the National Health and Nutrition Examination Survey (NHANES I). Lancet 1998; 351: 781-785.
Death Death (x1000 person years)(x1000 person years)
3030
2525
2020
1515
1010
55
00
1° 2° 3° 4° 1° 2° 3° 4° sodiumsodium
……. these results do not support current recommendations for routine reduction of sodium consumption, nor do they justify advice to increase salt intake or to decrease its concentration in the diet…..
Death Death (x1000 person years)(x1000 person years)
3030
2525
2020
1515
1010
55
00
1° 2° 3° 4° 1° 2° 3° 4° caloriescalories
2008: 23(9):1297–302
CV death