Embed Size (px)
Citation preview

1
Educational Objectives
After completing this activity, the participant should be better able to:
• Explain how the proper recognition and management of ADHD in adolescents by MCOs can improve clinical outcomes and reduce theeconomic burden of disease
• Indicate the link between ADHD and the most common psychiatric comorbidities
• Describe current ADHD guidelines and treatment protocols• Outline opportunities to maximize health plan performance for the
ADHD HEDIS measure• State examples of ADHD quality improvement strategies for MCOs
Effectively Recognizing and Managing ADHD in Adolescents
Timothy E. Wilens, M.DClinical & Research Program in Pediatric Psychopharmacology
Massachusetts General HospitalHarvard Medical School

2
Overview
• Estimated prevalence: – 6 to 8% of children– 6% of adolescents– 4% of adults
• 4:1 male to female ratio in children and adolescents• Treatment utilization varies widely within and between cultures,
ethnicities, and socioeconomic status
Goldman LS, et al. JAMA 1998;279:1100-1107. Barkley RA. In: Mash EJ, Barkley RA. eds. Treatment of Childhood Disorders. New York; Guildford Press 1989.
ADHD Subtypes
• DSM-IV-TR* ADHD subtypes– Combined subtype (50–75%)– Primarily inattentive (20–30%)
• Increases with age– Primarily hyperactive–impulsive (<15%)
*DSM-IV-TR: Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision.American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th Edition, Text Revision. Washington, DC. American Psychiatric Association. 2000;48:85-93.
Etiology
• ADHD is a heterogeneous behavioral disorder with multiple possible etiologies
NeuroanatomicNeurochemical
CNS insults
Genetic origins
Environmental factors
ADHD
Biederman J, Faraone SV. Lancet 2005;336:237-48.

3
DSM-IV Diagnostic Criteria for ADHD
1. Either (1) Symptoms of inattention, or (2) symptoms of hyperactivity-impulsivity or (3) both
2. Onset <7 years of age (childhood-onset)3. >6 months of disturbance4. Cross-situational (home, work, school)5. Impairment in functioning
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th Edition, Text Revision. Washington, DC. American Psychiatric Association. 2000;48:85-93.
Clinical Presentation in an Adolescent (13-18 Years of Age)
• May seem restless rather than hyperactive• Problems with attention, task completion, shifting of activities
prematurely• School work disorganized and shows poor follow-through; fails
to work independently• Seems emotionally immature • Has poor self-esteem• Has poor peer relationships• May engage in irresponsible or risky behavior
Wolraich ML, et al. Pediatrics. 2005;115:1734-1746.Barkley RA. Attention-Deficit Hyperactivity Disorder: A Handbook for Diagnosis and Treatment. 3rd ed. New York, NY: Guilford Press; 2006.Barkley RA, et al. J Am Acad Child Adolesc Psychiatry. 1991;30:752-761.
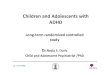
Motoric hyperactivityLow frustration toleranceImpulsivenessDistractibilityShifting of activitiesFidgetinessImpatienceRestlessnessInattentiveness
Children
Adults
ADHD Developmental Trends by Age
• Symptoms of ADHD decline and change from childhood to adulthood
Wolraich et al. Pediatrics. 2005;115:1734-1746.Millstein et al. J Attention Disorder 1997.

4
Evidence of Persistence of ADHD Into Adulthood
6572
31
6658
0
20
40
60
80
1 2 3 4 5*
Perc
enta
ge
Biederman J, et al. Arch Gen Psychiatry. 1996;53:437-446.Barkley RA, et al. J Am Acad Child Adolesc Psychiatry. 1990;29:546-557.Gittelman R, et al. Arch Gen Psychiatry. 1985;42:937-947.Weiss G, et al. J Am Acad Child Psychiatry. 1985;24:211-220.Biederman J, et al. Psychol Med. 2006;36;167-179.
Age at follow-up
Age at diagnosis
16 to 28
6 to 18
21 to 33
6 to 12
16 to 2312 to 2010 to 21
6 to 124 to 126 to 17
*Same cohort as study 1 at 10-year follow-up.
Common Co-occurring Conditions
• Oppositional defiant disorder (ODD)• Conduct disorder (CD)• Anxiety disorders
– Generalized anxiety disorder– Obsessive-compulsive disorder (OCD)– Posttraumatic stress disorder (PTSD)
• Depression• Bipolar disorder• Tic disorder• Learning disabilities
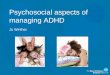
Cumulative Morbidity Risks for Psychiatric Disorders in Young Men With ADHD
0
0.2
0.4
0.6
0.8
1
MDD BPD OCD Ticdisorders
ODD CD
Cum
ulat
ive
mor
bidi
ty ri
sk ADHDControl
Biederman J, et al. Psychol Med. 2006;36:167-179.
10-year follow-up of males with ADHD (n = 112) and case controls (n = 105)Mean age at follow-up: 22 yearsMDD = major depressive disorder; BPD = bipolar disorder; OCD = obsessive-compulsive disorder; ODD = oppositional defiant disorder; CD = conduct disorder.
*ADHD vs Control, P<.001†P = .004
*
* *
*
*
†

5
Academic and Behavioral Impairments Continue in Adolescence
• 15–25% of children have poor academic outcome1–5
• Almost 30% of ADHD subjects fail grades2
• 46% of ADHD pupils suspended2
• 25% of persistently antisocial6–9
1. Gittelman R, et al. Arch Gen Psychiatry. 1985;42:937-947.2. Barkley RA. Attention-Deficit Hyperactivity Disorder. A Handbook for Diagnosis and Treatment, 2nd ed. New York: Guilford Press;1998.3. Mannuzza S, et al. J Am Acad Child Adolesc Psychiatry. 1997;36:1222-1227.4. Mannuzza S, et al. Arch Gen Psychiatry. 1993;50:565-576.5. Weiss G, Hechtman L. Hyperactive Children Grown Up. 2nd ed. New York: Guilford Press 1993.6. Mannuzza S, et al. Arch Gen Psychiatry. 1989;46:1073-1079.7. Mannuzza S and Klein RG. Child Adolesc Psychiatr Clin N Am. 2000;9:711-726.8. Barkley RA. Attention-Deficit Hyperactivity Disorder. A Handbook for Diagnosis and Treatment, 2nd ed. New York: Guilford Press;1998.9. Fischer M, et al. J Abnorm Child Psychol. 2002;30(5):463-475.
ADHD Adolescents and Driving
Barkley RA, et al. Pediatrics. 1993;92:212-218.Cox D, et al. J Nerv Ment Dis. 2000;188;230-234.Barkley RA, et al. Pediatrics. 1996;98:1089-1095.Murphy K, Barkley RA. Comp Psychiatry. 1996;37:393-401.
Increased likelihood of outcome compared with age-matched controls
0 2 4 6 8
More damage
Injuries
Fault
Accidents
Other traffic violations
Speeding violations
License suspended
Biederman J, et al. J Am Acad Child Adolesc Psychiatry. 1997;36:21-29.Biederman J, et al. Am J Psychiatry. 1995;152:1652-1658.Wilens TE, et al. J Nerv Ment Disord. 1997;185:475-482.
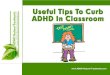
Sharp rise in Substance Abuse betweenmid-adolescence and adulthood
ADHD: Risk of Substance Abuse
15% 15%
27%
55%
0%
10%
20%
30%
40%
50%
60%
Youth Adults
Perc
ent I
ncre
ase
in R
isk Control
ADHD

6
Flory K, et al. J Clin Child Adolesc Psychology. 2006;35:571-577.
Sexual Behavior
0 10 20 30 40 50 60 70
Pregnancy
>4 sex partners (lifetime)
Casual sex + infrequent condom use
Casual sex past year
Participants (%)Control (n = 111) ADHD (n = 175)
Young men (aged 18–26) with and without childhood ADHD; self-reports
P = 0.01
P = 0.02
P <0.001
P <0.001
Criminality
0
20
40
60
80
100
Stolenproperty
Assault withfists
Assault withweapon
Carriedconcealed
weapon
Ever arrested Arrestedtwice or more
Misdemeanorarrest
Felony arrest
Part
icip
ants
(%)
ADHD Control
Barkley RA, et al. J Child Psychol Psychiatry 2004;45:195-211.
ADHD: n = 147; 87% Male; mean age = 21.1Control: n = 73; 92% Male; mean age = 20.5
P <0.001
P = 0.001
P = 0.005
P <0.001
P = 0.019
P <0.001
P = 0.025 P = 0.006
Neurobiology of ADHD
• Smaller frontal lobes, basal ganglia, cerebellar vermus• Delay in white matter/frontal tract maturation• Abnormal PET and fMRI studies (multiple)• Abnormal DAT binding• Abnormal dopamine transmission• Genetic studies (multiple)
– Twin > 0.80 concordance– Candidate genes (D4, D2, DAT, SNAP, 5HT)
Faraone SV, et al. Am J Psych 1999;156:768-70. Zametkin AJ, Liotta W. J Clin Psych 1998;59 Suppl 7:17-23.Ernst M, et al. Am J Psychiatry. 1999;156:1209-15.Casetellanos FX, et al. JAMA 2002;288:1740-8. Faraone SV, et al. Biol Psychiatry. 2005;57:1313-23.
PET: Positron Emission Tomography; fMRI: Functional magnetic resonance imaging; DAT: Dopamine transporter; SNAP: S-nitroso-N-acetylpenicillamine; 5HT: 5-hydroxytryptamine

7
Treatment Considerations in Adolescents with ADHD
• Psychoeducation• Educational intervention/remediation• Counseling• Supportive problem-directed therapy• Cognitive/behavioral intervention• Coaching• Family therapy• Medication
Wolraich et al. Pediatrics 2005:115:1734-46.
Treatment Considerations for Adolescents With ADHD
Adolescents are neither children nor adults• Adolescents often need to feel “in control” of condition and
treatment– Problems negotiating treatment alliance– Adherence
• In selecting medication– Tailor treatment to fit adolescent’s schedule– Keep treatment private/out of school– Consider and discuss risk for substance abuse, misuse, and diversion
Wolraich et al. Pediatrics 2005:115:1734-46.
Pharmacologic Treatments Approved for ADHD
Duration of effect
12 hoursLisdexamfetamine dimesylate (Vyvanse®)6–8 hoursDextroamphetamine (Dexedrine® Spansule)
3–4 hoursMethylprenidate (Ritalin®)
Up to 24 hoursAtomoxetine (Strattera®)Nonstimulant
4–6 hoursMixed amphetamine salts (Adderall®)10–12 hours Mixed amphetamine salts (Adderall XR®)
Amphetamine-based treatments
~12 hours (worn for 9)Methylphenidate (Daytrana®)
3–4 (8–10) hoursDexmethylphenidate (Focalin® XR)~8 hoursMethylprenidate (Ritalin® LA)
8–10 hoursMethylprenidate (Metadate® CD)
~12 hoursMethylprenidate (Concerta®)Methylphenidate-based formulations
Physicians’ Desk Reference. 59th ed. Montvale, NJ: Thomson PDR; 2005.

8
Dosing Stimulants
• Start with low dose to establish tolerability• Titrate until no further improvement is seen or until significant
side effects are noted• Underdosing is a common concern (methylphenidate)• No simple association between optimal dosage and age,
weight, or blood levels, although adolescents and adults usually require a higher dose than do children
• If an effective medication seems to become less effective as a child reaches adolescence, try increasing the dose
Potential for Abuse
• Nonstimulants (eg, atomoxetine, bupropion) are less likely to be misused or diverted than stimulants
• The slower the uptake into the brain, the lower the abuse liability of the stimulant
• Long-acting formulations of stimulants are less likely to be misused or diverted than immediate-release formulations
Volkow ND, et al. Nature 1997;386:827-830.Spencer TJ, et al. Am J Psychiatry. 2006;163:387-395.
ADHD and Substance Abuse
Wilens T, et al. J Nerv Ment Dis. 1997;185:475-482.
Survival Curve: Risk for Substance Use Disorder (SUD) Onset in Adults With Untreated ADHD
ControlADHD
P ≤0.05, ADHD vs control at endpoint
Ris
k fo
r SU
D (%
)
0102030405060708090
100
Age at onset (years)0 10 20 30 40 50 60
Earlier onset
Higher risk

9
Biederman J, et al. Pediatrics. 1999;104:20; Wilens et al. Pediatrics. 2003;11:179-183. Faraone SV, Wilens T. J Clin Psychiatry. 2003;64(suppl 11):9-13.
Pharmacotherapy for ADHD may be protective against
substance abuse
Pharmacotherapy and Substance Abuse With Stimulants
• Fear: Stimulant therapy may lead to substance abuse • Fact: Untreated ADHD is a significant risk factor for substance
abuse in adolescence
Misuse and Diversion of Stimulants
11%
22%
10%
22%
0%
5%
5%
5%
0% 5% 10% 15% 20% 25%
Sold
Used too much
Got high
Misused
Patients
No ADHD (n = 43)ADHD (n = 55)
Wilens T, et al. J Am Acad Child Adolesc Psychiatry. 2006;45:408-414.
Adolescents with ADHD are more likely to misuse or divert their medication than are non-ADHD adolescents taking psychoactive drugs
Characteristics of ADHD Patients Who Misuse or Divert Medication
83%
58%
31%
83%
75%
53%
0% 20% 40% 60% 80% 100%
Divert
Misuse
All ADHD
Patients
SUDCD
Wilens T, et al. J Am Acad Child Adolesc Psychiatry. 2006;45:408-414.
ADHD patients with comorbid CD or SUD are more likely to misuse or divert their medication.
(N = 55)
(n = 6)
(n = 12)

10
Possible Predictors of Misuse of ADHD Medications
• Signals alerting to the possible motivation to misuse ADHD agents include
– Competitiveness of the college environment1
– Other drug use2
– Presence of: • Current ADHD and depressive symptoms3,4,5
• Neuropsychological deficits5
1. McCabe SE, et al. Addict Behav 2005;30:1342-50.2. White BP et al. J Am Coll Health 2006;54:261-8.3. Poulin C. Addiction 2007;102:740-51.4. Upadhyaya HP, et al. J Child Adolesc Psychopharmacol 2005 ;15 :799-809.5. Wiens TE, et al. J Am Acad Child Adolesc Psychiatry 2008: In press.
Time (hrs)
Feel
an
Effe
ct
OROS MPH (90 mg) & IR MPH (40 mg):“Feel an Effect”
0
5
10
15
20
25
0 1 2 3 4 5 6 7 8 9 10
IR-MPHOROS-MPH
*
** †*
N=6 per group.*p < 0.05.†p < 0.01.IR: extended release; OROS = osmotically controlled-release oral delivery systemSpencer TJ, et al. Am J Psychiatry. 2006;163:387-395.
Does Stimulant Treatment Effect Neural Activity?
Bush G, et al. Arch Gen Psychiatry. 2008;65:102-114.
• ADHD associated with dysfunction of the dorsal anterior midcingulate cortex (daMCC) and other cingulofrontoparietal regions associated with attention
• Stimulants are effective therapy for ADHD• Study conducted to determine if stimulant treatment
effects neural activity• daMCC activation during the Multi-Source Interference Task
measured by functional MRI (fMRI) in 21 adults with ADHD treated for 6 weeks
• MPH OROS (n=11)• Placebo (n=10)

11
Treatment with OROS MPH Increased Activation in Regions Associated with Attention
Bush G, et al. Arch Gen Psychiatry. 2008;65:102-114.
• MPH OROS treatment elicited increased activation of the cingulofrontoparietalnetwork including:• Dorsal anterior
midcingulate cortex(daMCC) bilaterally
• Right-sided dorsolateralprefrontal cortex (DLPFC)
• Bilateral superior parietal cortices (Parietal)
Sagittal Axial Coronal
ADHD Treatment SummaryIn Adolescents
• Methylphenidate, mixed amphetamine salts, and atomoxetine are all safe and efficacious in adolescents with ADHD
• MPH has the most clinical trial data• Long-acting forms of methylphenidate and mixed
amphetamine salts are also safe and effective and are thought to have a lower risk of abuse compared to immediate-release forms
• Atomoxetine is the only FDA-approved nonstimulant for ADHD
Treatment Plan (continued)
• Management of comorbid disorders– Psychotherapy– Medication– Substance abuse treatment programs
• Assistance with time management and organization (consult ADHD coaches or therapists)
• Psychosocial treatments– Family therapy or parent management training– Individual therapy
• Vocational assessment/career counseling

12
Adolescent ADHD Summary
• ADHD is frequently persistent into adolescence• Common domains of impairment
– Academic underachievement– Family functioning– Driving
• Adolescents with ADHD respond favorably to treatment• Medication is fundamental to treatment• Medications in ADHD
– Improve ADHD symptoms– Improve functional outcomes (family, driving, social)– Reduce risk for substance abuse– Permit many to succeed and go to college
Managed Care Strategies to Improve ADHD Outcomes
Jeffrey D. Dunn, PharmD, MBAFormulary and Contract Manager
SelectHealth Plans (formerly IHC Health Plans, Inc.)
ADHD is a Common Diagnoses in Children Less Than 18 Years Old
0.140.12
0.08 0.07
0%
5%
10%
15%
20%
Asthma
Respira
tory Alle
rgy
Learn
ing Disa
bility
ADHD
Asthma
RespiratoryAllergyLearningDisabilityADHD
(n=73,493)
(n=73,493) (n=61,354)(n=61,354)
Perc
ent o
f chi
ldre
n <1
8 ye
ars
old
with
dia
gnos
is
2006 National Health Interview Survey
Bloom B, Cohen RA. Vital Health Stat 10. 2007;234:1-79.

13
Consequences of Untreated ADHD Increase with Age
Kewley GD. Attention Deficit Hyperactivity Disorder (ADHD): Recognition,Reality and Resolution. Oxon, United Kingdom: David Fulton Publishers;2002.
• ADHD only• Low Self-Esteem
• Disruptive Behavior
• Poor Social Skills
• Learning Delay
• Oppositional Defiant Disorder
• Mood Disorder
• Challenging Behavior
• Antisocial Behavior
• School Exclusion
• Substance Abuse
• Conduct Disorder
• Lack of Motivation
• Complex Learning Disorder
6 10 14-16Age (years)
Impact of ADHD in Childhood and Adolescence Compared to non-ADHD Peers
Health Care Use50% ↑ Bicycle accidents1
33% ↑ Emergency visits2
>4x ↑ Vehicle accidents3
Society2X > Risk for SUD6
Earlier onset of SUD7
More likely to continue SUD into adulthood8
School/Work46% Expelled4
35% Dropped out4Lower occupational status5
Family>4x h Sibling fighting9
>4x h Separation/divorce in adulthood10
1. DiScala C, et al. Pediatrics 1998102:1415-21 . 2. Liebson CL, et al. JAMA 2001;285-60-66.3. Barkley RA, et al. Pediatrics 1996;98:1089-1095.4. Barkley RA, et al. J Am Acad Child Adolesc Psychiatry 1990;29:546-557.5. Mannuzza S, et al. J Am Acad Child Adolesc Psychiatry 1997;36:1222-1227.
6. Biederman J, et al. J Am Acad Child Adolesc Psychiatry 1997;36:21-29.
7. Pomerleau OF, et al. J Subst Abuse 1995;7:373-8.8. Wilens T, et al. Psychiatr Serv 1995;46:761-3, 765.9. Mash EJ, Johnston C. J Consult Clin Psychol 1983;51:86-99.10. Barkley RA, et al. J Child Psychol Psychiatry 1991;32:233-55.
ADHD Associated with Lower Educational Achievement and Income
22%30%
55%65%
34%
56%
72% 77%
0%
25%
50%
75%
100%
Less thanhigh
school
Highschool;some
college
College;some post
grad
Post-graddegree
Biederman J, Faraone SV. MedGenMed. 2006;8:12.
Fulltime Employed by Academic Achievement
†p<.001 for all comparisons.
Average Income by Academic Achievement
*p<.05; **p<001.
0
20,000
40,000
60,000
80,000
100,000
Less thanhigh
school
Highschool;some
college
College;some post
grad
Post-graddegree
29.5K23.8K
38.7K
46.7K
63.0K 66.6K
52.4K
91.3K
*
**
†
†
††
ADHD (n=500)No ADHD (n=501)

14
ADHD Associated with Greater Use of Hospital Care
26%
41%
81%
18%
33%
74%
0%
25%
50%
75%
100%
In-patient Care Out-patient Care ED Admission
ADHDNo ADHD
Population based Cohort Study of Adolescents (Mean Age: 15.3 years)
Prop
ortio
n re
quiri
ng
hosp
ital s
ervi
ces
Leibson CL, et al. JAMA 2001;285:60-66.
n=4119
p<.001
p=.006
p=.005
Presence of ADHD Increases Health Care Utilization Costs
$245
$20 $66
$690
$427
$222$335
$1,465
$0
$300
$600
$900
$1,200
$1,500
Primary Care MentalHealth Care
Pharmacy Total
No ADHD(n=11,968)ADHD (n=2,992)
Guevara J, et al. Pediatrics 2001;108:71-78.
Patients 3-17 Years of Age Enrolled in the Group Health Cooperative
Cos
ts p
er p
atie
nt p
er y
ear
*p <0.001 vs. no ADHD
*
*
**
ADHD Diagnostic and Treatment Guidelines
AACAP Practice Parameters October 1997
AAP Practice Guideline
May 2000
NIH Consensus Statement February 2000
Organizations with ADHD Practice Guidelines
AAP: American Academy of PediatriciansAACAP: American Academy of Child and Adolescent PsychiatryNIH: National Institutes of Health

15
Are Providers Using the Guidelines?
• Survey of 1374 physicians indicated– 92% of pediatricians and 60% of primary care physicians were familiar with the
AAP guidelines– Only 26% used all 4 diagnostic components in the guidelines
• DSM criteria• Parent surveys• Teacher surveys• Assessment for co-existing conditions
Rushton JL, et al. Pediatrics 2004;114:e23-e28.
Approach to ADHD Treatment
• ADHD is highly treatable1
– Combination of behavioral and pharmacological approaches most effective to control symptoms1
• Stimulants remain 1st line treatment1– Any individual stimulant effective in ~70% of ADHD patients2
– Many who fail to respond to one may respond to another2,3
• Stimulants generally safe and well tolerated3
• Non-stimulating agents recently introduced
1. American Academy of Pediatrics. Pediatrics. 2001;1081033-44.2. US Department of Health and Human Services, 1999.3. Scott-Levin Inc., Physician Drug and Diagnosis Audit (PDDA), 2001.
American Academy of Pediatrics (AAP): ADHD Treatment Goals
• Immediate and long-term control of symptoms• Decreased disruptive behaviors• Improved academic performance• Increased independence• Improved self-esteem• Improvements in relationships
American Academy of Pediatrics. Pediatrics. 2001;1081033-44.

16
AAP Treatment Plan
• Begin patient and family education about ADHD immediately after diagnosis
• Implement home, work, school, and lifestyle adjustments• Initiate therapy with appropriate medication targeting
symptoms• Identify and manage comorbid conditions
– Psychotherapy or cognitive therapy– Substance abuse treatment
American Academy of Pediatrics. Pediatrics. 2001;1081033-44.
StimulantsMethylphenidate Amphetamine
Short ActingSODAS MPH
Dexmethylphenidate
Long ActingMAS XR
Short ActingDextroamphetamine
Dextroamphetamine tabs
Long ActingOROS MPH
Diffucaps MPHMPH LA
Dexmethylphenidate XRMPH transdermal patch
IntermediateDextroamphetamine ER
MAS
IntermediateMPH SRMPH SR
Nonstimulant
TCAModafinil; Bupropion
Guanfacine; ClonidineVenlafaxine
Not ApprovedApproved
Atomoxetine
SODAS = spheroidal oral drug absorption system; MPH = methylphenidate; SR = sustained release;ER = extended release; OROS = osmotically controlled-release oral delivery system; LA = long acting;XR = extended release; TCA = tricyclic antidepressants
Pharmacologic Intervention in ADHD
Drug Therapy of ADHD is Highly Cost-Effective
• For the routine treatment of children with ADHD, medication management is more cost-effective than behavioral treatment or combined medication + behavioral therapy*
Jensen PS, et al. Am J Psychiatry 2005;162:1628-1636.
*From the Multimodal Treatment Study of Children with ADHD (n=579 children 7-9.9 years of age treated for 14 months)

17
Managed Care Considerations with ADHD Therapy
• Dosing flexibility and convenience• Duration of action
– Short- vs. long-acting agents
• Risk for abuse or diversion• Tolerability and safety• Cost• Access/reimbursement• Pediatric vs. adult• Polypharmacy• Formulary management
– DACON, future generics, new products
Considerations for Stimulants
• Stimulant usually chosen for most children and teens– Efficacy supported by over 200 randomized, placebo-controlled, blinded clinical
trials– Most studies of short duration (i.e., 2-4 months)– Few long term trials
• MPH and DEX have similar profiles– DEX slightly more side effects, which are mild– Mixed amphetamine salt preparation (Adderall)
• Recent withdrawal of long acting product in Canada• Warning of use in children with cardiac conditions
• Selective nature of stimulants can vary from one agent to another
• Consider parent preference
First Line Therapy
• Stimulants recommended as first line therapies– Efficacy ranges from 68-80%– 3-4% of patients experience side effects causing discontinuation– Many generics available in the short-acting formulation
• Long-acting generics are not yet available– Duration of effect ranges from 2-12 hours
American Academy of Pediatrics. Pediatrics. 2001;1081033-44.

18
Second and Third Line Interventions
• Atomoxetine second line– Effective in 50 – 60% of patients– Similar side effects to stimulants– Provides 24 hour coverage– 1-3 weeks to reach effect
• Bupropion– Fewer studies, more serious side effects– Role of antidepressant effect– 24 hour coverage with twice daily dosing– 3-4 weeks to reach effect
American Academy of Pediatrics. Pediatrics. 2001;1081033-44.
Newer ADHD Pharmacotherapies
Once/twice daily8-24 hoursNon-Stimulants• Atomoxetine (Strattera®)
Once dailyMultiple
Twice dailyOnce daily
12 hours~4 (8) hours
6-8 hours12 hours
Amphetamine Formulations• Mixed amphetamine salts (Adderall® XR)• Dextroamphetamine (Dexedrine Spansules®)• Mixed amphetamine salts (Adderall®)• Lisdexamfetamine dimesylate (Vyvanse®)
Once dailyOnce dailyOnce daily
Twice (once) dailyOnce daily
12 hours8-10 hours~8 hours
~5 (10) hours7-12+ hours
MPH Formulations• Methylprenidate (Concerta®)• Methylprenidate (Metadate® CD)• Methylprenidate (Ritalin® LA)• Dexmethylphenidate [(Focalin® (XR)]• Methylprenidate (Daytrana®)
Dosing ScheduleDuration of effect
ADHD Drug Dosing
Wilens TE, et al. Ann Rev Med. 2002;53:113-131.
QD/BID100 mg40mgAtomoxetine (Strattera)
QD70mg30 mgLisdexamfetamine dimesylate (Vyvanse)
BID50 mg5 mgDextroamphetamine (Dexedrine Spansules)
BID/TID40 mg2.5 to 5 mgDextroamphetamine (Dexedrine)
QD30 mg5 to 10 mgMixed amphetamine salts (Adderall XR)
BID40 mg2.5 to 5 mgMixed amphetamine salts (Adderall)
QD30 mg10 mgMethylprenidate (Daytrana)
QD20 mg5 mgDexmethylphenidate (Focalin XR)
QD60 mg10 mgMethylprenidate (Ritalin LA)
QD60 mg20 mgMethylprenidate (Metadate CD)
QD72 mg18 mgMethylprenidate (Concerta)
BID10 mg2.5 mgDexmethylphenidate (Focalin)
TID60 mg5 mgMethylprenidate (Ritalin)
Dosing Schedule
Maximum Dose
Starting Dose
Medication

19
Drug Delivery Systems May Reduce Risk for Abuse and Diversion
• Newer delivery systems may reduce misuse liability • Different formulations alter pharmacokinetics and/or limit
access to the active drug by using – Prodrugs [lisdexamfetamine dimesylate (Vyvanse)]– Beaded preparations [methylprenidate (Adderall XR; Ritalin LA);
dexmethylphenidate (Focalin XR)]– Osmotic preparations [methylprenidate (Concerta; Metadate CD)]– Transdermal delivery systems [methylprenidate (Daytrana)]
Volkow ND, et al. Nature 1997;386:827-830.Spencer TJ, et al. Am J Psychiatry. 2006;163:387-395.
Pharmacy Management Issues in the Treatment of ADHD
• Polypharmacy– Combination of long-acting agents– Combination of short-acting agents– Use with modafinil (Provigil), sedative hypnotics, etc.– Different doctors
• Suboptimal dosing– High DACON
• Appropriate use vs. potential for abuse• Off-label use
Recommendations for Managing Polypharmacy
• Polypharmacy– Limit to one long-acting agent at one time (a short-acting in combination could be
allowed)• Methylprenidate (Concerta; Adderall XR) would not be allowed at the same
time – Limit to one short-acting agent at one time (a long-acting in combination could be
allowed)• MPH IR and mixed amphetamine salts would not be allowed at the same time
• Dose optimization– Methylprenidate (Concerta) 18 mg bid → methylprenidate (Concerta) 36 mg qd or
methylprenidate (Concerta) 18 mg qd + MPH IR qd
• Quantity limits– One long-acting agent per day

20
Improving Adherence to Treatment
• 48% of patients 9-15 years of age discontinued therapy over 3 year period1
• Strategies to improve adherence2
• Educate patients and parents regarding anticipated results, benefits and possible adverse events
– Provide frequent follow-up early in treatment– Strive for dose optimization – Identify and treat comorbid conditions
• Dose response vs. titration– Dosing needs to increase when patients get older and their weight increases
1. Wolraith EL, et al. Pediatrics. 2005;115:1734-46.2. Grcevich S, et al. Presented at: The 53rd Annual Meeting of the American Academy of Child and Adolescent Psychiatry; October 2006, San Diego,
CA.
Patient Monitoring Recommended Every 3-4 Months
• Optimal frequency of follow up is not well studied• If intervals longer than 4 months
– Potential for medication to be continued even if its not effective– Potential for medication to be prematurely discontinued or switched to another with
greater potential for side effects
American Academy of Childhood and Adolescent Psychiatry. J Am Acad Child Adolsec Psychiatry 2007;46:894-921.
Monitoring for Adverse Events
• At all visits, patients should be monitored for– Appetite, headache, abdominal pain, sleep, emergence of tics, mood changes,
irritability
• “Rebound” phenomena• Most side effects are responsive to changes in dose or timing
American Academy of Childhood and Adolescent Psychiatry. J Am Acad Child Adolsec Psychiatry 2007;46:894-921.

21
HEDIS ADHD Measure
• Recently developed HEDIS measure for ADHD assesses follow-up care for children (6-12 years) prescribed ADHD therapy
• Initiation Phase Management– Percentage of children with a prescription for ADHD medication who had one
follow-up visit with a practitioner during the 30-day Initiation Phase
• Continuation and Maintenance– Percentage of children with a prescription for ADHD medication, who remained on
the medication for at least 210 days and had at least two follow-up visits in the nine months after the end of the Initiation Phase
National Committee for Quality Assurance. The state of health care quality: Industry trends and analysis. Washington, DC. 2007.
Achievement of the HEDIS ADHD Measure
32% 33%
0%
10%
20%
30%
40%
2005 2006
Perc
ent o
f Pla
ns
National Committee for Quality Assurance. The state of health care quality: Industry trends and analysis. Washington, DC. 2007.
Percent of Commercial Plans Achieving the ADHD Initiation Phase Performance Measure
Achieving the HEDIS ADHD Performance Measure
• Steps to improve performance on the HEDIS ADHD measure include
– Education and implementation of evidence-based care– Registry of patients with current ADHD diagnosis to allow for long-term follow up– Implementation of drug therapy management
• Drug utilization review• Step edits
– Patient education to ensure maximizing adherence

22
Patient Management Plan
Patient Management Plan
Patient Education Materials

23
Physician Education Materials
Summary
• Early and effective treatment minimizes the long-term negative effects of ADHD
– Fewer and less costly emergency department visits– Fewer traffic accidents– Better long term employment prospects
• Treatment choices now include – Longer-acting agents– New delivery systems – Availability of non-stimulants
• New delivery system therapies– Provide continuous treatment of symptoms– Minimize abuse/diversion potential– Enhance adherence
Summary (continued)
• Greater adherence to practice guidelines is needed– Patient and parent education– Frequent monitoring– Optimize dosing and medication choice
• Improvement is needed with patient care follow up– Only 1/3 of all plans achieved the HEDIS performance measure for ADHD– Implement drug therapy management– Establish patient registry– Implement guideline driven care