Embed Size (px)
Citation preview
Implementing Family Team Conferencing
into a System of Care:
Lessons Learned from a Federal GrantRobin Perry, Ph.D.
Toni Spoliansky, B.A.
2015 Florida Child Protection Summit
Orlando, Florida
Friday, September 11This project was funded through the Department of Health and Human Services, Administration for
Children and Families, Children's Bureau, Grant # 90CF0021.
Introductions and
Presentation Objectives
• Presentation objectives– To provide contextual information about Partnership for Strong Families (PSF) and the
awarded federally-funded Family Connections Grant [Family Team Conferencing (FTC)
study]
– To provide an overview of the efforts, processes, protocols, and lessons learned that
contributed to the development of effective working collaborations as part of this FTC study
– To share strategies for effective working collaborations within:
• Model fidelity
• Family involvement and experience with each FTC model
• Organization culture and climate
• Evaluation and outcomes
– To discuss outcome findings and recommendations for FTC practices in Florida
– Partnership for Strong Families- Current FTC practice
Context: Privatization Milestones
1996: Pilot Legislation
1997: 1st CBC-YMCA Children, Youth & Family Services
1999: Statute Mandates Statewide Implementation
Statewide Roll-Out Schedule
Service Contracts for Community-Based Care Organizations by year:
2000 – 2 Contracts
2002 – 3 Contracts
2003 – 5 Contracts
2004 – 9 Contracts
2005 – 3 Contracts
Statewide completion of CBC complete in April 2005
Currently 20 Lead Agencies with Services Contracts
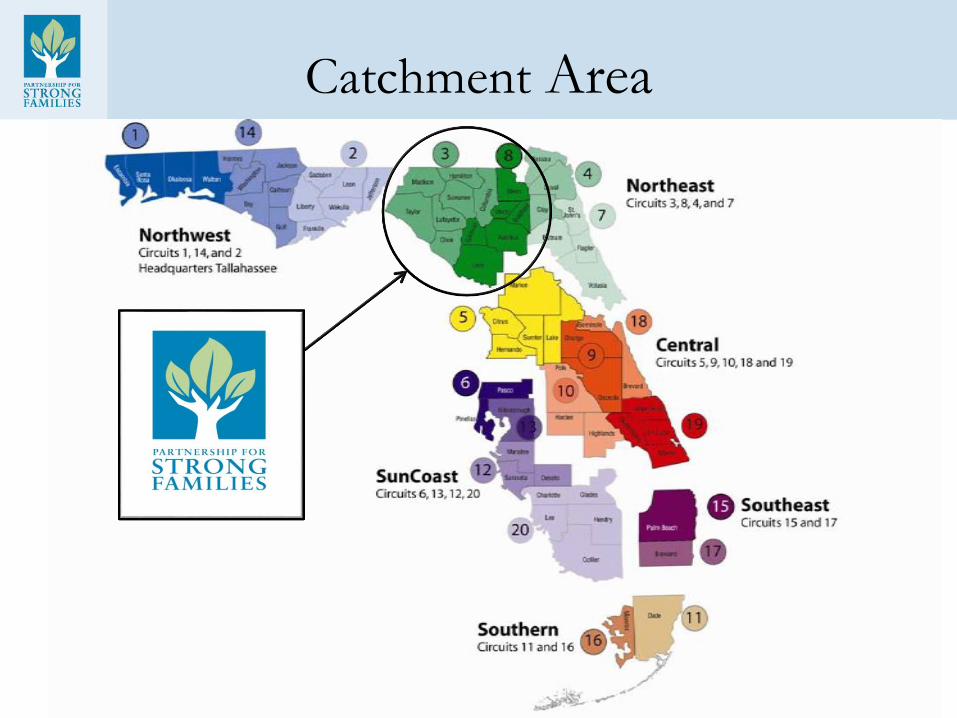
Catchment Area
Partnerships with Community Organizations
• Formal relationships consist of: Sub-recipient
Contracts, Vendor Contracts, Rate Letters
and MOUs
• Primary FTC Collaborations:
– Department of Children and Families
– Case Management Agencies
– Children’s Legal Services
– Guardian ad Litem
– Substance Abuse and Mental Health offices
– Service Providers and Consultants
Pre-Grant Context
• In 2007, Casey Family Programs partners with Florida to explore how to
safely reduce the number of children in care by 50% by 2020.
• In 2008, DCF and PSF staff in C3 and C8 (with technical assistance and
funding provided by Casey Family Programs) began a major system change
initiative called the “Foster Care Redesign” (Redesign).
• The Redesign initially focused: 1) on co-locating PSF staff with Child
Protective Investigator (CPI) staff to improve communication and
coordination; 2) new staff hires to access services for cases diverted from the
formal child welfare system, as well as in-home supervision and shelter cases;
3) new staff hires to coordinate multi-disciplinary decision team staffings to
ensure that a team of professionals was working together to help ensure that
all children who remained in their homes were safe and that those who were
removed were placed with relatives, if possible.
Pre-Grant Context
• While professional team decisions were becoming the norm for
many cases (especially high-risk), an internal examination of
practices suggested: 1) that the family had limited, if any,
involvement in decision making, case planning or ongoing
service provision; 2) re-referral rates in PSF’s service area were
higher than the state average; 3) families were being required to
complete an array of services that were often overwhelming; and
4) non-compliance with case plans was very high.
• Subsequently practice model changes Family Team
Conferencing, Solution Based Casework and Permanency
Roundtables introduced.
FTCs as a Pillar of Service
Partnership for Strong Families’ Pillars of Service include:
• Resource Centers– A hallmark of PSF's system of care is our belief that child
abuse is preventable. We have found that by providing resources and supports to
families in need on the front end, many can avoid reaching the crises that lead to
formal child welfare involvement. Not only is this best for the children, it is a
more cost-effective use of resources.
• The Permanency Roundtable – This program provides support to the
caseworker while taking an in-depth look at helping achieve permanency for
every child in out-of-home care, particularly teenagers who have had a difficult
time obtaining permanent placement solutions.
• Family Team Conferencing – This and other services help reinforce family
values, resolve conflicts, improve communication and provide parents tools to
cope with daily challenges.
Family Connections Grant
• Awarded to Partnership for Strong Families on September 28, 2009
• Grant awarded by the Administration of Children and Families/Children’s
Bureau
• Grant Award = $1.8 million over 3 year period (completed fall 2012)
• Purpose: Demonstration project designed to evaluate Family Team
Conferencing elements leading to a nationwide model
• Six new full-time positions created to facilitate and coordinate Family
Team Conferences
• Population includes In-home Supervision and Shelter Cases
• Each of the three research models include special attention and processes
for cases involving serious domestic violence, substance abuse and/or
mental health issues
Research Model Pathways
FTC as Usual
• Case worker plans and facilitates FTC
• Modeled after pre-grant process
FTC- New
• Grant staff plan and facilitate FTC
• Case worker participates as co-facilitator
• Service providers and family supports encouraged to attend
FTC- New + Family Alone Time
• Same process as FTC- new
• Additional time given where family is able to meet alone, without professionals, to develop their own service and safety plan
FTC Models
The key components of the proposed experimental FTC models are aligned with
the components of FGDM and other types of family meetings that have shown
the most promise or some evidence of success in specific jurisdictions. The key
components include:
• A non-case carrying facilitator who will facilitate each FTC
• The family will be prepared for the FTC
• The extended family and support system will be involved in the FTC
• Key service providers who can meet the family's needs will be involved in the FTC and
provide expedited services
• The family will have alone time to develop their own case plan
• A support person will prepare the victim and attend the FTC when there is domestic
violence involved
• Follow-up FTCs will be conducted at critical junctures throughout the life of each case
Overview of Topic Areas
• Model fidelity– Intake/assignment process
– Adherence to model timelines
– Comparison group FTCs
– Training all staff levels
• Family Involvement – Family alone time
– Empowering families and their
supports to drive the conference
– Parent’s legal counsel
• Org. culture and climate– Leadership support
– Case manager adjustment
– FTC drives case plans
– Tracking systems
• Evaluation and outcome
findings– Principle questions
– Select process evaluation findings
– Select outcome evaluation findings
Model Fidelity
Barrier
• Difficulty with staff following
intake process appropriately
– Intake notifications not sent timely
– Late notification of case initiation
• Ability to complete initial FTCs
within proposed timeframe
– Overwhelming schedules
– Initiating contact with families
– Family schedules
• Comparison group FTCs
– Administering informed consent
– Collecting research material
Solution
• Constant follow-up and reminders
to leadership, supervisory and front
line staff
• Implementation of new scheduling
process
– Helped with timeliness
– Impact: More FTCs without case
manager presence
• Offering of support
– Shadowing and case consultation
– Helpful hints tool and example packet
Model Fidelity
• There were no major modifications to the FTC models
made during project implementation.
• However, one major change to the system as a whole
that had implications for the project was the start of
Solutions Based Casework (SBC).
• Since that time, Florida has introduced a new practice
model-Safety Decision Making Methodology which
incorporates family centered practice and focuses on
standardizing the information collection process and
improving quality and consistency for decision making.
Family Involvement
Barrier
• Families not taking advantage of
Family Alone Time
• Professionals, rather than family,
driving the FTC
– Families are withdrawn, quiet during
FTC
– Professionals come to FTC with own
agenda
– Difficulty getting informal (family
supports) to the FTC
• Opposition from client legal
counsel
– Concern clients will agree to
inappropriate services
Solution
• Addressing/explaining Family
Alone Time at onset of FTC
• Participation of family’s support
system makes big difference
– Best practice to have more family
supports than professionals around the
table
– FTC Coordinators research case to
determine which informal supports
would be appropriate to participate
• Inclusion of defense attorneys
– Invitations to FTC, where appropriate
– Processes implemented in response to
some attorneys reluctance to allow
clients participation in FTCs
Organizational Culture and Climate
• Leadership support
– Executive leadership buy in
– Leading by example
• Case Manager adjustment
– Professional case manager
approach to family centered
approach
– Scheduling/ FTC champions
– Permanency staffing timelines
– Frequency and length of FTCs
• FTC drives Case Plans
– Family now has a say in
services
– Build on strengths to address
needs
• Tracking systems
– Implemented and improved
tracking systems
– Process streamlined across
service sites
– P-Kids
Evaluation
Principal Main Process Evaluation Questions:
• Was the FTC model implemented with fidelity?
• To what extent were linkages made between
community partners?
• To what extent were family members involved
in the FTC process; did families have a real
voice in the process?
Evaluation
Principal Main Process Evaluation Questions:
• What was the role of the Family Service
Facilitator (FSF), Family Team Conference
Coordinator and primary caseworker/Family
Care Counselor in the FTC?
• Did the availability (or lack thereof) of
community resources impact the FTC process?
Evaluation
Principal Outcome Evaluation Questions:
• To what extent did each FTC model impact
removal or re-entry into foster care for In-Home
Supervision cases?
• To what extent did each FTC model meet the
needs of children and parents/caregivers?
• Did the FTC model affect the rates of
reunification, guardianship and permanent
placement with relatives?
Evaluation
Principal Outcome Evaluation Questions:
• Does immediate engagement with families and
engagement throughout the life of the case lead
to desired outcomes for children and families?
• Does utilizing a separate entity to exclusively
provide FTCs impact child and family
outcomes?
• Does a skilled approach (using specially trained
staff) to connecting families to services impact
child and family outcomes?
Evaluation
Study Participants and Primary Data Sources/Tools
Families/children (in conjunction with each FTC):
• Goal Attainment Scale (GAS)
• Protective Factors Survey (PFS)
• Strengths and Difficulties Questionnaire (SDQ)
• Questionnaire for Family Members and Professionals
(QFMP)
• Focus groups and interviews
• Independent observation of randomly selected FTCs
Evaluation
Study Participants and Primary Data Sources/Tools
Family supports*:
• Questionnaire for Family Members and Professionals (QFMP)
*Family supports are other family members, friends or family advocates who are invited by the
family to participate in the FTC.
Professionals:• Questionnaire for Family Members and Professionals (QFMP)
• Key informant interviews of randomly selected Family Care Counselors and FTC Facilitators
• Independent observations of FTCs in all pathways
• Focus groups with community partners/professionals
• Survey of community partners/professionals
Evaluation
Secondary Data Sources
• Florida Department of Children and Families’
Florida Safe Families Network (FSFN), the
SACWSIS system for Florida
• Partnership for Strong Families’ P-Kids Data
System (service utilization and case monitoring
database)
Population and Sample Info.
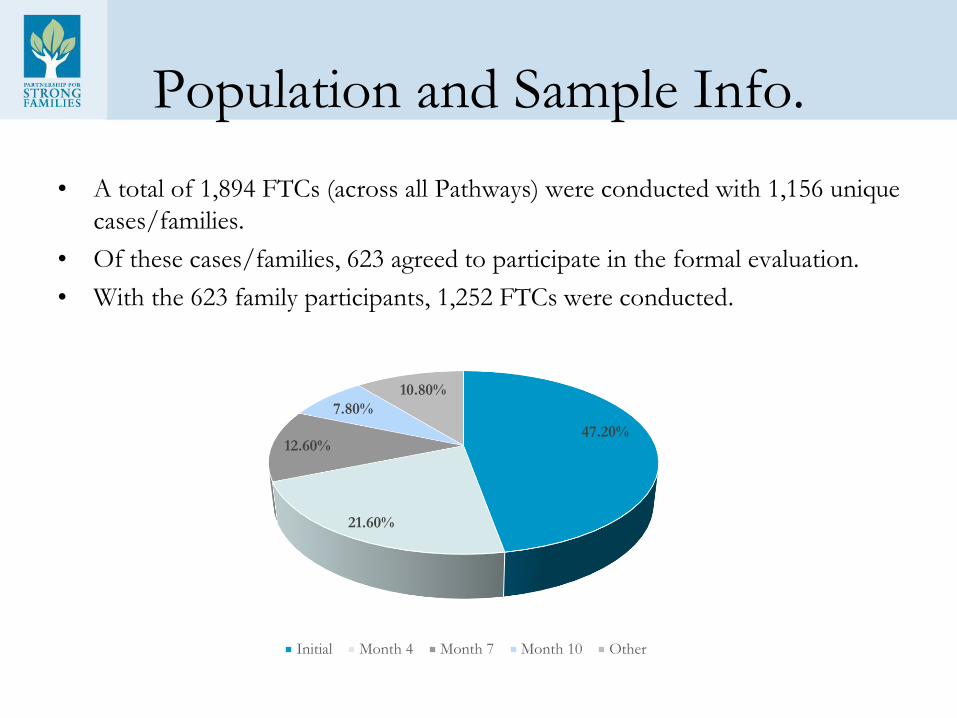
• A total of 1,894 FTCs (across all Pathways) were conducted with 1,156 unique
cases/families.
• Of these cases/families, 623 agreed to participate in the formal evaluation.
• With the 623 family participants, 1,252 FTCs were conducted.
47.20%
21.60%
12.60%
7.80%
10.80%
Initial Month 4 Month 7 Month 10 Other
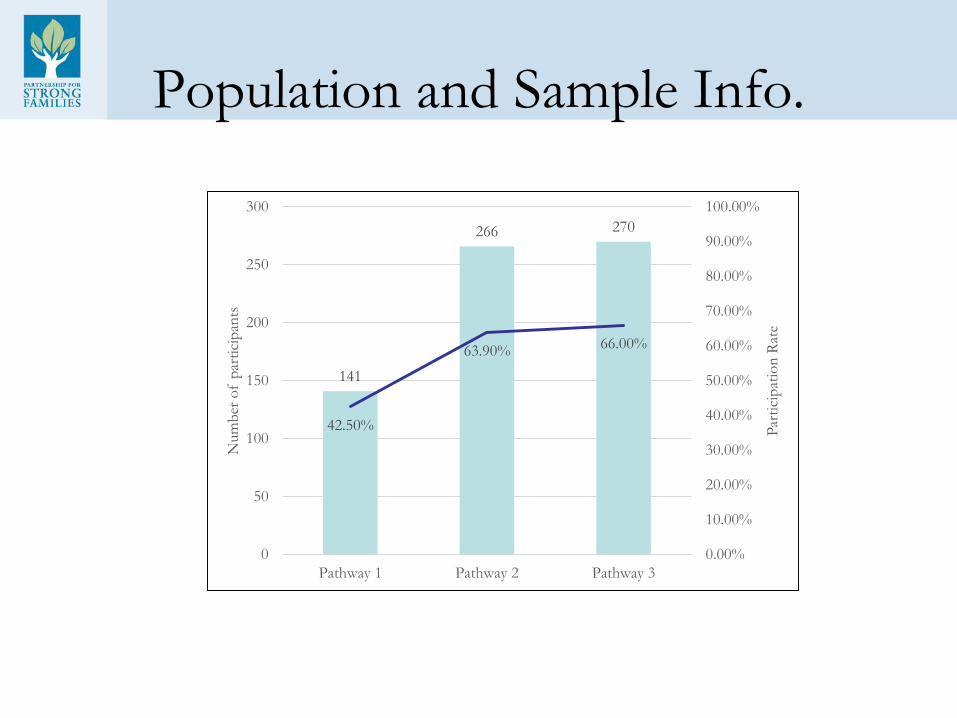
Population and Sample Info.
141
266 270
42.50%
63.90% 66.00%
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
100.00%
0
50
100
150
200
250
300
Pathway 1 Pathway 2 Pathway 3
Par
tici
pat
ion
Rat
e
Num
ber
of
par
tici
pan
ts
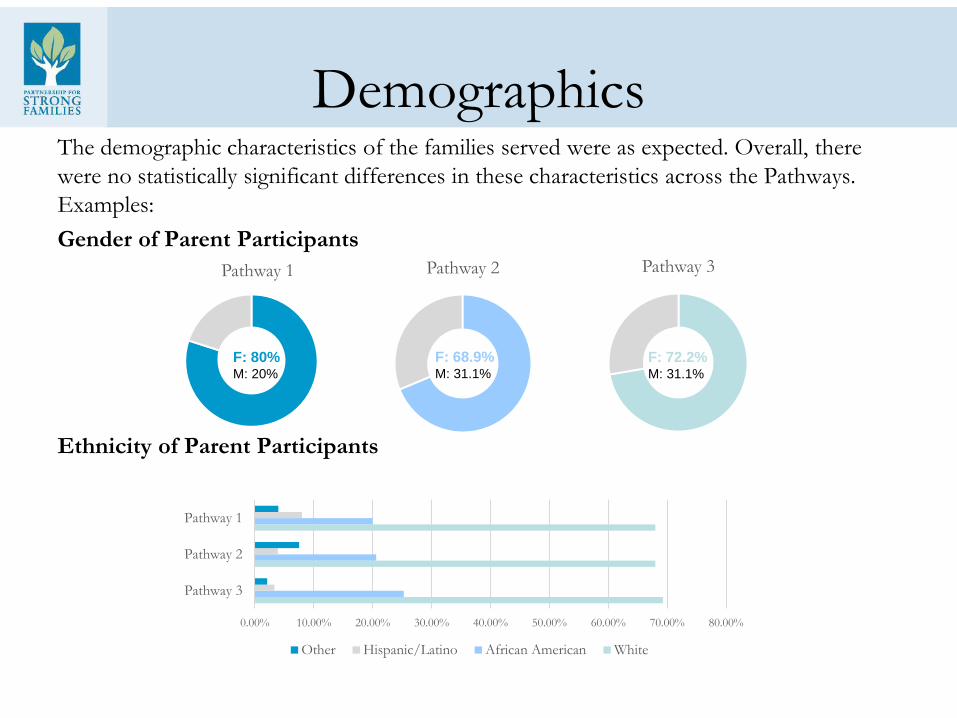
DemographicsThe demographic characteristics of the families served were as expected. Overall, there
were no statistically significant differences in these characteristics across the Pathways.
Examples:
Gender of Parent Participants
Ethnicity of Parent Participants
Pathway 1 Pathway 2
F: 68.9%M: 31.1%
Pathway 3
F: 72.2%M: 31.1%
F: 80%M: 20%
0.00% 10.00% 20.00% 30.00% 40.00% 50.00% 60.00% 70.00% 80.00%
Pathway 3
Pathway 2
Pathway 1
Other Hispanic/Latino African American White
Demographics
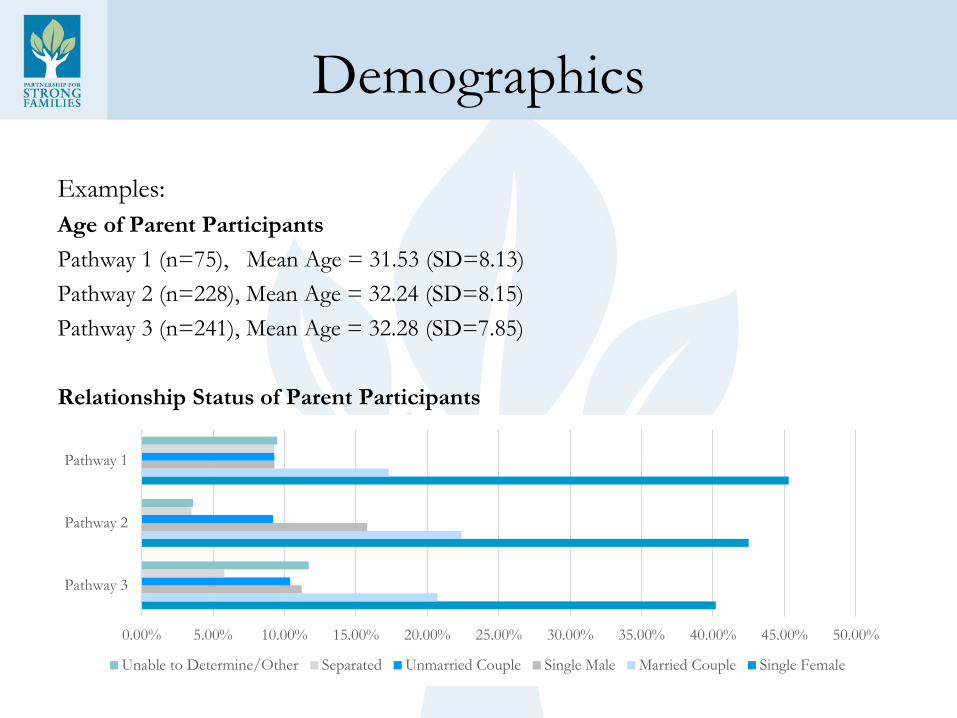
Examples:
Age of Parent Participants
Pathway 1 (n=75), Mean Age = 31.53 (SD=8.13)
Pathway 2 (n=228), Mean Age = 32.24 (SD=8.15)
Pathway 3 (n=241), Mean Age = 32.28 (SD=7.85)
Relationship Status of Parent Participants
0.00% 5.00% 10.00% 15.00% 20.00% 25.00% 30.00% 35.00% 40.00% 45.00% 50.00%
Pathway 3
Pathway 2
Pathway 1
Unable to Determine/Other Separated Unmarried Couple Single Male Married Couple Single Female
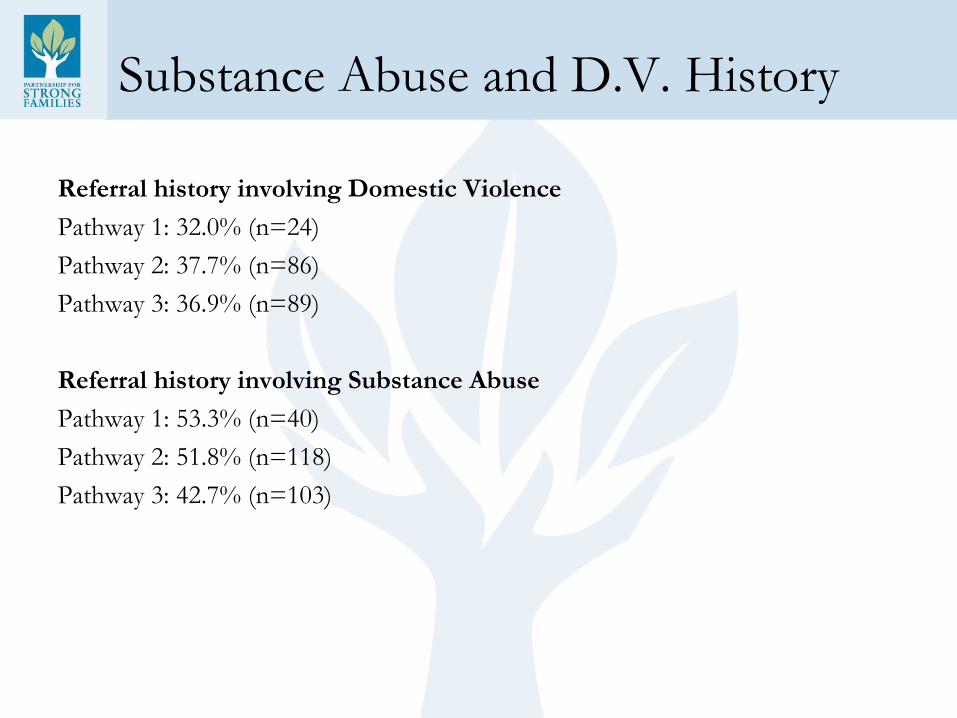
Substance Abuse and D.V. History
Referral history involving Domestic Violence
Pathway 1: 32.0% (n=24)
Pathway 2: 37.7% (n=86)
Pathway 3: 36.9% (n=89)
Referral history involving Substance Abuse
Pathway 1: 53.3% (n=40)
Pathway 2: 51.8% (n=118)
Pathway 3: 42.7% (n=103)
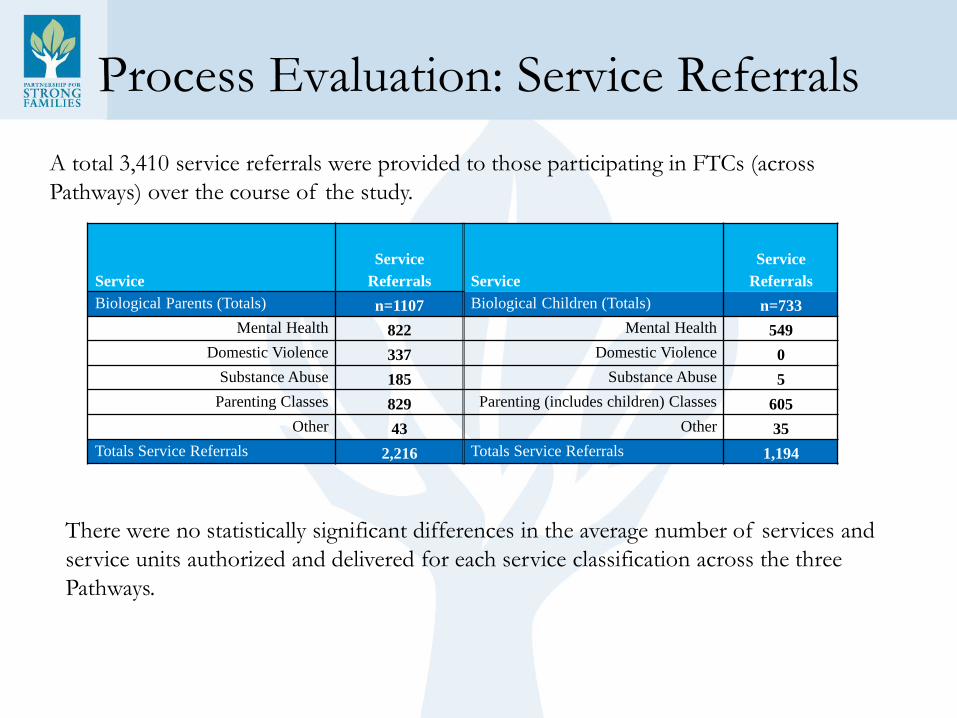
Process Evaluation: Service Referrals
Service
Service
Referrals Service
Service
Referrals
Biological Parents (Totals) n=1107 Biological Children (Totals) n=733
Mental Health 822 Mental Health 549
Domestic Violence 337 Domestic Violence 0
Substance Abuse 185 Substance Abuse 5
Parenting Classes 829 Parenting (includes children) Classes 605
Other 43 Other 35
Totals Service Referrals 2,216 Totals Service Referrals 1,194
A total 3,410 service referrals were provided to those participating in FTCs (across
Pathways) over the course of the study.
There were no statistically significant differences in the average number of services and
service units authorized and delivered for each service classification across the three
Pathways.
Process Evaluation: Service Costs
In total, $1,437,655.13 was spent on referred services for study participants across all three
Pathways.
There are no statistically significant differences in the average expenditures across service
categories for services delivered to cases across FTC Pathways. The greatest expenditures
(and number of cases receiving services) are for mental health services followed by
parenting classes and supports and substance abuse services.
The project cost data suggests that the costs of service are equal across all Pathways in
terms of average service costs (to the system) that result from case plans and service
recommendations. The amount, type and cost of service referrals did not change as a
result of a family’s participation in any FTC Pathway.
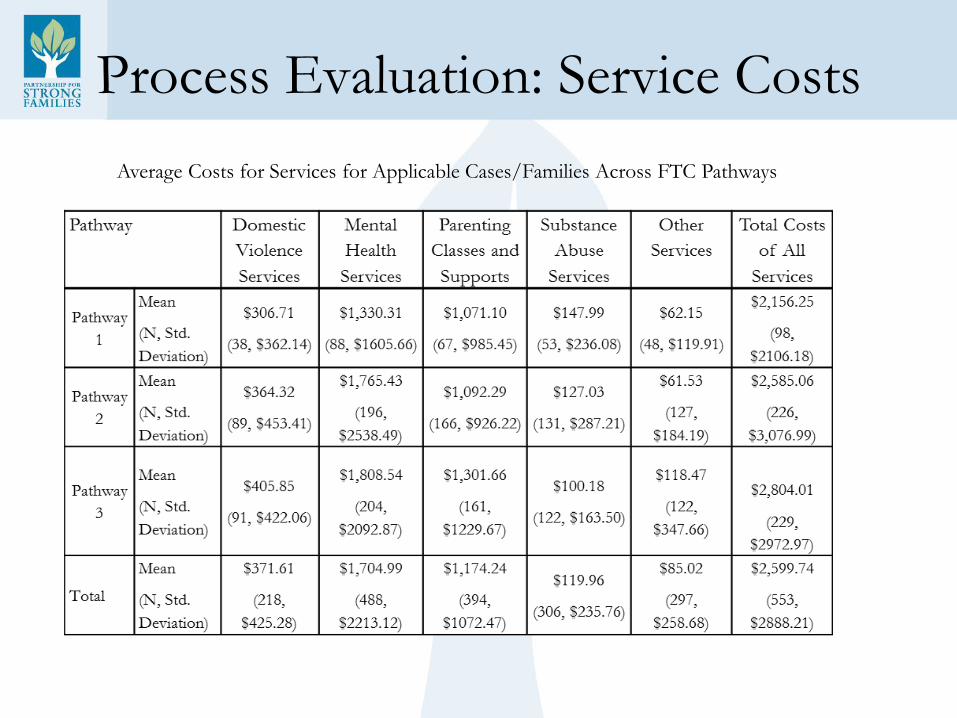
Process Evaluation: Service Costs
Average Costs for Services for Applicable Cases/Families Across FTC Pathways
Process Evaluation: QFMP
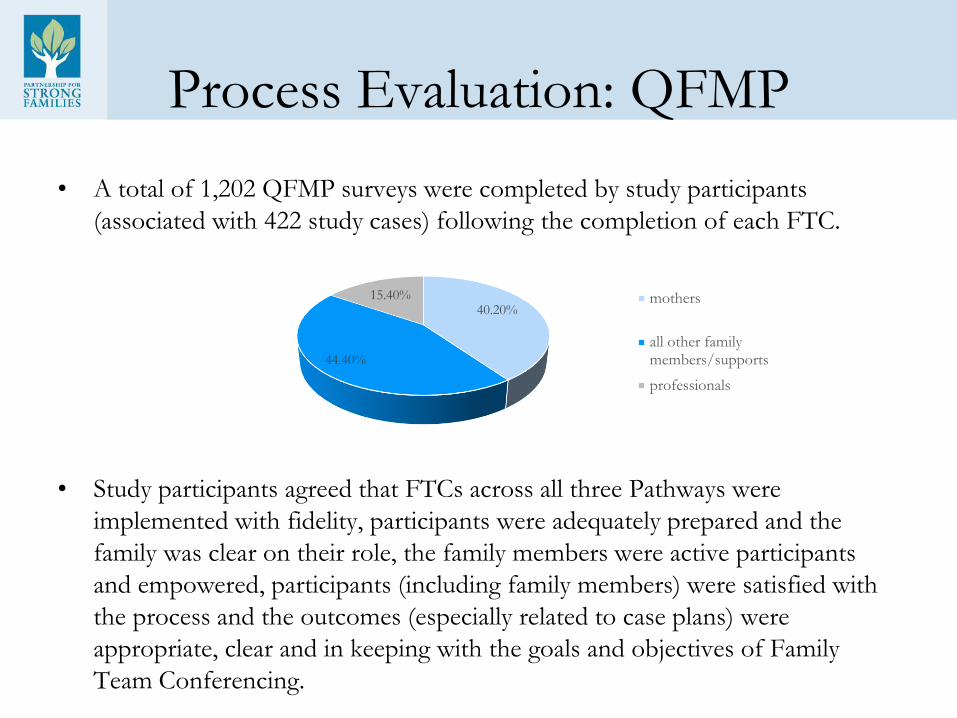
• A total of 1,202 QFMP surveys were completed by study participants
(associated with 422 study cases) following the completion of each FTC.
• Study participants agreed that FTCs across all three Pathways were
implemented with fidelity, participants were adequately prepared and the
family was clear on their role, the family members were active participants
and empowered, participants (including family members) were satisfied with
the process and the outcomes (especially related to case plans) were
appropriate, clear and in keeping with the goals and objectives of Family
Team Conferencing.
40.20%
44.40%
15.40% mothers
all other familymembers/supports
professionals
Process Evaluation: Independent Observations
• Occurred in the early implementation phase of the project
• The FTC Facilitators demonstrate high fidelity to the FTC models with respect to
facilitating the FTCs and engaging families in the decision-making process.
• Some families were not aware of the purpose and goals of the FTC. Also, few families
invited their supports to attend the FTC. There seemed to be inconsistent and at times
insufficient communication about the FTC purpose and goals. As a result of this
finding, the procedures for contacting families and providing more information to
better prepare families for the FTC was revamped.
• Some FCCs were uncertain about their role in the FTC. They were unaware of the
partnership between themselves and the FTC Facilitator in facilitating the FTC. As a
result of this finding, this partnership was emphasized in trainings with FCCs on the
FTC models and grant implementation.
Process Evaluation: Focus Groups
The parents in the focus group responded positively to FTCs, as did the service
providers from both Circuits, but identified glitches in how, when and by whom
FTCs are implemented suggest that a number of improvements could be made
(for example, processes that reinforce the invitation of family supports).
A larger-scale and longer-term area of improvement is the idea of “culture
change” that was raised in the focus groups. Despite promising features of the
FTC models that have been identified from various sources, there is the bigger
challenge of culture change (among FCCs and others to put into practice the
philosophy and approach of FTCs) that is necessary for FTCs to be successful
and sustainable. All in all, the information collected to provide insights into this
challenge suggested that culture change is attainable and that current practices
through FTCs and other means are evidence of culture change.
Process Evaluation: Community Partners Survey
• The Community Partners Survey results showed that service providers
support the FTC philosophy and approach; praise the FTC Facilitators for
their skilled facilitation; believe families are respected during the FTCs and
support greater flexibility in the timeframes for FTCs.
• These positively perceived features, however, were counter-balanced with
perceived challenges to implementation, impact and sustainability of Family
Team Conferencing from the perspective of survey respondents.
• The ambivalence of survey respondents about the impact of FTCs on their
own work and whether a cultural change has occurred to fully promote FTCs
across the entire system presented the need to modify the FTC program to
assure sustainability.
Outcome Evaluation: Protective Factors
• Protective Factors Survey were used to measure and monitor: Family
Functioning/ Resiliency, Social Emotional Support, Concrete Support, Child
Development/Knowledge of Parenting, Nurturing and Attachment.
• A total of 653 Protective Factors Surveys were completed over the course of
the study with 124 (19.0%), 246 (37.7%) and 283 (43.3%) of the sample
associated with Pathway 1, Pathway 2 and Pathway 3 (respectively).
• The vast majority (79.5% or n=519) of these were completed at the baseline
(i.e. Initial FTC) with no follow-up measure. The willingness of study
participants to complete this instrument at follow-up periods was low.
Outcome Evaluation: Protective Factors
• The panel of cases (for which there was a baseline and follow-up
measure[s]) included a total of only 10 Pathway 1 cases, 65
Pathway 2 cases and 59 Pathway 3 cases for which change in
Protective Factors could be measured over time. The very low
follow-up response rate (especially for Pathway 1) does not allow
valid comparisons across Pathways (especially between Pathway
1 with Pathway 2 or Pathway 3).
• For Pathway 2, the protective factor of family functioning
increased over time; for all other scales of the PFS, there were no
statistically significant changes over time. For Pathway 3, there
were no significant changes over time to any protective factor.
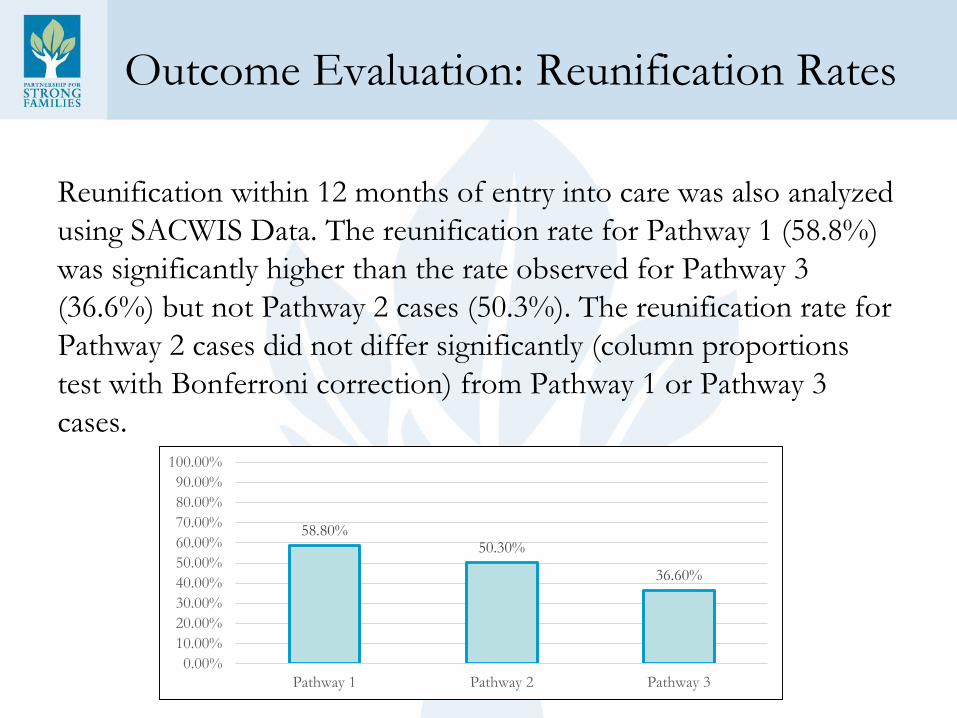
Outcome Evaluation: Reunification Rates
Reunification within 12 months of entry into care was also analyzed
using SACWIS Data. The reunification rate for Pathway 1 (58.8%)
was significantly higher than the rate observed for Pathway 3
(36.6%) but not Pathway 2 cases (50.3%). The reunification rate for
Pathway 2 cases did not differ significantly (column proportions
test with Bonferroni correction) from Pathway 1 or Pathway 3
cases.
58.80%50.30%
36.60%
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
100.00%
Pathway 1 Pathway 2 Pathway 3
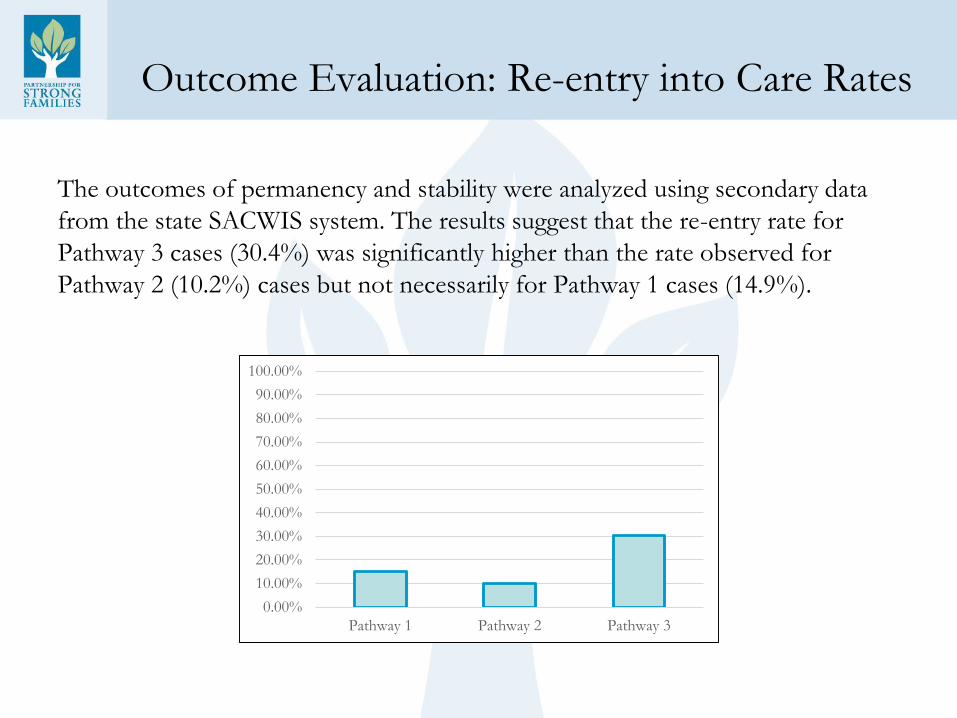
Outcome Evaluation: Re-entry into Care Rates
The outcomes of permanency and stability were analyzed using secondary data
from the state SACWIS system. The results suggest that the re-entry rate for
Pathway 3 cases (30.4%) was significantly higher than the rate observed for
Pathway 2 (10.2%) cases but not necessarily for Pathway 1 cases (14.9%).
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
100.00%
Pathway 1 Pathway 2 Pathway 3
Number of Placements
When the actual number of placements was examined,
there were no significant differences in the average
number (and variance) of placements of children from
Pathway 1 (Mean=1.56, SD=1.094, Range 1-9),
Pathway 2 (Mean=1.63, SD=.893, Range=1-5) and
Pathway 3 (Mean=1.57, SD=1.031, Range=1-8).
Outcome Evaluation: SDQ Results
The Strengths and Difficulties Questionnaire asks about 25
attributes, some positive and others negative that are divided
between 5 scales measuring:
1) emotional symptoms (5 items)
2) conduct problems (5 items)
3) hyperactivity/inattention (5 items)
4) peer relationship problems (5 items)
5) prosocial behavior (5 items)
The first four sub-scores are added together to generate a total
difficulties score.
Outcome Evaluation: SDQ Results
• A total of 1,103 Strengths and Difficulties Questionnaires were completed over the
course of the study. These apply to 617 individual children, who may have been rated
by one or more caregivers at any point in time. In total there were 503
unique/individual caregivers (within 293 unique study cases) that rated 617 unique
children for a total combination of 822 unique child and rater cases. The vast majority
of these ratings were associated with Initial FTCs. When follow-up data is considered,
there are 178 children with multiple measures over time.
• Using panels of cases for available baseline and follow-up scores on the Strengths and
Difficulties Questionnaire, Pathway 2 children were rated as having a significant
reduction in Hyperactivity. The average Total Difficulties scores for Pathway 2
children showed a significant reduction from an average score within the “abnormal”
range to an average score within the “borderline” range. With respect to Pathway 3
children, there was a statistically significant reduction (a positive trend) in the average
scores measuring Emotional Symptoms, Conduct Problems, Hyperactivity and Total
Difficulties.
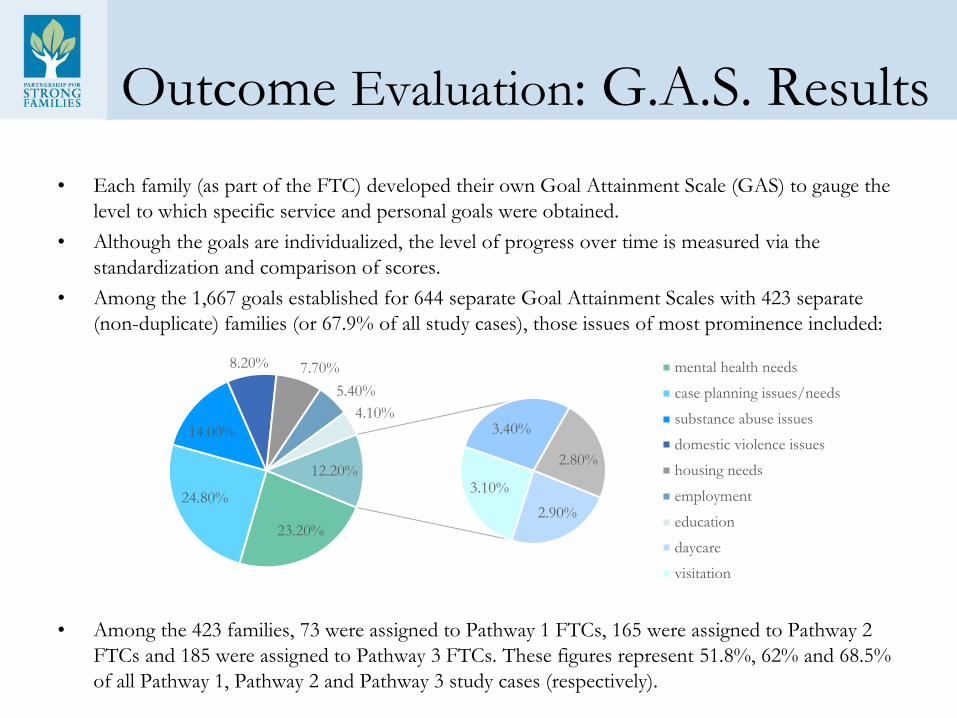
Outcome Evaluation: G.A.S. Results
• Each family (as part of the FTC) developed their own Goal Attainment Scale (GAS) to gauge the
level to which specific service and personal goals were obtained.
• Although the goals are individualized, the level of progress over time is measured via the
standardization and comparison of scores.
• Among the 1,667 goals established for 644 separate Goal Attainment Scales with 423 separate
(non-duplicate) families (or 67.9% of all study cases), those issues of most prominence included:
• Among the 423 families, 73 were assigned to Pathway 1 FTCs, 165 were assigned to Pathway 2
FTCs and 185 were assigned to Pathway 3 FTCs. These figures represent 51.8%, 62% and 68.5%
of all Pathway 1, Pathway 2 and Pathway 3 study cases (respectively).
23.20%
24.80%
14.00%
8.20% 7.70%
5.40%
4.10%
2.90%
3.10%
3.40%
2.80%12.20%
mental health needs
case planning issues/needs
substance abuse issues
domestic violence issues
housing needs
employment
education
daycare
visitation
Outcome Evaluation: G.A.S. Results
• There were 157 families (37.1% of 432) for which
multiple measures using the GAS were available; 15, 66
and 76 families assigned to Pathway 1, 2 and 3
(respectively) are represented in this sub-sample.
• Findings from the Goal Attainment Scale suggest that
Pathway 2 and Pathway 3 cases to have a more
significant impact in moving families toward plan of
care goals. These same effects were not manifested with
Pathway 1 cases (imbalance in sample size).
Recommendations for Future Similar Projects
• Use the dedicated facilitator model (Pathway 2) that separates the primary role
of the FTC Facilitator from the role of the Family Care Counselor.
• Allow for quick/immediate engagement of families regarding the FTC
process.
• Encourage but not require follow-up FTCs.
• Encourage family members to seek and involve family and other supports in
the FTCs and as part of their broader service plan.
• Minimize the role of Family Care Counselors in data collection activities apart
from that which is mandated by state statutes.
• Engage in regular and effective communication between FTC project and
administrative staff and key service providers to help facilitate achievement of
family and case goals.
• Encourage a culture change that embraces the philosophy of FTCs in the day-
to-day practices of FCCs.
Recommendations to the Child Welfare Field
• Consider a staggered introduction of major system or practice
changes over time so that sufficient information regarding the
impact of one intervention or system change can be assessed
before another practice or system change is introduced.
• Have in place a well-structured and user-friendly Management
Information System to monitor and evaluate any newly
introduced practice or system change.
• Be prepared for a major time commitment to changing practice
to involve families in decision making that is genuine and
meaningful.
FSDMM and FTCs- Current Agency Practice
• Current FTC staff includes 2 full time Facilitators and a Department Manager
• FTC practice and timeline is complementary to FSDMM
• The Facilitators are responsible for engaging clients in the FTC planning process, as well as facilitating the meeting
• Case Managers act in a co-facilitator role during the FTC
• FTCs are scheduled to occur within 25 days after PFSF has accepted the case from DCF
• FTC prep staffing occurs 14 days after case transfer and before the FTC is completed
• Follow up FTCs can occur at any time during the case, as requested by the family team
• The family Team is built by the biological family- they choose who is invited to the FTC.
FSDMM and FTCs- Current Agency Practice
• Families are asked if they want to invite CPI and Guardian ad Litem Staff
• Time, date and location is set based on what works best for the family, however it is preferable for the FTC to occur at a neutral location (e.g.: school, church, community center)
• Age appropriate children should be included in the FTC and if they are not present, should be the focus of the goals discussed at the FTC.
• For cases involving Domestic Violence, separate FTCs are offered for both the victim and the aggressor and DV advocates are included if possible.
• Family Alone Time is offered to the family, although is not a
mandatory part of the process
• Exemptions to the FTC process are considered when an FTC is not
possible for the family or the family declines participation

Questions/Comments
5950 NW 1st Place, Suite AGainesville, FL 32607352-244-1500pfsf.org
Partner. Foster. Adopt.
Engaging Families Through Family Team Conferencing Replication Manual
Children’s Bureau Family Connections Grant 2009-2012: Family Team Conference Project
We would like to thank the Department of Health and Human Services, Administration for Children and Families, Children’s Bureau for funding this project. Without their support and guidance, the work outlined in the following pages would not be possible. Also, we would like to thank the Florida Department of Children and Families, the staff of our contracted Case Management Agencies and our numerous service providers and private practitioners. Finally, a special thanks to Dr. Robin Perry of the Institute for Child and Family Services Research, Dr. Jane Yoo of Clarus Research, Mona Gil de Gibaja of United Way of North Central Florida and the grant-funded staff members who participated in this project for their hard work and dedication to this project.
The contents of this manual do not necessarily reflect the views or policies of the Children’s Bureau.
PSF’s Grant Team - From Left to Right:Cherie Watters - FTC Facilitator; Cynthia Reneke - FTC Coordinator; Patricia Murphy - FTC Coordinator; Toni Spoliansky - Project Director; Gillian Nassau - FTC Facilitator; Rhonda Abercrombie - FTC Facilitator
Abstract:
In September 2009, Partnership for Strong Families (PSF) was awarded a $1.8 million grant from the Children’s Bureau to conduct an evaluation of Family Team Conferencing (FTC). The purpose of this research project was to test different approaches of FTC. FTC was already an established part of services provided by PSF, however different models of FTC are practiced and researched elsewhere, and PSF wanted to learn more about these different models and how they could benefit clients within their system of care. The project tested the FTC approach utilized at Partnership for Strong Families prior to receipt of the grant with two alternative models to see if each produced different results or were perceived and valued differently by all participants, especially the family.
The results that were of interest to the study included: increasing child and family safety at home, reducing time frames to achieve permanent homes for children, improving child and family well-being, greater family involvement in case planning and decision making and other service goals and outcomes deemed of value by families working with service providers. In order to test these different models, an experiment had to be conducted. The results of this study were of major importance in helping Partnership for Strong Families evaluate the value of FTC in achieving desired outcomes and improving services with children and families.
Table of Contents:
Section 1: Introduction 1 Project Overview FTC Structure Project Goals
Section 2: Implementation 3 Staff Roles and Responsibilities Implementation Timeline
Section 3: Procedures 6 FTC Intake and Case Assignment Process Family Information Tool Informed Consent and Data Collection Family Plans and FTC Exemptions
Section 4: What we discovered 9 Process Evaluation Outcome Evaluation Discussion and Results
Section 5: Dissemination Activities 14
Section 6: Appendices 16 Family Information Tool Protective Factors Survey Strengths and Difficulties Questionnaire Goal Attainment Scale Questionnaire for Family Members and Participants Family Plan FTC Exemption Form FTC Brochure
PSF-Partnership for Strong Families * FTC-Family Team Conference * FCC-Family Care Counselor * CPI-Child Protective InvestigatorEE-Early Engagement * GAL-Guardian ad Litem * FSF-Family Service Facilitator * DCF-Department of Children and Families

Section 1: Introduction
Florida’s Child Welfare System:
Florida’s provision of child protective services is unlike any other system in the nation. In 1998, the Florida legislature made the bold decision to move toward privatization of most child welfare functions, handing them over to nonprofit organizations in local communities. This transformation was completed in 2003. Today, 19 Community-Based Care agencies across the state are responsible for the provision of services ranging from child abuse prevention and protective supervision all the way to foster care and adoption. The Department of Children and Families still maintains the oversight, contract management, abuse hotline and initial investigations of abuse.
Privatization has enabled Florida to go from being of the worst performing in the nation in terms of child welfare outcomes to being one of the top performers whom other systems are trying to emulate. It has also opened the door for innovation, both at a community and a state level. Perhaps one of the best examples has been the increased ability for Community-Based Care agencies like Partnership for Strong Families to obtain grants such as the one funding this project, where best practice models can be developed and implemented. Systemic change in the last decade has been dramatic, but there is still work to do.
Project Overview:
The Family Connections Grant, titled Engaging Families through Family Team Conferencing, was awarded to Partnership for Strong Families September 28, 2009, by the Federal Government (Administration of Children and Families). Federal funding provided $1.2 million over a 3 year period (with a $600,000 agency match). The project’s purpose was designed to evaluate Family Team Conferencing elements leading to a nationwide model. The project focused on a random sample of over 700 families from the 13 counties comprising our catchment area who are receiving case management services. PSF’s catchment consists of Alachua, Baker, Bradford, Columbia, Dixie, Gilchrist, Hamilton, Levy, Lafayette, Madison, Suwannee, Taylor and Union Counties (please insert map of catchment area within Florida). All In-home Supervision and Shelter Cases were considered for inclusion in the study. Two experimental models were compared to a control model of Family Team Conferencing. The control model, FTC as usual, left the responsibility of planning and facilitating the FTC to the Family Care Counselor. This is the manner in which FTCs were conducted prior to the receipt of the Grant. The first experimental model, FTC- New, provided designated, trained staff to plan and facilitate the FTC. The second experimental model also provided the specialized staff and added a component of Family Alone Time to the FTC. Please see the chart on next page for a better detailed comparison of the three FTC models, as well as what the structure of an FTC looks like.
What is Family Alone Time?Family Alone Time is a part of the second experimental FTC model, where the core members of the family are given as much time as they need to meet, without professional involvement, to discuss case planning activities during the FTC. This practice is based on the Family Group Decision Making (FGDM) model. Family alone time can include non-blood relatives if the other members of the group agree to their inclusion.
PSF-Partnership for Strong Families * FTC-Family Team Conference * FCC-Family Care Counselor * CPI-Child Protective InvestigatorEE-Early Engagement * GAL-Guardian ad Litem * FSF-Family Service Facilitator * DCF-Department of Children and Families
1
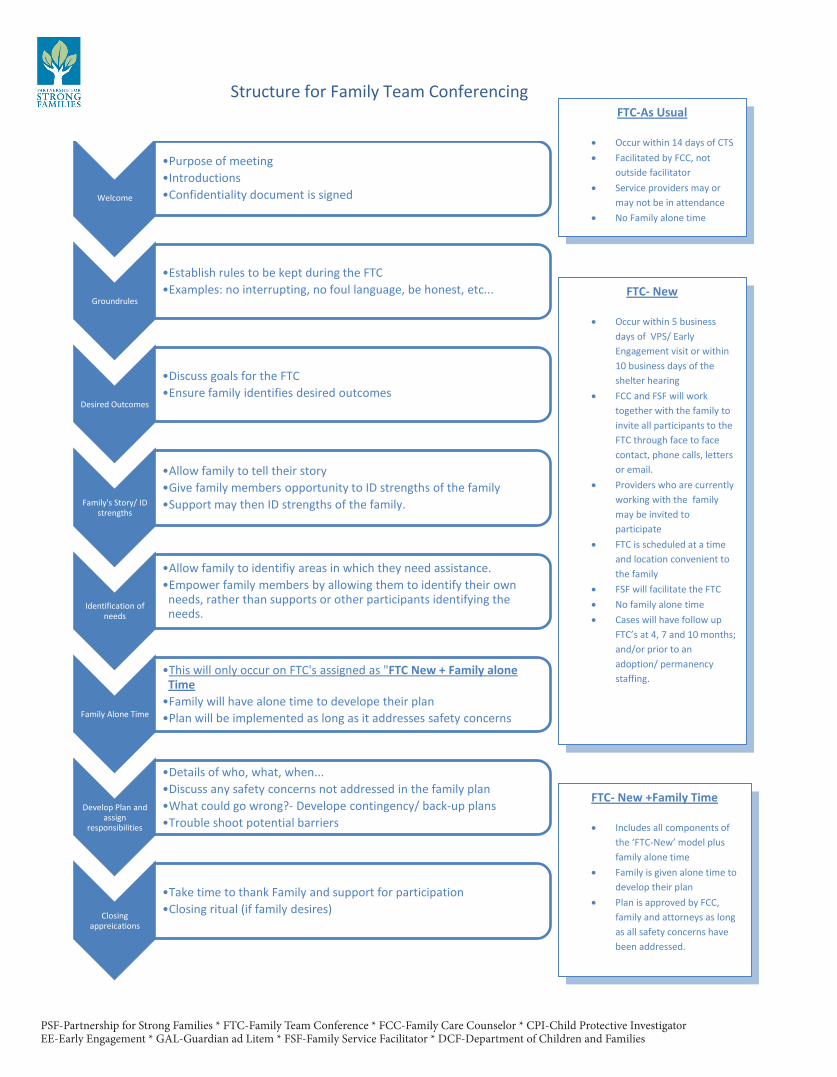
Welcome
•Purpose of meeting•Introductions•Confidentiality document is signed
Groundrules
•Establish rules to be kept during the FTC•Examples: no interrupting, no foul language, be honest, etc...
Desired Outcomes
•Discuss goals for the FTC•Ensure family identifies desired outcomes
Family's Story/ ID strengths
•Allow family to tell their story•Give family members opportunity to ID strengths of the family•Support may then ID strengths of the family.
Identification of needs
•Allow family to identifiy areas in which they need assistance.•Empower family members by allowing them to identify their own
needs, rather than supports or other participants identifying the needs.
Family Alone Time
•This will only occur on FTC's assigned as "FTC New + Family alone Time•Family will have alone time to develope their plan•Plan will be implemented as long as it addresses safety concerns
Develop Plan and assign
responsibilities
•Details of who, what, when...•Discuss any safety concerns not addressed in the family plan•What could go wrong?- Develope contingency/ back-up plans•Trouble shoot potential barriers
Closing appreications
•Take time to thank Family and support for participation•Closing ritual (if family desires)
Structure for Family Team Conferencing FTC-As Usual
• Occur within 14 days of CTS • Facilitated by FCC, not
outside facilitator • Service providers may or
may not be in attendance • No Family alone time
FTC- New
• Occur within 5 business days of VPS/ Early Engagement visit or within 10 business days of the shelter hearing
• FCC and FSF will work together with the family to invite all participants to the FTC through face to face contact, phone calls, letters or email.
• Providers who are currently working with the family may be invited to participate
• FTC is scheduled at a time and location convenient to the family
• FSF will facilitate the FTC • No family alone time • Cases will have follow up
FTC’s at 4, 7 and 10 months; and/or prior to an adoption/ permanency staffing.
FTC- New +Family Time
• Includes all components of the ‘FTC-New’ model plus family alone time
• Family is given alone time to develop their plan
• Plan is approved by FCC, family and attorneys as long as all safety concerns have been addressed.
PSF-Partnership for Strong Families * FTC-Family Team Conference * FCC-Family Care Counselor * CPI-Child Protective InvestigatorEE-Early Engagement * GAL-Guardian ad Litem * FSF-Family Service Facilitator * DCF-Department of Children and Families

Project Goals and Objectives:
Goal:To respectfully engage families in decision-making and case planning through a strength-based, family-centered, culturally appropriate system of care that includes initial and ongoing Family Team Conferences for every new in-home supervision and shelter (removal) case.
Objectives:1. Hire and train four full-time Family Service Facilitators (FSF) who will serve as the facilitators
for all initial and ongoing FTCs for a random sample of new in-home supervision and shelter cases. Hire two full-time Family Team Conference Coordinators to help coordinate all of the planning and logistics for the FTCs.
2. Ensure meaningful participation in case planning and decision-making of families participating in an initial and ongoing FTC.
3. Increase participation of children and extended family members in initial and ongoing FTCs for families with new in-home supervision or shelter cases.
4. Increase participation of service providers at initial and ongoing FTCs who can meet the immediate and ongoing needs of families with new in-home supervision or shelter cases.
5. Ensure expedited services are provided to all of the families who participate in initial FTCs.6. Improve Goal Attainment Scale score for the families who participate in an initial and ongoing
FTC (measured by completing and monitoring the Goal Attainment Scale).7. Increase protective factors for the families who participate in an initial and ongoing FTC
(measured by administering the Protective Factors Survey).8. Reduce re-referral rates among families who have received an
initial and ongoing FTC.
Section 2: Implementation
Staff Roles and Responsibilities:
Project Director:• Provides day-to-day management of operations related to the project• Receives notification of case assignment from designated point of contact for each service site• Enters case information into data management system for tracking of assignments and due dates• Through random assignment, determines which type of FTC will be designated to the case• Assigns FTC to Coordinator and Facilitator staff• Manages and cleans data to be provided to evaluation team• Manages quality assurance and project fidelity• Ongoing communication and collaboration with IT and Finance departments• Participates in Grant Operations Team• Troubleshoots any barriers• Mentors FTC staff for purposes of training and certification• Provides ongoing support and training to FTC staff
PSF-Partnership for Strong Families * FTC-Family Team Conference * FCC-Family Care Counselor * CPI-Child Protective InvestigatorEE-Early Engagement * GAL-Guardian ad Litem * FSF-Family Service Facilitator * DCF-Department of Children and Families 3
FTC Facilitator:• Reviews available case information upon assignment of an FTC• Communicates with FTC coordinator regarding participants and attendance confirmations• Facilitates Family Team Conferences to engage the family and assist in the development of an
appropriate family plan• Maintains integrity of the Family Team Conference process• Ensures Family Plan is completed • Addresses any safety concerns• Ensures all participants have signed plan• Assists families in completing some of the grant-required evaluation tools (Goal Attainment
Scale, Protective Factors Survey and the Strengths and Difficulties Questionnaire)• Recommends services for family based on needs identified during FTC• Maintains information regarding the services available in the family’s area • Authorizes service allocation and coordinates service delivery with providers and community
resources• Oversees the authorization and utilization of services to ensure resources are maximized• Fosters relationships with service providers, hospitals, courts, education system, Domestic
Violence and Substance Abuse & Mental Health agencies • Participates in staff meeting and coordinates activities between various stakeholders within the
System of Care
FTC Coordinator:• Responsible for all logistical planning of FTC, including:• Coordinate date and time of FTC• Engage and invite all attendees to participate in FTC• Consider the need for professional staff to be in attendance• Coordinate the schedules of all FTC attendees• Reserve a location for the conference that is safe and allows for open dialogue • Address need for and arrange daycare services, in the situation in which the children of the
family are not able to attend the FTC• Organize the research materials and appropriate forms to be completed at each FTC• Input data associated with FTC in the appropriate PSF data management systems (P-Kids, FSFN)• Export data from data management systems for tracking and performance measures• Ensure evaluation materials are stocked, organized, and well maintained• Participate in staff meetings to address any concerns associated with the project• Link with professional staff to ensure appropriate attendance by domestic violence, substance
abuse and mental health experts as needed
Training StrategiesOngoing training was offered to PSF and partner agency staff throughout the entire grant period. Trainings occurred with new case management staff on a semi-annual basis and as requested by management staff. Nearly 20 formal trainings, in addition to informal discussions, took place during the three year grant period. Each case manager who completed the training was provided with an ‘FTC Grant’ binder, which contained helpful hints, necessary paperwork and procedural information.
PSF-Partnership for Strong Families * FTC-Family Team Conference * FCC-Family Care Counselor * CPI-Child Protective InvestigatorEE-Early Engagement * GAL-Guardian ad Litem * FSF-Family Service Facilitator * DCF-Department of Children and Families
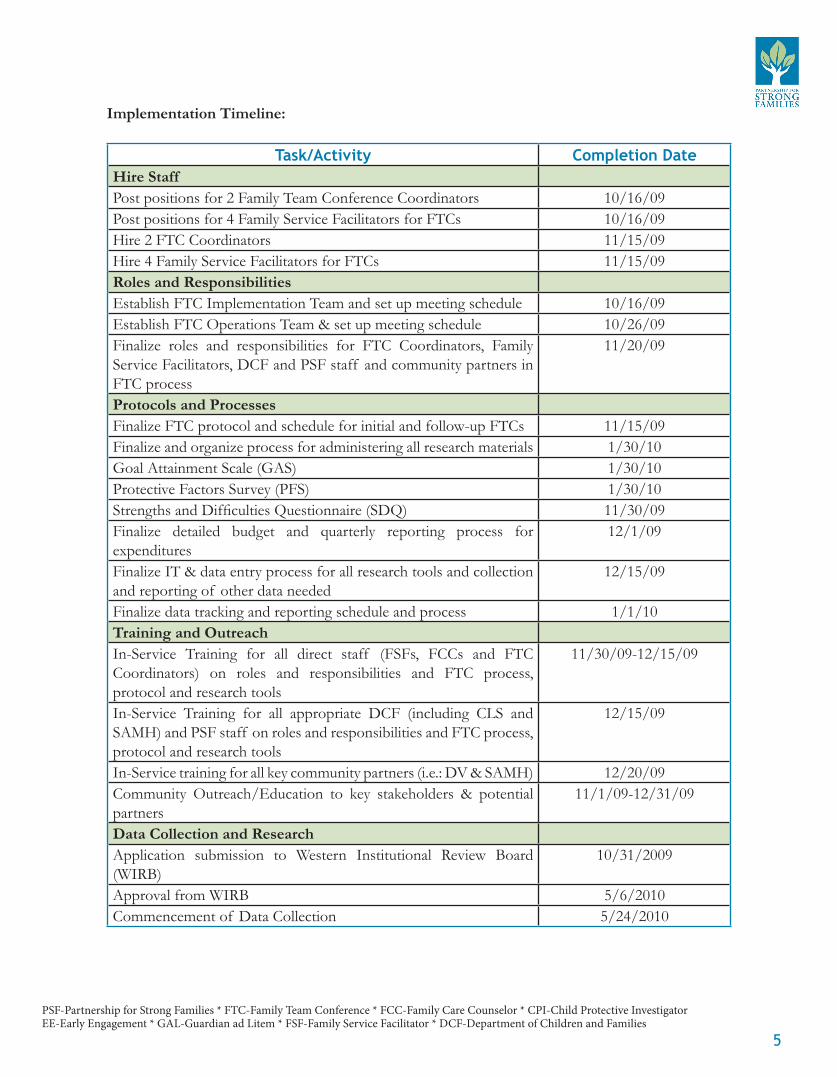
Implementation Timeline:
Task/Activity Completion DateHire StaffPost positions for 2 Family Team Conference Coordinators 10/16/09Post positions for 4 Family Service Facilitators for FTCs 10/16/09Hire 2 FTC Coordinators 11/15/09Hire 4 Family Service Facilitators for FTCs 11/15/09Roles and ResponsibilitiesEstablish FTC Implementation Team and set up meeting schedule 10/16/09Establish FTC Operations Team & set up meeting schedule 10/26/09Finalize roles and responsibilities for FTC Coordinators, Family Service Facilitators, DCF and PSF staff and community partners in FTC process
11/20/09
Protocols and ProcessesFinalize FTC protocol and schedule for initial and follow-up FTCs 11/15/09Finalize and organize process for administering all research materials 1/30/10Goal Attainment Scale (GAS) 1/30/10Protective Factors Survey (PFS) 1/30/10Strengths and Difficulties Questionnaire (SDQ) 11/30/09Finalize detailed budget and quarterly reporting process for expenditures
12/1/09
Finalize IT & data entry process for all research tools and collection and reporting of other data needed
12/15/09
Finalize data tracking and reporting schedule and process 1/1/10Training and OutreachIn-Service Training for all direct staff (FSFs, FCCs and FTC Coordinators) on roles and responsibilities and FTC process, protocol and research tools
11/30/09-12/15/09
In-Service Training for all appropriate DCF (including CLS and SAMH) and PSF staff on roles and responsibilities and FTC process, protocol and research tools
12/15/09
In-Service training for all key community partners (i.e.: DV & SAMH) 12/20/09Community Outreach/Education to key stakeholders & potential partners
11/1/09-12/31/09
Data Collection and ResearchApplication submission to Western Institutional Review Board (WIRB)
10/31/2009
Approval from WIRB 5/6/2010Commencement of Data Collection 5/24/2010
PSF-Partnership for Strong Families * FTC-Family Team Conference * FCC-Family Care Counselor * CPI-Child Protective InvestigatorEE-Early Engagement * GAL-Guardian ad Litem * FSF-Family Service Facilitator * DCF-Department of Children and Families
5
Section 3: Procedures
FTC Intake and Case Assignment Process:
1. Child Protective Investigator (CPI) commences investigation2. CPI staffs case with Decision Team Consultant at a decision team staffing or appropriate team
meeting and determines if ongoing case management is necessary. Case progresses to either: a) In-home supervision b) Shelter
3. CPI sends e-mail to ‘[email protected]’ with the following information: a) Name of the case b) Tentative Early Engagement (EE) date for in-home supervision cases or shelter date for court cases c) Abuse report number d) City and County of location
4. Project Director inputs information into P-Kids a) P-Kids randomly assigns which FTC path the case will receive b) Project Director assigns FTC to facilitator and coordinator
5. Case Management Program Director assigns case to unit supervisor and Family Care Counselor (FCC) and notifies Project Director of assignment
6. Guardian Ad Litem (GAL) program assigns staff or volunteer guardian and notifies FCC and assigned FTC coordinator
Note: Steps 4, 5 and 6 occur simultaneously in this process7. Case Management Program Director, GAL staff member and Project Director communicate
with each other (via e-mail) which staff have been assigned to the case8. Project Director sends e-mail to assigned FTC Facilitator and Coordinator, notifying them of
the case assignments. Copied on this e-mail notification are: a) Family Care Counselor assigned to manage the case b) Case Management Program Director and FCC Supervisor c) Child Protective Investigator involved on the case d) GAL assigned or Senior AA of the GAL program if guardian is not yet assigned
9. Initial staffing occurs for shelter cases (these staffing notes along with DTC notes should be obtained)
10. Joint Early Engagement visit occurs for in-home supervision cases
11. FTC coordinator, facilitator and FCC begin communication regarding the case info, participants involved and FTC elements
12. FTC coordinator begins the scheduling process and notifies both the FCC, GAL and Facilitator of any barriers
13. Finalized conference time and location is sent by Coordinator to all involved in the case and clearly denotes who has been invited to the conference
14. FCC and/or FTC Facilitator complete Strength and Difficulties Questionnaire (SDQ) and Protective Factors Survey (PFS) with family prior to initial FTC (can be done at the location of
PSF-Partnership for Strong Families * FTC-Family Team Conference * FCC-Family Care Counselor * CPI-Child Protective InvestigatorEE-Early Engagement * GAL-Guardian ad Litem * FSF-Family Service Facilitator * DCF-Department of Children and Families
the FTC prior to the start of the FTC)15. FTC occurs with FCC and Facilitator (and all other individuals invited by the family). The GAL
program is discussed at FTC if assigned GAL is not present. The FTC occurs: a) Within 5 business days of initial joint visit (in-home supervision cases) b) Within 10 business days of shelter hearing (shelter cases)
16. FCC and/or FTC Facilitator complete Goal Attainment Scale (GAS) that aligns with family plan 17. Two week follow-up staffing occurs with Quality Operations Manager18. FTC Facilitator completes two week follow-up call with family to address barriers and engagement
*No formal data collection for grant in this step19. FCC completes first progress update of Goal Attainment Scale (GAS), which is completed
within 30 days of Initial FTC
Family Information Tool (FIT):
FTC Coordinators used the Family Information Tool (FIT) to help organize case information when planning an FTC. The FTC Facilitators used this completed form to assist with their preparation for the FTC. The FIT included case participants, demographic and contact information, as well as pertinent case information such as abuse/neglect allegations, prior reports and safety concerns. Special considerations regarding transportation, child care and visitation were also noted on the FIT. Additionally, family and individual needs, as identified in previous staffing, were also outlined on the FIT. A full copy of the FIT document can be found in the Appendix section of the manual.
Informed Consent and Data Collection:
Prior to the beginning of an initial FTC, clients are asked whether or not they would like to participate in the FTC research study. The FCC and/or FTC Facilitator explains the informed consent document, explaining to the family that their participation is voluntary and that they will have access to an FTC and services regardless of whether or not they consent. The family is also informed that there is no monetary reward for participation as well as no foreseeable risk in participating. Families are given the opportunity to review the entire document, which is written at a 4th grade reading level, before making their choice to consent or not. Regardless of their choice, the FTC is completed. If the family consents, the Protective Factors Survey, Strengths and Difficulties Questionnaire, Goal Attainment Scale and Questionnaire for Family Members and Participants are administered before and after the FTC. If the family declines participation in the research study, these instruments are not administered. Copies of these instruments can be found in the Appendix section of this manual.
Quality Assurance Process for Informed Consents and Data Collection:
1. Informed Consent is obtained prior to the Family Team Conference (FTC) and reviewed by the assigned FTC Facilitator/Family Care Counselor (FCC) to ensure it is signed appropriately
2. Prior to the dissemination of any instruments, the FTC Facilitator/FCC will verify based on completed Informed Consent documents who is to receive which instrument(s)
PSF-Partnership for Strong Families * FTC-Family Team Conference * FCC-Family Care Counselor * CPI-Child Protective InvestigatorEE-Early Engagement * GAL-Guardian ad Litem * FSF-Family Service Facilitator * DCF-Department of Children and Families
7
3. Upon completion of the FTC, assigned FTC Facilitator and/or FCC verifies that all research instruments have been completed by the client as appropriate
a) This verification is to occur prior to all parties leaving the FTC b) If the research instruments are incomplete, the FTC Facilitator and/or FCC will ensure that all necessary corrections are made
4. Assigned FTC Facilitator and/or FCC submit the signed Informed Consents and completed research instruments to the assigned FTC Coordinator for data entry
5. Assigned FTC Coordinator reviews the Informed Consents and research instruments to verify they are complete and appropriately signed
a) If they are not complete or appropriately signed, the FTC Coordinator notifies the assigned FTC Facilitator/FCC of the error b) The assigned FTC Facilitator, FCC and FTC Coordinator work together to contact the client, as necessary, to obtain missing signatures/missing information c) If missing signature on the Informed Consent is unable to be collected, the associated client will not be counted as part of the research pool
6. Upon verification that the Informed Consent and research materials are complete, the FTC Coordinator inputs the data into P-Kids and scans the Informed Consent and research material packet into PSF’s secure electronic record keeping system
7. Monthly, the Project Director and FTC Coordinators review documents in the secure electronic record keeping system to ensure that data entered into P-Kids matches information electronically filed in the record system
8. If information in P-Kids does not match what is filed in the secure electronic record keeping system, steps will be taken to ensure data in P-Kids is corrected
9. Documentation of all changes is kept in a data cleaning log
Family Plans:
The Family Plan is the document produced as a result of the FTC. The Family Plan includes a list of the family’s strengths as well as individual and family level needs that are identified at the FTC. The Family Plan also outlines steps to be taken and person(s) responsible to address the identified needs. Participants sign the Family Plan, acknowledging their identified responsibilities and agreeing to confidentiality. The Family Care Counselor uses the Family Plan as a basis for writing the court approved Case Plan (for cases with court involvement). For in-home supervision cases, the Family Plan is used as the Case Plan. A copy of the Family Plan can be found in the Appendix section of this manual.
FTC Exemptions:
It is the policy of Partnership for Strong Families for Family Team Conferencing to occur with all families receiving supervision and case management services from PSF. Only under extreme circumstances should a family be determined not appropriate for the FTC process. Such circumstances would include situations in which conducting an FTC would be detrimental or harmful to the child, family member, Family Care Counselor or another member of the FTC team. Research indicates that
PSF-Partnership for Strong Families * FTC-Family Team Conference * FCC-Family Care Counselor * CPI-Child Protective InvestigatorEE-Early Engagement * GAL-Guardian ad Litem * FSF-Family Service Facilitator * DCF-Department of Children and Families
children benefit from Family Team Conferencing even if their parents are not willing to participate and/or are deemed to be exempt from the FTC process. Children can be empowered by others in their lives to assist them in meeting their goals and permanency plans. Foster parents, relatives, school teachers, Guardians ad Litem, siblings and others can assist the children through the FTC process. A copy of the FTC Exemption form can be found in the Appendix section of this manual.
Determination of Family Team Conferencing Exemptions:
1. Designated FTC staff, the Family Care Counselor Supervisor and the Case Management Program Director, in conjunction with the Family Care Counselor, is responsible for ensuring the Family Team Conference Exemption Form is completed, documenting the reason the case is not appropriate for FTC. This form must be signed and dated by the staff person documenting the information.
2. Once complete, the Family Team Conference Exemption Form must be reviewed and signed by the assigned Family Care Counselor Supervisor and Case Management Program Director. The exemption form is then submitted to the FTC Project Director or another approved administrative staff for final approval.
a) If form is complete and presents adequate reason for exemption, it will be signed for approval. b) If form is incomplete or is lacking adequate reason for approval, it will be returned to the submitting staff member for revision. c) The designated FTC staff member will sign and approve completed and appropriate Family Team Conference Exemption Forms within 72 business hours of submission.
3. Once approved, the designated staff member will ensure the Family Team Conference Exemption Form is sent to Data Management.
4. The data manager will scan the form into the PSF database and will place the document in the client’s file.
Section 4: What We Discovered
The evaluation of the Family Connections grant was multi-faceted. A variety of methods and sources of data were used as part of a comprehensive process and outcome evaluation.
Process Evaluation:
The process evaluation examined the extent to which the FTC models were implemented with fidelity, the strengths and limitations of each model (in the eyes of all participants) and the perceived value and utility of each model in light of practice realities. The process evaluation involved a variety of activities, including independent observations of randomly selected FTCs (across all Pathways), focus groups with participant families and service providers, surveys of community partners, structured interviews
PSF-Partnership for Strong Families * FTC-Family Team Conference * FCC-Family Care Counselor * CPI-Child Protective InvestigatorEE-Early Engagement * GAL-Guardian ad Litem * FSF-Family Service Facilitator * DCF-Department of Children and Families
9

with FCCs and FTC facilitators and standard surveys given to participants after the completion of each FTC.
Outcome Evaluation:
The outcome evaluation examined the impact of each FTC on a number of indicators of child and family well-being and service effectiveness. Standardized measures, service utilization data, examination of service goal accomplishment, as well as other data were used to measure the extent to which there was a meaningful/statistically significant change for participant children and families (across each Pathway) as such relates to:
1. A reduction of emotional, conduct, hyperactivity and peer problems of children and youth (measured via the Strengths and Difficulties Questionnaire - SDQ)
2. An improvement in positive social behaviors of children and youth (measured via the SDQ)3. Improvements in a variety of protective factors with the family, including measures of family
functioning/resiliency, social supports, concrete supports, levels of nurturing and attachments and parental knowledge of child development and parenting skills (measured via the Protective Factors Survey)
4. Attainment of family service and plan of care goals (using the Goal Attainment Scales)5. Attainment of service outcomes linked to select statewide performance measures associated
with reunification, child safety and permanency indicators.
Discussion and Results:
Through the end of the study, a total of 1894 FTCs (initial and follow-up) were scheduled with 1156 individual families, of whom 623 (53.9%) agreed to participate (in whole or part) in the formal study/evaluation.
Select findings (see the forthcoming final report for all findings and recommendations) from the process evaluation are revealing. The focus groups with parents and service providers and the FCC and FTC Facilitator interviews reveal similar strengths and promises associated with FTCs.
Specifically, FTCs are generally well received, and there is strong support for FTCs with respect to the philosophy and approach. The FTC Facilitators also are praised for their skilled work, and the independent observations and responses to process questions following each FTC affirm the fidelity to which FTC Facilitators are implementing the FTC models. Among FCCs and FTC Facilitators, the FTC – regardless of the Pathway – was perceived to be an integral part of managing both in-home supervision and shelter cases. Among those interviewed, both FCCs and FTC Facilitators unanimously believed that the FTC engaged families in decision-making and linked families to services that families themselves identified as potentially helpful.
PSF-Partnership for Strong Families * FTC-Family Team Conference * FCC-Family Care Counselor * CPI-Child Protective InvestigatorEE-Early Engagement * GAL-Guardian ad Litem * FSF-Family Service Facilitator * DCF-Department of Children and Families
“Everything I’ve expressed concerns about, they’ve brought in resources to help. They are really good.”
- A Parent and FTC Participant
There was a strong preference among FCCs for Pathway 2 FTCs, which involves the FCC and FTC Facilitator as co-facilitators. This FTC model utilizes the skills of FTC Facilitators to facilitate FTCs with families and promotes direct and immediate linkage of services through the FTC Facilitators. The FTC Facilitators were perceived to play an important supportive role for the FCC. Pathway 3 is identical to Pathway 2 with respect to the FTC Facilitator roles, but the FCCs supported Pathway 2 over Pathway 3. They believed that families under utilize family alone time and that family alone time is redundant to the FTC itself.
It should be noted that FTCs are not perfect in practice overall. The parents in the focus group responded positively to FTCs, as did the service providers from both Judicial Circuits covered by the agency, but glitches identified in how, when and by whom FTCs are implemented suggest that a number of improvements could be made. For example, the interviews, observations and focus groups all suggest that families are not inviting their family members and supports to participate in the FTCs. Therefore, there could be better communication with families about this goal, as well as a concerted effort to work with families in inviting their supports (including professionals) to the FTCs. Some service providers highlighted they are challenged by the logistics of scheduling and participating in FTCs. As to the impact of FTCs, select service providers are uncertain as to whether FTCs truly give decision-making power to families when they are typically outnumbered by professionals during the FTCs. Also, they highlighted barriers to service linkages (e.g., lack of transportation, limited availability of certain services and low family motivation) that potentially undermine the goal of FTCs to better connect families to services.
A larger-scale and longer-term area of improvement is the idea of “culture change” that was raised in the focus groups and feedback from select professionals. Despite promising features of the FTC models that have been identified from various sources, there is the bigger challenge of culture change (among FCCs and others to put into practice the philosophy and approach of FTCs) that is necessary for FTCs to be successful and sustainable. All in all, the information collected to date that provides insights into this challenge suggests that culture change is attainable and that current practices through FTCs and other means are evidence of culture change.
Yet despite these concerns, the majority of respondents/participants believe in FTCs and feel strongly that FTCs should continue. It is rare that changes in practice are instituted quickly and without big challenges. Therefore,
PSF-Partnership for Strong Families * FTC-Family Team Conference * FCC-Family Care Counselor * CPI-Child Protective InvestigatorEE-Early Engagement * GAL-Guardian ad Litem * FSF-Family Service Facilitator * DCF-Department of Children and Families
11
“With FTC, I can speak my mind and they [FTC Facilitators] don’t turn around what I say. They took what I said and then said ‘This is what I can do to help you.’ Every time, the facilitator repeats back what I say so that I am clear that she is hearing me. She makes sure she understands what I am saying.”
- A Parent and FTC Participant
“I got the help I need. I had all eyes focused on me, and everyone listened.”
- A Parent and FTC Participant
“Before we became FTC focused, we just went in and said ‘This is what we want you to do – no ifs, ands or buts.’ [An FTC] allows the families more freedom to communicate and not just for us to take the information in.”
- A Family Care Counselor

the pace of acceptance by service providers and others to the FTCs model is expected to be steady if not slow at times. The results of the process evaluation show the expected mixed reactions to implementing a new practice model. However, overriding these mixed reactions has been a generally positive sentiment about FTCs and the potential of Family Team Conferencing to have a positive and meaningful impact on families.
With respect to the outcome evaluation, analyses suggest that there is a significant disproportion in the likelihood that those families originally assigned to Pathway 1 (20.7%) will participate in the study than those originally assigned to experimental Pathway 2 (40.1%) or Pathway 3 (39.2%) groups. This disproportion in participation rate limits the extent to which Pathway 1 may be a legitimate comparison/control group for which select results from Pathway 2 and Pathway 3 cases can be compared.
Using data through December 31, 2011, among the 1,375 goals established for 506 separate Goal Attainment Scales with 332 separate (non-duplicate) families (or 97.4% of all study cases at that time), those issues of most prominence included mental health needs (23.8% of all goals), case planning issues/needs (23.1%), substance abuse issues (12.8%), domestic violence issues (8.4%) and housing needs (8.3%). Other goals focused on employment (5.7%), education (4.6%), daycare (3.3%), visitation (3.3%), dental and medical needs (3.1%) and safety planning (2.8%). Analysis of GAS scores over time with a panel of cases reveals there is no significant measured change in the rate of improvement for Pathway 1 cases; however, noteworthy and significant changes exist for families assigned to Pathway 2 FTCs and Pathway 3 FTCs. These preliminary findings suggest that Pathway 2 and Pathway 3 FTC models have a more distinctive effect on moving the family (in a favorable direction) toward agreed upon service goals.
Findings from analyses of data (through the end of the study) from the Protective Factors Survey suggest that Pathway 2 FTCs have the most significant impact on protective factors for families.
PSF-Partnership for Strong Families * FTC-Family Team Conference * FCC-Family Care Counselor * CPI-Child Protective InvestigatorEE-Early Engagement * GAL-Guardian ad Litem * FSF-Family Service Facilitator * DCF-Department of Children and Families
“I am a firm believer in FTC… Having families take a look at who they are and where they were before the problems started. Usually people have some strengths. I see the FTC as being the catalyst for acknowledging the family’s strengths. Once you get people to look at their power then you can get them to look at changes that are needed.”
- A Family Care Counselor
“I’ve had quite a few FTCs with [one of the FTC Facilitators], and I was so impressed. Her level of organization is superb, but her ability to respect the client…I remember being astonished because one of the clients was being disrespectful and belligerent and not entirely honest. She was consistently respectful. It was an outstanding example of her continuing to say, ‘Well, what more can we do?’ She did the most remarkable job of meeting that person and respecting them and wanting to know what we could do to make them feel better. It brought a sense of everyone coming together and a structure that gave me a sense of clarity regarding my part and what I am working on. I felt it has made the clients feel more equal and respected. It’s a more humble approach.”
- A Service Provider

Using data through December 31, 2011, cases in Pathway 2 demonstrated statistically significant improvement in family functioning and resiliency, nurturing and attachment and increasing parents’ knowledge about “what to do as a parent.” By the end of the study, significant improvement in family functioning was maintained for Pathway 2 cases with no significant changes/improvements in other protective factors across all Pathways.
Using data throughout the entire study, the observed aggregate counts (across all pathways at the start of service) of children assessed (via the Strengths and Difficulties Questionnaire) as “borderline” and “abnormal” for each symptom scale suggest the highest proportions (rank ordered) of concerns are associated with Conduct Problems (41.4% of children are score at borderline or abnormal), Peer Problems (35.3%),
Hyperactivity (32.0%), Emotional Symptoms (22.8%) and Pro-Social Behaviors (i.e. absence thereof) (14.2%). When the Total Difficulties Scale scores are examined, 70.0% of all children and youth score at the “borderline” (18.5%) or “abnormal” (51.5%) level. Select analyses to date suggest there is no significant change or improvement over time for children in Pathway 1 FTCs that are assessed at the start of service as borderline or abnormal on each strength and difficulty. However, thus far, analyses suggest significant improvement on all SDQ measures for children involved in Pathway 2 FTCs. With respect to Pathway 3, select analyses suggest significant improvement with respect to conduct problems, hyperactivity, peer problems and total symptoms. These findings suggest that Pathway 2 and Pathway 3 FTCS are demonstrating a positive impact upon child behavior and difficulties as reported by caregivers and teen self-reports.
Preliminary analyses on data through the fall of 2011 found no significant differences on select permanency, family reunification and placement stability outcomes across FTC groups and in contrast with those families not receiving an FTC (pre-study cases and those exempt from FTCs). In sum, findings thus far suggest Pathway 2 and Pathway 3 (more so Pathway 2) have demonstrated a positive influence on plan of care and service goal attainment, select child well-being/behavior indicators and on family functioning. Findings generated from additional analyses on other outcomes will be presented in the final evaluation report.
13
PSF-Partnership for Strong Families * FTC-Family Team Conference * FCC-Family Care Counselor * CPI-Child Protective InvestigatorEE-Early Engagement * GAL-Guardian ad Litem * FSF-Family Service Facilitator * DCF-Department of Children and Families
“The FTC is set up where we are listening to the family. We are asking them what they need and what they want to see happen. So the family feels that “they’re really listening to me and they want to hear from me.” It really helps to build that relationship between the family and the FCC because it feels like we’re working together. We’re not here to make decisions for you or tell you want you need. So I think the FTC is a great foundation for the relationship between the FCC and the family.”
- A Family Care Counselor
“I feel like they ask my opinion and [the plan] is developed right as we are sitting there. I think everyone puts in their two cents and talks about what’s been accomplished and what still needs to be done.”
- A Parent and FTC Participant

Section 5: Dissemination Activities
Throughout the grant period, PSF took several steps to ensure that the evolution of the project was shared, both internally and externally, on a local, state and national level.
PSF’s website, www.pfsf.org, had a special page, which contained information related to FTCs and the Grant.
This area of the website provided an overview of the study project, as well as staff information and monthly data reports. Success stories, as well as the current Friends of the Grant recognition recipients were also highlighted on the web page. The Friends of the Grant award was an acknowledgement, given quarterly, to thank a Family Care Counselor for going above and beyond to ensure a meaningful FTC process for their clients. This award’s purpose was to serve as an incentive to motivate FCC staff to be more involved in the FTC and study project processes.
PSF-Partnership for Strong Families * FTC-Family Team Conference * FCC-Family Care Counselor * CPI-Child Protective InvestigatorEE-Early Engagement * GAL-Guardian ad Litem * FSF-Family Service Facilitator * DCF-Department of Children and Families
Success Story: FTC Provides Hope and a Plan to Overcome AddictionSubmitted by an FTC Facilitator
I recently met with a mother whose rights to her two children were terminated several years ago in another state; she then moved to Florida, gave birth to a third child, and the baby was sheltered as a result of the mother’s ongoing substance abuse. At the initial FTC, the mother relayed that she had previously made several unsuccessful attempts at substance abuse treatment; she truly had the desire to be drug-free but never had a plan of action and didn’t know who she could turn to for support. At the FTC, conversation focused not only on local treatment providers, but also about building a strong support system for the family, the importance of establishing a relapse plan and the need for ongoing after-care upon completion of a treatment program.
Eight months later, at a follow-up FTC, the mother proudly announced that she had been drug-free since the initial FTC. Additionally, she was able to share that she had utilized the resources discussed in the first FTC to acquire stable housing, part-time employment and was planning on returning to school. More than anything else, the mother was excited to celebrate having recently been granted unsupervised visitation with her child and told staff that those visits were going so well all parties anticipated that the family would be reunified at the next court hearing.
When asked, the mother noted that the clear outline of a plan of action, the development of a strong support system established at the beginning of the case and an overall tone of helping, teamwork, positive affirmations and celebrations of success as being essential components that were instrumental to her overall success. These interactions, she said, were in stark contrast to her previous involvements with the dependency system, during which she felt blamed, chastised and looked down upon.
PSF-Partnership for Strong Families * FTC-Family Team Conference * FCC-Family Care Counselor * CPI-Child Protective InvestigatorEE-Early Engagement * GAL-Guardian ad Litem * FSF-Family Service Facilitator * DCF-Department of Children and Families
15
A brochure was created to introduce families to the concept of Family Team Conferencing and to provide an overview of the grant. These brochures were distributed to families at the inception of their case so that they had some understanding of what an FTC was before being contacted to schedule the conference. A full copy of the brochure can be found in the Appendix section of this manual.
Three national level presentations were made during the Grant period. In June 2011, Grant Management and Evaluator staff travelled to Las Vegas, NV to present at the American Humane Association’s 2011 Family Group Decision Making Conference. In March 2012, evaluator Dr. Robin Perry provided a summary of the study design and processes at a Community of Child Welfare Scholars meeting at the University of Toronto. This meeting was hosted by Dr. Aron Shlonsky who is one of the lead authors in a systematic review of Family Group Decision Making sanctioned by the Campbell Collaboration Social Welfare Group. The project was invited to present final findings to this group upon conclusion of the study. Finally, in June 2012, PSF Grant Management staff gave a presentation regarding their dissemination activities at the 2012 National Grantees Conference in Washington, DC.
Additional dissemination activities included articles in PSF’s newsletters, as well as highlights in the PSF E-Blast e-mail, which is distributed to more than 400 recipients, including 90 service providers, 200 employees and 129 community partners and PSF board members.
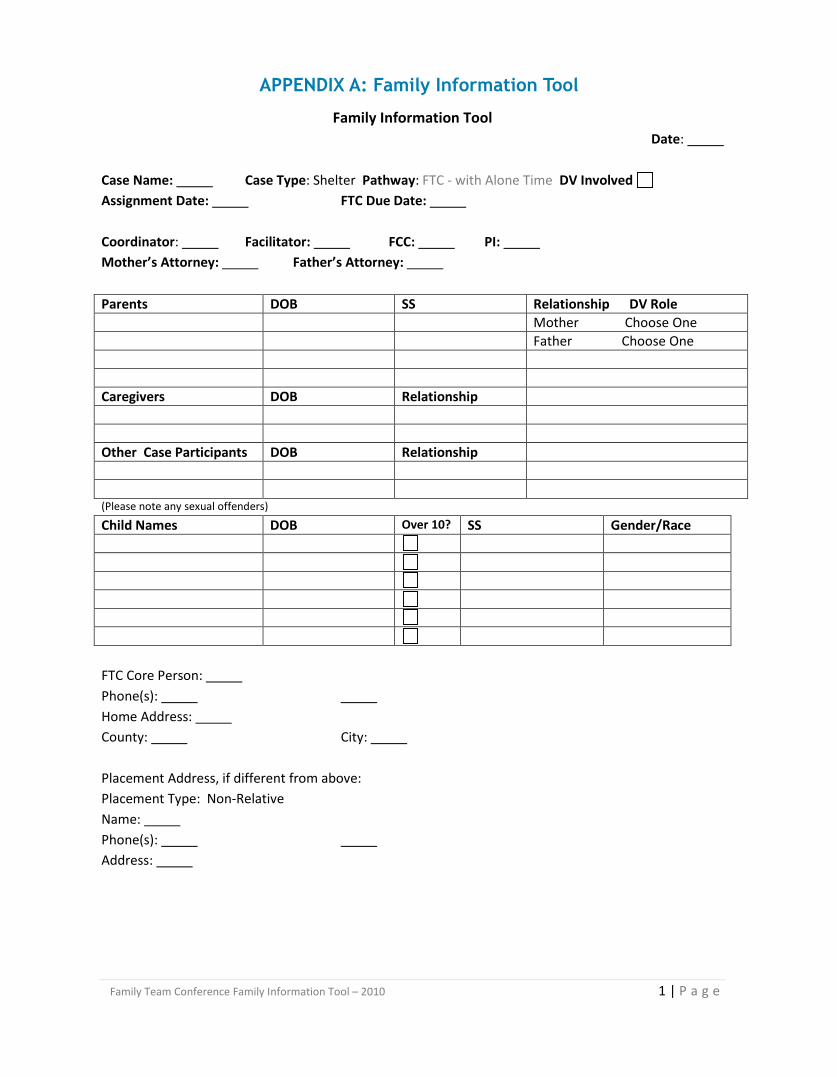
Family Team Conference Family Information Tool – 2010 1 | P a g e
Family Information Tool Date:
Case Name: Case Type: Shelter Pathway: FTC - with Alone Time DV Involved Assignment Date: FTC Due Date: Coordinator: Facilitator: FCC: PI: Mother’s Attorney: Father’s Attorney: Parents DOB SS Relationship DV Role Mother Choose One Father Choose One Caregivers DOB Relationship Other Case Participants DOB Relationship (Please note any sexual offenders)
Child Names DOB Over 10? SS Gender/Race FTC Core Person: Phone(s): Home Address: County: City: Placement Address, if different from above: Placement Type: Non-Relative Name: Phone(s): Address:
APPENDIX A: Family Information Tool
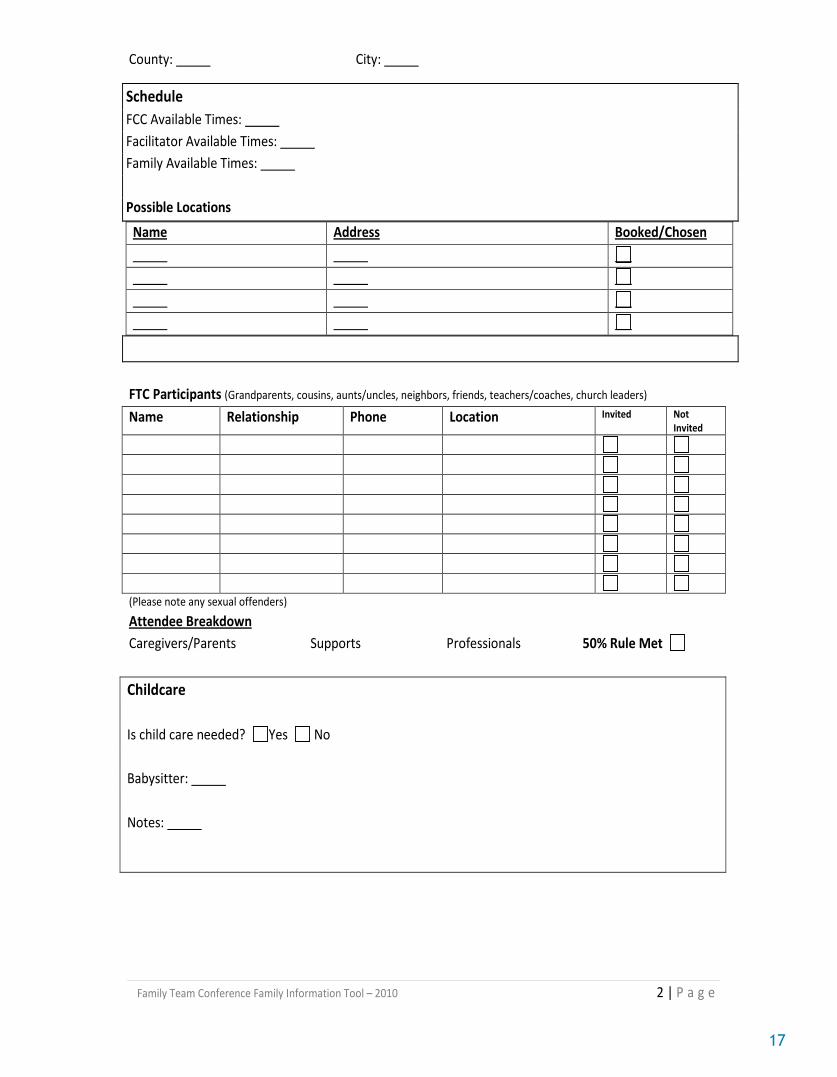
Family Team Conference Family Information Tool – 2010 2 | P a g e
County: City:
FTC Participants (Grandparents, cousins, aunts/uncles, neighbors, friends, teachers/coaches, church leaders) Name Relationship Phone Location Invited Not
Invited
(Please note any sexual offenders)
Attendee Breakdown Caregivers/Parents Supports Professionals 50% Rule Met
Schedule FCC Available Times: Facilitator Available Times: Family Available Times: Possible Locations
Name Address Booked/Chosen
Childcare Is child care needed? Yes No Babysitter: Notes:
17
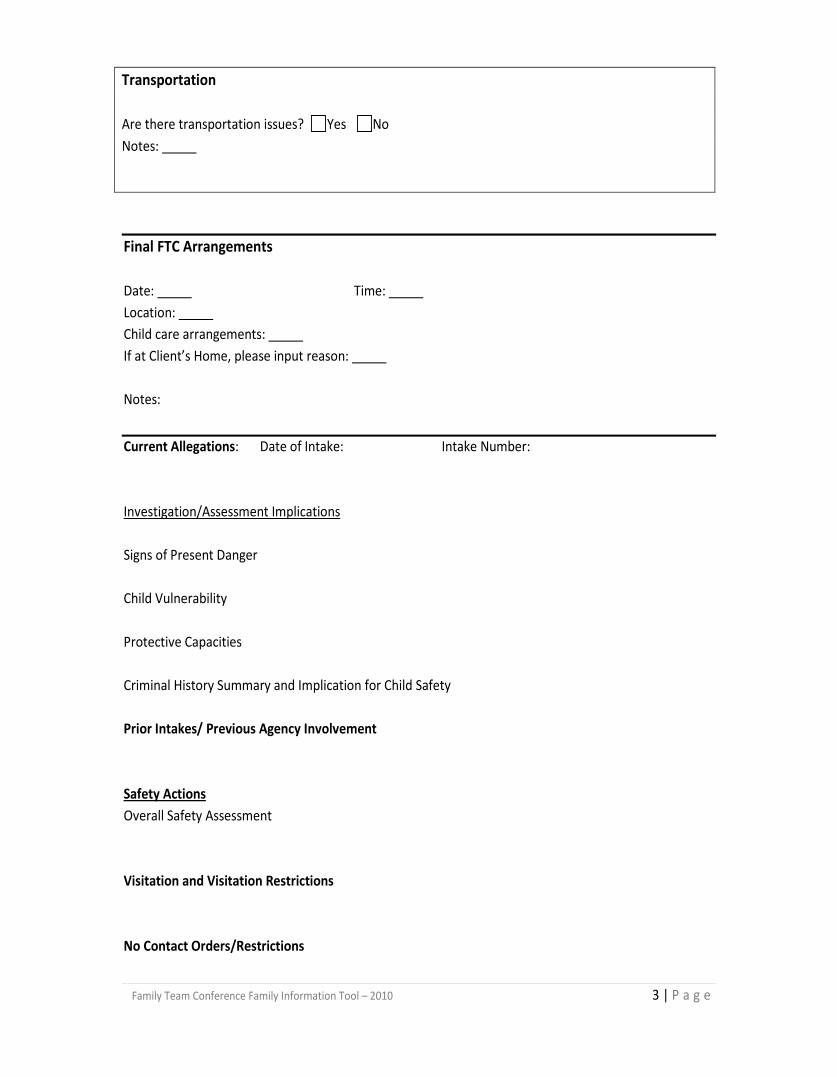
Family Team Conference Family Information Tool – 2010 3 | P a g e
Final FTC Arrangements Date: Time: Location: Child care arrangements: If at Client’s Home, please input reason: Notes:
Current Allegations: Date of Intake: Intake Number: Investigation/Assessment Implications Signs of Present Danger Child Vulnerability Protective Capacities Criminal History Summary and Implication for Child Safety Prior Intakes/ Previous Agency Involvement Safety Actions Overall Safety Assessment Visitation and Visitation Restrictions No Contact Orders/Restrictions
Transportation Are there transportation issues? Yes No Notes:
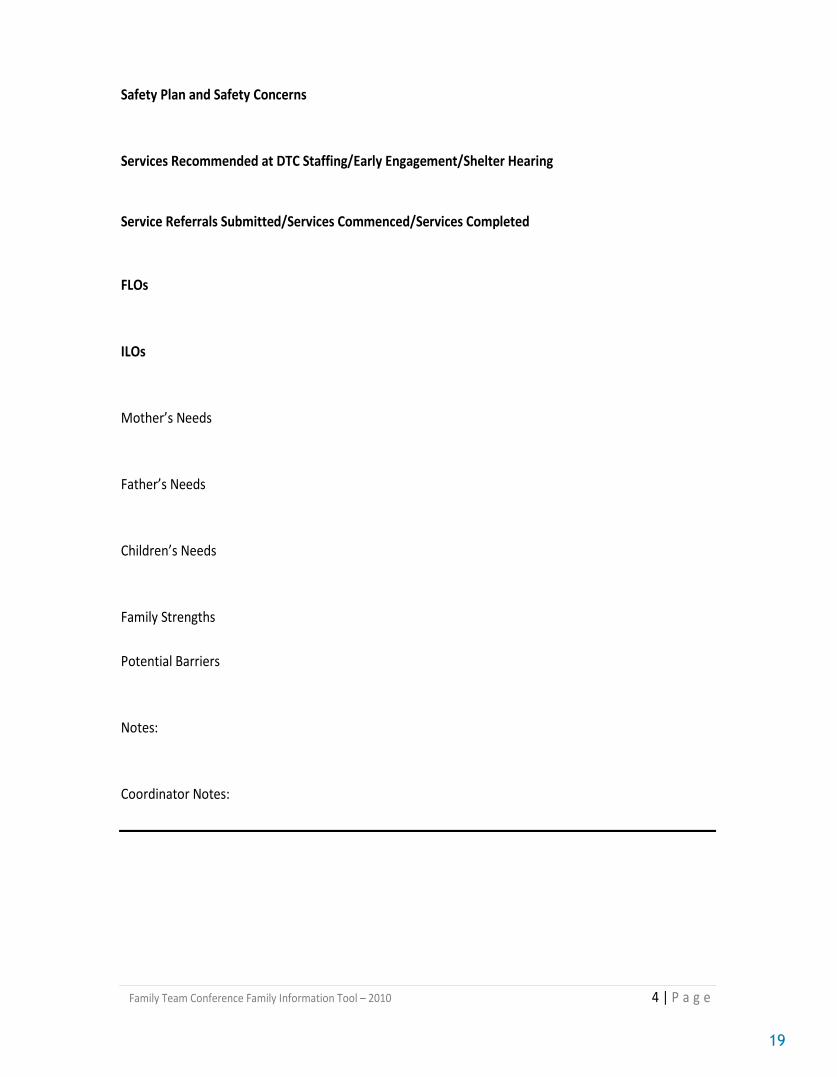
Family Team Conference Family Information Tool – 2010 4 | P a g e
Safety Plan and Safety Concerns Services Recommended at DTC Staffing/Early Engagement/Shelter Hearing Service Referrals Submitted/Services Commenced/Services Completed FLOs ILOs Mother’s Needs Father’s Needs Children’s Needs Family Strengths Potential Barriers Notes: Coordinator Notes:
19
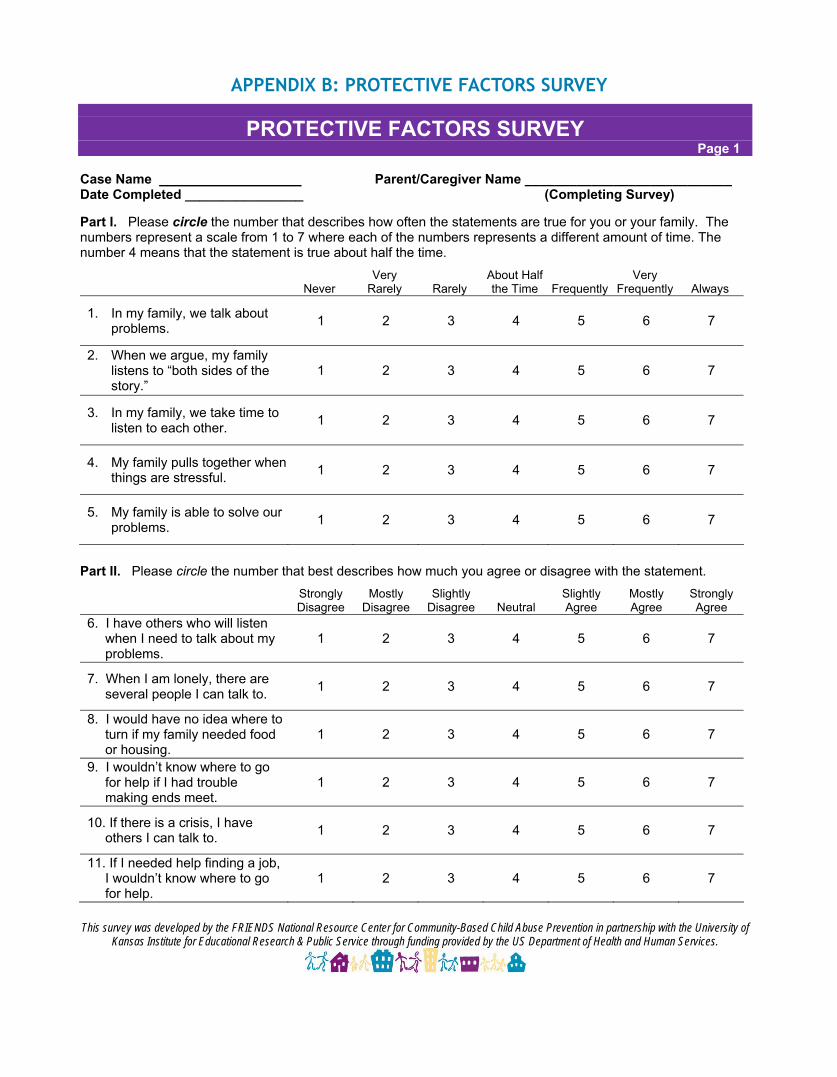
APPENDIX B: PROTECTIVE FACTORS SURVEY
PROTECTIVE FACTORS SURVEY Page 1
Case Name Parent/Caregiver Name ____________________________ Date Completed ________________ (Completing Survey)
Part I. Please circle the number that describes how often the statements are true for you or your family. The numbers represent a scale from 1 to 7 where each of the numbers represents a different amount of time. The number 4 means that the statement is true about half the time.
NeverVery
Rarely Rarely About Half the Time Frequently
Very Frequently Always
1. In my family, we talk about problems. 1 2 3 4 5 6 7
2. When we argue, my family listens to “both sides of the story.”
1 2 3 4 5 6 7
3. In my family, we take time to listen to each other. 1 2 3 4 5 6 7
4. My family pulls together when things are stressful. 1 2 3 4 5 6 7
5. My family is able to solve our problems. 1 2 3 4 5 6 7
Part II. Please circle the number that best describes how much you agree or disagree with the statement. Strongly Disagree
Mostly Disagree
Slightly Disagree Neutral
Slightly Agree
Mostly Agree
Strongly Agree
6. I have others who will listen when I need to talk about my problems.
1 2 3 4 5 6 7
7. When I am lonely, there are several people I can talk to. 1 2 3 4 5 6 7
8. I would have no idea where to turn if my family needed food or housing.
1 2 3 4 5 6 7
9. I wouldn’t know where to go for help if I had trouble making ends meet.
1 2 3 4 5 6 7
10. If there is a crisis, I have others I can talk to. 1 2 3 4 5 6 7
11. If I needed help finding a job, I wouldn’t know where to go for help.
1 2 3 4 5 6 7
This survey was developed by the FRIENDS National Resource Center for Community-Based Child Abuse Prevention in partnership with the University of Kansas Institute for Educational Research & Public Service through funding provided by the US Department of Health and Human Services.
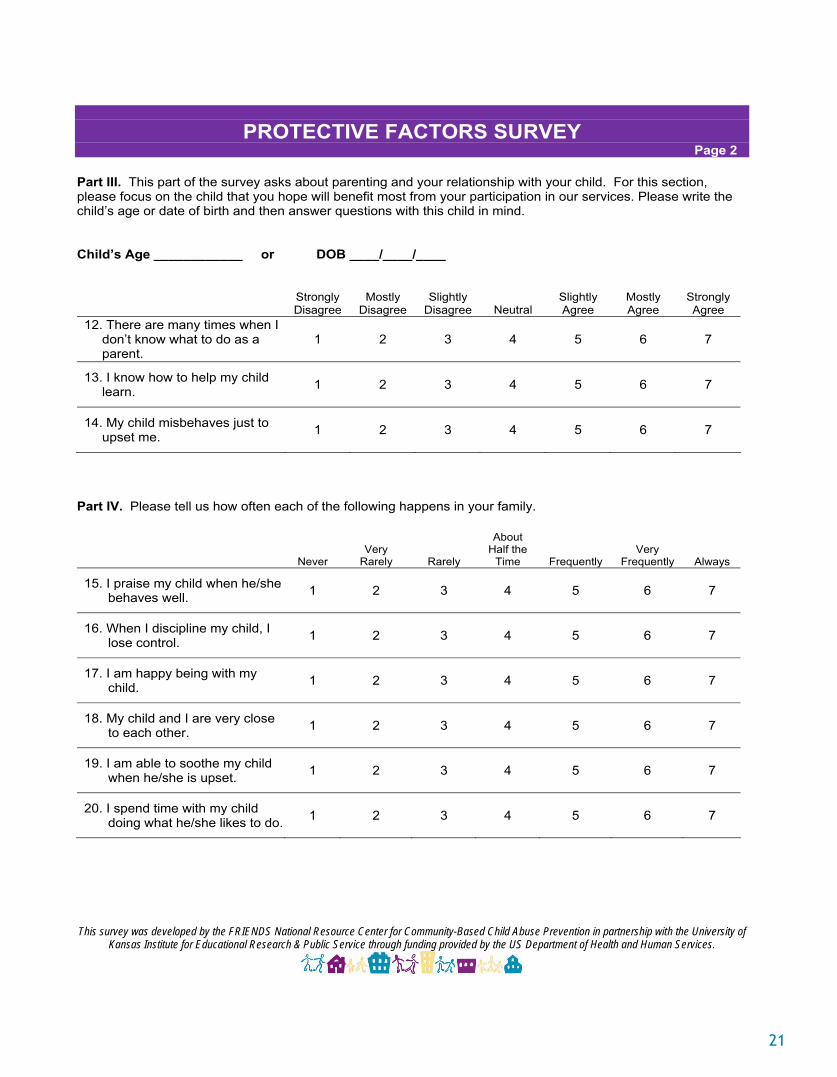
PROTECTIVE FACTORS SURVEY Page 2
Part III. This part of the survey asks about parenting and your relationship with your child. For this section, please focus on the child that you hope will benefit most from your participation in our services. Please write the child’s age or date of birth and then answer questions with this child in mind.
Child’s Age ____________ or DOB ____/____/____
Strongly Disagree
Mostly Disagree
Slightly Disagree Neutral
Slightly Agree
Mostly Agree
Strongly Agree
12. There are many times when I don’t know what to do as a parent.
1 2 3 4 5 6 7
13. I know how to help my child learn. 1 2 3 4 5 6 7
14. My child misbehaves just to upset me. 1 2 3 4 5 6 7
Part IV. Please tell us how often each of the following happens in your family.
Never Very
Rarely Rarely
AboutHalf the
Time Frequently Very
Frequently Always
15. I praise my child when he/she behaves well. 1 2 3 4 5 6 7
16. When I discipline my child, I lose control. 1 2 3 4 5 6 7
17. I am happy being with my child. 1 2 3 4 5 6 7
18. My child and I are very close to each other. 1 2 3 4 5 6 7
19. I am able to soothe my child when he/she is upset. 1 2 3 4 5 6 7
20. I spend time with my child doing what he/she likes to do. 1 2 3 4 5 6 7
This survey was developed by the FRIENDS National Resource Center for Community-Based Child Abuse Prevention in partnership with the University of Kansas Institute for Educational Research & Public Service through funding provided by the US Department of Health and Human Services.
21
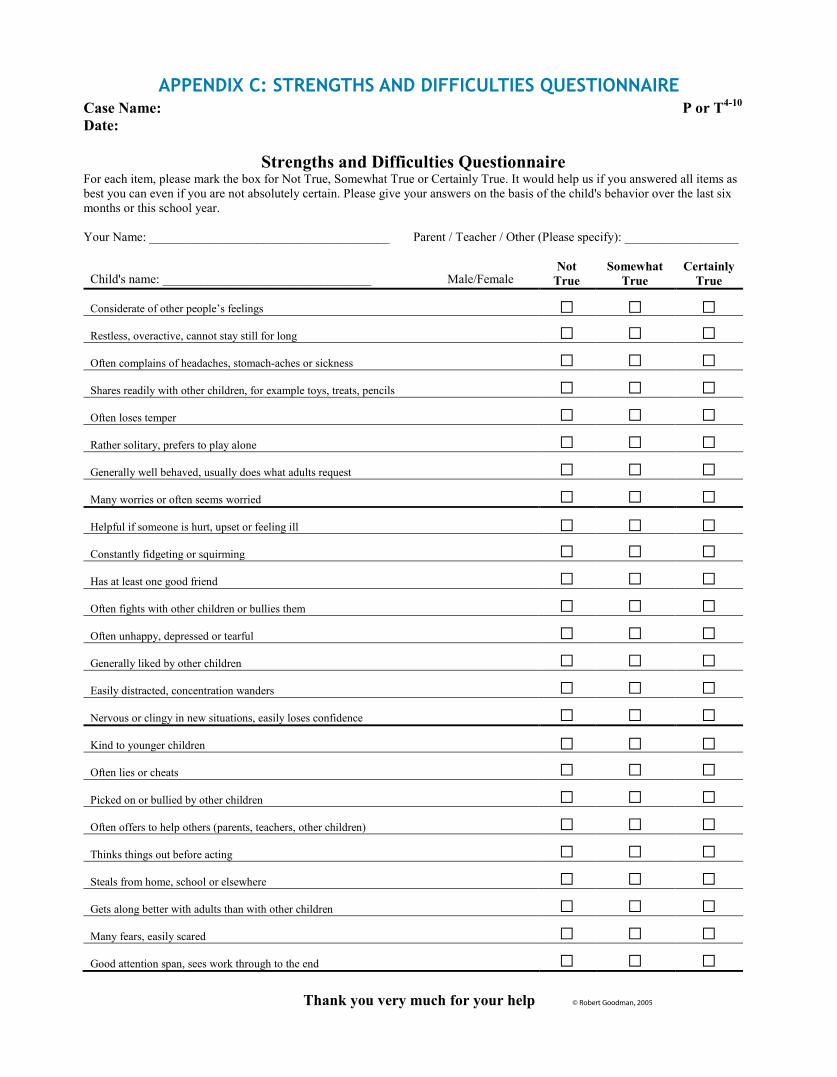
Case Name: P or T4-10
Date:
Thank you very much for your help © Robert Goodman, 2005
Strengths and Difficulties Questionnaire For each item, please mark the box for Not True, Somewhat True or Certainly True. It would help us if you answered all items as best you can even if you are not absolutely certain. Please give your answers on the basis of the child's behavior over the last six months or this school year. Your Name: ______________________________________ Parent / Teacher / Other (Please specify): __________________
Child's name: _________________________________ Male/Female
Not True
Somewhat True
Certainly True
Considerate of other people’s feelings □ □ □ Restless, overactive, cannot stay still for long □ □ □ Often complains of headaches, stomach-aches or sickness □ □ □ Shares readily with other children, for example toys, treats, pencils □ □ □ Often loses temper □ □ □ Rather solitary, prefers to play alone □ □ □ Generally well behaved, usually does what adults request □ □ □ Many worries or often seems worried □ □ □ Helpful if someone is hurt, upset or feeling ill □ □ □ Constantly fidgeting or squirming □ □ □ Has at least one good friend □ □ □ Often fights with other children or bullies them □ □ □ Often unhappy, depressed or tearful □ □ □ Generally liked by other children □ □ □ Easily distracted, concentration wanders □ □ □ Nervous or clingy in new situations, easily loses confidence □ □ □ Kind to younger children □ □ □ Often lies or cheats □ □ □ Picked on or bullied by other children □ □ □ Often offers to help others (parents, teachers, other children) □ □ □ Thinks things out before acting □ □ □ Steals from home, school or elsewhere □ □ □ Gets along better with adults than with other children □ □ □ Many fears, easily scared □ □ □ Good attention span, sees work through to the end □ □ □
APPENDIX C: STRENGTHS AND DIFFICULTIES QUESTIONNAIRE
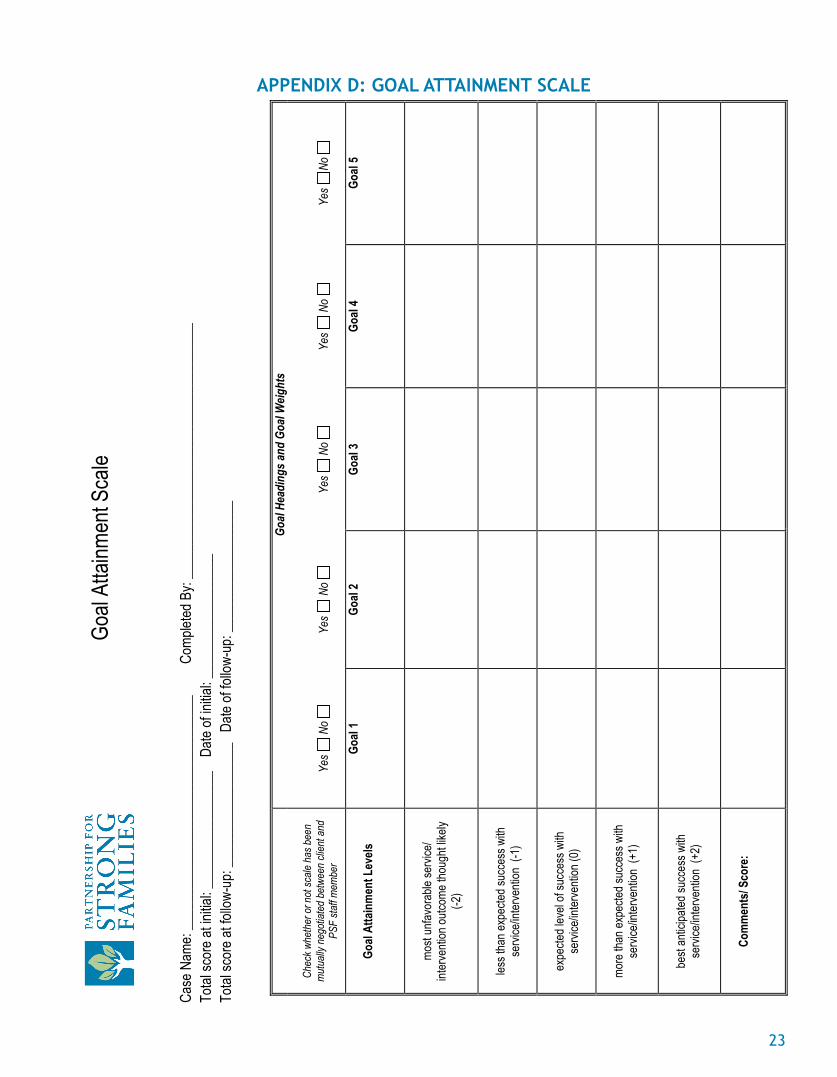
Goal
Attai
nmen
t Sca
le
Case
Nam
e: __
____
____
____
____
____
____
____
____
Com
pleted
By:
____
____
____
____
____
____
____
____
____
_ To
tal sc
ore a
t initia
l: ___
____
____
____
__
Date
of ini
tial: _
____
____
____
____
_ To
tal sc
ore a
t follo
w-up
: ___
____
____
____
___
Date
of fo
llow-
up: _
____
____
____
____
__
Go
al He
adin
gs an
d Go
al W
eight
s
Chec
k whe
ther
or n
ot sc
ale h
as b
een
mut
ually
neg
otiat
ed b
etwe
en cl
ient a
nd
PSF
staff
mem
ber
Ye
s N
o
Ye
s N
o
Ye
s N
o
Ye
s N
o
Ye
s No
Goal
Atta
inm
ent L
evels
Go
al 1
Goal
2
Goal
3
Goal
4
Goal
5
mo
st un
favor
able
servi
ce/
inter
venti
on ou
tcome
thou
ght li
kely
(-2
)
les
s tha
n exp
ected
succ
ess w
ith
servi
ce/in
terve
ntion
(-1
)
ex
pecte
d lev
el of
succ
ess w
ith
servi
ce/in
terve
ntion
(0)
mo
re th
an ex
pecte
d suc
cess
with
se
rvice
/inter
venti
on (
+1)
be
st an
ticipa
ted su
cces
s with
se
rvice
/inter
venti
on (
+2)
Com
men
ts/ S
core
:
APPENDIX D: GOAL ATTAINMENT SCALE
23
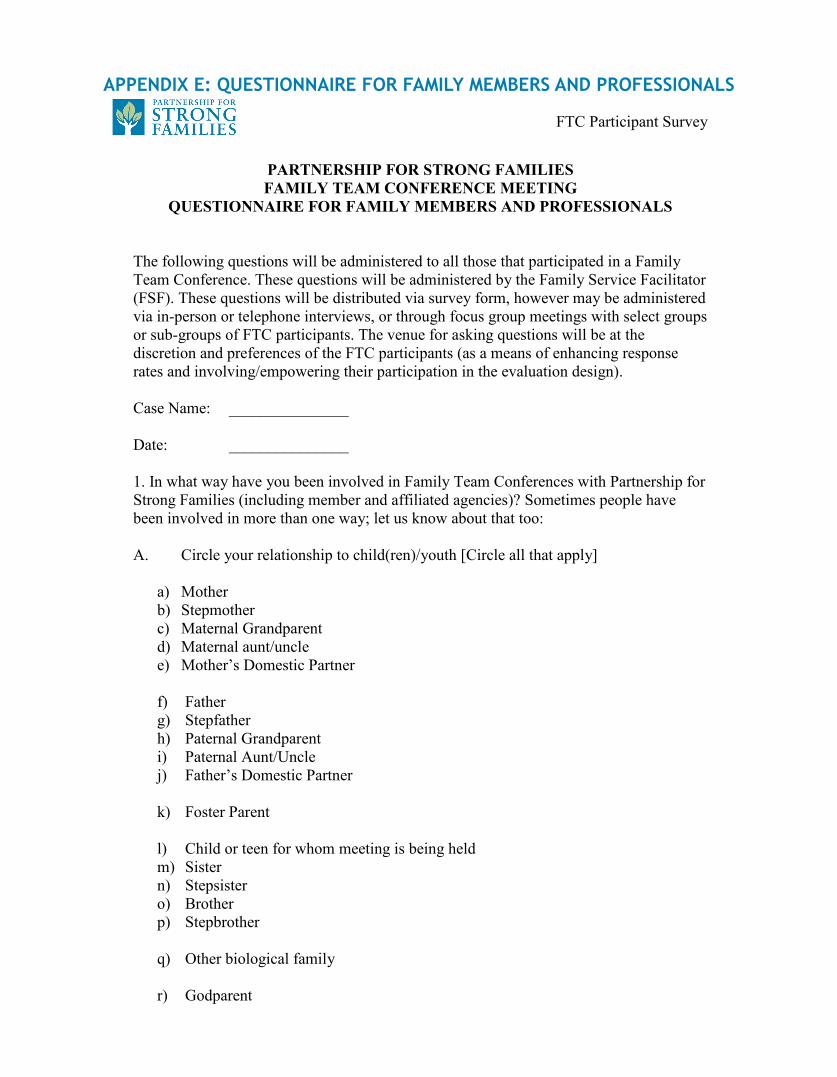
FTC Participant Survey
PARTNERSHIP FOR STRONG FAMILIES FAMILY TEAM CONFERENCE MEETING
QUESTIONNAIRE FOR FAMILY MEMBERS AND PROFESSIONALS
The following questions will be administered to all those that participated in a Family Team Conference. These questions will be administered by the Family Service Facilitator (FSF). These questions will be distributed via survey form, however may be administered via in-person or telephone interviews, or through focus group meetings with select groups or sub-groups of FTC participants. The venue for asking questions will be at the discretion and preferences of the FTC participants (as a means of enhancing response rates and involving/empowering their participation in the evaluation design). Case Name: _______________ Date: _______________ 1. In what way have you been involved in Family Team Conferences with Partnership for Strong Families (including member and affiliated agencies)? Sometimes people have been involved in more than one way; let us know about that too: A. Circle your relationship to child(ren)/youth [Circle all that apply]
a) Mother b) Stepmother c) Maternal Grandparent d) Maternal aunt/uncle e) Mother’s Domestic Partner
f) Father g) Stepfather h) Paternal Grandparent i) Paternal Aunt/Uncle j) Father’s Domestic Partner
k) Foster Parent
l) Child or teen for whom meeting is being held m) Sister n) Stepsister o) Brother p) Stepbrother
q) Other biological family
r) Godparent
APPENDIX E: QUESTIONNAIRE FOR FAMILY MEMBERS AND PROFESSIONALS
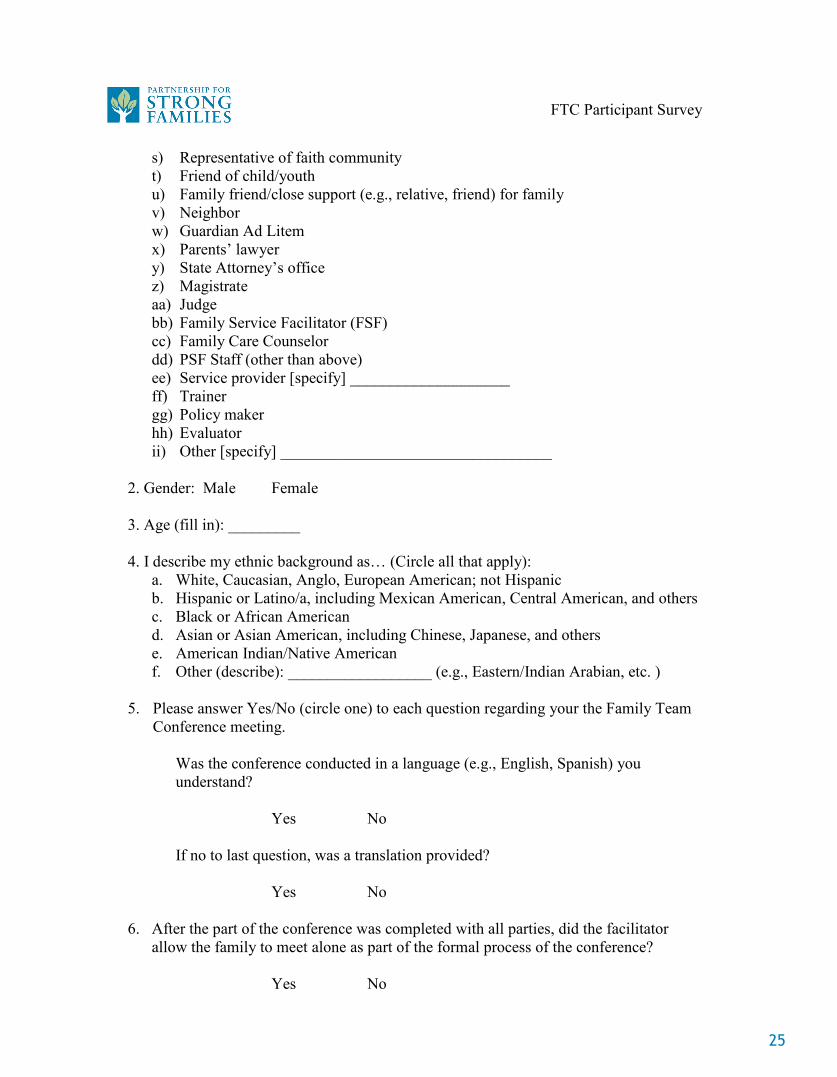
FTC Participant Survey
s) Representative of faith community t) Friend of child/youth u) Family friend/close support (e.g., relative, friend) for family v) Neighbor w) Guardian Ad Litem x) Parents’ lawyer y) State Attorney’s office z) Magistrate aa) Judge bb) Family Service Facilitator (FSF) cc) Family Care Counselor dd) PSF Staff (other than above) ee) Service provider [specify] ____________________ ff) Trainer gg) Policy maker hh) Evaluator ii) Other [specify] __________________________________
2. Gender: Male Female 3. Age (fill in): _________ 4. I describe my ethnic background as… (Circle all that apply):
a. White, Caucasian, Anglo, European American; not Hispanic b. Hispanic or Latino/a, including Mexican American, Central American, and others c. Black or African American d. Asian or Asian American, including Chinese, Japanese, and others e. American Indian/Native American f. Other (describe): __________________ (e.g., Eastern/Indian Arabian, etc. )
5. Please answer Yes/No (circle one) to each question regarding your the Family Team Conference meeting.
Was the conference conducted in a language (e.g., English, Spanish) you understand?
Yes No
If no to last question, was a translation provided? Yes No 6. After the part of the conference was completed with all parties, did the facilitator allow the family to meet alone as part of the formal process of the conference?
Yes No
25
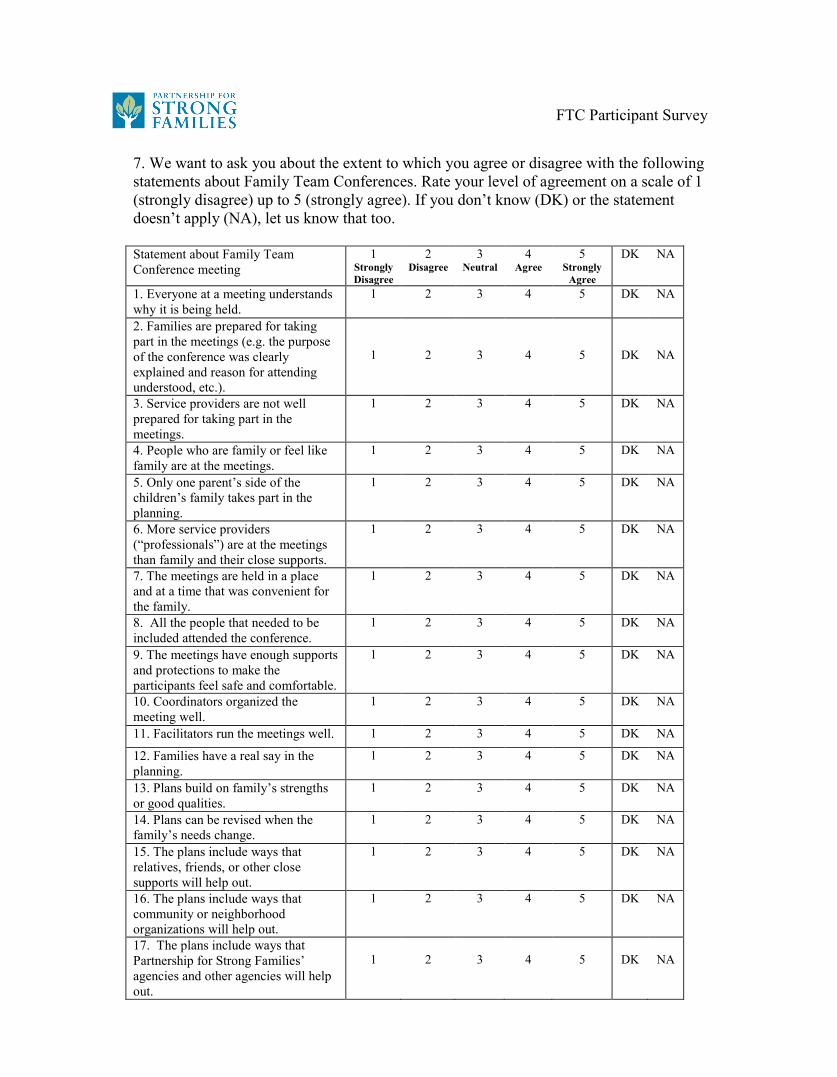
FTC Participant Survey
7. We want to ask you about the extent to which you agree or disagree with the following statements about Family Team Conferences. Rate your level of agreement on a scale of 1 (strongly disagree) up to 5 (strongly agree). If you don’t know (DK) or the statement doesn’t apply (NA), let us know that too. Statement about Family Team Conference meeting
1 Strongly Disagree
2 Disagree
3 Neutral
4 Agree
5 Strongly
Agree
DK NA
1. Everyone at a meeting understands why it is being held.
1 2 3 4 5 DK NA
2. Families are prepared for taking part in the meetings (e.g. the purpose of the conference was clearly explained and reason for attending understood, etc.).
1
2
3
4
5
DK
NA
3. Service providers are not well prepared for taking part in the meetings.
1 2 3 4 5 DK NA
4. People who are family or feel like family are at the meetings.
1 2 3 4 5 DK NA
5. Only one parent’s side of the children’s family takes part in the planning.
1 2 3 4 5 DK NA
6. More service providers (“professionals”) are at the meetings than family and their close supports.
1 2 3 4 5 DK NA
7. The meetings are held in a place and at a time that was convenient for the family.
1 2 3 4 5 DK NA
8. All the people that needed to be included attended the conference.
1 2 3 4 5 DK NA
9. The meetings have enough supports and protections to make the participants feel safe and comfortable.
1 2 3 4 5 DK NA
10. Coordinators organized the meeting well.
1 2 3 4 5 DK NA
11. Facilitators run the meetings well. 1 2 3 4 5 DK NA
12. Families have a real say in the planning.
1 2 3 4 5 DK NA
13. Plans build on family’s strengths or good qualities.
1 2 3 4 5 DK NA
14. Plans can be revised when the family’s needs change.
1 2 3 4 5 DK NA
15. The plans include ways that relatives, friends, or other close supports will help out.
1 2 3 4 5 DK NA
16. The plans include ways that community or neighborhood organizations will help out.
1 2 3 4 5 DK NA
17. The plans include ways that Partnership for Strong Families’ agencies and other agencies will help out.
1
2
3
4
5
DK
NA
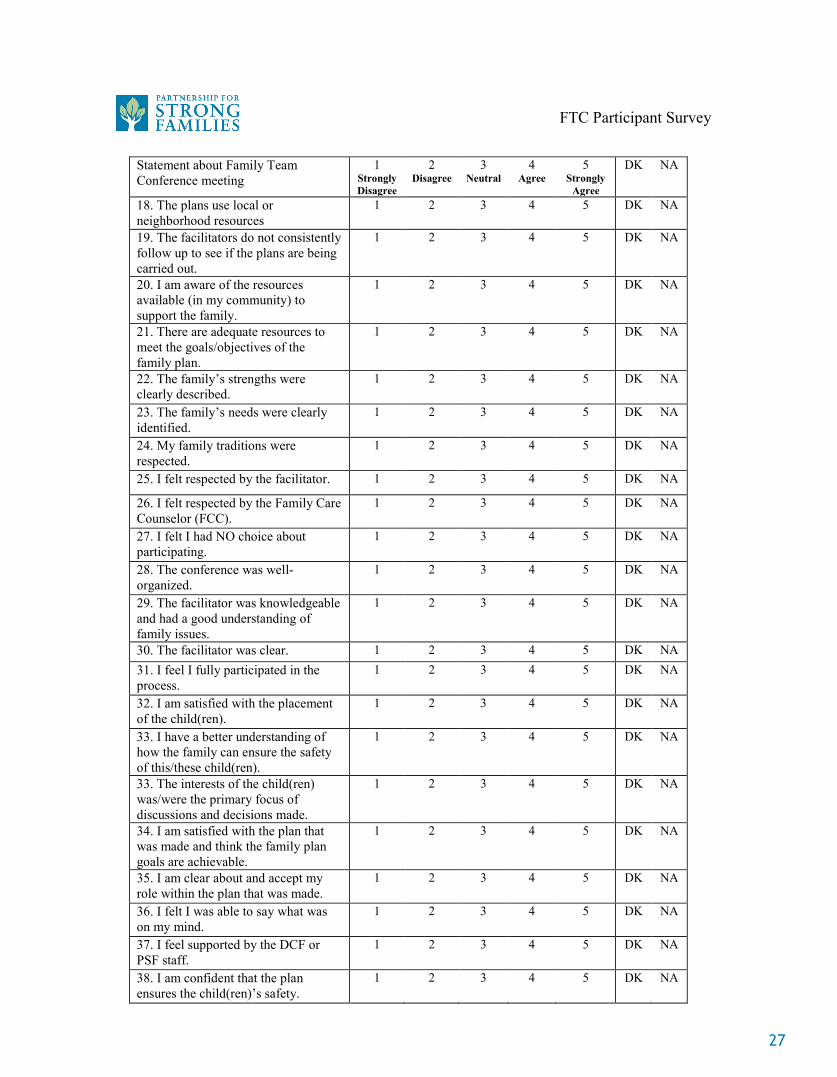
FTC Participant Survey
Statement about Family Team Conference meeting
1 Strongly Disagree
2 Disagree
3 Neutral
4 Agree
5 Strongly
Agree
DK NA
18. The plans use local or neighborhood resources
1 2 3 4 5 DK NA
19. The facilitators do not consistently follow up to see if the plans are being carried out.
1 2 3 4 5 DK NA
20. I am aware of the resources available (in my community) to support the family.
1 2 3 4 5 DK NA
21. There are adequate resources to meet the goals/objectives of the family plan.
1 2 3 4 5 DK NA
22. The family’s strengths were clearly described.
1 2 3 4 5 DK NA
23. The family’s needs were clearly identified.
1 2 3 4 5 DK NA
24. My family traditions were respected.
1 2 3 4 5 DK NA
25. I felt respected by the facilitator. 1 2 3 4 5 DK NA
26. I felt respected by the Family Care Counselor (FCC).
1 2 3 4 5 DK NA
27. I felt I had NO choice about participating.
1 2 3 4 5 DK NA
28. The conference was well-organized.
1 2 3 4 5 DK NA
29. The facilitator was knowledgeable and had a good understanding of family issues.
1 2 3 4 5 DK NA
30. The facilitator was clear. 1 2 3 4 5 DK NA 31. I feel I fully participated in the process.
1 2 3 4 5 DK NA
32. I am satisfied with the placement of the child(ren).
1 2 3 4 5 DK NA
33. I have a better understanding of how the family can ensure the safety of this/these child(ren).
1 2 3 4 5 DK NA
33. The interests of the child(ren) was/were the primary focus of discussions and decisions made.
1 2 3 4 5 DK NA
34. I am satisfied with the plan that was made and think the family plan goals are achievable.
1 2 3 4 5 DK NA
35. I am clear about and accept my role within the plan that was made.
1 2 3 4 5 DK NA
36. I felt I was able to say what was on my mind.
1 2 3 4 5 DK NA
37. I feel supported by the DCF or PSF staff.
1 2 3 4 5 DK NA
38. I am confident that the plan ensures the child(ren)’s safety.
1 2 3 4 5 DK NA
27
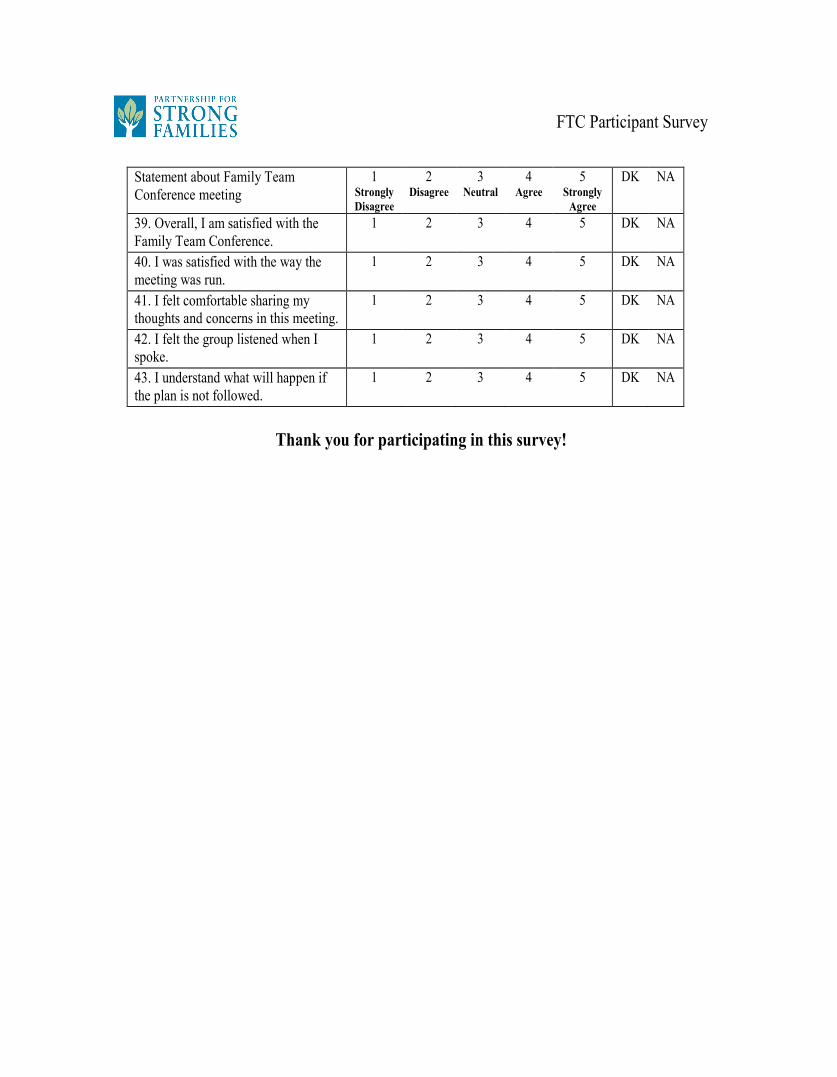
FTC Participant Survey
Statement about Family Team Conference meeting
1 Strongly Disagree
2 Disagree
3 Neutral
4 Agree
5 Strongly
Agree
DK NA
39. Overall, I am satisfied with the Family Team Conference.
1 2 3 4 5 DK NA
40. I was satisfied with the way the meeting was run.
1 2 3 4 5 DK NA
41. I felt comfortable sharing my thoughts and concerns in this meeting.
1 2 3 4 5 DK NA
42. I felt the group listened when I spoke.
1 2 3 4 5 DK NA
43. I understand what will happen if the plan is not followed.
1 2 3 4 5 DK NA
Thank you for participating in this survey!
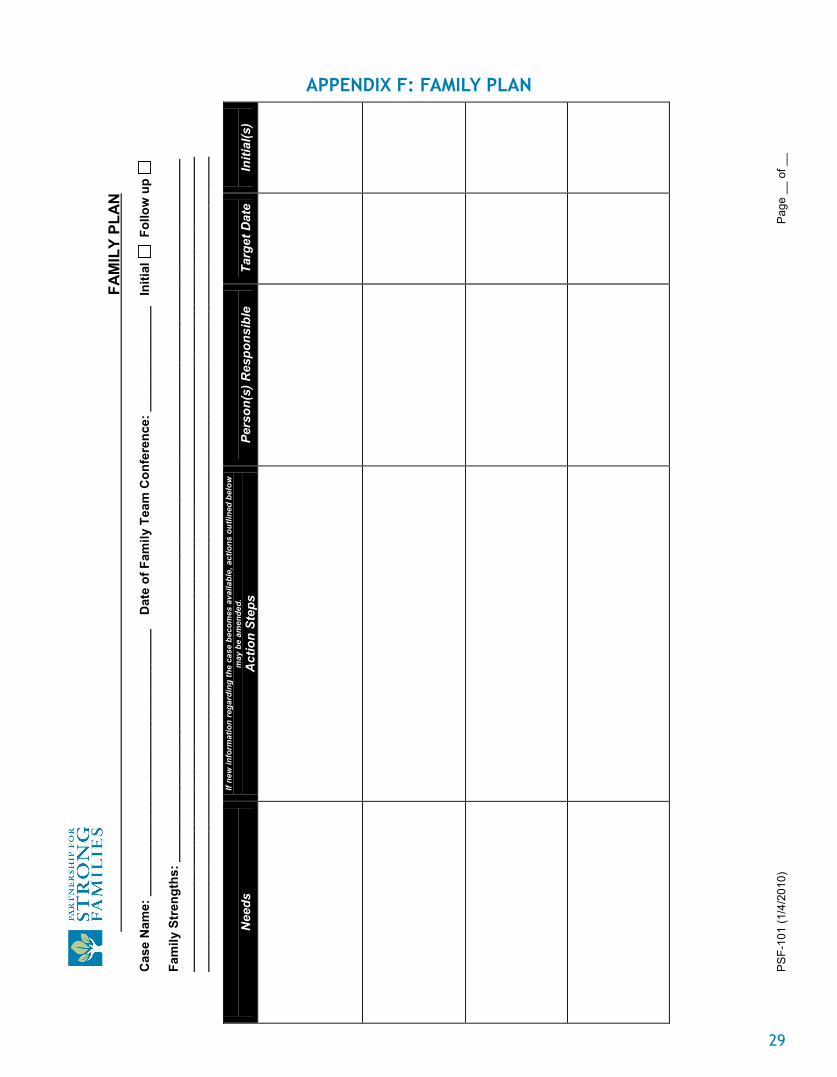
FA
MIL
Y PL
AN
PS
F-10
1 (1
/4/2
010)
P
age
__ o
f __
Cas
e N
ame:
___
____
____
____
____
____
____
____
____
___
D
ate
of F
amily
Tea
m C
onfe
renc
e: _
____
____
____
__
Initi
al
Fol
low
up
Fa
mily
Str
engt
hs: _
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
___
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
__
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
__
N
eeds
If
new
info
rmat
ion
rega
rdin
g th
e ca
se b
ecom
es a
vaila
ble,
act
ions
out
lined
bel
ow
may
be
amen
ded.
A
ctio
n St
eps
Pe
rson
(s) R
espo
nsib
le
Ta
rget
Dat
e
Initi
al(s
)
APPENDIX F: FAMILY PLAN
29
Fam
ily N
ame:
___
____
____
____
____
____
Fa
mily
Pla
n
Dat
e of
Con
fere
nce:
____
____
____
___
PSF-
101
(1/4
/201
0)
Page
__
of _
_ Co
nfid
entia
lity
Agre
emen
t: A
ll in
form
atio
n pr
esen
ted
and
shar
ed w
ithin
the
Fam
ily T
eam
Con
fere
nce
mus
t be
kept
con
fiden
tial.
I ha
ve
been
info
rmed
of t
he c
onfid
entia
lity
guid
elin
es fo
r PSF
Fam
ily T
eam
Con
fere
nces
, and
her
eby
agre
e to
hol
d al
l inf
orm
atio
n re
gard
ing
the
child
ren
and
fam
ilies
ser
ved
conf
iden
tial.
If
new
info
rmat
ion
rega
rdin
g th
e ca
se b
ecom
es a
vaila
ble,
act
ion
step
s ou
tline
d ab
ove
may
be
amen
ded.
Sign
atur
e be
low
den
otes
dis
cuss
ion
and
agre
emen
t to
conf
iden
tialit
y. Y
ou w
ill b
e as
ked
to in
itial
any
abo
ve it
ems
that
you
are
resp
onsi
ble
for.
Addi
tiona
l not
es a
nd T
eam
Mem
bers
to in
vite
to fo
llow
-up
Fam
ily T
eam
Con
fere
nce
(incl
ude
nam
es a
nd c
onta
ct in
form
atio
n):
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
___
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
___
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
___
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
___
Nam
e Ro
le
Phon
e Si
gnat
ure
Date
Fam
ily C
are
Cou
nsel
or
FTC
Fac
ilitat
or
FA
MIL
Y TE
AM
CO
NFE
REN
CE
– EX
EMPT
ION
__
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
___
PSF
101
b (3
/24/
2011
)
1
Fam
ily D
eter
min
ed N
on-A
pplic
able
for F
TC:
D
ate
of D
eter
min
atio
n:
C
ase
Nam
e:
AD
ULT
FA
MIL
Y M
EMB
ERS:
C
HIL
DR
EN:
Nam
e R
elat
ions
hip
N
ame
Cus
tody
Sta
tus
Perm
anen
cy G
oal
Shel
ter C
ase
Dat
e of
she
lter:
In
-Hom
e Su
perv
isio
n C
ase
Dat
e of
initi
al jo
int v
isit:
INIT
IAL
INFO
RM
ATIO
N R
ECEI
VED
IND
ICAT
ES E
XEM
PTIO
N F
RO
M F
TC IS
WA
RR
AN
TED
?
YES
N
O
PRES
ENTI
NG
CO
ND
ITIO
NS:
Wha
t wer
e th
e ab
use
alle
gatio
ns a
nd is
sues
resu
lting
in D
CF/
PSF
invo
lvem
ent w
ith th
e fa
mily
?
EFFO
RTS
MA
DE
TO F
AC
ILIT
ATE
PAR
TIC
IPAT
ION
IN F
AMIL
Y TE
AM C
ON
FER
ENC
E: P
rior t
o a
dete
rmin
atio
n fo
r exe
mpt
ion
the
follo
win
g ef
forts
wer
e m
ade
to e
ngag
e th
e fa
mily
in th
e Fa
mily
Tea
m C
onfe
renc
e pr
oces
s:
R
EASO
N F
OR
EXE
MPT
ION
TO
FAM
ILY
TEAM
CO
NFE
REN
CIN
G:
Spe
cific
reas
on(s
) and
circ
umst
ance
s w
hich
just
ify e
xem
ptio
n fro
m F
TC:
St
aff m
embe
r mak
ing
dete
rmin
atio
n:
____
____
____
____
____
____
____
____
____
__
Si
gnat
ure
D
ate
R
evie
win
g FC
C S
uper
viso
r:
____
____
____
____
____
____
____
____
____
_
Si
gnat
ure
Dat
e
Agen
cy:
PSF
C
HS
D
ever
eux
FP
S
Cam
elot
Uni
t:
Rev
iew
ing
Cas
e M
anag
emen
t Pro
gram
Dire
ctor
:
___
____
____
____
____
____
____
____
____
__
Sign
atur
e
D
ate
Appr
ovin
g U
M S
taff
Mem
ber:
__
____
____
____
____
____
____
____
____
___
Sign
atur
e
D
ate
APPENDIX G: EXEMPTION FORM
31
PSF
101
b (3
/24/
2011
)
2
Inst
ruct
ions
: To
be
com
plet
ed b
y th
e Fa
mily
Car
e C
ouns
elor
or b
y FT
C C
oord
inat
or w
hen
and
exem
ptio
n fro
m F
amily
Tea
m C
onfe
renc
ing
has
been
det
erm
ined
to b
e ap
prop
riate
. Th
e sp
ecifi
c re
ason
(s) f
or th
e ex
empt
ion
mus
t be
reco
rded
on
the
form
. Th
e fo
rm m
ust b
e si
gned
by
the
Fam
ily C
are
Supe
rvis
or a
nd P
rogr
am D
irect
or, p
rior t
o be
ing
subm
itted
for U
tiliz
atio
n M
anag
emen
t app
rova
l. T
he s
igne
d an
d co
mpl
eted
form
is
then
sen
t to
the
FTC
Pro
ject
Man
ager
or D
irect
or o
f Util
izat
ion
Man
agem
ent f
or fi
nal a
ppro
val a
nd w
ill th
en b
e lo
gged
into
Pki
ds.
NO
TE:
It is
the
Polic
y of
the
Par
tner
ship
for S
trong
Fam
ilies
for F
amily
Tea
m C
onfe
renc
ing
to o
ccur
with
all
fam
ilies
rece
ivin
g su
perv
isio
n an
d ca
se m
anag
emen
t ser
vice
s fro
m P
SF.
Onl
y un
der e
xtre
me
circ
umst
ance
s sh
ould
a fa
mily
be
dete
rmin
ed n
on-a
pplic
able
for a
FTC
. S
uch
circ
umst
ance
s w
ould
incl
ude
situ
atio
ns in
whi
ch c
ondu
ctin
g a
FTC
wou
ld b
e de
trim
enta
l or h
arm
ful t
o th
e ch
ild, f
amily
mem
ber,
Fam
ily C
are
Cou
nsel
or o
r ano
ther
mem
ber o
f the
FTC
team
. Pl
ease
kee
p in
min
d ch
ildre
n of
age
can
ben
efit
from
Fam
ily T
eam
Con
fere
ncin
g ev
en if
thei
r pa
rent
s ar
e no
t will
ing
to p
artic
ipat
e an
d/or
are
dee
med
to b
e ex
empt
from
the
FTC
pro
cess
. C
hild
ren
can
be e
mpo
wer
ed b
y ot
hers
in th
eir l
ives
to
ass
ist t
hem
in m
eetin
g th
eir g
oals
and
per
man
ency
pla
ns.
Fost
er P
aren
ts, r
elat
ives
, sch
ool t
each
ers,
Gua
rdia
ns a
d Li
tem
, sib
lings
and
oth
ers
can
assi
st th
e ch
ildre
n th
roug
h th
e FT
C p
roce
ss.
Visi
t us a
t pfs
f.org
Hea
dqua
rter
s . 5
950
NW
1st
Pla
ce, S
uite
A .
Gai
nesv
ille,
FL 3
2607
. 35
2.24
4.15
00
PRIN
CIP
LES
OF
TH
E C
HIL
D A
ND
FA
MIL
Y T
EAM
PR
OC
ESS
•T
he fo
cus
is o
n th
e ne
eds
rath
er th
an th
e sy
mpt
oms.
•Pe
ople
are
cap
able
of
chan
ge
•A
ll pe
ople
and
fam
ilies
hav
e st
reng
ths.
•A
sol
utio
n th
at a
fam
ily g
ener
ates
with
a te
am
is m
ore
likel
y to
fit t
hat f
amily
.
•A
fam
ily is
mor
e in
vest
ed in
a p
lan
in w
hich
th
ey b
elie
ve.
•Fa
mily
mem
bers
and
frie
nds
can
iden
tify
solu
tions
that
no
form
al s
yste
m w
ould
be
able
to
gen
erat
e.
•Fa
mily
and
frie
nds
prov
ide
love
and
car
ing
in
a w
ay th
at n
o fo
rmal
hel
ping
sys
tem
can
.
•W
hen
you
brin
g to
geth
er a
num
ber
of c
arin
g pe
ople
in th
e sa
me
room
you
obt
ain
ener
gy
that
fuel
s th
e en
gine
of
chan
ge.
Cor
e Prin
ciples
of
Eng
agin
g Fam
ilies
and
Fam
ily
Team
Con
feren
cing i
nclu
de:
Resp
ect
Aut
hent
icity
/Gen
uine
ness
Em
path
yFa
mily
Tea
m C
onfe
renc
ing
APPENDIX H: FTC BROCHURE
33

The
Fam
ily
Team
Fa
mili
es n
eed
help
in
times
of
crisi
s, so
the
y dr
aw
toge
ther
peo
ple
who
m t
hey
trus
t an
d w
ho c
an h
elp
in
resp
ondi
ng to
the
issue
s th
ey fa
ce. A
lmos
t eve
ryon
e ca
n id
entif
y a
time
whe
n th
ey f
orm
ed a
tea
m,
som
etim
es
involvingprofessionalhelpers,tomeetaspecificneed.
Like
wise
, mos
t pe
ople
who
hav
e dr
awn
a te
am a
roun
d th
em a
re w
illin
g to
bec
ome
cont
ribut
ors
to s
uch
a te
am
or c
ircle
of
frie
nds.
Fam
ily T
eam
Con
fere
ncin
g is
an
activ
ity a
ll fa
mili
es r
eceiv
ing
serv
ice
at P
artn
ersh
ip f
or
Stro
ng F
amili
es h
ave
an o
ppor
tuni
ty to
par
ticip
ate
in. I
t is
a pr
oces
s in
whi
ch p
artic
ipan
ts:
•Le
arn
wha
t the
fam
ily h
opes
to a
ccom
plish
•Se
t rea
sona
ble
and
mea
ning
ful g
oals
•Recognizeandaffirmthefamilystrengths
•A
sses
s fam
ily n
eeds
•Fi
nd so
lutio
ns to
mee
t fam
ily n
eeds
•D
esig
n in
divi
duali
zed
supp
orts
an
d se
rvic
es
that
mat
ch t
he f
amily
’s ne
eds
and
build
s on
the
ir st
reng
ths
•A
chie
ve c
larity
abo
ut w
ho is
resp
onsib
le fo
r agr
eed
upon
task
s •
Agr
ee o
n th
e ne
xt st
eps
The
FTC
is alr
eady
an
esta
blish
ed p
art o
f se
rvic
es
prov
ided
by
PSF,
alth
ough
diff
eren
t mod
els o
f FT
C ar
e pr
actic
ed a
nd re
sear
ched
else
whe
re.
The
proj
ect
plan
s to
test
the
curr
ent m
odel
util
ized
by
PSF
with
two
alter
nativ
e m
odel
s:•
Will
eac
h m
odel
pro
duce
diff
eren
t res
ults
?•
Will
par
ticip
ants,
esp
ecial
ly th
e fa
mily
, per
ceiv
e an
d va
lue
each
mod
el d
iffer
ently
?
Resu
lts o
f in
tere
st to
the
stud
y in
clud
e:•
Incr
easin
g ch
ild a
nd fa
mily
safe
ty a
t hom
e•
Redu
cing
tim
elin
ess t
o ac
hiev
e pe
rman
ent h
omes
fo
r chi
ldre
n•
Impr
ovin
g ch
ild a
nd fa
mily
wel
l-bei
ng•
Gre
ater
fam
ily in
volv
emen
t in
case
plan
ning
and
de
cisio
n m
akin
g•
Oth
er se
rvic
e go
als a
nd o
utco
mes
dee
med
of
valu
e by
fam
ilies
wor
king
with
serv
ice
prov
ider
s
The
resu
lts o
f th
e st
udy
will
be
of m
ajor i
mpo
rtan
ce
in h
elpi
ng P
SF e
valu
ate
the
valu
e of
FTC
in a
chie
ving
de
sired
out
com
es a
nd im
prov
ing
serv
ice
with
chi
ldre
n an
d fa
mili
es.
Plea
se re
view
the
Info
rmed
Con
sent
For
m. I
f yo
u ha
ve
any
ques
tions
rega
rdin
g th
is st
udy
and
your
pos
sible
part
icip
atio
n, p
leas
e co
ntac
t Dr.
Perr
y at
(850
) 322
-19
01; I
nstit
ute
for C
hild
and
Fam
ily S
ervi
ces R
esea
rch,
14
00 V
illag
e Sq
uare
Blv
d., S
uite
3-2
58, T
allah
asse
e, FL
32
312;
or R
obin
_Per
ry_P
hd@
com
cast
.net
.
STU
Dy O
N F
amil
y Te
am C
ON
FeRe
NCi
NG
The
Part
ners
hip
for
Stud
y Fa
mili
es
is
cond
ucti
ng
an
eval
uati
on o
f Fa
mily
Tea
m C
onfe
renc
ing
(FTC
). a
sum
mar
y of
the
Stu
dy a
nd P
urpo
se i
s de
taile
d be
low
. Pl
ease
see
th
e in
form
ed C
onse
nt F
orm
(pr
ovid
ed w
ith
this
bro
chur
e)
for
mor
e de
tails
reg
ardi
ng t
he s
tudy
and
you
r po
ssib
le
part
icip
atio
n. y
ou w
ill h
ave
an o
ppor
tuni
ty t
o ta
lk w
ith
a Fa
mily
Tea
m C
onfe
renc
e Co
ordi
nato
r (w
ho w
ill c
all
you)
ab
out
FTCs
and
the
stu
dy a
nd m
eet
and
disc
uss
this
stu
dy
befo
re s
igni
ng a
ny c
onse
nt f
orm
.
SUm
maR
yYo
u an
d yo
ur fa
mily
are
bei
ng a
sked
to p
artic
ipat
e in
a re
sear
ch st
udy
on se
rvic
es p
rovi
ded
by th
e Pa
rtne
rshi
p fo
r Stro
ng F
amili
es (h
erei
n re
ferr
ed to
as P
SF).
The
inde
pend
ent e
valu
ator
/Prin
cipa
l Inv
estig
ator
for t
his
stud
y is
Robi
n Pe
rry,
Ph.D
. fro
m th
e In
stitu
te fo
r Chi
ld
and
Fam
ily S
ervi
ces R
esea
rch.
You
wer
e se
lect
ed a
s a
poss
ible
par
ticip
ant i
n th
is st
udy
beca
use
you
are
curr
ently
invo
lved
with
the
Flor
ida
Stat
e D
epar
tmen
t of
Chi
ldre
n an
d Fa
mili
es (D
CF) i
n-ho
me
supe
rvisi
on
or o
ut-o
f-hom
e ca
re in
Circ
uit 3
and
8.
PURP
OSe
OF
The
STU
DyTh
e pu
rpos
e of
the
stud
y is
to te
st d
iffer
ent a
ppro
ache
s of
Fam
ily T
eam
Con
fere
ncin
g, a
mee
ting
that
invo
lves
va
rious
par
ticip
ants.
Par
ticip
ants
can
incl
ude,
but a
re n
ot
limite
d to
: par
ent(s
), ca
regi
ver(s
), th
eir
child
ren,
oth
er
fam
ily m
embe
rs, f
riend
s of
the
fam
ily a
nd p
rofe
ssio
nals
from
DCF
, PSF
and
oth
er c
omm
unity
-bas
ed a
genc
ies.

Visit us at pfsf.org to learn more about the innovative ways we’re changing child welfare!

5950 NW 1st Place, Suite A Gainesville, FL 32607
www.pfsf.org