Embed Size (px)
Citation preview

Review
10.1586/14779072.4.1.59 © 2006 Future Drugs Ltd ISSN 1477-9072 59www.future-drugs.com
Imaging techniques in cardiac electrophysiologyMichael S Panutich and Bradley P Knight†
†Author for correspondenceUniversity of Chicago, 5758 S Maryland Ave.,MC9024, Chicago, IL 60637, USATel.: +1 773 702 5988Fax: +1 773 702 [email protected]
KEYWORDS: ablation, arrhythmias, computed tomography, echocardiography, electrophysiology, fluoroscopy, imaging, infrared, magnetic resonance imaging, mapping
Modern cardiac electrophysiology procedures include catheter-based arrhythmia ablation and transvenous device implantation, which are highly dependent on accurate, real-time cardiac imaging. With the realization that anatomic structures are critical to successful electrophysiologic procedures, accurately defining a patient’s cardiac anatomy has become more important. Fluoroscopy allows for 2D imaging of cardiac structures in real-time, and is used to guide catheter and lead placement, but does not allow for visualization of soft tissues. Intracardiac echocardiography allows for both direct visualization of anatomic structures within the heart and real-time imaging during catheter placement. Despite advances in intracardiac echocardiography catheters that allow for larger windows, the ability to accurately delineate anatomic structures depends on the patient’s anatomy and operator experience. Neither of these techniques allows for electrical mapping of the heart; however, both anatomic and electrical intracardiac mapping can be achieved with advanced mapping systems. These systems allow for real-time catheter localization, help elucidate cardiac anatomy, evaluate electrical activation during arrhythmias and guide catheter placement for deliverance of radiofrequency current. More recently, 3D cardiac computed tomography has been used to accurately define intracardiac anatomy; however, catheter tracking and electrical mapping cannot be performed by computed tomography. Mapping systems are now being merged with computed tomography images to produce an accurate anatomic and electrical map of the heart to guide catheter ablations. The objective of this paper is to describe the current imaging and mapping techniques used in electrophysiologic procedures.
Expert Rev. Cardiovasc. Ther. 4(1), 59–70 (2006)
Modern cardiac electrophysiology (EP) proce-dures include catheter-based arrhythmia abla-tion and transvenous device implantation.These procedures are highly dependent onaccurate, real-time cardiac imaging. Ablationprocedures are increasingly anatomically based.For example, it has been demonstrated that apurely anatomic approach can be successful forablation of the cavotricuspid isthmus for typicalatrial flutter [1]. Likewise, during device implan-tation, successful lead placement depends onreal-time imaging to guide advancement andmanipulation of the transvenous lead to theappropriate intracardiac location.
With the realization that anatomic structuresare critical to successful electrophysiologic pro-cedures, accurately defining a patient’s cardiac
anatomy has become more important. Fluoro-scopy allows for 2D imaging of cardiac struc-tures in real-time and is used to guide catheterplacement, but does not allow for soft tissuevisualization. Echocardiography also allows forreal-time imaging of the cardiac anatomy. Int-racardiac echocardiography (ICE), in particu-lar, allows for direct visualization of anatomicstructures within the heart and real-time imag-ing during catheter placement. However, theICE windows may not be able to accuratelydelineate anatomic structures in the left atrium(LA) from the right atrium. Neither of thesetechniques allow for electrical mapping of theheart. Both anatomic and electrical mappingof the heart can be achieved with advancedmapping systems, including electroanatomic
CONTENTS
Fluoroscopy
Transthoracic echocardiography
Transesophageal echocardiography
Advanced arrhythmia mapping systems
Computed tomography
Magneticresonance imaging
Infrared imaging
Expert commentary
Five-year view
Key issues
References
Website
Affiliations
For reprint orders, please contact [email protected]

Panutich & Knight
60 Expert Rev. Cardiovasc. Ther. 4(1), (2006)
mapping. These systems allow for real-time catheter localiza-tion and have helped elucidate cardiac anatomy, evaluate elec-trical activation during arrhythmias, and guide catheter place-ment for deliverance of radiofrequency (RF) current. Morerecently, 3D cardiac computed tomography (CT) has beenused to accurately define intracardiac anatomy; however, cath-eter tracking and electrical mapping cannot be performed byCT. Due to this, new cardiac mapping and imaging techniquesare being aggressively investigated. These mapping systems arenow being merged with CT images to produce an accurateanatomical and electrical map of the heart to guide catheterablations. The objective of this paper is to describe the currentimaging and mapping techniques used in electrophysiologicprocedures.
FluoroscopyFluoroscopy is the primary imaging modality in the EP lab,and provides an invaluable tool for real-time imaging of thepatient and the catheters. Fluoroscopy uses continuous x-raybeams that are directed at the patient. The x-rays that pene-trate through the patient strike a florescent plate that is linkedto an image intensifier. This process subtracts the x-rays thatare absorbed or deflected by structures in the patient’s bodyfrom the x-rays that strike the plate, thus producing an imagethat can be projected on a television screen. This produces areal-time x-ray image of the patient.
During catheter ablation procedures, fluoroscopy is used todirectly visualize catheter placement and manipulation. Upongaining vascular access, each catheter is advanced to an intracar-diac position under fluoroscopic guidance. After arrhythmiainduction and determination of the tachycardia mechanism,the tip of the ablation target is navigated to the ablation targetusing fluoroscopic guidance. Biplane fluoroscopy can be used,when available, to image from perpendicular views. The rightanterior oblique view allows the operator to have a long axisview of the right atrium and right ventricle, while the left ante-rior oblique view projects a short axis image from the apex ofthe heart extending cranially. With these two perpendicularviews available, the operator can reconstruct catheter placementthree-dimensionally.
Although catheter movement is guided with fluoroscopy, thepoor soft tissue resolution and 2D projections limit the accu-racy of catheter placement. Structures not easily seen on fluor-oscopy can be elucidated by contrast injections. During abla-tion for atrial fibrillation (AF), for example, it is routine toinject iodinated contrast in a retrograde fashion into each pul-monary vein (PV), which allows the operator to outline theanatomy of the venous drainage into the LA (FIGURE 1). Thisallows for more accurate catheter placement in and around thePVs. It also helps the operator to avoid ablating close to the PVostia, which can cause complications such as PV stenosis. How-ever, despite the use of contrast, fluoroscopy does not providedetailed anatomical information regarding the LA and PVs.Other imaging techniques, such as ICE and CT, are superiorimaging modalities for evaluating the LA and PV anatomy.
The posterior left atrial wall lies near the esophagus. Abla-tions in the posterior LA can cause damage to the esophagusand result in an atrial-esophageal fistula. A barium swallowallows the operator to visualize the esophagus in relation to theLA on fluoroscopy, and can help the operator avoid creatingdeep lesions over the esophagus (FIGURE 2). Despite the use ofcontrast and biplane fluoroscopic imaging, accurate catheterlocalization and catheter stability cannot be completely assuredwith fluoroscopy. This has led to the investigation of newerimaging techniques that can assist in catheter navigation duringablation procedures.
Fluoroscopy plays a vital role in imaging before, during andafter transvenous lead placement and extractions. A preoperativeupper extremity venogram can be performed under fluoroscopyin patients suspected to have a venous anomaly or stenosis. Dur-ing the procedure, upper extremity venograms may also be usedto help guide venous access by showing the venous anatomy inrelation to other bony structures. Once venous access is obtained,fluoroscopy is used to visualize, in real-time, the advancementand manipulation of the leads to appropriate positions. Contrastinjections into the coronary sinus under fluoroscopy help eluci-date the coronary sinus anatomy to aid appropriate placement ofleft ventricular leads. With active fixation leads, the deploymentof the helix can be visualized in real-time to ensure that it hasbeen fully deployed. At the end of device implantation, lead posi-tion is again confirmed with fluoroscopy. During lead extrac-tions, the advancement of the laser sheath over the lead is guidedusing fluoroscopy to ensure that the sheath is not advanced pastthe tip of the lead to avoid cardiac perforation.
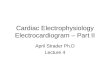
Figure 1. Pulmonary venogram performed under fluoroscopy during atrial fibrillation ablation. The catheters are located in the right atrium (RA), left common pulmonary vein ostium (LPV) and coronary sinus (CS). Contrast dye is being injected in a retrograde fashion into the LPV outlining the ostium (oval). Visualization of the ostium can be used as a guide for catheter placement and lesion formation during ablation ofatrial fibrillation.
CS
RA
LPV

Imaging techniques in cardiac electrophysiology
www.future-drugs.com 61
A major limitation of fluoroscopy is the risk it carries forboth the patient and healthcare professionals. The most com-mon injury to patients and health professionals from fluoro-scopy is skin and soft tissue injury (TABLE 1). Whether these inju-ries occur depends on multiple variables, such as cumulativedose of radiation, rate of delivery of radiation, the fractionationof the absorbed dose, age of the person receiving the radiationand the skin site exposed [101].
Fluoroscopy is a readily available and cost-effective real-timeimaging modality. The authors routinely use fluoroscopy in allprocedures in which imaging is needed to guide catheter orlead placement.
Transthoracic echocardiographyTransthoracic echocardiography (TTE) is a mainstay cardiacimaging modality in the evaluation of multiple disease proc-esses. It has roles in every aspect of cardiology including electro-physiology. Echocardiography is used mostly in diagnosis andevaluation of patients prior to procedures.
Patients who have any tachyarrhythmia should undergo tran-sthoracic echocardiography to evaluate for structural abnormali-ties of the heart that could predispose to arrhythmias. The TTEmay identify abnormalities, such as occult valvular disease,hypertrophic obstructive cardiomyopathy, congenital disease orpericardial disease, that need to be corrected or investigated fur-ther prior to any invasive eletrophysiologic procedure. Inpatients with AF, the LA volume and size can be determined byechocardiography. The presence of left atrial enlargementdecreases the probability of a patient to remain in sinus rhythmfollowing cardioversion [2,3]. In patients with ventricular tachy-
cardia, the echocardiogram can also identify left or right ven-tricular abnormalities, such as regional wall motion abnormali-ties, cardiomyopathies or infiltrative processes, that may requirefurther evaluation.
There is only a limited role for transthoracic echocardiogra-phy during EP procedures. It is cumbersome to perform theevaluation while maintaining a sterile field during procedures.Likewise, performing echocardiography during EP proceduresexposes the technician to radiation. After ablation procedures,echocardiography is useful when evaluating for complicationssuch as cardiac tamponade or valvular damage.
Transthoracic echocardiography is invaluable in the evaluationof patients for implantable cardioverter defibrillators (ICDs)and biventricular pacing. Patients with left ventricular dysfunc-tion may be candidates for ICD implantation for primary pre-vention of sudden cardiac death. The Sudden Cardiac death inHeart Failure (SCD-HeFT) trial showed an improved survivalin patients with an ejection fraction (EF) of 35% or less due toeither ischemic or nonischemic cardiomyopathy, who receivedan ICD for primary prevention of sudden cardiac death [4].Based on this, any patient with an EF of 35% or less should beconsidered for ICD placement.
The role for transthoracic echocardiography in the evaluationof heart failure patients who may be candidates for biventricularpacing is still being defined. In certain patients with New YorkHeart Association (NYHA) Class III or IV heart failure and ven-tricular dyssynchrony, cardiac resynchronization pacing therapy(CRT) has been demonstrated to improve heart failure symp-toms [5,6]. Recently, the Cardiac Resynchronization in Heart Fail-ure (CARE-HF) study showed, not only an improvement inquality of life, but also a mortality benefit with biventricular pac-ing in these patients [7]. Transthoracic echocardiography mayhave a role in determining candidates for resynchronization ther-apy with biventricular pacing. Both intra- and interventriculardyssynchrony can be diagnosed with transthoracic echocardiog-raphy, and may identify patients who may benefit from biven-tricular pacing regardless of their QRS duration [8]. Currently,there is no consensus on which echocardiographic markers bestdefine dyssynchrony and predict benefit from CRT. The ongoingPROSPECT trial is a multicenter prospective trial that willattempt to define which echocardiographic markers will predictbenefit from CRT [9]. Echocardiography can also be used postop-eratively to guide optimization of pacing intervals to maximizeventricular synchrony [10–12].
More recently, 3D transthoracic echocardiography (TTE) hasbeen demonstrated to be able to quantify the degree of ventriculardyssynchrony, evaluate resynchronization with CRT and predictresponders to CRT [13]. 3D echocardiography may play an impor-tant role in selecting patients for CRT and evaluating the responseto CRT in the future, but its role needs to be better defined.
Transesophageal echocardiographyTransesophageal echocardiography (TEE) overcomes some ofthe limitations of using TTE in the EP lab. It is less cumber-some around the sterile field during an EP procedure and
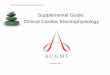
Figure 2. An esophagram performed during an atrial fibrillation ablation. Fluoroscopy image from the left anterior oblique view of a barium swallow with catheters in the right atrium (RA), left atrium (LA) and coronary sinus (CS). The course of the esophagus (E) posterior to the left atrial wall can be seen as the patient swallows barium. Creation of deep lesions during ablation should be avoided near the course of the esophagus to prevent damage to the esophagus or an atrial–esophageal fistula.
E
CS
RALA

Panutich & Knight
62 Expert Rev. Cardiovasc. Ther. 4(1), (2006)
allows for better imaging of intracardiac anatomy. It is also use-ful in the diagnosis of procedural complications. However,TEE requires esophageal intubation, which is uncomfortablefor the patient and carries a risk of esophageal perforation. Itmay require the patient to need higher levels of sedation or gen-eral anesthesia, both of which can increase the complicationrate of the procedure. Using TEE also exposes the healthcaretechnician to excess radiation from fluoroscopy.
TEE accurately identifies intra-atrial thrombi in patients withAF, with a sensitivity and specificity approaching 100% [14,15].
Left atrial appendage thrombi are seen in approximately 13% ofpatients who have been in AF for more than 3 days [16,17]. Cur-rent recommendations are that any patient who has been in AFor atrial flutter for greater than 48 h without adequate anticoagu-lation should undergo TEE to rule out an intracardiac thrombusprior to a cardioversion or ablation procedure.
Both congenital abnormalities and cardiac surgery can leadto anatomic obstacles to the ablation of arrhythmias. TEE canhelp identify areas where catheter placement and lesion forma-tion may be difficult prior to an ablation procedure. It can alsoidentify surgical baffles and patches that should be avoided. IfTEE is used during the ablation procedure, it can be a usefulto guide catheter placement and stability. However, intracar-diac echocardiography is the preferred ultrasound-based imag-ing modality during ablation procedures for guiding catheterplacement and lesion formation.
Intracardiac echocardiographyEchocardiography is a useful tool in the EP laboratory; how-ever, both TTE and TEE have significant limitations, as dis-cussed. ICE has overcome these limitations, and has proven tobe a useful adjunctive imaging modality in the EP lab.
There are two types of ICE transducers: mechanical andphased-array. The only commercially available mechanical ICEcatheter is 9 Fr and has a 4-cm radial imaging field [18]. This cath-eter has three major limitations: the radial imaging only allowsfor views within one plane (the horizontal plane), the catheterdoes not have doppler capabilities and the catheter tip is notdeflectable. The phased-array ICE catheters have doppler capa-bilities, a deflectable tip, and image in a longitudinal fashion witha 90° window that extends 2–12 cm deep [19,20]. Commerciallyavailable phased-array ICE catheters range in size from 8–10 Fr.
ICE has been used to guide trans-septal punctures foraccess to the LA [21,22]. ICE allows for imaging of the fossaovalis and for confirming needle placement prior to trans-septal puncture to reduce the risk of atrial or aortic perfora-tion. It can also identify unusual anatomy in the atria thatmay impact ablation strategies.
Fluoroscopy does not allow for assessment of endocardial anat-omy during ablation procedures due to its poor resolution of softtissue structures. Inability to identify anatomic irregularities canlead to technical limitations in the ablation of left atrial arrhyth-mias [23]. In treatment of AF, identification of the ostia of the PVsis critical. Pulmonary venograms under fluoroscopy often do notallow for accurate identification of the PV ostia. ICE does not
only accurately identify these structures, but can also be used toguide placement of ablation and mapping catheters in andaround the PVs [24].
In patients with congenital heart disease or previous surgery,ICE can help identify scar tissue, baffles or patches. Scar tissueand surgical baffles or patches will appear as regions of lowamplitude electrograms during intracardiac electrical mapping;however, only ICE will be able to differentiate scar tissue from asurgically placed patch or baffle. This is important, as scar tis-sue can be arrhythmogenic and is a potential target for ablation;however, surgically placed baffles and patches should beavoided [25]. Fluoroscopy also does not allow for accurate assess-ment of tissue contact by the catheter or of lesion creation [23].
ICE has demonstrated that significant catheter migration canoccur during ablation, despite apparent catheter stability onfluoroscopy [26]. Catheter instability leads to poor heating effi-ciency and lesion formation. The use of ICE during catheterablation improves both catheter stability and contact, as well aslesion size (FIGURE 3) [23,27]. Monitoring for stable catheterplacement and PV stenosis during PV isolation for AF withICE has been demonstrated to improve outcomes [28]. Temper-ature is often used to monitor energy delivery during ablation.However, this can be inaccurate in high-flow areas. ICE allowsfor the observation of lesion formation by detecting vaporiza-tion bubbles and tissue characteristics during RF energy deliv-ery [29]. Using these observations on ICE, lesions with fewergaps can be created, leading to more successful ablations of car-diac arrhythmias [30]. ICE also allows the operator to monitorcatheter localization. Multipolar catheters, such as circular PVmapping catheters, which appear to be at the PV ostium onfluoroscopy, can actually be 2–3 cm into the PV. ICE allows formore accurate placement of such catheters.
ICE has been used during catheter ablation of other atrialand ventricular arrhythmias. During atrial tachycardia, ICEhas been used to identify anatomic structures that are not seenon fluoroscopy, such as the crista terminalis, and to guidemapping in areas of interest [31,32]. Ablation of atrial flutter canbe difficult due to deep pockets and ridges in the area targetedfor ablation [33]. Delineation of these anatomical structures inthe area targeted for lesion formation can help guide ablationstrategies so that a line with no gaps can be created. In ven-tricular tachycardia ablations, ICE has been used to confirmstructural abnormalities that lead to reentry [30]. It may also beof benefit in assessing catheter stability and placement andlesion formation during ventricular tachycardia ablations [25].
ICE is useful in diagnosing intraprocedural complications.The overall incidence of stroke during RF ablation of AF hasbeen reported to be 1% [34], but may be as high as 5%, withadvanced age or prior thromboembolism being risk factors [35].
Thrombus formation has been reported to be visualized inapproximately 10% of cases. Directly visualizing thrombus oncatheters, sheaths and endocardial lesion sites using ICE maybe useful in preventing thromboembolism [26,36]. ICE may alsobe useful in diagnosing PV stenosis using doppler before andafter the procedure [37]. Finally, ICE allows for the prompt

Imaging techniques in cardiac electrophysiology
www.future-drugs.com 63
diagnosis of cardiac perforation and the development of tam-ponade. The ability to quickly diagnose procedural complica-tions may lead to more prompt treatment and better outcomeswhen complications occur.
In the authors’ laboratory, ICE is used in all procedures thatrequire trans-septal puncture to gain access to the LA from theRA. It is considered by the authors to be the best imaging modal-ity available to confirm, in real-time, needle placement at theintra-atrial septum. ICE is not routinely used to confirm catheterplacement or to diagnose procedure-related complications.
Advanced arrhythmia mapping systemsUsing fluoroscopy and intracardiac electrograms, an operatorcan mentally create a 3D activation map; however, this is notadequate in the complex arrhythmias encountered in the EP lab.Several advanced mapping systems have become available overthe past decade to display activation wavefronts on a 3D recon-struction of the intracardiac chamber of interest. Each systemuses different technology to generate the 3D image, record elec-trograms and localize the electrode catheter in space. These sys-tems each have their own advantages and disadvantages, but arehighly valuable during complex ablation procedures and havethe potential to significantly lower fluoroscopy exposure.
One advanced mapping system is referred to as an electro-anatomic mapping system. This system uses a magnetic field totriangulate the position of the ablation catheter and create ananatomical and electrical map. The magnetic field is created bya magnetic emitter located under the patient table. A patchwith three reference points is placed on the patient’s back.These create a 3D magnetic field in which the system canrecord and display, in real-time, the location of the catheter tip
relative to the reference points in the magnetic field. Once sev-eral points are taken at different locations, the system can createan accurate 3D image of the chamber.
At a given point, the location of the catheter tip and the elec-trogram recorded at that site are gated to a local activation pointrecorded from another reference catheter in a stable position(such as a catheter in the coronary sinus or right ventricularapex). At each point taken, the catheter stability, local activationtime, cycle length and 3D position of the catheter are recorded.Either during or after mapping, any points that appear unstablebased on these variables can be deleted. The gating produces apropagation map by comparing the local activation at one pointwith the local activation at the stable, reference catheter. Anypoint where no electrical activation can be recorded is labeled asscar tissue. The system then creates an electrical map by deter-mining the earliest to latest activation at each taken point inrelation to the activation of the reference catheter. The systemthen uses color to produce a propagation wave map from earliestactivation up to the latest in the chamber mapped. One majorlimitation of this system is that the points must be taken duringtachycardia, so the patient must have a sustained tachycardia inorder to produce an accurate electrical map. Thus, accurate elec-trical maps are difficult to create for patients with short bursts oftachycardia, polymorphic tachycardia or hemodynamicallyunstable tachycardia [38].
The electroanatomic system has been validated for anatomicand electrical accuracy in the atria, as well as theventricles [39–41]. It accurately identifies anatomical structures,such as scars, and allows for accurate creation of ablation linesin ventricular tachycardia and AF ablations [40–43]. This systemhas been demonstrated to decrease the fluoroscopy time when
Table 1. Radiation-induced skin injuries.
Skin injury Threshold absorbed dose (Gy*) Hours of fluoroscopy needed to reach threshold dose (at 0.02 Gy/min)‡
Time to onset of skin injury from a single radiation exposure
Transient erythema 2 1.7 Hours
Temporary epilation 3 2.5 3 weeks
Early erythema 6 5.0 10 days
Permanent epilation 7 5.8 3 weeks
Dry desquamation 10 8.3 4 weeks
Invasive fibrosis 10 8.3
Dermal atrophy 11 9.2 >14 weeks
Telangiectasis 12 10.0 >52 weeks
Moist desquamation 15 12.5 4 weeks
Late erythema 15 12.5 6–10 weeks
Dermal necrosis 18 15 >10 weeks
Ulceration 20 16.7 >6 weeks
*Gray (Gy) units are the international measurement of radiation. One Gy = 100 rad; ‡The absorbed dose of radiation from direct fluoroscopy typically ranges from 0.02–0.05 Gy/min, but may reach as high as 0.5 Gy/min. Table adopted from Food and Drug Administration information [101].

Panutich & Knight
64 Expert Rev. Cardiovasc. Ther. 4(1), (2006)
used in atrial flutter ablations [45]. One major advantage is thatrecently it has been upgraded to allow the map to be super-imposed on a CT reconstruction of the atrium. This mayimprove the accuracy of the anatomical reconstruction, catheterposition and lesion creation.
Another mapping system that can create both anatomicaland electrical maps of the cardiac chambers uses ultrasoundcrystals on intracardiac catheters to triangulate and localize theablation catheter tip. This system has been used to treat atrialand ventricular arrhythmias [45]. The reference catheters areplaced in stable orthogonal positions such as the coronary sinusand the right ventricular apex. Ultrasound pulses that are sentthrough the ablation and reference catheters are transmitted tothe transducers on the other catheters, creating a 3D space. Thesystem determines the time from transmission of the ultra-sound pulse from one catheter to when it is sensed on anothercatheter to triangulate the position of the ablation catheter inrelation to the reference catheters. By moving the catheter todifferent positions in the chamber, the system automaticallytakes anatomical points to create an anatomical map.
The ultrasound-based system can also create an electricalmap in a similar fashion to the electroanatomic system. At eachanatomical point taken, the system will also record an electro-gram. One benefit of this system is that it allows visualizationof the recorded electrogram along with the anatomical point atwhich it was taken. The timing of the local activation at eachpoint is compared with the activation times at other anatomiclocations allowing the system to create an electrical activationmap of the tachycardia.
A third advanced mapping system uses three high-frequencyradiowaves emitted from skin electrodes placed on the patientthat are sensed by a reference catheter to create a 3D field [46].
The system calculates the position of the ablation catheter inthis field by averaging the radio signals over a 1–2-s period toreduce cardiac cycle variation [38]. Although this can preciselylocalize catheter position to within 2 mm [47], it is unable toproduce an anatomical or electrical map of the atrium. It does,however, allow for important anatomical landmarks or ablationsites to be labeled on a 3D grid. Benefits of this system includethe reduction of fluoroscopy time and a lower cost than othermapping systems.
This radiowave technology has been incorporated into a plat-form that can also be used as a noncontact mapping system. Thenoncontact mapping system uses a balloon covered with a multie-lectrode array that is mounted in the end of a catheter and posi-tioned within the chamber of interest. The noncontact mappingsystem uses the intracavitary potentials recorded from the multi-electrode array to derive virtual endocardial electrograms. Theablation catheter is used to define the endocardial border and cre-ate a 3D reconstruction of the chamber on which the virtual elec-trograms are displayed. The advantage of the noncontact map-ping system is the ability to record a single beat of tachycardia andanalyze the wavefront offline during sinus rhythm. This can beparticularly useful during infrequent nonsustained arrhythmias orhemodynamically unstable ventricular tachycardia.
The authors routinely use electroanatomical mapping sys-tems merged with 3D CT images of the patient’s LA during AFablation procedures. They consider this, in combination withfluoroscopy, to allow for the most accurate assessment of cathe-ter placement outside of the PV currently available. These sys-tems allow anatomic and electrical areas of interest to bemarked so that these areas can be reassessed at a later time ifneeded. For complicated or atypical atrial flutter and supra-ventricular tachycardia ablations, an electroanatomic mappingsystem is used to aid in determining anatomic areas critical tothe tachycardia that may be targets for ablation, as well as toguide catheter placement in these areas. The authors do notbelieve that the advantages of these mapping systems justifytheir cost for use in typical atrial flutter, slow pathway andaccessory pathway ablations.
Computed tomographyThe success and safety of ablation procedures is partiallydependent on the operator’s understanding of intracardiacanatomy. Only 70% of patients undergoing AF ablation have‘traditional’ anatomy, with four PVs each having an individualostium, while the other 30% have various anatomicalvariants [48]. Although anatomic points can be marked andlabeled with many imaging systems, the true anatomy of theatria can not be accurately evaluated with these techniques. Theadvent of multidimensional computed tomography (MDCT)now allows for an accurate, 3D reconstruction of the LA andfor PVs to be created [49,50]. These accurate reconstructionsallow the electrophysiologist to evaluate atrial and PV anatomybefore the procedure. Recently, these 3D images have beenmerged with other advanced mapping systems to produce anaccurate anatomic and activation map that allows for real-timecatheter tracking within the atrium.
Prior to the advent of MDCT, the pulmonary venous anat-omy during left atrial ablation was defined using pulmonaryvenograms by fluoroscopy [51] and ICE. Pulmonary venogramsdo not provide accurate information regarding the anatomy ofthe vein and the venous–atrial connection. ICE visualizes thelocation of the PVs, delineates the pulmonary venous anatomyand accurately measures ostial size [51]. Despite advances in ICEcatheters that allow for larger windows, the ability to accuratelydelineate anatomic structures, such as the distal PVs and atrialwall, depends on the patient’s anatomy and operator experience.Imaging of these structures with ICE can be extremely difficultin patients with a dilated LA [52]. ICE has been compared withMDCT in patients undergoing AF ablations using MDCT asthe gold standard. MDCT had a higher sensitivity for detectingadditional pulmonary venous branches and suggested that ICEunderestimated the size of the PV ostia [53].
Prior to ablation procedures, the location, length and numberof PV ostia and branches help guide ablation techniques. MDCTcan accurately define the PV ostium at the junction with the LA,pulmonary venous branch points and the saddle of left atrial tis-sue inbetween the ipsilateral pulmonary venous ostia [52]. Themost common anomalies found include ipsilateral single PV

Imaging techniques in cardiac electrophysiology
www.future-drugs.com 65
ostium, accessory PVs and early branching (≤5 mm from theostium of the main PV). Single PV drainage into the LA mostoften occurs on the left side. The common ostia are generallylarger than individual pulmonary venous ostia, and the myocar-dial sleeve around the common ostia is circumferential. Due tothis, segmental PV isolation is rarely feasible in these patients [54].
Accessory PVs are more commonly found on the right side.Accessory veins usually drain a pulmonary lobe directly into theLA with the right middle and right lower lobes most commonlyhaving accessory venous drainage [55]. The ostia of these accessoryveins are often much smaller than those of the true PVs [55]; thus,they are at a higher risk for developing stenosis following an abla-tion procedure. When an accessory vein is located between theupper and lower PVs, it may be difficult to deliver RF lesionsbetween the upper and lower PVs due to the small amount ofatrial tissue between the three ostia [54]. Unstable catheter positionon a small isthmus of atrial tissue can lead to delivering lesions inthe PV, thus increasing the risk for PV stenosis. Accessory veinsmay also drain into different locations in the LA. If this is notknown prior to the ablation procedure, the accessory vein may bemissed and not isolated with the lesions delivered. Early branch-ing of the PV may place the branch close to the left atrial wall.Ablation of the atrial wall at these sites can lead to damage to thePV branch and stenosis, or occlusion of that branch [54].
MDCT can also be used to evaluate the presence of a left atrialthrombus and the proximity and course of the esophagus in rela-tion to the LA, prior to undergoing catheter ablation. TEE isconsidered the gold standard to visualize the LA and the left atrialappendage (LAA) for thrombus formation. In a small head-to-head comparison, MDCT reconstruction of the LA and LAAidentified all patients in whom an LA and LAA thrombus wasobserved on TEE. There were also no thrombi falsely identifiedby the MDCT [56]. More studies are needed to determine theaccuracy of MDCT in identifying LA and LAA thrombi beforethis can be routine practice.
Due to the proximity of the esophagus to the LA, RF lesionsdelivered in the LA over the esophagus can lead to atrio-esophageal fistula formation [57–60]. The relationship of theesophagus to the LA and the thickness of the LA wall overlyingthe esophagus have been described by means of MDCT [61].
Incorporation of esophageal and left atrial imaging into a cath-eter navigation system may help avoid creating lesions in areaswhere there is a higher chance of causing esophageal injury.However, during ablation procedures, the esophagus canmigrate to different positions [62]. Therefore, still images such asesophagram by fluoroscopy or MDCT may be of little benefitin preventing damage to the esophagus. Real-time imaging ofthe esophagus during the ablation procedure may be necessaryto avoid creating lesions in high-risk areas [61].
Now that the LA can be reconstructed using MDCT, combin-ing an accurate 3D, anatomic MDCT image with electrical map-ping and catheter tracking from the available systems may allowfor more precise catheter tracking and lesion formation withinthe LA (FIGURE 4). This approach has been validated in humansand animals, and catheter position accuracy and lesion formation
to within 2 mm [63]. In order for accurate registration of the twoimages, the patient must be in the same rhythm at the time ofMDCT and intracardiac mapping [63]. In one case report,MDCT was used to delineate LV scar tissue and to guide theablation of recurrent ventricular tachycardia originating from theLV [64]. The incorporation of MDCT images and cardiac map-ping may improve the accuracy, safety and outcomes of catheterablation for AF, as well as other cardiac arrhythmias.
MDCT can diagnose complications of ablation proceduressuch as PV stenosis, dissection and perforation. When segmentalPV ostial ablations are performed, the ostial diameter narrows byan average of 1.5 mm, and a 28–61% focal stenosis occurs within7.6 mm from the ostium in 3% of cases [50]. Pulmonary vein ste-nosis can lead to pulmonary edema, pulmonary venous infarc-tion or pulmonary veno-occlusive disease with pulmonaryhypertension [55]. Pulmonary vein stenosis should be suspected inany patient who underwent an ablation procedure who presentswith shortness of breath, chronic cough, or hemoptysis. Mag-netic resonance imaging (MRI) has also been used to accuratelyevaluate for PV stenosis [65]. Despite the benefits of no radiationexposure to the patient and no nephrotoxic contrast, MDCT isthe preferred imaging modality due to a better special resolutionand a very short acquisition time [66]. MRI is an alternativemodality that can be used if a patient has a contraindication tocontrast dye used in MDCT.
Magnetic resonance imagingCardiac MRI is becoming a popular and useful imaging tech-nique for evaluation and diagnosis of many cardiac diseases.Advantages of this imaging modality over MDCT include noradiation and nephrotoxic contrast dye exposure for thepatient, while still giving high-resolution 3D images. Dis-advantages include long scanning times, which increases thechance for artifact in the images, and risks to patients with
Figure 3. Intracardiac echocardiography (ICE) during atrial flutter ablation. Long axis ICE image of the right atrium (RA), tricuspid valve (TV), and right ventricle (RV) that shows an ablation catheter (A) positioned at the posterolateral aspect of the tricuspid valve annulus just anterior to the cavotricuspid isthmus (CTI) during an ablation procedure for atrial flutter.
RA
A
CTI TV
RV

Panutich & Knight
66 Expert Rev. Cardiovasc. Ther. 4(1), (2006)
pacemakers or defibrillators. MRI has long been known as anaccurate imaging modality to evaluate the PV system. It hasalso been demonstrated to be superior to TEE in evaluatingthe PVs [65]. Due to this, MRI is an excellent modality forevaluation of the PVs prior to ablation procedures and evalu-ating for PV stenosis after ablation procedures [67,68]. 3D MRIreconstructions of the left ventricle have been incorporatedinto mapping systems to accurately guide lesionformation [69]. This suggests that it may be possible to mergeMRI reconstructions of the LA and PVs into a mapping sys-tem to guide catheter ablations of AF; however, more studiesare needed to validate this concept.
Myocardial viability can be assessed by contrast-enhancedMRI. Enhancement of myocardium more than 10 min aftercontrast injection (delayed hyperenhancement [DHE]) indicatesmyocardial necrosis or scar tissue. After an acute myocardial inf-arction (MI), the presence of DHE indicates myocardial necrosis;however, DHE in patients with chronic coronary artery diseaseallows for identification of nonviable scar tissue [70]. MRI alsoallows for accurate localization and assessment of extent of non-viable scar tissue [71]. Due to this, MRI has promise for evaluatingthe myocardium for scar tissue that could be arrhythmogenic andact as a ‘road map’ to guide ablation procedures. In order to beable to use MRI in this fashion, a 3D-constructed image of theheart would need to be able to be incorporated into a mappingsystem so that catheter movement and lesion locations could befollowed in a real-time fashion. Preprocedure 3D MRI of the leftventricle has been integrated into the mapping system in a por-cine model to guide lesion formation. In this model, catheterscould be accurately navigated to the mitral valve annulus and scar
tissue. Lesions were found to be within 1.8 mm of the intendedtargets [69]. This suggests that preprocedure MRI may be a usefulimaging modality to help guide catheter ablations; however,more experience is needed.
Infrared imagingAlthough the current imaging techniques are effective, noneallow for direct visualization of cardiac anatomy, catheter posi-tion or lead placement. Real-time, direct imaging may decreaseprocedure time and help avoid possible complications of leadplacement and catheter ablations. Direct fiberoptic imaging hasbeen achieved within the heart, but requires displacement of theblood to view structures. Imaging using infrared light allows fordirect visualization of endocardial structures through movingblood because the wavelength of infrared light is greater than theoptical diameter of a red blood cell. One recent study evaluatedthe feasibility of direct visualization of cardiac structuresthrough infrared endoscopy during coronary sinus lead place-ment in dogs [72]. In this study, the infrared endoscope wasadvanced into the right atrium of 10 dogs. Once placed, differ-ent right atrial structures were identified when the catheter waswithin 1–2 cm of each structure. These included the inferiorvena cava ostium, tricuspid valve, Eustachian ridge, coronarysinus ostium, and branches of the coronary sinus. The trabecu-lated lateral wall of the right atrium could also be distinguishedfrom the smooth-walled atrial septum.
Infrared imaging may also be used for direct visualization ofthe electrode–endocardial interface during catheter ablations.An animal study has recently demonstrated feasibility of thismodality [73]. Infrared imaging may improve the ability totitrate RF energy delivery to the desired effect, and improvethe safety and efficacy of ablation procedures. However, moreresearch is needed. A single catheter that can be used for bothablation and imaging would be a useful addition to the EPlaboratory tool set.
Expert commentaryImaging has become increasingly important in the EP lab asprocedures have become more complex and dependent onaccurate anatomic definition. Although it is difficult to demon-strate an improvement in success or a reduction in complica-tions as a result of the use of more imaging, these additionalimaging tools have greatly improved our understanding of theanatomy related to the procedures and have likely improvedsafety and accuracy in the EP lab.
Standard fluoroscopy remains the standard imaging modalityduring device implantation and catheter ablation procedures.Contrast venography is useful during central venous access, andto image the coronary sinus and pulmonary veins. The authors’laboratory routinely uses phased-array ICE during all transeptalcatheterizations and to image the LA during ablation proce-dures for AF. The rotational ICE system is occassionally usedfor transeptal catheterization when ICE is not needed for theremainder of the ablation procedure, because the rotationalICE catheters are less expensive than the phased-array ICE
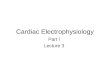
Figure 4. Three-dimensional computed tomography image of the left atrium merged with an electroanatomic mapping system. Right lateral view of the left atrium is shown displaying ablation lesions around the pulmonary vein pairs (red dots) and the course of the esophagus (pink dots) adjacent to the posterior wall of the left atrium.
1-LAAFIB > 207 points
1.13 cm
LA1
2
LAT2
1

Imaging techniques in cardiac electrophysiology
www.future-drugs.com 67
catheters. Preoperative CT imaging of the LA and pulmonaryveins are performed before catheter ablation for AF and theimages are imported and merged into the 3D electroanatomicmapping system.
Five-year viewThe ideal imaging tool for use during EP procedures should haveat least the following characteristics: highly accurate, minimallyinvasive, real-time, 3D, compatible with standard EP equipmentand not associated with harmful radiation. The electrophysiolo-gist should be able to easily manipulate the images during inter-ventions at the bedside to adjust the gain, image quality, viewingangle and depth of penetration. Adjustments should be possiblethat allow the operator to obtain a near-field image that permitshigh-resolution structural detail, as well as a more global imagethat permits orientation. The technology should be able to per-mit intracardiac imaging during transvenous lead placement,guide transeptal catheterization and image the electrode–tissueinterface during cardiac ablation procedures.
Fluoroscopy is an inexpensive and convenient real-time imag-ing modality that will continue to play a pivotal role duringelectrophysiology procedures. It is unlikely that this imaging
modality will be completely phased out by newer technologiessuch as ultrasound, CT or MRI over the next 5 years. How-ever, as newer real-time imaging techniques are improved,they should ultimately replace fluoroscopy. There are manyforces driving the increased use of nonfluoroscopic imaging inthe EP lab. One is that ablation techniques are increasinglyanatomically based. Another is the increased familiarity withthe tools by trainees who continue to rely on the tools aftertheir training.
The authors not only expect improvements in current imag-ing technologies, but also the development of new technolo-gies. Infrared imaging is an example of a new imaging tool thatmay have direct applications in the EP lab. This method usesinfrared technology to permit real-time imaging throughblood of intracardiac structures, such as the coronary sinus andintra-atrial septum, and the electrode–endocardial interface.The hardware currently used in the EP lab will also evolve tobetter take advantage of the imaging tools. Examples includethe development of a transparent ablation electrode that wouldpermit imaging directly through the tip of an ablation catheterand implantable leads and ablation catheters that are compatiblewith MRI.
ReferencesPapers of special note have been highlighted as:• of interest•• of considerable interest
1 Hiroshi T, Oral H, Ozaydin M et al. Randomized comparison of anatomic and electrogram mapping approaches to ablation of typical atrial flutter. J. Cardiovasc. Electrophysiol. 13, 662 (2002).
2 Brodsky MA, Allen BJ, Capparelli EV, Luckett C, Morton R, Henry WL. Factors determining maintenance of sinus rhythm after chronic atrial fibrillation with left atrial dilatation. Am. J. Cardiol. 63(15), 1065–1068 (1989).
3 Dittrich HC, Erickson JS, Schneiderman T, Blacky AR, Savides T, Nicod PH. Echocardiographic and clinical predictors for
outcome of elective cardioversion of atrial fibrillation. Am. J. Cardiol. 63(3), 193–197 (1989).
4 Moss AJ, Zareba W, Hall WJ et al. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N. Engl. J. Med. 346, 877–883 (2002).
Key issues
• Modern cardiac electrophysiology procedures include catheter-based arrhythmia ablation and transvenous device implantation, which are highly dependent on accurate, real-time cardiac imaging.
• Fluoroscopy allows for 2D imaging of cardiac structures in real-time and is used to guide catheter and lead placement, but it does not allow for visualization of soft tissues.
• Intracardiac echocardiography (ICE) allows for direct visualization of anatomic structures within the heart, and for real-time imaging during catheter placement. Despite advances in ICE catheters that allow for larger windows, the ability to accurately delineate anatomical structures depends on the patient’s anatomy and operator experience.
• Both anatomical and electrical intracardiac mapping can be achieved with advanced mapping systems that allow for real-time catheter localization, help elucidate cardiac anatomy, evaluate electrical activation during arrhythmias and guide catheter placement for deliverance of radiofrequency current.
• 3D cardiac computed tomography (CT) has been used to accurately define intracardiac anatomy; however, CT cannot track catheters nor perform electrical mapping.
• Mapping systems are now being merged with CT images to produce an accurate anatomical and electrical map of the heart to guide catheter ablations.
• Newer imaging techniques, such as infrared imaging, are being studied and show promise for allowing for direct visualization of intracardiac anatomy and catheter placement.

Panutich & Knight
68 Expert Rev. Cardiovasc. Ther. 4(1), (2006)
5 Cazeau S, Leclercq C, Lavergne T et al., for the MUSTIC study group. Effects of multisite biventricular pacing in patients with heart failure and intraventricular conduction delay. N. Engl. J. Med. 344, 873–880 (2001).
6 Abraham WT, Fischer WG, Smith AL et al., for the MIRACLE study group. Cardiac resynchronization in chronic heart failure. N. Engl. J. Med. 346, 1845–1853 (2002).
7 Cleland JG, Daubert JC, Erdmann E et al. Cardiac Resynchronization -Heart Failure (CARE-HF) Study Investigators. The effect of cardiac resynchronization on morbidity and mortality in heart failure. N. Engl. J. Med. 352(15), 1539–1549 (2005).
8 Pitzalis MV, Iacoviello M, Romito R et al. Ventricular asynchrony predicts a better outcome in patients with chronic heart failure receiving cardiac resynchronization therapy. J. Am. Coll. Cardiol. 45(1), 65–69 (2005).
9 Yu, Cheuk-Man, Abraham et al. For the PROSPECT investigators. Predictors of response to cardiac resynchronization therapy (PROSPECT)-study design. Am. Heart J. 149(4), 600–605 (2005).
10 Verbeek XA, Auricchio A, Yu Y et al. Tailoring cardiac resynchronization therapy using interventricular asynchrony. Validation of a simple model. Am. J. Physiol. Heart Circ. Physiol. (Epub ahead of print, Sept 19) (2005).
11 Pitzalis MV, Iacoviello M, Romito R et al. Cardiac resynchronization therapy tailored by echocardiographic evaluation of ventricular asynchrony. J. Am. Coll. Cardiol. 40, 1615–1622 (2005).
• Showed that dyssynchrony on echo predicts long-term, clinical improvement in patients with Class III chronic heart failure (CHF) and left bundle-branch block.
12 Knebel F, Reibis R, Bondke H et al. Tissue Doppler echocardiography and biventricular pacing in heart failure: Patient selection, procedural guidance, follow-up, quantification of success. Cardiovasc. Ultrasound. 2, 17 (2004).
13 Hong TE, Sugeng L, Weinert L, Mor-Avi V, Desai AD, Knight BP. Real-time three-dimensional echocardiographic index of ventricular dyssynchrony indentifies long-term responders to cardiac resynchronization therapy. J. Am. Coll. Cardiol. 45(3) S1, 264A (2005).
14 Manning WJ, Weintraub RM, Waksmonski CA et al. Accuracy of transesophageal echocardiography for identifying left atrial thrombi. A prospective, intraoperative study Ann. Intern. Med. 123(11), 817–822 (1995).
• Demonstrated that transesophageal echo identifies left atrial thrombi with a sensitivity of 100% and a specificity of 99%.
15 Hwang JJ, Chen JJ, Lin SC et al. Diagnostic accuracy of transesophageal echocardiography for detecting left atrial thrombi in patients with rheumatic heart disease having undergone mitral valve operations. Am. J. Cardiol. 72(9), 677–681 (1993).
16 Manning WJ, Silverman DI, Keighley CS, Oettgen P, Douglas PS. Transesophageal echocardiographically facilitated early cardioversion from atrial fibrillation using short-term anticoagulation: final results of a prospective 4.5-year study. J. Am. Coll. Cardiol. 25(6), 1354–1361 (1995).
17 Klein AL, Grimm RA, Murray RD et al. Use of transesophageal echocardiography to guide cardioversion in patients with atrial fibrillation. N. Engl. J. Med. 344(19), 1411–1420 (2001).
18 Chu E, Fitzpatrick AP, Chin MC, Sudhir K, Yock PG, Lesh MD. Radiofrequency catheter ablation guided by intracardiac echocardiography. Circulation 89, 1301–5 (1994).
•• Demonstrated that intracardiac echo can accurately guide catheter localization identify intracardiac anatomy, and guide ablation of right atrial arrhythmias.
19 Bruce CJ, Packer DP, Seward JB. Intracardiac Doppler hemodynamics and flow: New vector phased array ultrasound tipped catheter. Am. J. Cardiol. 83, 1509–1512 (1999).
20 Bruce CJ, Nishimura RA, Rihal CS et al. Intracardiac echocardiography in the interventional catheterization laboratory: Preliminary experience with a novel, phased-array transducer. Am. J. Cardiol. 89, 635–640 (2002).
21 Epstein L, Smith T, TenHoff H. Nonfluoroscopic trans-septal catheterization: safety and efficacy of intracardiac echocardiographic guidance. J. Cardiovasc. Electrophysiol. 9, 625–630 (1998).
22 Daoud E, Kalbfleisch S, Hummel J. Intracardiac echocardiography to guide trans-septal left heart catheterization for radiofrequency catheter ablation. J. Cardiovasc. Electrophysiol. 10, 358–363 (1999).
23 Epstein L, Mitchell M, Smith T, Haines D. Comparative study of fluoroscopy and intracardiac echocardiographic guidance for the creation of linear atrial lesions. Circulation 98, 1796–1801 (1998).
24 Mangrum JM, Mounsey JP, Kok LC, DiMarco JP, Haines DE. Intracardiac echocardiography-guided, anatomically based radiofrequency ablation of focal atrial fibrillation originating from pulmonary veins. J. Am. Coll. Cardiol. 39, 1964–1972 (2002).
•• Showed that intracardiac echo can accurately identify anatomical structures, guide catheter localization and guide radiofrequency (RF) ablation to isolatethe pulmonary veins for treatment ofatrial fibrillation.
25 Bruce CJ, Freidman PA. Intracardiac echocardiography. Eur. J. Echocardiography 2, 234–244 (2001).
26 Chu E, Kalman JM, Kwasman MA et al. Intracardiac echocardiography during radiofrequency catheter ablation of cardiac arrhythmias in humans. J. Am. Coll. Cardiol. 24, 1351–1357 (1994).
27 Kalman JM, Fitzpatrick AP, Olgin JE et al. Biophysical characteristics of radiofrequency lesion formation in vivo: Dynamics of catheter tip-tissue contact evaluated by intracardiac echocardiography. Am. Heart J. 133, 8–18 (1997).
28 Marrouche NF, Martin DO, Wazni O et al. Phased-array intracardiac echocardiography monitoring during pulmonary vein isolation in patients with atrial fibrillation: impact on outcome and complications. Circulation 107, 2710–2716 (2003).
29 Roman-Gonzalez J, Asirvatham S. Razavi M et al. Marked discrepancies between catheter tip temperature registration and pulmonary vein tissue changes during ablation of focal atrial fibrillation in patients. PACE 24, 656 (2001).
30 Razavi M, Asirvatham S, Roman-Gonzalez J, Monahan K, Packer D. Phased-array ultrasound guidance of substrate-mediated ventricular tachycardia in patients with underlying heart disease. PACE 24, 543 (2001).
31 Kalman JM, Olgin J, Karch M, Hamdan M, Lee R, Lesh M. Crista tachycardias: origin of right atrial tachycardias from the crista terminalis identified by intracardiac echocardiography. J. Am. Coll. Cardiol. 31, 451–459 (1998).
• Used intracardiac echo to show that many right atrial tachycardias arise from the crista terminalis.
32 Kalman JM, Olgin JE, Karch MR, Lesh MD. Use of intracardiac echocardiography in interventional electrophysiology. Pacing Clin. Electrophysiol. 20, 2248–2262 (1997).
33 Cabrera J, Sanchez-Quintana D, Ho S, Medina A, Anderson R. The architecture of the atrial musculature between the orifice of the inferior caval vein and the tricuspid valve: the anatomy of the isthmus. J. Cardiovasc. Electrophysiol. 9, 1186–1195 (1998).
34 Ellenbogen KA, Wood MA. Ablation of atrial fibrillation: Awaiting the new paradigm. J. Am. Coll. Cardiol. 42, 198–200 (2003).

Imaging techniques in cardiac electrophysiology
www.future-drugs.com 69
35 Kok LC, Mangrum JM, Haines DE, Mounsey JP. Cerebrovascular complication associated with pulmonary vein ablation. J. Cardiovasc. Electrophysiol. 13, 764–767 (2002).
36 Ren JF, Marchlinski FE, Callans DJ. Left atrial thrombus associated with ablation for atrial fibrillation: identification with intracardiac echocardiography. J. Am. Coll. Cardiol. 43(10), 1861–1867 (2004).
• Demonstrated that left atrial thrombi formation can be detected with intracardiac echo, and that the thrombi can be withdrawn into the righ atrium under ICE guidancewithout complications.
37 Morton J, Byne M, Power J, Mow C, Kalman J. Phased array intracardiac echocardiography to guide radiofrequency ablation at the pulmonary vein ostium. PACE 24, 626 (2001).
38 Markides V, Segal OR, Tondato F, Peters NS. Mapping. In: Cardiac Electrophysiology. From Cell to Bedside. Zipes DP, Jalife J (Ed.). Saunders Publishing, PA, USA. 858–866 (2004).
39 Gepstein L, Hayam G, Ben-Haim SA. A novel method for nonfluroscopic catheter-based electroanatomical mapping of the heart. In vitro and in vivo accuracy results. Circulation 95, 1611–1622 (1997).
40 Stevenson WG, Delacretaz E, Friedman PL, Ellison KE et al. Indetification and ablation of macroreentrant ventricular tachycardia with the CARTO electroanatomical mapping system. Pacing Clin. Electrophysiol. 21, 1448–1456 (1998).
41 Marchlinski FE, Callans DJ, Gottlieb CD, Zado E. Linear ablation lesions for control of unmappable ventricular tachycardia in patients with ischemic and nonischemic cardiomyopathy. Circulation 101, 1288–1296 (2000).
42 Pappone C, Oreto G, Lamberti F et al. Catheter ablation of paroxysmal atrial fibrillation using a 3D mapping system Circulation 100, 1203–1208 (1999).
•• First to use a 3D mapping system toguide RF ablation of atrial fibrillation.
43 Pappone C, Rosanio S, Oreto G et al. Circumferential radiofrequency ablation of pulmonary vein ostia: A new anatomical approach for curing atrial fibrillation. Circulation 102, 2619–2628 (2000).
44 Kottkamp H, Hügl B, Krauss B et al. Electromagnetic versus fluoroscopic mapping of the inferior isthmus for ablation of typical atrial flutter: a prospective randomized study. Circulation 102, 2082–2086 (2000).
45 Schreieck J, Ndrepepa G, Zrenner B et al. Radiofrequency ablation of cardiac arrhythmias using three-dimensional real-time position management and mapping system. Pacing Clin. Electrophysiol. 25, 1699–1707 (2002).
46 Kirchhof P, Loh P, Eckardt L et al. A novel nonfluoroscopic catheter visualization system (LocaLisa) to reduce radiation exposure during catheter ablation of supraventricular tachycardias. Am. J. Cardiol. 90(3), 340–343 (2002).
47 Wittkampf FH, Wever EF, Derksenet R et al. LocaLisa: New technique for real-time 3-dimensional localization of regular intracardiac electrodes. Circulation 99, 1312–1317 (1999).
48 Ghaye B, Szapiro D, Dacher JN et al. Percutaneous ablation for atrial fibrillation: the role of cross-sectional imaging. Radiographics. 23, S19–S33 (2003).
49 Schwartzman D, Lacomis J, Wiggintonet WG. Characterization of left atrium and distal pulmonary vein morphology using multidimensional computed tomography J. Am. Coll. Cardiol. 41(8), 1349–1357 (2003).
50 Scharf C, Sneider M, Case I et al. Anatomy of the pulmonary veins in patients with atrial fibrillation and effects of segmental ostial ablation analyzed by computed tomography. J. Cardiovasc. Electrophysiol. 14, 150–155 (2003).
51 Wood MA, Wittkamp M, Henry D et al. A comparison of pulmonary vein ostial anatomy by computerized tomography, echocardiography, and venography in patients with atrial fibrillation having radiofrequency catheter ablation. Am. J. Cardiol. 93(1), 49–53 (2004).
52 Lacomis JM, Wigginton W, Fuhrman C, Schwartzman D, Armfield DR, Pealer KM. Multidector CT of the left atrium and pulmonary veins before radio-frequency catheter ablation for atrial fibrillation. Radiographics 23, S35–S50 (2003).
53 Jongbloed MR, Bax JJ, Lamb HJ et al. Multislice computed tomography versus intracardiac echocardiography to evaluate the pulmonary veins before radiofrequency catheter ablation of atrial fibrillation: A head to head comparison. J. Am. Coll. Cardiol. 45(3), 343–350 (2005).
54 Mansour M, Holmvang G, Ruskin J. Role of imaging techniques in preparation for catheter ablation of atrial fibrillation. J. Cardiovasc. Electrophysiol. 15, 1107–1108 (2004).
55 Stanford W, Breen J. CT evaluation of left atrial pulmonary venous anatomy. Int. J. Cardiovas. Imag. 21, 133–139 (2005).
56 Jaber WA, White RD, Kuzmiak SA et al. Comparison of ability to identify left atrial thrombus by three-dimensional tomography versus transesophageal echocardiography in patients with atrial fibrillation. Am. J. Cardiol. 93(4), 486–489 (2004).
57 Scanavacca MI, D’Ávila A, Parga J, Sosa E. Left atrial-esophageal fistula following radiofrequency catheter ablation of atrial fibrillation. J. Cardiovasc. Electrophysiol. 15, 960–962 (2004).
58 Pappone C, Oral H, Santinelliet V et al. Atrio-esophageal fistula as a complication of percutaneous transcatheter ablation for atrial fibrillation. Circulation 109, 2724–2726 (2004).
59 Benussi S, Nascimbene S, Calvi S, Alfieriet O. A tailored anatomical approach to prevent complications during left atrial ablation. Ann. Thorac. Surg. 75(6), 1979–1981 (2003).
60 Cummings JE, Schweikert RA, Saliba WI et al. Assessment of temperature, proximity, and course of the esophagus during radiofrequency ablation within the left atrium. Circulation 112, 459–464 (2005).
61 Lemola K, Sneider M, Desjardinset B et al. Computed tomographic analysis of the anatomy of the left atrium and the esophagus: implications for left atrial catheter ablation. Circulation 110, 3655–3660 (2004).
62 Han J, Good E, Morady F, Oral H. Esophageal migration during left atrial catheter ablation for atrial fibrillation. Circulation 110, e528 (2004).
63 Sra J, Krum D, Hare J et al. Feasibility and validation of registration of three-dimensional left atrial models derived from computed tomography with a noncontact mapping system. Heart Rhythm 2(1), 55–63 (2005).
64 Bello D Kipper S, Valderrabano M, Shivkumar K. Catheter ablation of ventricular tachycardia guided by contrast-enhanced cardiac computed tomography. Heart Rhythm 4, 490–492 (2004).
65 Masui T, Seelos KC, Kersting-Sommerhoff BA, Higgins CB. Abnormalities of the pulmonary veins: evaluation with MR imaging and comparison with cardiac angiography and echocardiography. Radiology 181, 645–649 (1991).
66 Funabashi N, Yonezawa M, Iesaka Y et al. Complications of pulmonary vein isolation by catheter ablation evaluated by ECG-gated multislice computed tomography. Heart Vessels 18, 220–223 (2003).
67 Yang M, Akbari H, Reddy G, Higgins C. Identification of pulmonary vein stenosis after radiofrequency ablation for atrial fibrillation using MRI. J. Comput. Assist. Tomogr. 25(1), 34–35 (2001).

Panutich & Knight
70 Expert Rev. Cardiovasc. Ther. 4(1), (2006)
68 Dill T, Neumann T, Ekinci O et al. Pulmonary vein diameter reduction after radiofrequency catheter ablation for paroxysmal atrial fibrillation evaluated by contrast-enhanced three-dimensional magnetic resonance imaging. Circulation 107, 845–850 (2003).
69 Reddy VY, Malchano ZJ, Holmvang G et al. Integration of cardiac magnetic resonance imaging with three-dimensional electroanatomic mapping to guide left ventricular catheter manipulation. J. Am. Coll. Cardiol. 44, 2202–2213 (2004).
70 Rehwald WG, Fieno DS, Chen EL, Kim RJ, Judd RM. Myocardial magnetic resonance imaging contrast agent concentrations after reversible and irreversible ischemic injury. Circulation 105, 224–229 (2002).
71 Kim RJ, Wu E, Rafael A et al. The use of contrast-enhanced magnetic resonance imaging to identify reversible myocardial dysfunction. N. Engl. J. Med. 343, 1445–1453 (2000).
72 Nazarian S, Knight BP, Dickfeld TL et al. Direct visualization of coronary sinus ostium and branches with a flexible steerable fiberoptic infrared endoscope. Heart Rhythm 2, 844–848 (2005).
73 Knight BP, Burke MC, Hong TE et al. Direct imaging of transvenous radiofrequency cardiac ablation using a steerable fiberoptic infrared endoscope. Heart Rhythm 2, 1116–1121 (2005).
• First to use infrared imaging through a steerable, fiberoptic, endoscopic catheter to identify intracardiac structures.
Website
101 Food and Drug Administration. Important information for physicians and other healthcare professionals. www.fda.gov/cdrh/radinj.html
Affiliations
• Michael S Panutich, MD
University of Chicago, Section of Cardiology, Department of Internal Medicine, University of Chicago, Chicago, IL, USATel.: +1 773 702 5988Fax: +1 773 702 [email protected]
• Bradley P Knight, MD
University of Chicago, 5758 S. Maryland Ave. MC9024 Chicago, IL 60637, USATel.: +1 773 702 5988Fax: +1 773 702 [email protected]