-
7/27/2019 Imagingthe Cervical Spine
1/87
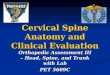
The CERVICAL SPINE
Imaging the Traumatized Patient
MI Zucker, MD
-
7/27/2019 Imagingthe Cervical Spine
2/87
A dr Z Lecture
on imaging cervical
spine trauma.
With much gratitude to
Jack Harris, MD.
-
7/27/2019 Imagingthe Cervical Spine
3/87
Michael I. Zucker, MD
Professor, Dept. of
Radiology
Faculty, Dept. ofEmergency Medicine
UCLA Medical Center,
David Geffen School
of Medicine at UCLA
-
7/27/2019 Imagingthe Cervical Spine
4/87
10,000 spinal cord injuries per
year in USA Two-thirds are cervical cord.
The monetary, physical and emotional
losses are great.
Our goal: Early detection of injuries to
prevent or decrease neurological and
mechanical damage to the spinal column.
-
7/27/2019 Imagingthe Cervical Spine
5/87
STABILITY: A Word or Two
We talk about it, but what is it?
A useful definition: An injury is STABLE if
putting the spinal column through normal
range of motion does not increase
neurological or mechanical deficits.
-
7/27/2019 Imagingthe Cervical Spine
6/87
-
7/27/2019 Imagingthe Cervical Spine
7/87
ANTERIOR COLUMN
The anterior
longitudinal ligament,
anterior 2/3 of thebody and disc.
-
7/27/2019 Imagingthe Cervical Spine
8/87
MIDDLE COLUMN
Posterior longitudinal
ligament and posterior
1/3 of body and disc.
-
7/27/2019 Imagingthe Cervical Spine
9/87
POSTERIOR COLUMN
The posterior osseous
arch and ligaments.
-
7/27/2019 Imagingthe Cervical Spine
10/87
DOES IT WORK?
If two or three columns injured, lesion is
unstable: Works well for C3 to T1.
Does not work so well for C1-2, so consider
most or all injuries here unstable.
-
7/27/2019 Imagingthe Cervical Spine
11/87
HOW DO YOU IMAGE THE
CERVICAL SPINE?Plain films?
CT?
MRI?
A combination of modalities?
Is there a consensus?
-
7/27/2019 Imagingthe Cervical Spine
12/87
NO
(But were headed toward one)
-
7/27/2019 Imagingthe Cervical Spine
13/87
My Opinion:
O*pin*ion: A belief held with confidence,
but not substantiated by proof.
-
7/27/2019 Imagingthe Cervical Spine
14/87
Imaging Minor Trauma
LATERAL view from skull base through at
least the top one-half of T1. May need to
supplement with Swimmers view.
Anterior-posterior (AP)
Open Mouth Odontoid (OMO)
If patient is not in cervical collar: Adding
Oblique views is an option.
-
7/27/2019 Imagingthe Cervical Spine
15/87
MINOR TRAUMA: Views
-
7/27/2019 Imagingthe Cervical Spine
16/87
Imaging Major Blunt Trauma
Cross-table
LATERAL plain film
in Trauma Suite. CT entire cervical
spine.
MRI also in selected
cases.
If you wish, AP,OMO, and Swimmersviews also -- IF theyDO NOT
cause delay.
CT: Axial sectionsbase of skull throughT1- AND- Sagittal(like a
lateral) andCoronal (like AP andOMO) reformatting.
-
7/27/2019 Imagingthe Cervical Spine
17/87
MAJOR TRAUMA: Imaging
Cross-table Lateral in
Trauma Suite
CT Base of skullthrough T1
-
7/27/2019 Imagingthe Cervical Spine
18/87
Swimmers View in Major
Trauma A SUPPLEMENTARY
view to see C7-T1 inlateral projection. NOT a
substitute for a bad lateral.One arm must be elevated,so
THEORETICALLYcould worsen amechanical or
neurological injury. A state-of-the-art CT
sagittal reformat ispreferable: dont need tomove patient and
imaging
easier and better.
-
7/27/2019 Imagingthe Cervical Spine
19/87
CT
Axial sections from
base of skull through
T1. ALWAYS do the
ENTIRE cervical
spine.
DONT do selective
imaging with modern
scanners.
-
7/27/2019 Imagingthe Cervical Spine
20/87
CT: Sagittal Reformatting
Reconstructed by
computer from axial
data: no additionalimaging needed.
Outstanding
lateral/swimmers
imaging.
-
7/27/2019 Imagingthe Cervical Spine
21/87
CT: Coronal Reformatting
Excellent OMO
Excellent AP
-
7/27/2019 Imagingthe Cervical Spine
22/87
MRI
Gold standard for
cord, thecal sac, nerve
root and disc injuries. Very good for
ligament injuries.
Fairly good for
fractures, but does
miss some. CT much
better.
-
7/27/2019 Imagingthe Cervical Spine
23/87
NEUROLOGIC DEFICIT
In my view, ANY neurologic deficit,extant or transient, is
MAJOR
trauma, and will need CT followed by
MRI.
-
7/27/2019 Imagingthe Cervical Spine
24/87
Any abnormality on Plain Films
or worrisome examination:
do CT!
Remember: Fractures often come in
2s and 3s. The more serious injurymay be the one that is
occult.
-
7/27/2019 Imagingthe Cervical Spine
25/87
ARE THERE RISKS?
Ionizing radiation can damage cells. Younger
people are more susceptible than older people.
Their cells are more sensitive and they have longerto manifest
somatic or genetic damage.
The radiation dose is significantly higher in CT
than in plain films.
As in most decisions in medicine, one must weigh
the risks versus the benefits.
-
7/27/2019 Imagingthe Cervical Spine
26/87
My Approach to Success in
Image Interpretation Know what to order.
Know what an optimal imaging series is and
dont accept less.
Read by check list.
Know the common lesions.
Know the commonly MISSED lesions.
-
7/27/2019 Imagingthe Cervical Spine
27/87
Remember: The lesions are the
SAME regardless of the imagingmodality
Plain films are still the most common
modality.
If you learn on them, you can
translate your knowledge to CT andMRI.
-
7/27/2019 Imagingthe Cervical Spine
28/87
PLAIN FILM Series
LATERAL
ANTERIOR-POSTERIOR (AP)
OPEN MOUTH ODONTOID (OMO)
*REVERSE WATERS
*SWIMMERS
*OBLIQUES
-
7/27/2019 Imagingthe Cervical Spine
29/87
THE CHECK LIST
View by view
-
7/27/2019 Imagingthe Cervical Spine
30/87
LATERAL view
This is your MAIN viewwhere 90% of injuries aredetected.
You MUST see T1. If notseen, do Swimmers view,unless not safe to
do so.
You did lateral andSwimmers and still no
luck? DONT QUIT: DOCT! Once you start anexam you must
completeit.
-
7/27/2019 Imagingthe Cervical Spine
31/87
LATERAL View: First Survey
Look for gross
fracture or dislocation.
Count vertebrae. Look at skull, entire
airway and adjacent
soft tissues.
-
7/27/2019 Imagingthe Cervical Spine
32/87
LATERAL View: Prevertebral
Soft Tissues Contour is more
important thanmeasurements:
straight or concaveanteriorly, except atlarynx.
Top normal limits: C2
6mm; C6 22mm foradult, 14mm for youngchild.
-
7/27/2019 Imagingthe Cervical Spine
33/87
LATERAL View: Alignment
Anterior body line.
Posterior body line.
Spino-laminar line(called posterior
cervical line at C1-3).
-
7/27/2019 Imagingthe Cervical Spine
34/87
LATERAL View: Alignment
Turning the lateral view HORIZONTALLY can
help detect subtle malalignment.
-
7/27/2019 Imagingthe Cervical Spine
35/87
LATERAL View: Spaces
Disc spaces: too wide,
too narrow, not
uniform? Facet joints: too wide,
not uniform?
Interspinous distances:
too wide, too narrow,not uniform?
-
7/27/2019 Imagingthe Cervical Spine
36/87
LATERAL View: C1 and C2
Basion-dens distance:
average 8mm, top
normal 12mm. C1: Anterior and
posterior arch.
C2: Dens, Harris ring,
body especially ant/infcorner, pars and
posterior arch.
-
7/27/2019 Imagingthe Cervical Spine
37/87
LATERAL VIEW:
Predental Space In an adult, upper
normal is 2.5mm.
Space is parallel ornarrow V shape.
In a young child,
upper normal is4.5mm.
-
7/27/2019 Imagingthe Cervical Spine
38/87
LATERAL VIEW: Predental
Space
-
7/27/2019 Imagingthe Cervical Spine
39/87
LATERAL View: C3-T1
Body: loss of straight
or concave anterior
contour, loss ofheight?
Posterior arch: subtle
cortical irregularity,
overt fracture line?
-
7/27/2019 Imagingthe Cervical Spine
40/87
LATERAL VIEW: Child
Vertebral bodies are bullet
shaped.
Physiologic
pseudosubluxations are
common, especially C2-4.
Predental space is wider.
Lymphoid tissue makes
soft tissues more
prominent.
-
7/27/2019 Imagingthe Cervical Spine
41/87
SWIMMERS View
A supplemental view
to see C7-T1.
Must raise one arm.Probably not a good
idea if neurologic
deficit, altered level of
consciousness, upperarm injury. Could
worsen an injury.
-
7/27/2019 Imagingthe Cervical Spine
42/87
ANTERIOR-POSTERIOR View
Look at first few ribs,
sterno-clavicle junction,
lung apices.
Contour of lateral margins
of lateral masses.
Uncovertebral joints.
Alignment and contour of
spinous processes.
Position and contour of
trachea.
-
7/27/2019 Imagingthe Cervical Spine
43/87
The ODONTOID Views
Open Mouth Odontoid
(OMO) is main view.
Reverse Waters view
is supplementary, to
see top half of dens
ONLY.
-
7/27/2019 Imagingthe Cervical Spine
44/87
OMO
C1-2 lateral mass alignment
of lateral margins.
Dens: cortical margin
irregularities, fracture
lines, tilt.
Upper body of C2 for
fracture lines.
Mach lines can be confusing.
-
7/27/2019 Imagingthe Cervical Spine
45/87
The INJURIES
C1 and C2: by anatomic location
C3 to T1: by mechanism of injury
(Modified from the classification of John
Harris, et al.)
-
7/27/2019 Imagingthe Cervical Spine
46/87
The Atlas and the Axis
C1 and C2 injuries differ from the rest of
the cervical spine and are considered
separately. Although controversial, best to consider
ALL C1 and C2 injuries as UNSTABLE in
the acute trauma setting.
-
7/27/2019 Imagingthe Cervical Spine
47/87
-
7/27/2019 Imagingthe Cervical Spine
48/87
-
7/27/2019 Imagingthe Cervical Spine
49/87
C1: Isolated Arch Fractures
Anterior arch
Posterior arch
CAUTION: You maybe dealing with a
Jefferson fracture with
occult components:
Best to CT all C1fractures.
-
7/27/2019 Imagingthe Cervical Spine
50/87
JEFFERSON Fracture: C1
Axial load (burst) injury
Pure (4) or variant (2 or 3)
fractures, involving both
ant. & post. arches of C1
Cord injury in 15%
Lateral view: anterior and
posterior arch fractures
OMO view: lateral
displacement of C1 lateral
masses
-
7/27/2019 Imagingthe Cervical Spine
51/87
JEFFERSON Fracture: C1
The lateral masses of C1and C2 must be aligned onthe OMO
view.
1-2mm of lateraldisplacement on one sideand an EQUAL
medialdisplacement on the otheris head rotation.
ANY other pattern: lateraldisplacement on bothsides or lateral
on oneside, and none on theother is abnormal.
-
7/27/2019 Imagingthe Cervical Spine
52/87
JEFFERSON Fracture
CT Classical Jefferson: 4
fractures, 2 ant./2 post.
Jefferson variants: 2or 3 fractures, but at
least 1 ant. & 1 post.
-
7/27/2019 Imagingthe Cervical Spine
53/87
-
7/27/2019 Imagingthe Cervical Spine
54/87
DENS Fractures
Type I: alar ligament
avulsion of the tip; rare.
Type II: the dens
excluding the tip; 2/3.
Type III: high C2 body;
1/3.
Mechanism of Type II and
III is controversial.
-
7/27/2019 Imagingthe Cervical Spine
55/87
TYPE II Dens Fracture
Interrupted cortical
margin, lucent fracture
line, tilt especially
anterior
Cord injury in 15%
Delayed or non-union
50+%
-
7/27/2019 Imagingthe Cervical Spine
56/87
-
7/27/2019 Imagingthe Cervical Spine
57/87
TYPE III Dens Fracture
Interrupted Harris
ring, fat C2, lucent
fracture line, tilt
especially ant.
Cord injury in 15%
Heals well.
-
7/27/2019 Imagingthe Cervical Spine
58/87
C2: PARS Fracture
Called Hangmans or
pedicle fracture, both
wrong.
Extension injury.
Cord injury in 15%.
Non-displaced,
displaced, subluxed.
-
7/27/2019 Imagingthe Cervical Spine
59/87
C2: Extension Teardrop Fracture
Avulsion by the
anterior longitudinal
ligament of the
anterior-inferior
corner of the body.
Extension mechanism.
Cord injury is low.
-
7/27/2019 Imagingthe Cervical Spine
60/87
C3 to T1
These levels are so similar they willbe considered as a
unit.
The injuries are grouped by
mechanism into families.
-
7/27/2019 Imagingthe Cervical Spine
61/87
-
7/27/2019 Imagingthe Cervical Spine
62/87
FAMILY FLEXION
Motto: Anterior impaction,
posterior distraction.
Family members:Wedge compression fracture
Hyperflexion sprain
Bilateral interfacetal dislocationHyperflexion teardrop
fracture-dislocation
Spinous process fracture
-
7/27/2019 Imagingthe Cervical Spine
63/87
Wedge Compression Fracture
Anterior-superior marginof the body is fractured.
If loss of height less than
50%, one column injuryand so stable.
If height loss greater than50%, posterior ligaments
presumed torn and so 3
column unstable injury. If 3 bodies fractured,
unstable even if less than50% height loss each.
-
7/27/2019 Imagingthe Cervical Spine
64/87
-
7/27/2019 Imagingthe Cervical Spine
65/87
Flexion-Extension Films
May be helpful inligament injuries
-but are-
Frequently useless dueto muscle spasm
-
7/27/2019 Imagingthe Cervical Spine
66/87
-
7/27/2019 Imagingthe Cervical Spine
67/87
-
7/27/2019 Imagingthe Cervical Spine
68/87
MRI
Gold Standard for
spinal canal, cord, disc
lesions.
Silver Standard for
ligament injuries, but
there is no Gold and
much better than plainfilms, CT, and
flexion/extension.
-
7/27/2019 Imagingthe Cervical Spine
69/87
Bilateral Interfacetal Dislocation
BID, also called locked
facets is anything but
locked. It is a severe 3
column injury that iscompletely unstable.
Cord is injured in 2/3.
Body is subluxed
anteriorly at least 50%. Marked posterior
distraction.
-
7/27/2019 Imagingthe Cervical Spine
70/87
Hyperflexion Teardrop Fracture-
dislocation Among the worst
survivable injuries,
with nearly 100%
severe cord lesion.
Completely unstable.
Little chance of
neurologicimprovement.
-
7/27/2019 Imagingthe Cervical Spine
71/87
Hyperflexion Teardrop Fracture-
dislocation CT Sagittal Reformat
-
7/27/2019 Imagingthe Cervical Spine
72/87
-
7/27/2019 Imagingthe Cervical Spine
73/87
Spinous Process Fracture
CT Sagittal Reformat
-
7/27/2019 Imagingthe Cervical Spine
74/87
FLEXION-ROTATION
Injuries
Unilateral Interfacetal Dislocation
and Fracture-dislocation
-
7/27/2019 Imagingthe Cervical Spine
75/87
-
7/27/2019 Imagingthe Cervical Spine
76/87
-
7/27/2019 Imagingthe Cervical Spine
77/87
-
7/27/2019 Imagingthe Cervical Spine
78/87
-
7/27/2019 Imagingthe Cervical Spine
79/87
P t i A h F t
-
7/27/2019 Imagingthe Cervical Spine
80/87
Posterior Arch Fractures
Plain films are insensitive,CT is outstanding.
Isolated: pedicle, lateralmass, lamina or spinous
process.
Multiple fractures arecommon. Pedicle/laminafractures cause
free-floating lateral mass.
May be additional elementof lateral bending.
Stability depends on whatis fractured.
-
7/27/2019 Imagingthe Cervical Spine
81/87
Extension Teardrop Fracture
Avulsion fracture caused
by anterior longitudinal
ligament.
Vertical narrow fracture ofanterior-inferior corner of
body.
Most common site is C2.
Unstable.
-
7/27/2019 Imagingthe Cervical Spine
82/87
-
7/27/2019 Imagingthe Cervical Spine
83/87
AXIAL Loading
Burst fracturesexplode the body.
All are very unstable
and cause cord injuryin 2/3 (except C1).
There is usually anelement of flexion
also.
-
7/27/2019 Imagingthe Cervical Spine
84/87
BURST Fractures
On lateral, body is
compressed anteriorly,
inferior end plate often
fractured, posterior
body contour is
convex.
On AP, body fractureis vertical or oblique
and pedicles spread.
-
7/27/2019 Imagingthe Cervical Spine
85/87
BURST Fractures
CT more accurately
displays the fracture
pattern and the very
important degree of
narrowing of the
spinal canal.
-
7/27/2019 Imagingthe Cervical Spine
86/87
REMEMBER:
CT is much more sensitive for
fractures than plain films.MRI is the standard for soft
tissue
injuries.
GOODBYE AND GOOD
-
7/27/2019 Imagingthe Cervical Spine
87/87
GOODBYE AND GOOD
IMAGING!
Copyright 2004 M. I. Zucker