Embed Size (px)
Citation preview

Journal of Biomedical Therapy 2010)Vol.4,No.1
Imprinting in Early Life Predisposes to Diseases in Adulthood By Marietta Kaszkin-Bettag, PhD Professor of pharmacology, toxicology, and phytotherapy
Introduction
Prenatal development and early childhood are influenced by endog-enous and environmental factors that act in concert by causing struc-tural and functional changes that may persist for the life span. This phenomenon is termed “early-life programming.”1 The concept of ear-ly-life physiological “programming” or “imprinting” tries to explain the associations among prenatal envi-ronmental events, altered fetal growth and development, and the occurrence of diseases in later life (as previously reviewed).1 Such pro-gramming factors include nutrients and endogenous hormones; they may also involve environmental ex-posure to biological materials, chem-icals, drugs, medical devices, and physical factors.2 Early-life programming reflects the action of certain factors on a specific tissue during a sensitive develop-mental period or “window,” thereby affecting its development, organiza-tion, and function. Different cells and tissues are sensitive at different times; therefore, the effects of envi-ronmental challenges will have dis-tinct consequences, depending not only on the challenge involved but also on its timing.
Developmental immunotoxicity and health risks for adulthood
Developmental immunotoxicity (DIT) is an increasing health con-cern because DIT outcomes predis-pose children to certain diseases; the diseases with increasing incidences in recent decades include childhood asthma, allergic diseases, autoim-mune conditions, and childhood in-fections.3 The enhanced vulnerabili-ty of the developing immune system for environmental influences is based on unique immune maturation events that occur during critical windows in early life (e.g., negative selection against autoreactive T cells in the developing thymus).
Environmental influences on prena-tal development and immunologic responsesThe in utero environment is thought to play a major role in the risk of later life disease. The semiallogeneic pregnancy state is characterized by a suppression of graft rejection be-cause during the course of matura-tion, the potential for maternal-fetal allogeneic reactions must be mini-mized. This situation is associated with an impairment of the fetal and neonatal immune system, which may influence the specific nature of DIT outcomes.4 The last-trimester fetus and the neonate normally have de-creased T-helper cell (Th) 1–depen-dent functions, and postnatal acqui-sition of necessary Th1 capacity is a
major concern with DIT.4 Evidence for the reduced Th1 capacity of newborns is reflected by the fact that the production of interferon g (the hallmark Th1 cytokine) is se-verely reduced in the neonate. In utero exposure to pesticides, such as polychlorinated biphenyls, or to-bacco smoke is known to produce a range of immunotoxic outcomes (e.g., immunosuppression, autoim-munity, or misregulated tissue in-flammation). Beyond T cells, den-dritic cells and macrophages are sensitive targets to chemicals, result-ing in macrophage dysregulation, changes in innate immunity, and in-flammatory damage.
Immune response during early lifeA cesarean delivery can affect neo-natal immune responses and can in-crease the risk of atopy. Children born by cesarean section have a 2-fold higher odds of atopy than those born by vaginal delivery (odds ratio, 2.1; 95% confidence interval, 1.1-3.9). In multivariate analyses, birth by cesarean section was sig-nificantly associated with increased odds of allergic rhinitis (odds ratio, 1.8; 95% confidence interval, 1.0-3.1), but not of asthma.5 This study demonstrated that cesarean delivery may be associated with allergic rhinitis and atopy, particularly among children with a parental his-tory of allergies. This could be ex-plained by lack of contact with the
) I n Fo c u s
) 4
Journal of Biomedical Therapy 2010)Vol.4,No.1
maternal vaginal/fecal flora during cesarean delivery.During the neonatal period, the mammalian host is exposed through mucosal surfaces to a broad spec-trum of environmental macromole-cules and microbial agents. The neo-natal mucosa has all major elements of innate and adaptive immunologic repertoire. The early neonatal pe-riod is also characterized by a rela-tive deficiency in antigen-presenting cell functions, altered cell-mediated immune responses, and a relative in-crease in apoptosis and eosinophilic responses.6 Recent investigations have shown that the nature of mu-cosal microflora acquired in early infancy determines the outcome of mucosal inflammation and the sub-sequent development of mucosal disease, autoimmunity, and allergic disorders later in life. It seems that altered mucosal microflora in early childhood affect signaling reactions that determine T-cell differentiation and/or the induction of tolerance. Reduced Th1 and increased Th2 cytokine expression in the respira-tory tract, associated with increased allergic disease, has been correlated with reduced exposure to microbial agents associated with Th1 respons-es. These observations suggest that the interaction between the external environment and the mucosal tissues in the early neonatal period and in-fancy may be critical in directing and controlling the expression of disease-specific responses in later life.
Thus, early-life toxicologic exposure to xenobiotic infectious agents or stress may be pivotal in producing the later-life onset of increased childhood infections; neurologic disorders; fatigue-related illnesses; autoimmune diseases; allergic dis-eases, including asthma; food aller-gies; and even cancers (e.g., child-hood leukemia).7
Childhood allergic diseasesThe incidence of asthma in industri-alized countries has increased dra-matically in recent decades, with the consequences of significant public health cost. In 2002, there were al-ready approximately 16 million ad-olescents with asthma.4 For child-hood allergic asthma and rhinitis in particular, various toxins, infectious agents, airborne pollutants, and ma-ternal smoking were identified as significant risk factors.2 In addition,
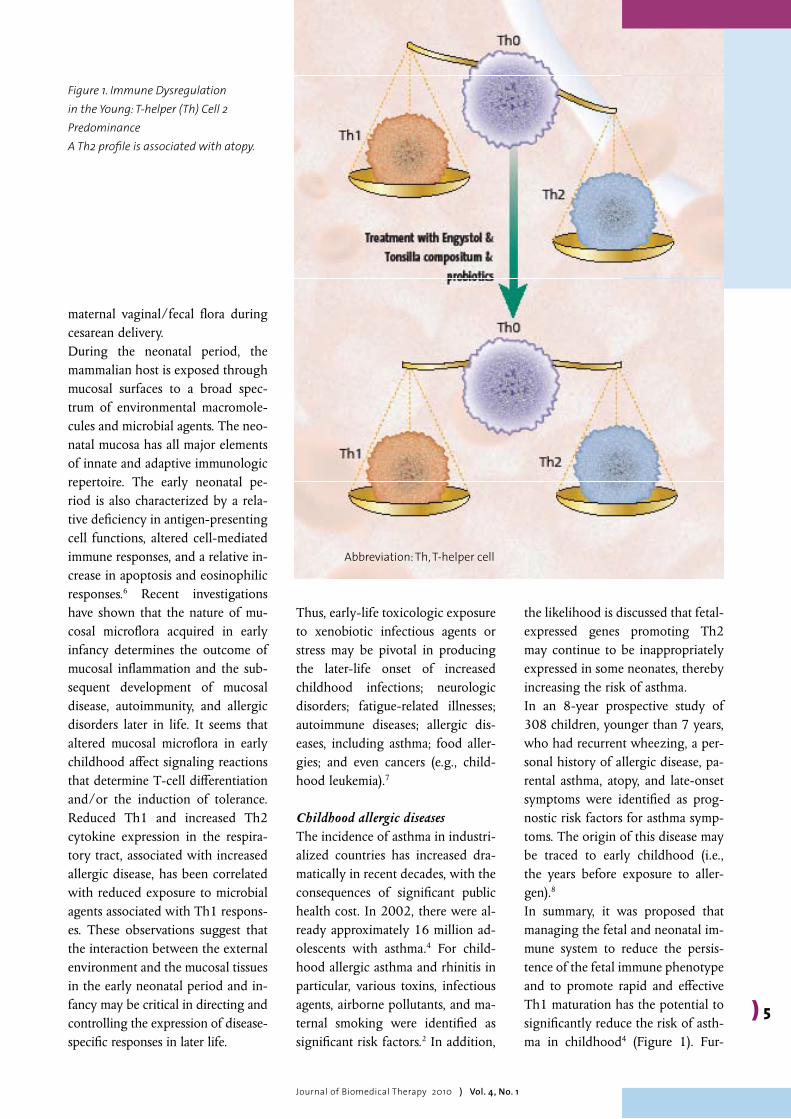
the likelihood is discussed that fetal-expressed genes promoting Th2 may continue to be inappropriately expressed in some neonates, thereby increasing the risk of asthma. In an 8-year prospective study of 308 children, younger than 7 years, who had recurrent wheezing, a per-sonal history of allergic disease, pa-rental asthma, atopy, and late-onset symptoms were identified as prog-nostic risk factors for asthma symp-toms. The origin of this disease may be traced to early childhood (i.e., the years before exposure to aller-gen).8 In summary, it was proposed that managing the fetal and neonatal im-mune system to reduce the persis-tence of the fetal immune phenotype and to promote rapid and effective Th1 maturation has the potential to significantly reduce the risk of asth-ma in childhood4 (Figure 1). Fur-
) 5
Figure 1. Immune Dysregulation in the Young: T-helper (Th) Cell 2 PredominanceA Th2 profile is associated with atopy.
Abbreviation: Th, T-helper cell
Journal of Biomedical Therapy 2010)Vol.4,No.1
) I n Fo c u s
thermore, an increased risk for sev-eral childhood allergic diseases was identified after maternal use of anti-biotics during pregnancy.2
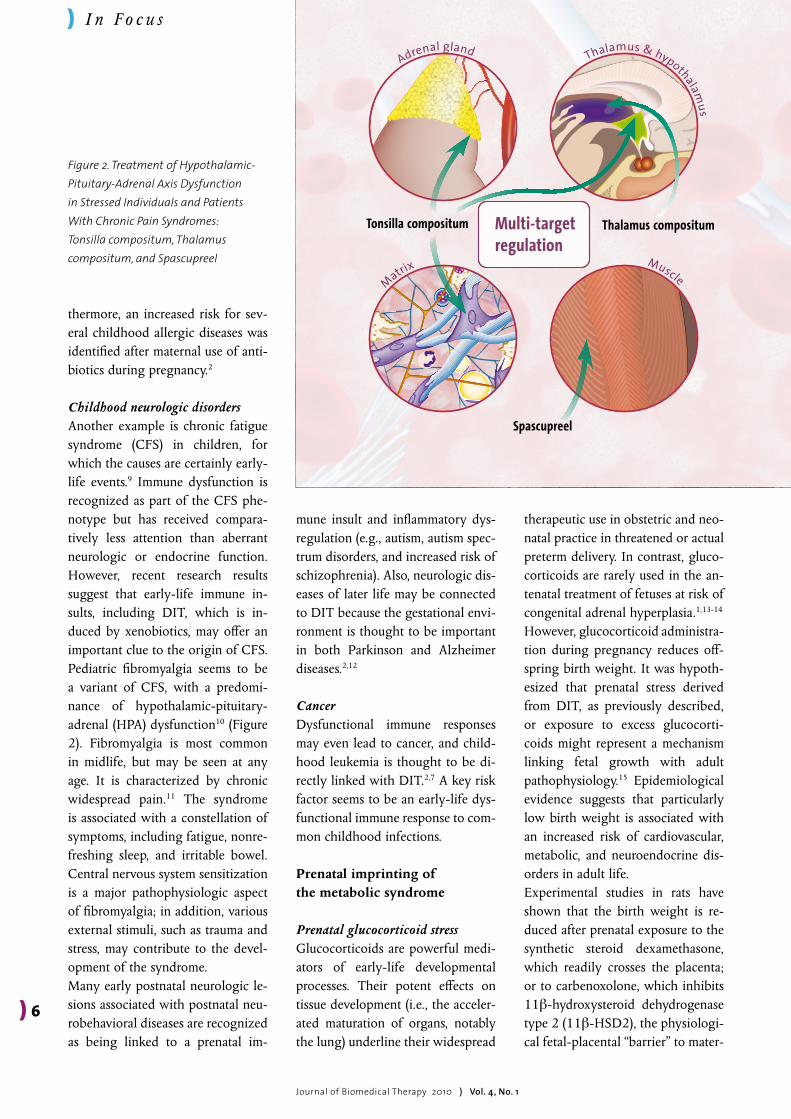
Childhood neurologic disordersAnother example is chronic fatigue syndrome (CFS) in children, for which the causes are certainly early-life events.9 Immune dysfunction is recognized as part of the CFS phe-notype but has received compara-tively less attention than aberrant neurologic or endocrine function. However, recent research results suggest that early-life immune in-sults, including DIT, which is in-duced by xenobiotics, may offer an important clue to the origin of CFS. Pediatric fibromyalgia seems to be a variant of CFS, with a predomi-nance of hypothalamic-pituitary-adrenal (HPA) dysfunction10 (Figure 2). Fibromyalgia is most common in midlife, but may be seen at any age. It is characterized by chronic widespread pain.11 The syndrome is associated with a constellation of symptoms, including fatigue, nonre-freshing sleep, and irritable bowel. Central nervous system sensitization is a major patho phy siologic aspect of fibromyalgia; in addition, various external stimuli, such as trauma and stress, may contribute to the devel-opment of the syndrome. Many early postnatal neurologic le-sions associated with postnatal neu-robehavioral diseases are recognized as being linked to a prenatal im-
mune insult and inflammatory dys-regulation (e.g., autism, autism spec-trum disorders, and increased risk of schizophrenia). Also, neurologic dis-eases of later life may be connected to DIT because the gestational envi-ronment is thought to be important in both Parkinson and Alzheimer diseases.2,12
CancerDysfunctional immune responses may even lead to cancer, and child-hood leukemia is thought to be di-rectly linked with DIT.2,7 A key risk factor seems to be an early-life dys-functional immune response to com-mon childhood infections.
Prenatal imprinting of the metabolic syndrome
Prenatal glucocorticoid stressGlucocorticoids are powerful medi-ators of early-life developmental processes. Their potent effects on tissue development (i.e., the acceler-ated maturation of organs, notably the lung) underline their widespread
therapeutic use in obstetric and neo-natal practice in threatened or actual preterm delivery. In contrast, gluco-corticoids are rarely used in the an-tenatal treatment of fetuses at risk of congenital adrenal hyperplasia.1,13-14 However, glucocorticoid administra-tion during pregnancy reduces off-spring birth weight. It was hypoth-esized that prenatal stress derived from DIT, as previously described, or exposure to excess glu co cor ti-coids might represent a mechanism linking fetal growth with adult pathophysiology.15 Epidemiological evidence suggests that particularly low birth weight is associated with an increased risk of cardiovascular, metabolic, and neuroendocrine dis-orders in adult life. Experimental studies in rats have shown that the birth weight is re-duced after prenatal exposure to the synthetic steroid dexamethasone, which readily crosses the placenta; or to carbenoxolone, which inhibits 11b-hydroxysteroid dehydrogenase type 2 (11b-HSD2), the physiologi-cal fetal-placental “barrier” to mater-
) 6
Figure 2. Treatment of Hypothalamic-Pituitary-Adrenal Axis Dysfunction in Stressed Individuals and Patients With Chronic Pain Syndromes: Tonsilla compositum, Thalamus compositum, and Spascupreel
Thalamus & hypothalamus
MuscleMatrix
Adrenal gland
Thalamus compositum
Spascupreel
Tonsilla compositum Multi-targetregulation

Journal of Biomedical Therapy 2010)Vol.4,No.1
) I n Fo c u s
nal glucocorticoids. As adults, the offspring exhibit permanent hyper-tension, hyperglycemia, increased HPA axis activity, and behavior rem-iniscent of anxiety. Physiological variations in placental 11b-HSD2 activity correlate directly with fetal weight. In humans, 11b-HSD2 gene muta-tions cause low birth weight. More-over, low-birth-weight newborns have higher plasma levels of corti-sol as a potential stress hormone throughout adult life.1,13
In human pregnancy, severe mater-nal stress affects the offspring’s HPA axis and is associated with neuro-psychiatric disorders; moreover, ma-ternal glucocorticoid therapy may alter offspring brain function.13
Low birth weight and metabolic complications Numerous studies have revealed an association between lower birth weight and the subsequent develop-ment of the common cardiovascular and metabolic disorders of adult life (i.e., hypertension, insulin resistance, type 2 diabetes mellitus, and cardio-vascular disease–related deaths).1 The early-life events described above that alter birth weight are im-portant predictors of adult morbidi-ty.In a study16 of 22,000 US men, those who weighed less than 2.2 kg at birth had relative risks of adult hypertension of 1.26 and of type 2 diabetes of 1.75 compared with
those with an average birth weight. Similar observations were made in women.17 Moreover, the association between birth weight and later car-diometabolic disease seems largely independent of classic lifestyle risk factors (e.g., smoking, adult weight, social class, excess alcohol intake, and sedentariness) that are additive to the effect of birth weight.18
Prenatal origin of obesity, cardiovascular disease, and insulin resistanceThe fetal origins of obesity, cardio-vascular disease, and insulin resis-tance have been investigated in a wide range of epidemiological and animal studies, which revealed an adaptation of the nutritionally ma-nipulated fetus to maintain energy homeostasis for ensuring survival.19 One consequence of such develop-mental plasticity may be a long-term resetting of cellular energy homeo-stasis, most probably via epigenetic modification of genes involved in a number of key regulatory path-ways.20 For example, reduced mater-nal-fetal nutrition during early to mid gestation affects adipose tissue development and adiposity of the fetus by setting an increased number of adipocyte precursor cells.21 More important, clinically relevant adap-tations to nutritional challenges in utero may only manifest as primary components of the metabolic syn-drome if followed by a period of ac-celerated growth early in the post-
) 7
natal period and/or if offspring become obese. This suggests that obesity is not simply the result of lifestyle but has developmental de-terminants that are not of genetic origin. Thus, an understanding of the mechanisms that mediate the epigenetic changes is crucial to de-termine dietary and pharmaceutical approaches that can be applied in the postnatal period.Fetal undernutrition and hypoxia are associated with an increased sus-ceptibility to a number of adult-on-set metabolic disorders. In addition to obesity, these include cardiovas-cular disease and insulin resistance. Interestingly, premature neonates also have an increased cardiovascu-lar risk in adult life.18 It was ob-served that different feeding regi-mens, particularly in human premature neonates, have long-term metabolic consequences.19 Some de-velopmental responses may persist through several generations. For ex-ample, the female reproductive tract develops in the first half of human fetal life. Girls who were growth re-tarded in utero have a reduced uter-ine size, and this reduction may lead to impaired uterine-placental func-tion when these women become pregnant.On the other hand, there is increas-ing evidence that maternal obesity is linked to numerous metabolic com-plications, including subfertility, gestational diabetes, hypertensive disorders of pregnancy, and throm-
boembolism, with potential long-term health consequences for both mother and child. Obesity and dia-betes in women before pregnancy, gestational diabetes, and glycosuria (both diagnosed and ascertained during pregnancy) result in a higher mean birth weight and an increased offspring obesity risk.22 Thus, ma-ternal lifestyle should be altered as possible to improve maternal and fe-tal outcomes.
Metabolic syndrome in childhood
Mechanisms for the development of metabolic syndrome in early lifeThe risks for obesity and insulin re-sistance may be programmed in ute-ro as a result of decreased or in-creased birth weight because of the reasons previously described. The development of metabolic syn-drome, however, is the result of a complex interaction of specific genes and environmental influences.23 A primary mechanism accounting for perinatal adaptation is the epigenet-ic modification, via DNA methyla-tion, that affects gene expression permanently, with consequent en-docrine and behavioral changes per-sisting into adulthood. In addition, genetic polymorphisms in a regula-tory pathway may accompany envi-ronmental factors acting on fetal development and, thus, the origins of many human diseases. Polymor-
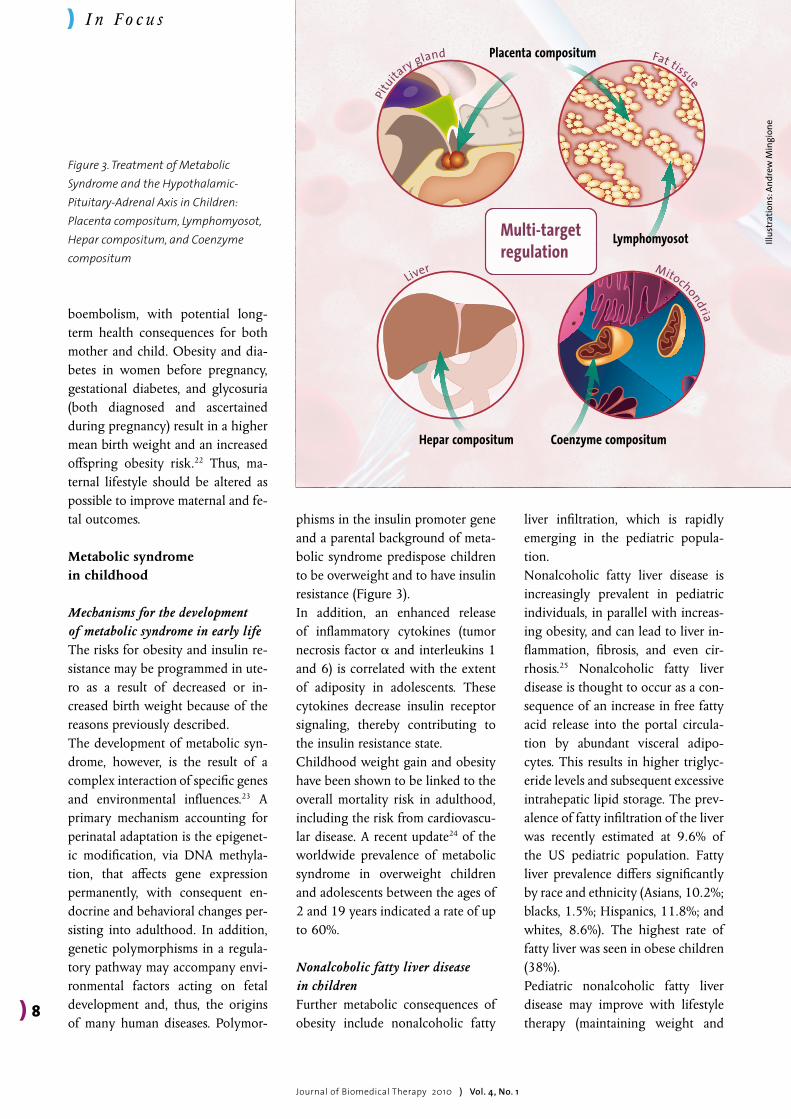
phisms in the insulin promoter gene and a parental background of meta-bolic syndrome predispose children to be overweight and to have insulin resistance (Figure 3). In addition, an enhanced release of inflammatory cytokines (tumor necrosis factor a and interleukins 1 and 6) is correlated with the extent of adiposity in adolescents. These cytokines decrease insulin receptor signaling, thereby contributing to the insulin resistance state.Childhood weight gain and obesity have been shown to be linked to the overall mortality risk in adulthood, including the risk from cardiovascu-lar disease. A recent update24 of the worldwide prevalence of metabolic syndrome in overweight children and adolescents between the ages of 2 and 19 years indicated a rate of up to 60%.
Nonalcoholic fatty liver disease in childrenFurther metabolic consequences of obesity include nonalcoholic fatty
liver infiltration, which is rapidly emerging in the pediatric popula-tion. Nonalcoholic fatty liver disease is increasingly prevalent in pediatric individuals, in parallel with increas-ing obesity, and can lead to liver in-flammation, fibrosis, and even cir-rhosis.25 Nonalcoholic fatty liver disease is thought to occur as a con-sequence of an increase in free fatty acid release into the portal circula-tion by abundant visceral adipo-cytes. This results in higher triglyc-eride levels and subsequent excessive intrahepatic lipid storage. The prev-alence of fatty infiltration of the liver was recently estimated at 9.6% of the US pediatric population. Fatty liver prevalence differs significantly by race and ethnicity (Asians, 10.2%; blacks, 1.5%; Hispanics, 11.8%; and whites, 8.6%). The highest rate of fatty liver was seen in obese children (38%).Pediatric nonalcoholic fatty liver disease may improve with lifestyle therapy (maintaining weight and
) I n Fo c u s
) 8
Journal of Biomedical Therapy 2010)Vol.4,No.1
Figure 3. Treatment of Metabolic Syndrome and the Hypothalamic- Pituitary-Adrenal Axis in Children: Placenta compositum, Lymphomyosot, Hepar compositum, and Coenzyme compositum
Placenta compositum
Lymphomyosot
Coenzyme compositumHepar compositum
Multi-targetregulation
Liver
Pitu
itary gland Fat tissue
Mitochondria
Illus
trat
ions
: And
rew
Min
gion
e

) I n Fo c u s
regular exercise) and agents that improve insulin sensitivity. Thus, identifying effective strategies for treating these obesity-related comorbi dities in children and ado-lescents is crucial to the prevention of future cardiovascular disease and poor health outcomes.
Metabolic risk factors for sexual development of female adolescentsA risk factor for female sexual de-velopment of adolescents, connected with type 2 diabetes mellitus and cardiovascular disease, is polycystic ovary syndrome (PCOS). Polycystic ovary syndrome refers to hyperan-drogenism, anovulatory menstrual cycles or oligomenorrhea, hirsutism, and the appearance of polycystic ovaries on ultrasonography.26 Insulin resistance and elevated serum luteinizing hormone levels are also common features of PCOS. Polycys-tic ovary syndrome is associated with an increased risk of type 2 dia-betes and cardiovascular events. In-sulin resistance, in conjunction with altered regulation of the HPA axis, promotes a hyperandrogenic state at the level of the ovary and adrenal gland.23 Obese adolescents with PCOS have an increased prevalence of impaired glucose tolerance, insu-lin resistance, and atherogenic lipid profiles compared with lean coun-terparts with PCOS.
Precocious pubertyAnother factor of health and social importance is precocious puberty (i.e., early sexual maturation in fe-male children). There is evidence that girls are maturing at an earlier age and that precocious puberty is increasing.27
Precocious puberty affects 1 in 5,000 children and is 10 times more common in girls. Statistics indicate that girls in the United States are maturing at an earlier age than they did 30 years ago and that the num-ber of girls with diagnosed preco-cious puberty (i.e., the appearance of secondary sex characteristics before the age of 8 years or the onset of menarche before the age of 9 years) is increasing. Early menarche has been linked to a greater risk of breast cancer as an adult. Therefore, a precocious onset would seem to increase that risk. Responsible factors included genetic and ethnic background, pediatric obesity, and environmental variables that disrupt endocrine function (i.e., chemicals, toxins, plasticizers, infant feeding methods, skin and hair products, and assisted reproductive technologies), psychosocial stress, and early exposure to a sexualized society.27 The role of obesity is often cited in association with the earlier onset of puberty. The number of overweight children aged 6 to 11 years has more than doubled in the past 20 years (from 7.0% in 1980 to 18.8% in 2004), and the rate has
more than tripled among adoles-cents aged 12 to 19 years (from 5.0% in 1980 to 17.1% in 2004).
ConclusionsThere is increasing evidence that ge-netic and epigenetic factors (i.e., early-life environmental influences) can affect prenatal development and cause structural and functional changes that may be responsible for the onset of diseases in childhood and adulthood. This concept of ear-ly-life physiological programming or imprinting1 has been examined for prenatal and postnatal exposure to endogenous factors (e.g., sex hor-mones) and exogenous agents (in-cluding toxins and drugs). Certain windows of vulnerability are identi-fied, in which different tissues, sig-naling pathways through the HPA axis, and more important, the im-mune system, are sensitive to these challenges. Many chronic diseases with an increasing incidence (e.g., childhood asthma, allergies, neuro-logic syndromes, and metabolic syn-drome) are triggered through early-life environmental risk factors and immune dysfunction. Therefore, the identification of and protection against risk factors for the develop-ing immune system and resulting immune dysfunction and tissue dam-age provide a major opportunity to reduce health risks for the most prominent chronic diseases of chil-dren and adults.|
) 9
Journal of Biomedical Therapy 2010)Vol.4,No.1

) 10
Journal of Biomedical Therapy 2010)Vol.4,No.1
References:
1. Seckl JR. Prenatal glucocorticoids and long-term programming. Eur J Endocrinol. 2004;151(suppl 3):U49-U62.
2. Dietert RR. Developmental immunotoxicol-ogy: focus on health risks. Chem Res Toxicol. 2009;22(1):17-23.
3. Dietert RR. Developmental immunotoxicol-ogy (DIT): windows of vulnerability, immune dysfunction and safety assessment. J Immuno-toxicol. 2008;5(4):401-412.
4. Dietert RR, Piepenbrink MS. The man-aged immune system: protecting the womb to delay the tomb. Hum Exp Toxicol. 2008;27(2):129-134.
5. Pistiner M, Gold DR, Abdulkerim H, Hoff-man E, Celedón JC. Birth by cesarean sec-tion, allergic rhinitis, and allergic sensi-tization among children with a parental history of atopy. J Allergy Clin Immunol. 2008;122(2):274-279.
6. Ogra PL, Welliver RC Sr. Effects of early en-vironment on mucosal immunologic homeo-stasis, subsequent immune responses and dis-ease outcome. In: Barker DJP, Bergmann RL, Ogra PL, eds. The Window of Opportunity: Pre-Pregnancy to 24 Months of Age. Vol. 61. Basel, Switzerland: Karger; 2008:145-181.
7. Dietert RR. Developmental immunotoxicity (DIT), postnatal immune dysfunction and childhood leukemia. Blood Cells Mol Dis. 2009;42(2):108-112.
8. Morais-Almeida M, Gaspar A, Pires G, Prates S, Rosado-Pinto J. Risk factors for asthma symptoms at school age: an 8-year prospective study. Allergy Asthma Proc. 2007;28(2):183-189.
9. Dietert RR, Dietert JM. Possible role for early-life immune insult including develop-mental immunotoxicity in chronic fatigue syndrome (CFS) or myalgic encephalomyeli-tis (ME). Toxicology. 2008;247(1):61-72.
10. Buskila D. Pediatric fibromyalgia. Rheum Dis Clin North Am. 2009;35(2):253-261.
11. Nampiaparampil DE, Shmerling RH. A re-view of fibromyalgia. Am J Manag Care. 2004;10(11, pt 1):794-800.
12. Barlow BK, Cory-Slechta DA, Richfield EK, Thiruchelvam M. The gestational envi-ronment and Parkinson’s disease: evidence for neurodevelopmental origins of a neu-rodegenerative disorder. Reprod Toxicol. 2007;23(3):457-470.
13. Seckl JR, Holmes MC. Mechanisms of dis-ease: glucocorticoids, their placental me-tabolism and fetal “programming” of adult
pathophysiology. Nat Clin Pract Endocrinol Metab. 2007;3(6):479-488.
14. Mercado AB, Wilson RC, Cheng KC, Wei JQ , New MI. Prenatal treatment and diagno-sis of congenital adrenal hyperplasia owing to steroid 21-hydroxylase deficiency. J Clin Endocrinol Metab. 1995;80(7):2014-2020.
15. Seckl JR, Meaney MJ. Glucocorticoid pro-gramming. Ann N Y Acad Sci. 2004;1032:63-84.
16. Curhan GC, Willett WC, Rimm EB, Spiegelman D, Ascherio AL, Stampfer MJ. Birth weight and adult hypertension, diabe-tes mellitus, and obesity in US men. Circula-tion. 1996;94(12):3246-3250.
17. Curhan GC, Chertow GM, Willett WC, et al. Birth weight and adult hyperten-sion and obesity in women. Circulation. 1996;94(6):1310-1315.
18. Irving RJ, Belton NR, Elton RA, Walker BR. Adult cardiovascular risk factors in premature babies. Lancet. 2000;355(9221):2135-2136.
19. Gluckman PD, Hanson MA, Spencer HG, Bateson P. Environmental influences during development and their later consequences for health and disease: implications for the inter-pretation of empirical studies. Proc Biol Sci. 2005;272(1564):671-677.
20. Joss-Moore LA, Lane RH. The developmen-tal origins of adult disease. Curr Opin Pediatr. 2009;21(2):230-234.
21. Symonds ME, Sebert SP, Hyatt MA, Budge H. Nutritional programming of the metabolic syndrome. Nat Rev Endocrinol. 2009;5(11):604-610.
22. Lawlor DA, Fraser A, Lindsay RS, et al. As-sociation of existing diabetes, gestational diabetes and glycosuria in pregnancy with macrosomia and offspring body mass index, waist and fat mass in later childhood: find-ings from a prospective pregnancy cohort [published online ahead of print October 20, 2009]. Diabetologia. 2010;23(1):89-97. doi:10.1007/s00125-009-1560-z.
23. Nathan BM, Moran A. Metabolic complica-tions of obesity in childhood and adoles-cence: more than just diabetes. Curr Opin Endocrinol Diabetes Obes. 2008;15(1):21-29.
24. Tailor AM, Peeters PH, Norat T, Vineis P, Romaguera D. An update on the prevalence of the metabolic syndrome in children and adolescents [published online ahead of print November 2, 2009]. Int J Pediatr Obes. doi:10.3109/17477160903281079.
25. Sundaram SS, Zeitler P, Nadeau K. The metabolic syndrome and nonalcoholic fatty
liver disease in children. Curr Opin Pediatr. 2009;21(4):529-535.
26. Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil Steril. 2004;81(1):19-25.
27. Cesario SK, Hughes LA. Precocious puberty: a comprehensive review of literature. J Ob-stet Gynecol Neonatal Nurs. 2007;36(3):263-274.
) I n Fo c u s
) 10





























