Embed Size (px)
Citation preview
BRIEF COMMUNICATION
Improving Diabetes Care for Minority, Uninsuredand Underserved Patients
Jose E. Rodrıguez • Kendall M. Campbell •
Otis W. Kirksey
� Springer Science+Business Media New York 2013
Abstract A local safety net clinic provides pharmacy
directed Diabetes Disease Management (DDM). The pur-
pose of the study was to determine if a program like this
would be successful in an underserved, uninsured poor
minority population. Clinic providers referred patients to
the DDM visits. Body Mass Index (BMI), low-density
lipoprotein, high-density lipoprotein (HDL), triglycerides
and hemoglobin A1c (HbA1c) were recorded pre- and post-
intervention. Those who participated in pre-intervention
and post-intervention visit were included in the study and
laboratory values were compared. Participants in the pilot
study showed statistically significant improvements in
HbA1c, triglycerides and BMI. HDL values did not show
statistical change. Pharmacy directed DDM can be effec-
tive in the reduction of HbA1c and triglycerides. It also
may be an effective weight loss intervention for patients
with diabetes.
Keywords Diabetes care � Underserved � Uninsured �Diabetes education � Pharmacy directed diabetes care
Background
Diabetes care can be challenging and frustrating, especially
when dealing with underserved and uninsured minority
populations that may have extreme social and economic
needs [1]. Many interventions have attempted to improve
glycemic control and decrease morbidity and mortality, but
few have been tested in underserved populations [2]. Dia-
betes and its related problems are costly to the health care
system. Recent data suggests that the US spends $306
billion annually in diabetes care [3]. As health care reform
is implemented, it is imperative that we find a way to assist
medically underserved and minority patients in their per-
sonal battles with diabetes in an effort to both reduce cost
and improve outcomes.
Neighborhood Medical Center (NMC) is a not-for-profit
clinic that provides clinical care for members of our com-
munity who are uninsured, underinsured, or recipients of
Medicaid or Medicare. As of the latest needs assessment, we
serve a population that is 60 % African American, 10 %
Hispanic or Latino, and 30 % Caucasian and other groups.
Ninety-four percent of our patients are uninsured self-pay
patients who reimburse the clinic on a sliding payment scale.
Almost 90 % of the patients pay the minimum amount,
which is currently $5. The remaining 6 % of patients have
Medicaid or Medicare [4]. Like many clinics for the under-
served, our clinic depends on funding from various charities
alongside the reimbursement patients can provide. Our
patient population also has a high prevalence of diabetes.
This study describes an intervention that can help in
diabetes management for uninsured patients. The Diabetes
J. E. Rodrıguez (&)
The Center for Underrepresented Minorities in Academic
Medicine, The Florida State University, 1115 West Call Street
#3210M, Tallahassee, FL 32306, USA
e-mail: [email protected]
K. M. Campbell
The Center for Underrepresented Minorities in Academic
Medicine, The Florida State University, 1115 West Call Street
#3210N, Tallahassee, FL 32306, USA
e-mail: [email protected]
O. W. Kirksey
The College of Pharmacy and Pharmaceutical Sciences, Florida
Agricultural and Mechanical University, 438 West Brevard St,
Tallahassee, FL 32301, USA
e-mail: [email protected]
123
J Immigrant Minority Health
DOI 10.1007/s10903-013-9965-7

Disease Management (DDM) program employs techniques
known to be effective for obesity [5] and diabetes. We
sought to test the hypothesis that DDM can be effective in
improving glycemic control in underserved and uninsured
minority patients.
At NMC, primary care is provided by family physicians
and nurse practitioners, some of whom are contracted or
volunteer their time. These volunteer physicians provide
services ranging from orthopedics, dermatology, and
gynecology. Additionally, a group of volunteer optome-
trists provide eye care to our patients. A county-sponsored
network of volunteer physicians, known as WeCare, pro-
vides those specialty services not provided on-site [4].
Patients who qualify for this program can receive virtually
any procedure at no cost to them. The WeCare program is
separate from the volunteering that occurs on-site. Many of
our on-site volunteer providers also see WeCare patients in
their private offices and hospitals, again at no cost to the
patients.
Theoretical/Conceptual Framework
Through collaboration with Florida Agricultural and
Mechanical University (FAMU), two pharmacists provide
services to the clinic at no charge. One pharmacist oversees
the dispensing pharmacy that serves the patients of the
NMC. Here, patients can receive most of their medications
at a discounted price. The other pharmacist, who is also a
Certified Diabetes Educator (CDE) provides individual
DDM during regularly scheduled office visits. Because of
the affiliation with the local universities, Medical and
Pharmacy students participate in the care of patients as a
part of their clinical rotation experiences.
Obtaining medications can be a challenge for low-
income patients, principally because of cost [6, 7]. To
address this challenge, the dispensing pharmacist super-
vises the medication distribution from the FAMU-operated
pharmacy located just across the hall from the clinic.
Medications are provided at a discounted rate, enabling
easier access for our patients. The pharmacist also works
with the patients who need emergency medications, and
supervises the patient assistance program (PAP). The PAP
allows patients to receive 3 months of medicine at no cost
provided the patient meets set financial criteria. This
enables many diabetic patients access certain costly brand
medications.
Inter-disciplinary collaboration is essential when work-
ing in safety net practices [6, 8]. The central feature of our
model is collaboration, as illustrated in Fig. 1. The PharmD/
CDE and primary care providers work together in seeking
the best outcome for the patients. The PharmD/CDE con-
sults with the treating physician, alerting him or her to
potential adverse effects as well as optimal medical man-
agement from a pharmacotherapeutic point of view. The
PharmD/CDE also provides additional services listed in
Table 1. These services can be difficult, if not impossible
for the primary care physician to provide due to time con-
straints. The PharmD/CDE spends 1 h with each new
patient, and 30 min in each follow up visit.
Methods
In order to determine the impact of these services, we
implemented a quality improvement study, which was
approved by the Institutional Review Board at FAMU.
Participants
Patients were selected by their primary care providers to
participate in the program. Patients with type 1 or type 2
diabetes who saw a primary care provider were encouraged
to attend DDM visits with the PharmD/CDE, and
were referred. Patients who kept pre-intervention and
Fig. 1 Pharmacy managed Diabetes Care Model
Table 1 Services renedered by PharmD/CDE
Services provided during patient encounters
Nutritional counseling Diabetes self-management
education
Carbohydrate counting Compliance and adherence
issues
Healthy food selections Development of patient specific
care plansFood labels
Weight-loss education and
advocacy
Medication dosage adjustments
Group Visits In conjunction with primary care
providers
Diabetic foot assessment for
sensory deficits
Review and interpretation of
laboratory data
J Immigrant Minority Health
123

post-intervention DDM appointments were included in the
study and were followed for 6 months.
Data Collection and Measures
The PharmD/CDE measured hemoglobin A1c, (HbA1c)
triglycerides, low density lipoproteins (LDL), high density
lipoproteins (HDL) and Body Mass Index (BMI) at the pre-
intervention visit and the post-intervention visit. Only
patients whose data set was complete were included in the
study. Patients missing any data were not included in this
analysis.
Analysis
Patients HbA1c, triglycerides, and HDL levels were aver-
aged for pre-intervention and post-intervention groups and
were subsequently compared. LDL data sets were not
complete due to multiple patients with triglycerides too
elevated to calculate LDL, so the LDL results could not be
compared. Statistical analysis was performed using SPSS.
Results
There were 36 patients that met criteria for inclusion in the
study. Additional patient demographic data is listed in
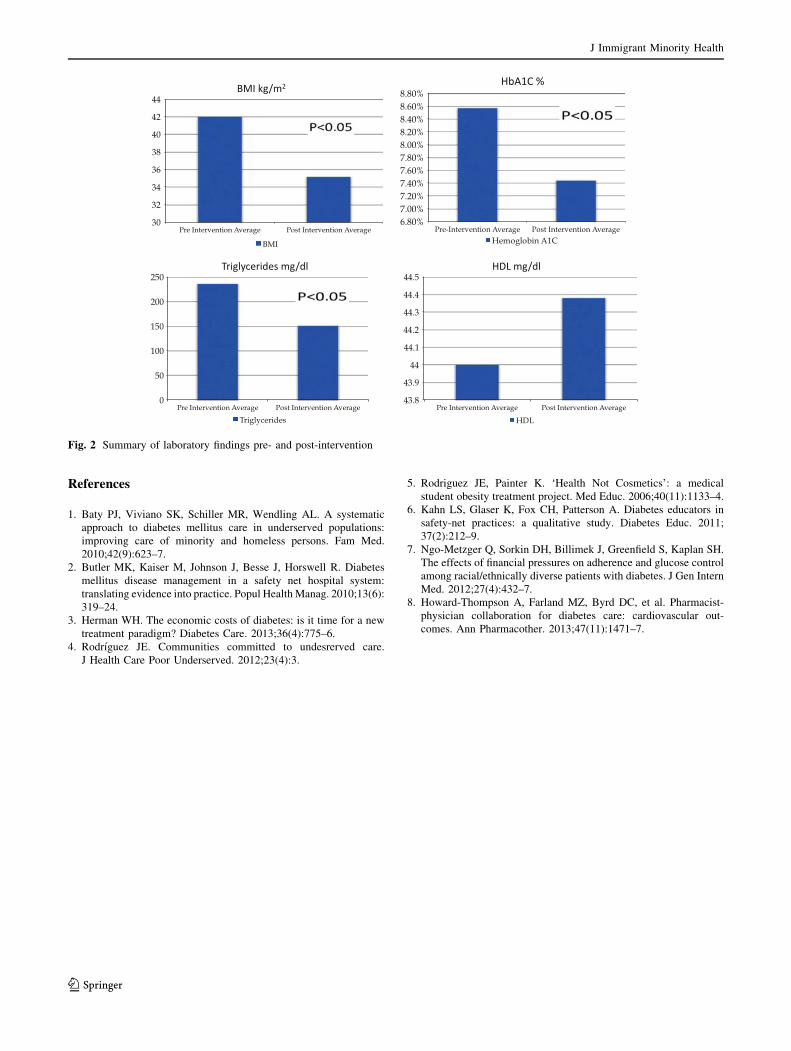
Table 2. Pre- and post-intervention data are illustrated in
‘‘Appendix’’. Results suggest that after one DDM visit
HbA1c (pre = 8.57 %, post 7.44 %, p \ 0.05), triglycer-
ides (pre = 236, post = 15.66, p \ 0.05), and BMI
(pre = 42, post 35.16, p \ 0.05) can be significantly
reduced. HDL levels, however, did not increase signifi-
cantly (pre = 44, post = 44.38, p [ 0.05).
Discussion
Treatment of diabetes among the underserved is difficult
and sometimes frustrating [6]. Lack of resources makes it
difficult for patients to keep appointments, and to consis-
tently purchase medications [4]. In spite of these existing
obstacles, those patients who consulted with the PharmD/
CDE for DDM over the study period had significant
decreases in HbA1c, triglycerides, and BMI. These find-
ings show that patients who participate in PharmD/CDE
DDM along with primary care collaboration can have
improvements in a relatively short period of time. This
finding holds promise, as it may be another modality that
can be used in the fight against obesity, in addition to group
visits and other collaborations [5].
Our study had some significant challenges and limita-
tions, one of which was a small study population. This was
due in part to the newness of the program, as well as the
difficulties involved in following a patient population as
transient as ours. Frequently, patients will obtain employ-
ment that provides commercial health insurance and leave
our practice. Another limitation was the brief time period
of the study. We suspect a longer time frame would be
beneficial, as it would allow an assessment of the potential
for lasting change.
Our study has also indicated future directions for
research. Based on these findings, a 3-year case control
study is indicated to determine the difference between
usual care and the PharmD/CDE collaborative model. We
will also encourage all of our patients to continue with their
DDM, as it is effective for those who were seen more than
once. In the future, a more detailed analysis of the patients
who did not continue with diabetes management can be
performed to identify barriers and propose solutions for
that segment of our patient population, using qualitative
measures.
New Contribution to the Literature
This study adds to the current medical literature as it
illustrates that DDM given by a PharmD/CDE can be
effective in an uninsured, underserved minority population.
In addition, it is an effective tool in promoting and
achieving clinically significant weight loss.
Appendix
See Fig. 2.
Table 2 Demographic data of study participants
Intervention cohort (N = 36)
African American 15
Caucasian 10
Hispanic or Latino 1
Not declared 10
Males 16
Females 20
Average age 51
Average follow up time (months) 6
J Immigrant Minority Health
123
References
1. Baty PJ, Viviano SK, Schiller MR, Wendling AL. A systematic
approach to diabetes mellitus care in underserved populations:
improving care of minority and homeless persons. Fam Med.
2010;42(9):623–7.
2. Butler MK, Kaiser M, Johnson J, Besse J, Horswell R. Diabetes
mellitus disease management in a safety net hospital system:
translating evidence into practice. Popul Health Manag. 2010;13(6):
319–24.
3. Herman WH. The economic costs of diabetes: is it time for a new
treatment paradigm? Diabetes Care. 2013;36(4):775–6.
4. Rodrıguez JE. Communities committed to undesrerved care.
J Health Care Poor Underserved. 2012;23(4):3.
5. Rodriguez JE, Painter K. ‘Health Not Cosmetics’: a medical
student obesity treatment project. Med Educ. 2006;40(11):1133–4.
6. Kahn LS, Glaser K, Fox CH, Patterson A. Diabetes educators in
safety-net practices: a qualitative study. Diabetes Educ. 2011;
37(2):212–9.
7. Ngo-Metzger Q, Sorkin DH, Billimek J, Greenfield S, Kaplan SH.
The effects of financial pressures on adherence and glucose control
among racial/ethnically diverse patients with diabetes. J Gen Intern
Med. 2012;27(4):432–7.
8. Howard-Thompson A, Farland MZ, Byrd DC, et al. Pharmacist-
physician collaboration for diabetes care: cardiovascular out-
comes. Ann Pharmacother. 2013;47(11):1471–7.
Fig. 2 Summary of laboratory findings pre- and post-intervention
J Immigrant Minority Health
123





























