Embed Size (px)
Citation preview
www.practicalradonc.org
Practical Radiation Oncology (2011) 1, 16–21
Special Article
Improving patient safety in radiation oncologyWilliam R. Hendee PhDa, Michael G. Herman PhDb,⁎
aMedical College of Wisconsin, Rochester, MinnesotabDepartment of Radiation Oncology, Mayo Clinic, Rochester, Minnesota
Received 5 November 2010; accepted 12 November 2010
Abstract Beginning in the 1990s, and emphasized in 2000with the release of an Institute ofMedicinereport, health care providers and institutions have dedicated time and resources to reducing errors thatimpact the safety and well-being of patients. However, in January 2010, the first of a series of articlesappeared in The New York Times that described errors in radiation oncology that grievously impactedpatients. In response, the American Association of Physicists in Medicine and the American Societyfor Radiation Oncology sponsored a working meeting entitled “Safety in Radiation Therapy: A Callto Action.” The meeting attracted 400 attendees, including medical physicists, radiation oncologists,medical dosimetrists, radiation therapists, hospital administrators, regulators, and representatives ofequipment manufacturers. The meeting was co-hosted by 14 organizations in the United States andCanada. The meeting yielded 20 recommendations that provided a pathway to reducing errors andimproving patient safety in radiation therapy facilities everywhere.© 2011 American Society for Radiation Oncology and American Association of Physicistsin Medicine.
The problem
In the early 1990s, articles began to appear in thescientific literature1,2 describing the frequency of medicalmistakes that place patients at risk. Soon thereafter, reportssurfaced in the public media regarding medical errors (eg,chemotherapy overdose, wrong-sided surgery, anesthesiaerror) that caused the death or severe disability of patients.Partly in response to these reports, an internationalconference was held in 1993 (in Rancho Palos Verdes,CA) to examine the causes and consequences of severeerrors in medicine. The conference was hosted by theAmerican Medical Association and had several organi-
This article is being published simultaneously in the January issue ofMedical Physics.
Conflicts of interest: None.⁎Corresponding author. Department of Radiation Oncology, Mayo
Clinic, 200 First St SW, Rochester, MN 55905.E-mail address: [email protected] (M.G. Herman).
1879-8500/$ – see front matter © 2011 bauthorN. Published by Elsevier Inc.reserved.doi:10.1016/j.prro.2010.11.003
zational co-sponsors. This conference spawned theNational Patient Safety Foundation3 and several otherinitiatives (eg, the Veterans Administration NationalPatient Safety Partnership) that devoted substantialresources to the identification and mitigation of medicalerrors. The National Academy of Sciences Institute ofMedicine formed the Committee on Quality of HealthCare in America that published a seminal report in 2000,entitled “To Err is Human: Building a Safer HealthSystem.”4 This report estimated that between 44,000 and98,000 patients died in the United States in 1997 as aconsequence of medical errors, and it captured theattention of health care providers and public interestgroups. For the past decade, programs to reduce medicalerrors have been established in most of the nation'shospitals and health care organizations.
Errors are known to occur in radiation oncology. Thetreatment of cancer patients with radiation is complicatedfor several reasons: the complexity of the disease, thesophistication of the technologies employed, the
on behalf of the American Society for Radiation Oncology. All rights
Improving patient safety 17Practical Radiation Oncology: January-March 2011
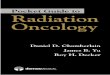
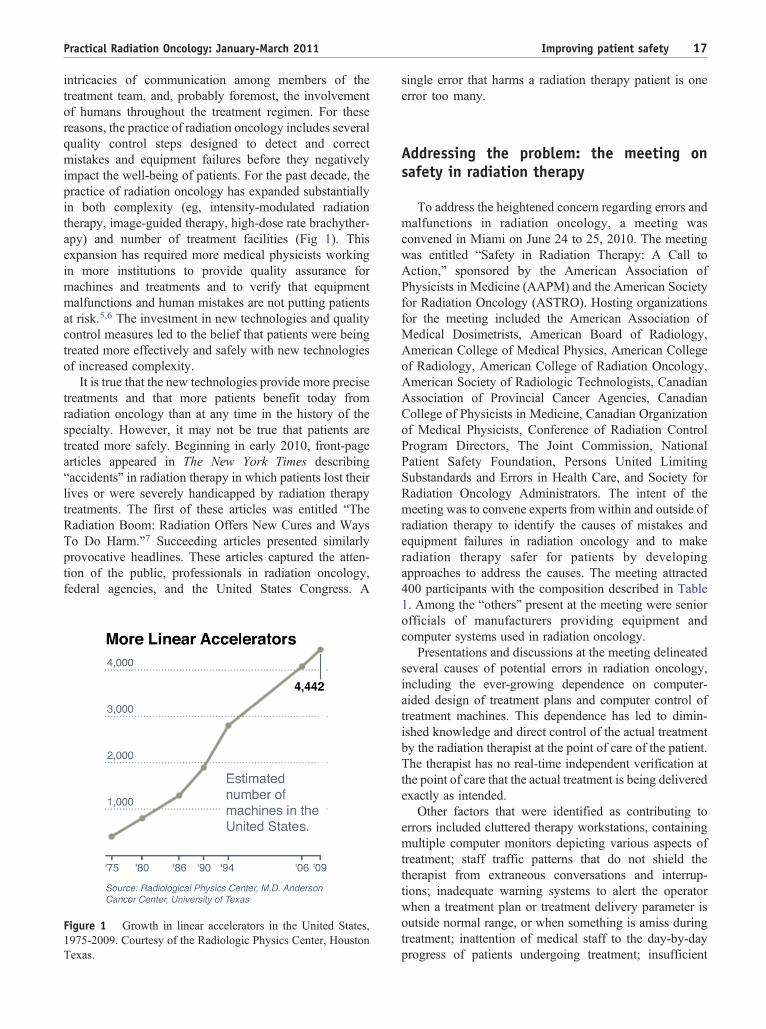
intricacies of communication among members of thetreatment team, and, probably foremost, the involvementof humans throughout the treatment regimen. For thesereasons, the practice of radiation oncology includes severalquality control steps designed to detect and correctmistakes and equipment failures before they negativelyimpact the well-being of patients. For the past decade, thepractice of radiation oncology has expanded substantiallyin both complexity (eg, intensity-modulated radiationtherapy, image-guided therapy, high-dose rate brachyther-apy) and number of treatment facilities (Fig 1). Thisexpansion has required more medical physicists workingin more institutions to provide quality assurance formachines and treatments and to verify that equipmentmalfunctions and human mistakes are not putting patientsat risk.5,6 The investment in new technologies and qualitycontrol measures led to the belief that patients were beingtreated more effectively and safely with new technologiesof increased complexity.
It is true that the new technologies provide more precisetreatments and that more patients benefit today fromradiation oncology than at any time in the history of thespecialty. However, it may not be true that patients aretreated more safely. Beginning in early 2010, front-pagearticles appeared in The New York Times describing“accidents” in radiation therapy in which patients lost theirlives or were severely handicapped by radiation therapytreatments. The first of these articles was entitled “TheRadiation Boom: Radiation Offers New Cures and WaysTo Do Harm.”7 Succeeding articles presented similarlyprovocative headlines. These articles captured the atten-tion of the public, professionals in radiation oncology,federal agencies, and the United States Congress. A
Figure 1 Growth in linear accelerators in the United States,1975-2009. Courtesy of the Radiologic Physics Center, HoustonTexas.
single error that harms a radiation therapy patient is oneerror too many.
Addressing the problem: the meeting onsafety in radiation therapy
To address the heightened concern regarding errors andmalfunctions in radiation oncology, a meeting wasconvened in Miami on June 24 to 25, 2010. The meetingwas entitled “Safety in Radiation Therapy: A Call toAction,” sponsored by the American Association ofPhysicists in Medicine (AAPM) and the American Societyfor Radiation Oncology (ASTRO). Hosting organizationsfor the meeting included the American Association ofMedical Dosimetrists, American Board of Radiology,American College of Medical Physics, American Collegeof Radiology, American College of Radiation Oncology,American Society of Radiologic Technologists, CanadianAssociation of Provincial Cancer Agencies, CanadianCollege of Physicists in Medicine, Canadian Organizationof Medical Physicists, Conference of Radiation ControlProgram Directors, The Joint Commission, NationalPatient Safety Foundation, Persons United LimitingSubstandards and Errors in Health Care, and Society forRadiation Oncology Administrators. The intent of themeeting was to convene experts from within and outside ofradiation therapy to identify the causes of mistakes andequipment failures in radiation oncology and to makeradiation therapy safer for patients by developingapproaches to address the causes. The meeting attracted400 participants with the composition described in Table1. Among the “others” present at the meeting were seniorofficials of manufacturers providing equipment andcomputer systems used in radiation oncology.
Presentations and discussions at the meeting delineatedseveral causes of potential errors in radiation oncology,including the ever-growing dependence on computer-aided design of treatment plans and computer control oftreatment machines. This dependence has led to dimin-ished knowledge and direct control of the actual treatmentby the radiation therapist at the point of care of the patient.The therapist has no real-time independent verification atthe point of care that the actual treatment is being deliveredexactly as intended.
Other factors that were identified as contributing toerrors included cluttered therapy workstations, containingmultiple computer monitors depicting various aspects oftreatment; staff traffic patterns that do not shield thetherapist from extraneous conversations and interrup-tions; inadequate warning systems to alert the operatorwhen a treatment plan or treatment delivery parameter isoutside normal range, or when something is amiss duringtreatment; inattention of medical staff to the day-by-dayprogress of patients undergoing treatment; insufficient

Table 1 Composition of participants at Safety in RadiationTherapy: A Call to Action
Who was there?
45% Medical physicists15% Administrators10.5% Radiation oncologists7% Radiation therapists2.5% Dosimetrists2.2% Regulators6.8% Other11% Nonresponders
18 W.R. Hendee, M.G. Herman Practical Radiation Oncology: January-March 2011
quality oversight or inaccurate calibrations by physicists;failure of manufacturers to respond to problems intreatment devices identified by physicists; inability orunwillingness of users to attend product trainingeducational sessions for complex equipment; lack ofempowerment of staff to challenge decisions made higherin the hierarchy; absence of specific policies andprocedures defining treatment processes and responsibil-ities of the treatment team; and absence of explicitdirections on how to react to unexpected conditions orevents during treatment.
Participants at the meeting concluded that theseproblems are best addressed through a multidisciplinaryapproach that includes members of treatment teams(radiation oncologists, physicists, dosimetrists, radiationtherapists, nurses) working with vendors, administrators,and regulators.
Participants at the meeting acknowledged that althougherrors in radiation oncology can be reduced, theycannot be eliminated because the treatment process iscomplex, the hardware and software technology canmalfunction, the communications can be misunderstood,and, especially, because humans are involved. There-
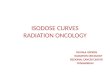
Figure 2 Hierarchy of short-term effectiveness in hazardmitigation in which the top is most effective. Courtesy of J.Goldwein, Elekta AB.
fore, treatment approaches must be fault tolerant (ie,they must be designed to catch and correct errors beforethey can harm the patient). There was considerablediscussion regarding the hierarchy of effectiveness inmitigating errors presented in Fig 2. In this illustration,short-term effectiveness in reducing error increases fromthe bottom to the top of the figure, suggesting that forquick results, automated forcing functions and con-straints on operation are most effective, and educationand training are least effective.
ASTRO has responded to the challenge of improvingquality and reducing errors in radiation oncology bydeveloping a 6-point action plan to improve the safety ofpatients undergoing radiation therapy. The action plan isoutlined in Table 2.
Presentations and discussions at the meeting yieldedseveral recommendations. These recommendations arepresented as follows:
Recommendations
1. As the complexity of treatment devices increases,control over the devices should be simplified. Theinterface of operators with treatment machinesshould be streamlined, layered, and standardized tothe extent possible. Therapist workstations shouldnot be a collection of monitor screens and multiplekeyboards simultaneously depicting and controllingmultiple treatment features and variables that aredisplayed differently from one treatment machine tothe next. Instead, they should present information ina tiered fashion, and a single keyboard should besufficient to access the information. The interfaceshould be ergonomically engineered to providelogical access to and control of treatment variablesin a call-up and early-alert fashion under control ofthe radiation therapist.
2. Radiation therapist workstations should bedesigned according to principles of human factorsengineering. Workstations should be clutter-freeand designed to access information on demand,with an integrated early warning system. Trafficnear the workstation should be minimal, as shouldextraneous noise and idle conversations. Therapistsshould not be interrupted while treatments areunder way.
3. Return control to the point of care. The thera-pist must have greater knowledge of the correct-ness of radiation delivery to the patient duringtreatment. This knowledge is essential if thetherapist is to maintain control of the deliveryprocess and take appropriate action if somethingshould happen that is inconsistent with thetreatment plan. Greater control must be provided to

Table 2 ASTRO 6-point action plan
Create an anonymous national database for event reportingEnhance and accelerate the ASTRO/ACR PracticeAccreditation Program
Expand education and training programs to include intensivefocus on quality and safety
Develop tools for cancer patients to use in discussions withradiation oncologists
Accelerate development of the IHE-RO (Integrated HealthEnterprise – Radiation Oncology) program
Advocate for passage of the CARE (Consistency,Accountability, Responsibility, Excellence in MedicalImaging and Radiation Therapy) act
ACR, American College of Radiology; ASTRO, American Societyfor Radiation Oncology.
Improving patient safety 19Practical Radiation Oncology: January-March 2011
the operator so that treatment can be terminated ifsomething unexpected occurs.
4. Provide improved early warnings. Early warningsystems alert the operator to an unusual feature of thetreatment plan or a possible malfunction in the treatmentdevice. These systems should be more comprehensiveand fail-safe than those currently available, and anoperator should be instructed to pay attention to earlywarnings and not reset the system to continue operationunless he or she is sure that the warning is erroneous orthe problem has been corrected. Early warning systemsshould include an automated treatment system andprocess checks that compare performance with estab-lished performance metrics. Checks that fall outside awindow of acceptable performance should trigger analert that identifies the aberrant condition and offerspossible solutions.
5. Vendors should quickly and intelligibly addressconcerns reported by physicists and other membersof the treatment team. Qualitative and dismissiveresponses are not satisfactory answers to a problem.Every question raised by a user deserves an answer,and the answer should be useful, timely, under-standable, and comprehensive.
6. User groups. Professional associations (AAPM andASTRO) should sponsor “user groups” of indivi-duals who use complex treatment machines fromparticular vendors. Vendor representatives should beincluded in the groups, but agendas should be setand meetings should be run by members of thesponsoring organizations. User groups should pro-vide a forum for open discussion between users andvendors on the operational issues (including safetyconcerns) related to the vendor's equipment.
7. The billing process should be simplified, and theradiation therapist should not be burdened withbilling duties while overseeing patient treatments.Some institutions expect radiation therapists tohandle billing forms while patients are being
treated. This expectation of therapists to multitaskduring patient treatments risks devoting inadequateattention to either task and providing insufficientdiligence during the process of treatment delivery.
8. Develop recommended staffing levels. Radiationtreatment technologies have become highly complexdevices that require greater diligence in their use byall members of the treatment team. Staffing levelsrecommended years ago when treatments andtreatment devices were much simpler are no longerrelevant. A task force should be appointed byprofessional organizations to develop new staffinglevels for oncologists, physicists, and therapistsinvolved in radiation oncology procedures. The taskforce should be sponsored by ASTRO, AAPM, andthe American Society of Radiologic Technologists.
9. Radiation therapy facilities should use techniquesfor failure mode effects analysis to identify potentialsources of error and root cause analysis to identifyand correct errors when they occur. Methods forassessing the potential for error (eg, failure modeeffects analysis) and the cause of errors when theyoccur are very useful approaches for identifying andreducing errors and malfunctions.8 These methodsshould be used by all radiation oncology facilities intheir efforts to improve the safety of patients. AnAAPM task group (Task Group 100 on Methods forEvaluating Quality Assurance Needs in RadiationTherapy) is completing a report on improved qualitymeasures based on risk analysis and techniques thatuse failure mode effects analysis, fault tree analysis,and other analytical tools. This report should beuseful in establishing baseline quality measures forradiation therapy facilities.
10. Error reporting systems should be developed inradiation therapy. There is growing interest in theanonymous reporting of mistakes and equipmentfailures in radiation oncology. Through a reportingprocess, members of a treatment team could bealerted to problems occurring elsewhere that may berelevant to their institution. Multiple reports of anequipment problem would notify vendors to theneed for rapid action. Regulatory agencies (UnitedStates Food and Drug Administration and theNuclear Regulatory Commission) and state regula-tory authorities acting through the Conference ofRadiation Control Program Directors have allexpressed interest in establishing a reporting pro-cess. At the international level, the InternationalAtomic Energy Agency is developing a voluntaryreporting system called Safety in Radiation Oncol-ogy to compile reports of medical radiation“incidents” that put patients at risk. An errorreporting system should be a centralized, modalityindependent repository that is easy to use, univer-sal, anonymous, and nonpunitive. It should use
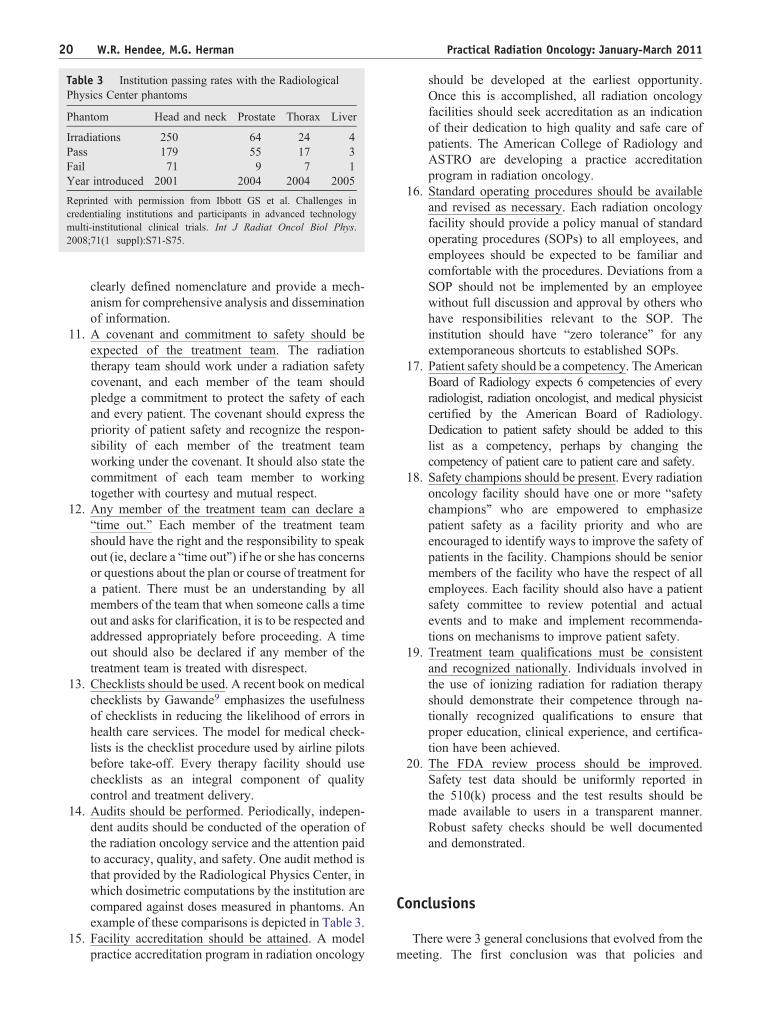
Table 3 Institution passing rates with the RadiologicalPhysics Center phantoms
Phantom Head and neck Prostate Thorax Liver
Irradiations 250 64 24 4Pass 179 55 17 3Fail 71 9 7 1Year introduced 2001 2004 2004 2005
Reprinted with permission from Ibbott GS et al. Challenges incredentialing institutions and participants in advanced technologymulti-institutional clinical trials. Int J Radiat Oncol Biol Phys.2008;71(1 suppl):S71-S75.
20 W.R. Hendee, M.G. Herman Practical Radiation Oncology: January-March 2011
clearly defined nomenclature and provide a mech-anism for comprehensive analysis and disseminationof information.
11. A covenant and commitment to safety should beexpected of the treatment team. The radiationtherapy team should work under a radiation safetycovenant, and each member of the team shouldpledge a commitment to protect the safety of eachand every patient. The covenant should express thepriority of patient safety and recognize the respon-sibility of each member of the treatment teamworking under the covenant. It should also state thecommitment of each team member to workingtogether with courtesy and mutual respect.
12. Any member of the treatment team can declare a“time out.” Each member of the treatment teamshould have the right and the responsibility to speakout (ie, declare a “time out”) if he or she has concernsor questions about the plan or course of treatment fora patient. There must be an understanding by allmembers of the team that when someone calls a timeout and asks for clarification, it is to be respected andaddressed appropriately before proceeding. A timeout should also be declared if any member of thetreatment team is treated with disrespect.
13. Checklists should be used. A recent book on medicalchecklists by Gawande9 emphasizes the usefulnessof checklists in reducing the likelihood of errors inhealth care services. The model for medical check-lists is the checklist procedure used by airline pilotsbefore take-off. Every therapy facility should usechecklists as an integral component of qualitycontrol and treatment delivery.
14. Audits should be performed. Periodically, indepen-dent audits should be conducted of the operation ofthe radiation oncology service and the attention paidto accuracy, quality, and safety. One audit method isthat provided by the Radiological Physics Center, inwhich dosimetric computations by the institution arecompared against doses measured in phantoms. Anexample of these comparisons is depicted in Table 3.
15. Facility accreditation should be attained. A modelpractice accreditation program in radiation oncology
should be developed at the earliest opportunity.Once this is accomplished, all radiation oncologyfacilities should seek accreditation as an indicationof their dedication to high quality and safe care ofpatients. The American College of Radiology andASTRO are developing a practice accreditationprogram in radiation oncology.
16. Standard operating procedures should be availableand revised as necessary. Each radiation oncologyfacility should provide a policy manual of standardoperating procedures (SOPs) to all employees, andemployees should be expected to be familiar andcomfortable with the procedures. Deviations from aSOP should not be implemented by an employeewithout full discussion and approval by others whohave responsibilities relevant to the SOP. Theinstitution should have “zero tolerance” for anyextemporaneous shortcuts to established SOPs.
17. Patient safety should be a competency. TheAmericanBoard of Radiology expects 6 competencies of everyradiologist, radiation oncologist, and medical physicistcertified by the American Board of Radiology.Dedication to patient safety should be added to thislist as a competency, perhaps by changing thecompetency of patient care to patient care and safety.
18. Safety champions should be present. Every radiationoncology facility should have one or more “safetychampions” who are empowered to emphasizepatient safety as a facility priority and who areencouraged to identify ways to improve the safety ofpatients in the facility. Champions should be seniormembers of the facility who have the respect of allemployees. Each facility should also have a patientsafety committee to review potential and actualevents and to make and implement recommenda-tions on mechanisms to improve patient safety.
19. Treatment team qualifications must be consistentand recognized nationally. Individuals involved inthe use of ionizing radiation for radiation therapyshould demonstrate their competence through na-tionally recognized qualifications to ensure thatproper education, clinical experience, and certifica-tion have been achieved.
20. The FDA review process should be improved.Safety test data should be uniformly reported inthe 510(k) process and the test results should bemade available to users in a transparent manner.Robust safety checks should be well documentedand demonstrated.
Conclusions
There were 3 general conclusions that evolved from themeeting. The first conclusion was that policies and

Improving patient safety 21Practical Radiation Oncology: January-March 2011
procedures to improve patient safety are successful only ifsenior management emphasizes their importance. At theinstitutional level, safety must be supported and encour-aged by the institution's board of directors and seniormanagement. At the level of individual services, such asradiation oncology, the physician director, departmentaladministrator, chief physicist, and chief therapist mustemphasize the importance of patient safety.
The second conclusion was that patient safety iseveryone's responsibility. This statement is more than aslogan, it is a commitment that should be inculcated intoevery employee in the institution and radiation oncologyservice. However, it should go further because acommitment to safety also involves persons outside theinstitution. In particular, representatives of equipmentvendors and members of regulatory agencies must bewilling to work with the radiation therapy team to improvethe safety of patients.
The third conclusion was that everyone in the radiationoncology service and beyond should work together toensure the safety of patients, and each person should berespected, supported, and appreciated for his or hercommitment to safety. It is only through valuing theopinions of others and treating all persons with courtesyand respect that a radiation oncology service can achieve
the goal of providing the greatest possible level ofeffectiveness and safety for patients.
References
1. Brennan TA, Leape LL, Laird NM, et al. Incidence of adverse eventsand negligence in hospitalized patients: results of the Harvard MedicalPractice Study I. N Engl J Med. 1991;324:370-376.
2. Leape LL, Brennan TA, Laird NM, et al. The nature of adverse eventsin hospitalized patients: Results of the Harvard Medical Practice StudyII. N Engl J Med. 1991;324:377-384.
3. National Patient Safety Foundation homepage. Available at: http://www.npsf.org. Accessed October 16, 2010.
4. Kohn LT, Corrigan JM, Donaldson MS, eds. To Err Is Human:Building a Safer Health System, Committee on Quality of Health Carein America. Washington, D.C.: Institute of Medicine NationalAcademy Press; 2000.
5. Hendee WR. Safety and accountability in health care from past topresent. Int J Radiat Oncol Biol Phys. 2008;71F:S157-S161.
6. International Committee on Radiological Protection, Publication 112.Preventing accidental exposures from new external beam radiationtherapy technologies. August 2009.
7. Bogdanich W. Radiation offers new cures and new ways to do harm.N Y Times. January 23, 2010.
8. Pawlicki T, Dunscombe P, Mund AJ, Scalliet P, eds. Quality andSafety in Radiotherapy. New York: Taylor & Francis; 2010.
9. Gawande A. The Checklist Manifesto: How to Get Things Right. NewYork: Metropolitan Books; 2009.