Embed Size (px)
Citation preview

Improvement in Severe Onchocercal Skin Disease After a Single Dose of Ivermectin MICHELPACQU~,M.D., Ba/timore,Mary/and, CRAIGELMETS,M.D.,ZWANNAHD.DUKULY, M.D., C/eve/and, ohio, BEATRIZMUFJOZ, M.s., Baltimore, Mary/and, ALBERTT. WHITE, M.D., C/eve/and,ohio, HUGH R.TAYLOR, M.D., Ba/timore,Mary/and, BRUCEM. GREENE, M.D., Birmingham, Alabama
PURPOSE: Skin disease is the most common clinically important manifestation of onchocer- ciasis. Ivermectin, a newly available drug, is well tolerated and effective in Onchocerca volvulus infection. However, little information is avail- able regarding its effect on onchocercal shin dis- ease. The purpose of this study was to examine, in patients with well-characterized onchoderma- titis, the effect of a single dose of ivermectin.
SU&IECTSANDMETHODS:Twenty-One persons with severe onchodermatitis were followed over a 6-month period. In order to evaluate the effect of ivermectin on their shin lesions, photographic transparencies were made before treatment and at 3 and 6 months after treatment. These were then evaluated in a blinded fashion.
RESULTS: Following a single dose of 150 pg/hg, there was a significant improvement in dermati- tis in the first 3 months after treatment. Ail 14 persons with the worst shin disease showed im- provement. The drug had no demonstrable effect on depigmented lesions over the period of obser- vation. Treatment was well tolerated.
CONCLUSION: Single-dose ivermectin shows promise as the first acceptable treatment for se- vere onchocercal dermatitis.
From the Dana Center for Preventive Ophthalmology (MP, BM. HRT), The Wilmer Institute, The Johns Hopkins University School of Medicine, Baltimore, Maryland; the Department of Dermatology (CE) and Division of Geographic Medicine and the Department of Medicine (ZDD, ATW), Case Western Reserve University and University Hospitals, Cleveland, Ohio; and the Division of Geographic Medicine (ATW. BMG), Department of Medicine, University of Alabama at Birmingham, Birmingham, Alabama.
This workwas supported in part byfundsfrom the UNDP/World Bank/ WHO Special Programme for Research and Training in Tropical Diseases (#870096). by the Onchocerciasis Chemotherapy Project of the FAO/ UNDP/World Bank/WHO Onchocerciasis Control Programme in the Vol- ta River Basin, and U.S. Public Health Service National Institutes of Health Grants RR04060, Al 15351, EY 03318, and AR 32593. Dr. Elmets is the recipient of a National Institutes of Health Research Career Devel- opment Award (AR 01765).
Requests for reprints should be addressed to Bruce M. Greene, M.D., Division of Geographic Medicine, Department of Medicine, University of Alabama at Birmingham, Birmingham, Alabama 35294.
Manuscript submitted July 6,199O. and accepted in revised form Janu- ary 12. 1991.
0 nchocerciasis is endemic in large areas of Afri- ca and Latin America. Altogether, it is esti-
mated that more than 17.5 million people are in- fected and that another 85 million are at risk of developing the disease [l]. Almost 1 million experi- ence visual impairment due to Onchocerca uoZuuZus infection, and it is known that such persons have significantly higher mortality rates than those with- out visual damage [2]. Less appreciated is the fact that onchocercal skin disease is even more common than visual impairment and is by itself a major cause of morbidity [3], leading to disability due to pruritus-related sleep deprivation and superinfec- tion, to ostracism by society, and even to suicide.
Ivermectin is a promising drug for the treatment of onchocerciasis. Preregistration studies suggest that an annual dose of 150 pglkg is the optimal regimen for safe and effective reduction of the mi- crofilarial load in people infected with 0. uoZvu2us [4-91. However, little is known about the effect of ivermectin on morbidity, particularly in regard to skin disease. We report on the effect of ivermectin on severe onchocercal dermatitis and depigmenta- tion in 21 persons treated during a community- based mass distribution trial in Liberia.
SUBJECTS AND METHODS A community-based distribution of ivermectin
was undertaken at the Liberian Agricultural Com- pany Rubber Plantation (LAC) in Grand Bassa County, Liberia, during the months of September to November [9]. Every person living at LAC was questioned by the field team as to the presence of onchocercal skin lesions and, if the response was positive, the individual was examined by the team physician. Those who were confirmed to clearly have active onchocercal dermatitis were enrolled in the study. Color photographic transparencies were taken of representative lesions before treatment was administered. During subsequent examina- tions in January and May, further photographs of the same sites were taken together with photo- graphs of any new lesions. The photographs thus provide an objective record of any change. For con- venience, the January and May follow-ups are re-
590 May 1991 The American Journal of Medicine Volume 90
IVERMECT!N TREATMENT OF ONCHODERMATITIS ,’ PACQlit ET AL
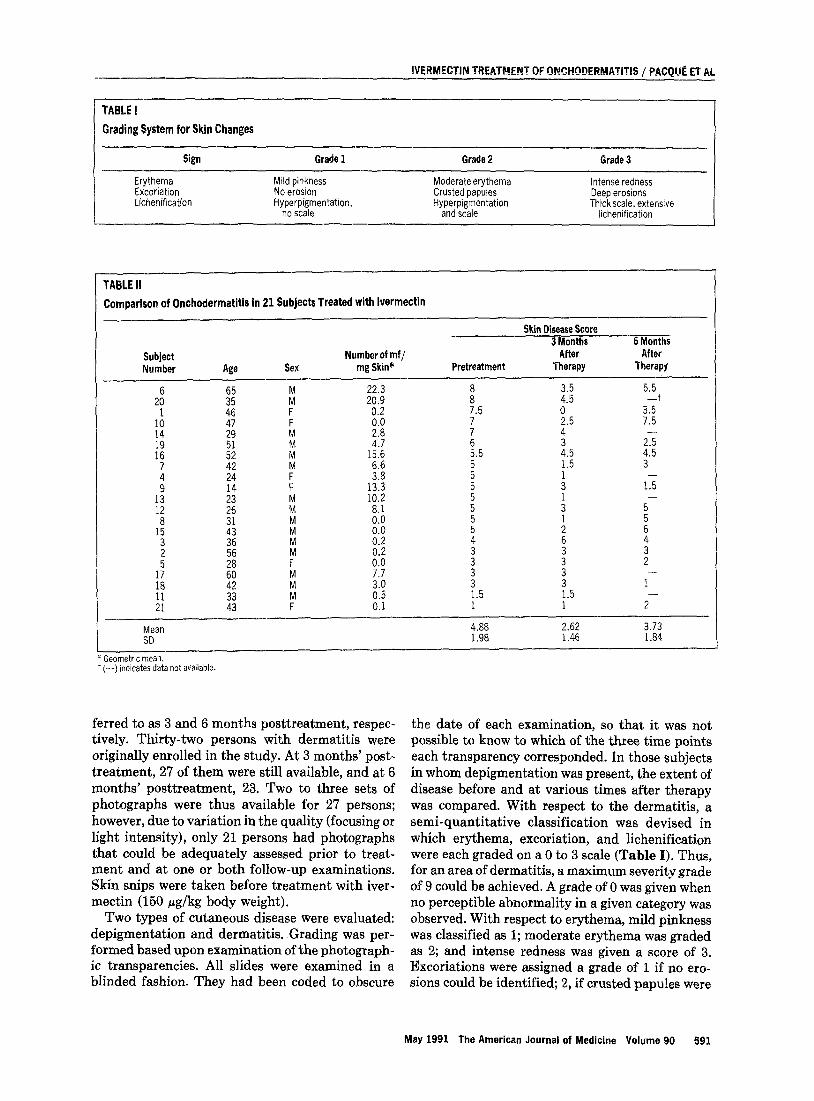
Grading System for Skin Changes
TABLE II Comparison of Onchodermatitis in 21 Subjects Treated with lvermectin
Skin Disease Score 3 Months 6 Months
Subject Number of mf/ After After Number Age Sex mg Skin* Pretreatment Therapy Therapy
2: 3"; i 20.9 22.3 ii 4.5 3.5 5.5
1 46 F 0.2 7.5 0 3x+ :: 47 29 Ll !:ii : 4 2.5 7.5
ii 5": ii 4.7
15.6 EI.5 i.5 2: 4.5
: 42 24 $" 6.6 3.8 : 1.5 3
9
fZ :3"
F 13.3 5 : 15
zt
Fi % z : 5-
1: 1 0.0 ; iz
: : i 4
1; :i
If4 i:: 0.2 i !I
2 LA Y:Y z
3 2"
!F M 3.0 3 1.5 z 1.5 1-
21 iz F E 1 1 2-
Mean 4.88 2.62 3.73 SD 1.98 1.46 1.84
* Geometric mean. t (-) indicates data not available.
ferred to as 3 and 6 months posttreatment, respec- tively. Thirty-two persons with dermatitis were originally enrolled in the study. At 3 months’ post- treatment, 27 of them were still available, and at 6 months’ posttreatment, 23. Two to three sets of photographs were thus available for 27 persons; however, due to variation in the quality (focusing or light intensity), only 21 persons had photographs that could be adequately assessed prior to treat- ment and at one or both follow-up examinations. Skin snips were taken before treatment with iver- mectin (150 pg/kg body weight).
Two types of cutaneous disease were evaluated: depigmentation and dermatitis. Grading was per- formed based upon examination of the photograph- ic transparencies. All slides were examined in a blinded fashion. They had been coded to obscure
the date of each examination, so that it was not possible to know to which of the three time points each transparency corresponded. In those subjects in whom depigmentation was present, the extent of disease before and at various times after therapy was compared. With respect to the dermatitis, a semi-quantitative classification was devised in which erythema, excoriation, and lichenification were each graded on a 0 to 3 scale (Table I). Thus, for an area of dermatitis, a maximum severity grade of 9 could be achieved. A grade of 0 was given when no perceptible abnormality in a given category was observed. With respect to erythema, mild pinkness was classified as 1; moderate erythema was graded as 2; and intense redness was given a score of 3. Excoriations were assigned a grade of 1 if no ero- sions could be identified; 2, if crusted papules were
May 1991 The American Journal of Medicine Volume 90 591
IVERMECTIN TREATMENT OF ONCHODERMATITIS / PACQUE ET AL
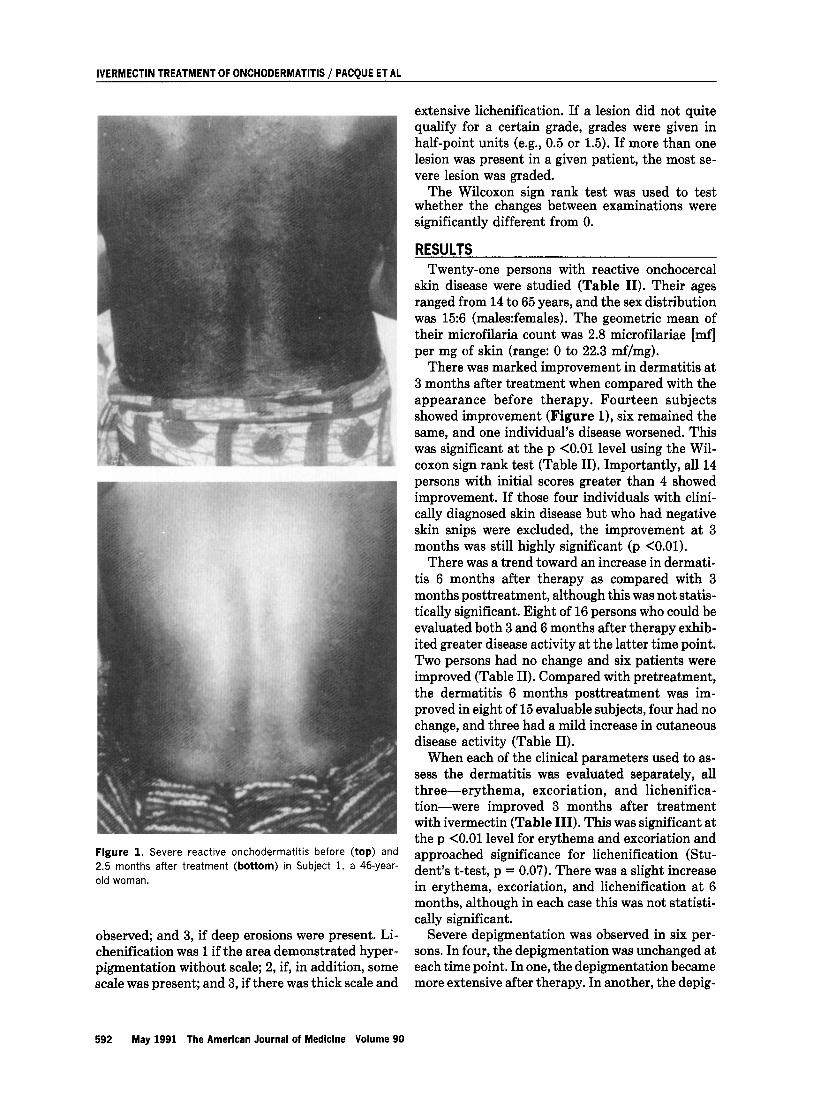
Figure 1. Severe reactive onchodermatitis before (top) and 2.5 months after treatment (bottom) in Subject 1, a 46-year- old woman.
observed; and 3, if deep erosions were present. Li- chenification was 1 if the area demonstrated hyper- pigmentation without scale; 2, if, in addition, some scale was present; and 3, if there was thick scale and
extensive lichenification. If a lesion did not quite qualify for a certain grade, grades were given in half-point units (e.g., 0.5 or 1.5). If more than one lesion was present in a given patient, the most se- vere lesion was graded.
The Wilcoxon sign rank test was used to test whether the changes between examinations were significantly different from 0.
RESULTS Twenty-one persons with reactive onchocercal
skin disease were studied (Table II). Their ages ranged from 14 to 65 years, and the sex distribution was 15:6 (males:females). The geometric mean of their microfilaria count was 2.8 microfilariae [mf] per mg of skin (range: 0 to 22.3 mf/mg).
There was marked improvement in dermatitis at 3 months after treatment when compared with the appearance before therapy. Fourteen subjects showed improvement (Figure l), six remained the same, and one individual’s disease worsened. This was significant at the p <O.Ol level using the Wil- coxon sign rank test (Table II). Importantly, all 14 persons with initial scores greater than 4 showed improvement. If those four individuals with clini- cally diagnosed skin disease but who had negative skin snips were excluded, the improvement at 3 months was still highly significant (p <O.Ol).
There was a trend toward an increase in dermati- tis 6 months after therapy as compared with 3 months posttreatment, although this was not statis- tically significant. Eight of 16 persons who could be evaluated both 3 and 6 months after therapy exhib- ited greater disease activity at the latter time point. Two persons had no change and six patients were improved (Table II). Compared with pretreatment, the dermatitis 6 months posttreatment was im- proved in eight of 15 evaluable subjects, four had no change, and three had a mild increase in cutaneous disease activity (Table II).
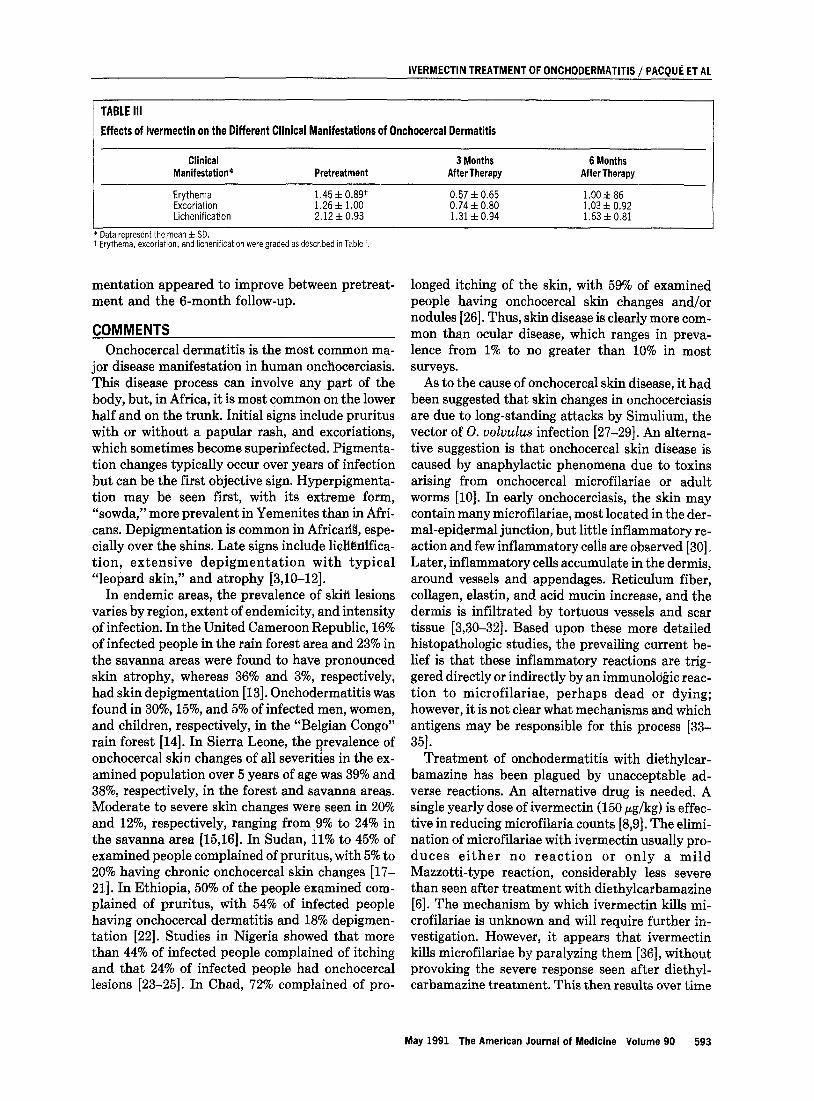
When each of the clinical parameters used to as- sess the dermatitis was evaluated separately, all three-erythema, excoriation, and lichenifica- tion-were improved 3 months after treatment with ivermectin (Table III). This was significant at the p <O.Ol level for erythema and excoriation and approached significance for lichenification (Stu- dent’s t-test, p = 0.07). There was a slight increase in erythema, excoriation, and lichenification at 6 months, although in each case this was not statisti- cally significant.
Severe depigmentation was observed in six per- sons. In four, the depigmentation was unchanged at each time point. In one, the depigmentation became more extensive after therapy. In another, the depig-
592 May 1991 The American Journal of Medicine Volume 90
IVERMECTIN TREATMENT OF ONCHODERMATITIS ,’ PACQUi ET AL
TABLE III Effects of lvermectin on the Different Clinical Manifestations of Onchocercal Dermatitis
Clinical Manifestation*
Erythema Excoriation Lichenification
Pretreatment
1.45 f 0.89t 1.26 f 1.00 2.12f0.93
3 Months 6 Months After Therapy After Therapy
0.57 f 0.65 l.OOf86 0.74 f 0.80 1.03 f 0.92 1.31 f 0.94 1.63i0.81
* Data represent the mean f SD. t Erythema. excoriation, and lichenification were graded as described in Table I.
mentation appeared to improve between pretreat- ment and the 6-month follow-up.
COMMENTS Onchocercal dermatitis is the most common ma-
jor disease manifestation in human onchocerciasis. This disease process can involve any part of the body, but, in Africa, it is most common on the lower half and on the trunk. Initial signs include pruritus with or without a papular rash, and excoriations, which sometimes become superinfected. Pigmenta- tion changes typically occur over years of infection but can be the first objective sign. Hyperpigmenta- tion may be seen first, with its extreme form, “sowda,” more prevalent in Yemenites than in Afri- cans. Depigmentation is common in Africa& espe- cially over the shins. Late signs include liolienlfica- tion, extensive depigmentation with typical “leopard skin,” and atrophy [3,10-121.
In endemic areas, the prevalence of skin lesions varies by region, extent of endemicity, and intensity of infection. In the United Cameroon Republic, 16% of infected people in the rain forest area and 23% in the savanna areas were found to have pronounced skin atrophy, whereas 36% and 3%, respectively, had skin depigmentation [13]. Onchodermatitis was found in 30%, 15%, and 5% of infected men, women, and children, respectively, in the “Belgian Congo” rain forest [14]. In Sierra Leone, the prevalence of onchocercal skin changes of all severities in the ex- amined population over 5 years of age was 39% and 38%, respectively, in the forest and savanna areas. Moderate to severe skin changes were seen in 20% and 12%, respectively, ranging from ,9% to 24% in the savanna area [15,16]. In Sudan, 11% to 45% of examined people complained of pruritus, with 5% to 20% having chronic onchocercal skin changes [17- 21]. In Ethiopia, 50% of the people examined com- plained of pruritus, with 54% of infected people having onchocercal dermatitis and 18% depigmen- tation [22]. Studies in Nigeria showed that more than 44% of infected people complained of itching and that 24% of infected people had onchocercal lesions [23-251. In Chad, 72% complained of pro-
longed itching of the skin, with 59% of examined people having onchocercal skin changes and/or nodules [26]. Thus, skin disease is clearly more com- mon than ocular disease, which ranges in preva- lence from 1% to no greater than 10% in most surveys.
As to the cause of onchocercal skin disease, it had been suggested that skin changes in onchocerciasis are due to long-standing attacks by Simulium, the vector of 0. volvulus infection [27-291. An alterna- tive suggestion is that onchocercal skin disease is caused by anaphylactic phenomena due to toxins arising from onchocercal microfilariae or adult worms [lo]. In early onchocerciasis, the skin may contain many microfilariae, most located in the der- mal-epidermal junction, but little inflammatory re- action and few inflammatory dis are observed [30]. Later, inflammatory cells accumulate in the dermis, around vessels and appendages. Reticulum fiber, collagen, elastin, and acid mucin increase, and the dermis is infiltrated by tortuous vessels and scar tissue [3,30-321. Based upon these more detailed histopathologic studies, the prevailing current be- lief is that these inflammatory reactions are trig- gered directly or indirectly by an immunologic reac- tion to microfilariae, perhaps dead or dying; however, it is not clear what mechanisms and which antigens may be responsible for this process [33- 35].
Treatment of onchodermatitis with diethylcar- bamazine has been plagued by unacceptable ad- verse reactions. An alternative drug is needed. A single yearly dose of ivermectin (150 pg/kg) is effec- tive in reducing microfilaria counts [8,9]. The elimi- nation of microfilariae with ivermectin usually pro- duces either no reaction or only a mild Mazzotti-type reaction, considerably less severe than seen after treatment with diethylcarbamazine [6]. The mechanism by which ivermectin kills mi- crofilariae is unknown and will require further in- vestigation. However, it appears that ivermectin kills microfilariae by paralyzing them [36], without provoking the severe response seen after diethyl- carbamazine treatment. This then results over time
May 1991 The American Journal of Medicine Volume 90 593

IVERMECTIN TREATMENT OF ONCHODERMATITIS / PACQUi ET AL
in a reduction in the chronic inflammation of the dermis caused by the microfilariae, allowing the skin to return to a clinically more normal appearance.
The use of ivermectin in community-based distri- bution is primarily aimed at the eventual preven- tion of blindness. Here, we have demonstrated a major additional beneficial effect, reduction of morbidity due to disfiguring or disabling skin dis- ease, the most common major disease manifesta- tions of 0. uoZuuZus infection. Importantly, the ben- eficial effect of treatment was most prominent in those with the most severe onchodermatitis. Addi- tional studies are needed to establish the optimal re-treatment interval and the long-term effects of therapy.
ACKNOWLEDGMENT We are grateful to the following people for their support and assistance: Mr. Ken Gerhart, Dr. P. Noel Williams, Dr. J. Boateng, and the staff of the Liberian Agricultural Company; Dr. Aloysius Hanson, Liberian Institute of Biomedical Research: Mrs. lnga Jackman, Johns Hopkins University; Ms. Sandra Ireland, University of Alabama at Birmingham; and Ms. Jody K. Judge, Case Western Reserve University.
REFERENCES 1. WHO Expert Committee on Onchocerciasis. Third report. Technical report series 752. Geneva: World Health Organization, 1987. 2. Kirkwood B, Smith P. Marshall T, Prost A. Relationships between mortality, visual acuity, and microfilarial load in the area of the Onchocerciasis Control Programme. Trans R Sot Trop Med Hyg 1983; 77: 862-8. 3. Buck AA, ed. Onchocerciasis: symptomatology, pathology, diagnosis. Gene- va: World Health Organization, 1974. 4. Aziz MA, Diallo S. Diop IM, Lariviere M. Efficacy and tolerance of ivermectin in human onchocerciasis. Lancet 1982; 2: 171-3. 5. Awadzi K. Dadzie KY, Schulz-Key H, Haddock DRW. Gilles MM, Aziz MA. The chemotherapy of onchocerciasis. X. An assessment of four single dose treat- ment regimens of MK-933 (ivermectin) in human onchocerciasis. Ann Trop Med Parasitol 1985; 79: 63-78. 6. Greene BM, Taylor HR, Cupp EW, et al. Comparison of ivermectin and diethyl- carbamazine in the treatment of onchocerciasis. N Engl J Med 1985; 373: 133- 8. 7. Greene BM, White AT, Newland HS, et al. Single dose therapy with ivermectin for onchocerciasis. Trans Assoc Am Physicians 1987; C: 131-8. 6. WhiteAT, Newland HS, Taylor HR. eta/. Controlled trial and dose-finding study of ivermectin for treatment of onchocerciasis. J Infect Dis 1987; 153: 463-70. 9. Pacque MC, Dukuly Z, Greene BM, et al. Community-based treatment of onchocerciasis with ivermectin. Bull WHO 1989; 67: 721-30. 10. Browne SG. Onchocercal depigmentation. Trans R Sot Trop Med Hyg 1960; 54: 325-34. 11. Anderson J. Fuglsang H, Al Zubaiby A. Onchocerciasis in Yemen with special reference to sowda. Trans R Sot Trop Med Hyg 1973; 67: 30-l. 12. Biittner W. v Laer G, Mannweiler E, Btittner M. Clinical, parasitological and serological studies on onchocerciasis in the Yemen Arab Republic. Trop Med Parasitol 1982; 33: 201-12. 13. Anderson J, Fuglsang H, Hamilton PJS, Marshall TFdeC. Studies on oncho-
cerciasis in the United Cameroon Republic. II. Comparison of onchocerciasis in rain-forest and Sudan-savanna. Trans R Sot Trop Med Hyg 1974; 68: 209-22. 14. Browne SG. Incidence and clinical manifestations of onchocerciasis in a focus in the Oriental Province of the Belgian Congo. Ann Trop Med Parasitol 1959; 53: 421-9. 15. McMahon JE. Sowa SI, Maude GH, Hudson CM, Kirkwood BR. Epidemiologi- cal studies of onchocerciasis in savanna villages of Sierra Leone. Trop Med Parasitol 1988; 39: 260-8. 16. McMahon JE, Sowa SIC. Maude GH. Hudson CM, Kirkwood BR. Epidemio- logical studies of onchocerciasis in forest villages of Sierra Leone. Trop Med Parasitol 1988; 33: 251-9. 17. Ghalib HW, Mackenzie CD, Kron MA, Williams JF, El Khalifa M, El Sheikh H. Severe onchocercal dermatitis in the Ethiopian border region of Sudan, Ann Trop Med Parasitol 1987; 81: 405-19. 18. El Sheikh H, Ghalib H, Hussein SMA, Barbiero V, Mustafe MB, Williams JF. Onchocerciasis in Sudan: the Southern Darfur focus. Trans R Sot Trop Med Hyg 1986; 80: 902-5.
19. Mackenzie CD, Williams JR, O’Day J, Ghalal I, Flockhart HA, Sisley BM. Onchocerciasis in Southwestern Sudan: parasitological and clinical characteris- tics. Am J Trop Med Hyg 1987; 36: 371-82. 20. Williams JF, Abu Yousif AH, Ballard M, Awad R, El Tayeb M. Rasheed M. Onchocerciasis in Sudan: the Abu Hamed focus. Trans R Sot Trop Med Hyg 1985; 79: 464-8. 21. Enarson DA. Observations on onchocerciasis in the Sudan Republic: ende- micity, intensity of infection and clinical features. Ann Trop Med Parasitol 1977; 71: 465-8. 22. Woodruff AW, Ten Eyck AR, Anderson J, Pettitt LE. The clinicopathological picture of onchocerciasis in Ethiopia. J Trop Med Hyg 1977; 80: 74-7. 23. Onwuliri COE, Nwoke BEB. Lawal IA, lwuala MOG. Onchocerciasis in Plateau State of Nigeria. II. The prevalence among residents around the Assob River area. Ann Trop Med Parasitol 1987; 81: 49-52. 24. Wyatt GB. Onchocerciasis in Ibarapa, Western State, Nigeria. Ann Trop Med Parasitol 1971; 65: 513-23. 25. Woodruff AW, Anderson J, Pettitt LE, Tukur M, Woodruff AHW. Someaspects of onchocerciasis in Sudan savanna and rain-forest. J Trop Med Hyg 1977; 80: 68-73. 26. Buck AA, Anderson RI, Kawata K, Hitchcock JC. Onchocerciasis: some new epidemiologic and clinical findings. Am J Trop Med Hyg 1969; 18: 217-30. 27. Gibbins EG, Loewenthal LJA. Cutaneous onchocerciasis in a Simulium dam noguminfected region of Uganda. Ann Trop Med Parasitol 1933; 27: 489-96. 28. Fuglsang H. Leopard skin and onchocerciasis [Correspondence]. Trans R Sot Trop Med Hyg 1983; 77: 881. 29. Fuglsang H, Anderson J. Marshall TFdeC. Studies on onchocerciasis in the United Cameroon Republic. V. A four year follow-up of 6 rain-forest and 6 Sudan- savanna villages. Some changes in skin and lymph nodes. Trans R Sot Trop Med Hyg 1979; 73: 118-9. 30. Connor DH. Williams PH, Helwig EB, Winslow DJ. Dermal changes in oncho- cerciasis. Arch Pathol 1969; 87: 193-200. 31. Connor DH, Morrison NE, Kerdel-Vegas F, et a/. Onchocercal dermatitis, lymphadenitis, and elephantiasis in the Ubangi territory. Human Pathol 1970; 87: 193-200. 32. Gibson DW, Connor DH, Brown HL, eta/. Onchocercal dermatitis: ultrastruc- tural studies of microfilariae and host tissues, before and after treatment with diethylcarbamazine (Hetrazan). Am J Trop Med Hyg 1970; 25: 74-87. 33. Connor DH, George GH. Gibson DW. Pathologic changes of human oncho- cerciasis: implications for future research. Rev Infect Dis 1985; 7: 809-19. 34. Mackenzie DC, Williams JF, Sisley BM, Stewart MW, O’Day J. Variation in host responses and the pathogenesis of human onchocerciasis. Rev Infect Dis 1985; 7: 802-8. 35. Bryceson ADM. What happens when microfilariae die? Trans R Sot Trop Med Hyg 1976; 70: 397-9. 36. Soboslay PT, Newland HS, White AT, et al. lvermectin effect on microfilariae of 0. volvulusafter a single oral dose in humans. Trop Med Parasitol 1987; 38: 8- 10.
594 May 1991 The American Journajof Medicine Volume 90




























