Embed Size (px)
Citation preview
CANADIAN JOURNAL OF DIABETES. 2010;34(3):218-226.
218 | CANADIAN JOURNAL OF DIABETES
ABSTRACTOBJECTIvE: The purpose of this study was to examine dia-betes educators’ perceptions of (a) their abilities, attitudes and difficulties/challenges related to physical activity and exercise counselling; and (b) their patients’ abilities and attitudes related to performing physical activity and exercise in managing their diabetes.
METhOD: Using a cross-sectional, observational design, diabetes educators (N=119) recruited from 3 provinces completed survey measures of counselling, referral and other efficacies; attitudes; perceived difficulty; barriers; and training practices related to physical activity and exercise.
RESULTS: Analyses revealed that diabetes educators lacked confidence in their own ability to counsel patients about, prescribe and make referrals for physical activity and exercise; they also lacked confidence in the ability of their patients to perform physical activity and exercise. While dia-betes educators had positive attitudes about physical activity and exercise, they perceived their typical patient’s attitudes to be much less positive. Diabetes educators perceived that including more in-depth physical activity and exercise coun-selling in their practice would be only somewhat difficult, but they indicated that they experienced multiple barriers in this area. Diabetes educators’ perceptions were also shown to be associated with their counselling practices related to physical activity and exercise.
CONCLUSION: These findings provide novel insight into dia-betes educators’ perceptions of their own abilities, as well as those of their patients, and further underscore the need to provide diabetes educators with greater training in physical activity and exercise counselling.
KEywORDS: counselling, diabetes, education, efficacy, exer-cise, patients, physical activity
RÉSUMÉOBJECTIF : Cette étude avait pour objet d’examiner comment les éducatrices/éducateurs spécialisés en diabète percevaient (a) leurs capacités et attitudes ainsi que les difficultés liées au counselling sur l’activité physique et l’exercice; et (b) les capacités des patients de faire de l’activité physique et de l’exercice pour gérer le diabète et les attitudes des patients en ce qui a trait à l’activité physique et à l’exercice.
MÉThODE : Une enquête transversale observationnelle a été menée auprès d’éducatrices/éducateurs spécialisés en diabète (N = 119) de trois provinces, qui ont rempli un questionnaire sur le counselling, l’orientation des patients et autres efficacités, les attitudes, la difficulté perçue, les obstacles et les pratiques de formation ayant trait à l’activité physique et à l’exercice.
RÉSULTATS : Les analyses ont révélé que les éducatrices/éducateurs spécialisés en diabète manquaient de con-fiance dans leurs capacités de counselling, de prescription et d’orientation des patients pour ce qui est de l’activité physique et de l’exercice, ainsi que dans les capacités de leurs patients de faire de l’activité physique et de l’exercice. Les éducatrices/éducateurs spécialisés en diabète avaient des attitudes favorables en ce qui concerne l’activité physique et l’exercice, mais ils considéraient que le patient typique avait des attitudes beaucoup moins favorables. Les éduca-trices/éducateurs spécialisés en diabète considéraient qu’il ne serait pas très difficile d’intensifier le counselling sur l’activité physique et l’exercice, mais ont dit faire face à de nombreux obstacles à ce chapitre. L’ enquête a aussi révélé
Carrie J. Dillman¹ BKinH, Christopher A. Shields1,2 PhD, Jonathon R. Fowles1,2 PhD, Arlene Perry¹ BSc, René J.L. Murphy1,2 PhD, Peggy Dunbar3 MEd
1School of Recreation Management & Kinesiology, Acadia University, Wolfville, Nova Scotia, Canada2Centre of Lifestyle Studies, Acadia University, Wolfville, Nova Scotia, Canada3Diabetes Care Program of Nova Scotia, Halifax, Nova Scotia, Canada
Address for correspondence: Christopher A. Shields, Associate Professor, School of Recreation Management and Kinesiology
Acadia University, Wolfville, Nova Scotia, Canada B4P 2R6, E-mail: [email protected]
ORIgINAL RESEARCh
Including Physical Activity and Exercise in Diabetes Management: Diabetes Educators’ Perceptions of Their Own Abilities and the Abilities of Their Patients

CANADIAN JOURNAL OF DIABETES. 2010;34(3):218-226.
DIABETES EDUCATORS’ PERCEPTIONS OF PHYSICAL ACTIVITY COUNSELLING | 219
que les perceptions des éducatrices/éducateurs spécialisés en diabète étaient associées à leurs pratiques en matière de counselling sur l’activité physique et l’exercice.
CONCLUSION : Ces résultats jettent un nouvel éclairage sur les perceptions qu’ont les éducatrices/éducateurs spécialisés en diabète de leurs capacités et de celles de leurs patients, et font encore une fois ressortir que les éducatrices/éducateurs spécialisés en diabète doivent recevoir davantage de forma-tion sur le counselling sur l’activité physique et l’exercice.
MOTS CLÉS : counselling, diabète, éducation, efficacité, exer-cice, patients, activité physique
INTRODUCTION Physical activity and exercise are acknowledged as one of the primary modifiable risk factors in the prevention and treatment of type 2 diabetes (1-3) and are key components of diabetes self-management (4-6). Specifically, regular physical activity has been shown to prevent the develop-ment of complications resulting from diabetes (1,6,7), decrease the need for blood glucose-lowering medication (8) and reduce premature, all-cause mortality in individu-als with diabetes (9,10). Despite these benefits and a recent emphasis on physical activity counselling in quality diabetes management (11), it is estimated that between 60 and 76% of Canadians with diabetes are not active enough to achieve health benefits (12-15). Individuals with diabetes have traditionally reported receiving less support, education and encouragement for physical activity than for other lifestyle management issues (16), and progress in this area is limited (11). The promotion of physical activity for people with diabetes continues to be generally insufficient (17).
The role of diabetes educatorsDiabetes educators are often viewed as the primary source of information and assistance for people living with diabe-tes and, as such, are in a position to effectively encourage physical activity and exercise (18). The most recent clinical practice guidelines by the Canadian Diabetes Association (CDA) highlight the effectiveness of structured physical activity counselling by healthcare professionals in increas-ing physical activity levels and improving diabetes-specific outcomes (19). The guidelines provide general recommen-dations about the amount of exercise to be encouraged (e.g., 150 min of moderate-intensity aerobic exercise per week), but they lack specific details about prescribing intensity, modes of exercise (particularly resistance exercise) and tai-loring programs to account for individuals with complica-tions (19,20). As a result, although diabetes educators are attempting to address physical activity with their patients, the majority of diabetes educators do not feel confident
in doing so. Specifically, diabetes educators feel that they lack sufficient training, knowledge, skills and experience to effectively counsel patients about physical activity and exer-cise (11,21) and have reported anxiety about encouraging physical activity due to fears about increasing patient risk (11,22). Consequently, there is a lack of standardization in physical activity and exercise counselling delivery (23), with varied and inconsistent procedures for individualizing physical activity and exercise promotion (11,23).
It is important to recognize that diabetes educators’ per-ceptions regarding physical activity and exercise counselling may have behavioural implications in diabetes practice. Specifically, Social Cognitive Theory (24) highlights percep-tions of confidence in one’s own abilities (known as self-efficacy) as a key determinant of personal behaviour (e.g. diabetes educators’ physical activity and exercise counselling practices). The health promotion literature appears to bear this out, showing that, in both general healthcare (25) and diabetes contexts (26), low levels of confidence in counselling to patients around lifestyle modification limits the provision of guidance in these areas. While diabetes educators’ lack of confidence with respect to physical activity and exercise counselling has been previously identified in small samples (11,24), the previous work does not recognize the social situ-ation in which much of diabetes self-management education occurs. This is not surprising given the theoretical focus and research emphasis on the role of self-efficacy (24).
However, Lent and Lopez (27) have offered some direc-tion in this regard, suggesting that in instructor–patient relationships, an understanding of an individual’s beliefs about both parties in the relationship may be essential (27). While they recognize the importance of self-efficacy as a determinant of behaviour, they also underscore the impor-tance of an individual’s beliefs about another’s capabilities, known as other efficacy. These other efficacy perceptions are theorized to affect the effort an individual expends in joint tasks with another person, the provision of assistance and satisfaction with the relationship (27). This may be particu-larly important in the context of diabetes management, as diabetes educators’ perceived confidence in their patients’ abilities to use physical activity and exercise to manage their diabetes may affect their interactions with patients and the feedback and support they provide. Nevertheless, despite the theoretical importance of these perceptions and pos-sible implications for counselling practices, there have been no examinations of diabetes educators’ confidence in their patients’ abilities in the diabetes/exercise literature.
Additionally, while providing information and guid-ance on physical activity and exercise directly to patients is the most studied aspect of physical activity promotion by diabetes educators, providing effective physical activity and exercise counselling for those with diabetes can require
220 | CANADIAN JOURNAL OF DIABETES
resources and expertise beyond those typically available to diabetes educators. For example, prior to engaging in regular exercise, it may be important for patients with signs of coronary artery disease or musculoskeletal problems to be referred to a specialist. As a result, recognizing when to make appropriate referrals to other healthcare profession-als (e.g. cardiologists, internists, physiotherapists, qualified exercise professionals) for further screening or advice is a key yet understudied aspect of the counselling process when working with people with diabetes.
Given the fundamental role of physical activity and exer-cise in the management of diabetes, the important position diabetes educators hold in assisting patients with managing their condition, and the potential impact of diabetes educa-tors’ perceptions on their counselling behaviour there is a need to examine diabetes educators’ beliefs about their patients’ abilities and their own abilities in a large sample. This study had 3 purposes. The first was to examine diabetes educators’ perceptions of their abilities, attitudes and difficulties related to physical activity and exercise counselling. The second was to examine diabetes educators’ perceptions of their patients’ abilities and attitudes related to physical activity and exercise
in managing their diabetes. The third was to examine the self-reported barriers diabetes educators face with respect to physical activity and exercise counselling. Also of interest was the training and experience diabetes educators have with regard to physical activity and exercise counselling.
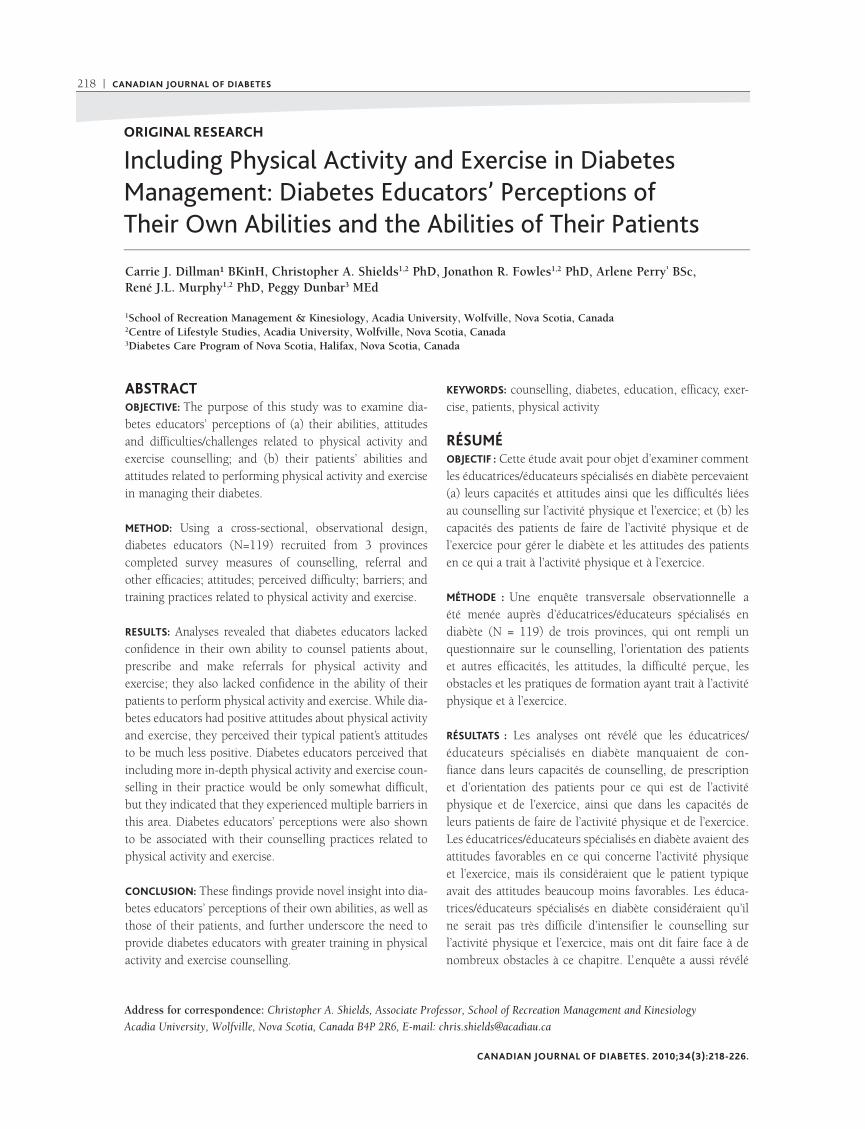
METhODSDesign and participantsThis study used a cross-sectional, survey-based design. Diabetes educators (N=119) were recruited across 3 Atlantic provinces: Nova Scotia (n=69), New Brunswick (n=34) and Newfoundland (n=16). The mean age of the sample was 44 years, almost all were female (97%) and most self-reported their ethnicity as Caucasian (90%). The majority of the sample (92%) held at least a bachelor’s degree, with the pri-mary educational backgrounds being in nutrition (59%) and nursing (16%). In terms of employment, 42% of diabetes educators reported having worked at a diabetes education centre for more than 10 years, while 15% had worked at a centre for less than 2 years. The majority of participants saw fewer than 10 patients per day (57%), with another 30% seeing 10 to 15 patients per day. In their practice, most participants (59%) reported that sessions with patients were typically between 20 and 40 minutes in length. Full partici-pant demographics are presented in Table 1.
MeasuresGiven that little to no research has examined many of the constructs of interest and that this represents the first such work in the context of diabetes education, all measures were developed by the researchers for use in the current study.
Counselling efficacyThis 13-item measure was used to assess participating diabe-tes educators’ confidence in their ability to perform specific aspects of physical activity and exercise counselling with their patients over the next month. For example, one item asks about diabetes educators’ confidence in “design[ing] a physical activity or exercise program that accommodates clients’ indi-vidual needs or limitations.” In line with recommendations regarding the measurement of efficacy-related constructs, all items were assessed using a 0% (not at all confident) to 100% (completely confident) scale (28). Items were averaged to pro-vide an overall indication of diabetes educators’ confidence to perform physical activity and exercise counselling. Cronbach’s alpha was calculated as a measure of internal consistency and was found to be acceptable (alpha=0.96) (29).
Referral efficacyThis efficacy measure assessed diabetes educators’ confi-dence in their ability to refer patients who required addition-al clearance or information prior to beginning an exercise
Table 1. Participant demographics (N=119)
Parameter % (n)
Educational backgroundGraduate schoolBachelor’sDiploma
8 (10)83 (98)
8 (10)
Diploma/degree*NutritionNursingHome economicsBScKinesiologyOther
59 (26)16 (7)14 (6)5 (2)5 (2)2 (1)
Time working at a DEC<2 years2–4 years4–6 years6–8 years8–10 years>10 years
15 (18)8 (9)
13 (15)13 (15)10 (12)41 (49)
Patients per day<55–1010–1515–20>20
14 (17)43 (51)29 (35)10 (12)3 (3)
Time spent with patients<10 min10–20 min20–30 min30–40 min40–50 min>50 min
1 (1)16 (19)24 (28)34 (41)
9 (11)16 (19)
DEC = diabetes education centre*N providing name of specific diploma/degree held = 44

CANADIAN JOURNAL OF DIABETES. 2010;34(3):218-226.
DIABETES EDUCATORS’ PERCEPTIONS OF PHYSICAL ACTIVITY COUNSELLING | 221
respect to physical activity and exercise. Specifically, single items were used to measure diabetes educators’ perceptions of (a) how important their patients felt physical activity and exercise was in diabetes management; (b) how receptive they felt their patients would be to an increased focus on physical activity in sessions on diabetes management; and (c) how knowledgeable diabetes educators felt their patients were in this area. All 3 items were assessed using a 1 (not at all) to 5 (extremely) scale.
BarriersA 3-pronged approach was used to assess the barriers dia-betes educators face when attempting to incorporate more physical activity and exercise counselling into their sessions. First, diabetes educators were asked to list up to 3 primary barriers they felt made incorporating more physical activity and exercise counselling more difficult. Open-ended items were used to allow diabetes educators to specify the par-ticular barriers and challenges they faced. Second, for each barrier listed, diabetes educators were asked to indicate the frequency with which they experienced the given barrier. Frequency was assessed on a 1 (rarely occurs) to 4 (constant barrier) scale. Finally, for each barrier listed, diabetes educa-tors were asked to indicate the impact the specific barrier had on incorporating more physical activity and exercise counselling into their practice. Impact was measured using a 1 (easily overcome) to 4 (completely prevents me) scale. For both frequency and impact, average scores were calculated separately for each component. This multi-step approach to assessing barriers is in line with previous recommendations concerning the evaluation of barriers in the physical activity and exercise literature (31).
Training and practicesParticipating diabetes educators were asked multiple ques-tions regarding their training and practices with respect to physical activity and exercise counselling. Specifically, single items providing multiple response options were used to assess the amount of training diabetes educators had received about physical activity and exercise counselling; the frequency and amount of time spent on physical activity and exercise counselling in their current practice; and who they felt was best equipped to provide physical activity and exercise information to those with diabetes.
ProcedurePrior to recruitment, the study received institutional ethi-cal approval. Diabetes educators were recruited across 3 Atlantic provinces in 2 ways: (1) through provincial annual meetings of diabetes educators and (2) through CDA Diabetes Educator Section chapter chairs. At annual meetings, a researcher trained in the study protocol used a
program. Three items, each scaled on a 0% (not at all con-fident) to 100% (completely confident) scale, were used. A sample item is as follows: “How confident are you in your ability to make appropriate referrals to physical therapists for those clients who exhibit musculoskeletal or orthopedic problems and may require further examination prior to par-ticipation in regular physical activity or exercise?” Items were averaged to provide an overall referral efficacy score for each diabetes educator (alpha=0.87).
AttitudesDiabetes educators’ attitudes about physical activity and exercise counselling as a part of diabetes management were assessed across 3 separate items, each using a 1 (not at all) to 5 (extremely) scale. The first item concerned the perceived importance of physical activity and exercise in diabetes man-agement. The second item asked participants how receptive they would be to an increased focus on physical activity and exercise counselling in the management of diabetes. The third item assessed how knowledgeable participants felt about physical activity and exercise. The use of single-item mea-sures is not uncommon in work examining exercise-related social cognitions in those with chronic conditions (30).
Perceived difficultyThis 4-item questionnaire assessed diabetes educators’ percep-tions of how difficult it would be to incorporate recommen-dations for physical activity and exercise into sessions with their patients. Each item assessed a more in-depth approach to delivering physical activity and exercise counselling as part of the diabetes management “message.” Specifically, items assessed diabetes educators’ perceived difficulty with including information, counselling, instruction or all 3 into their sessions with patients. Items were assessed on a 1 (not at all difficult) to 5 (very difficult) scale and were averaged to provide an overall perceived difficulty score out of 5 (alpha=0.89).
Confidence in patientThis other measure of efficacy concerned diabetes educators’ confidence in a typical patient’s ability to perform physical activity and exercise behaviours over the next month. Other efficacy was assessed across 6 items, including confidence in a typical patient’s ability to “perform exercise and physically active behaviours appropriate for their fitness level and con-dition” and to “set and work toward realistic and beneficial goals.” Items were assessed using a 0% (not at all confident) to 100% (completely confident) scale and averaged to pro-vide overall other efficacy scores (alpha=0.96).
Perceived patient attitudesThree separate items were used to assess participating dia-betes educators’ perceptions of their patients’ attitudes with

222 | CANADIAN JOURNAL OF DIABETES
ability to manage physical activity and exercise. Further, diabetes educators perceived patients’ attitudes to be less positive than their own on all 3 attitudinal items (i.e. impor-tance, receptiveness, knowledge) (Table 2).
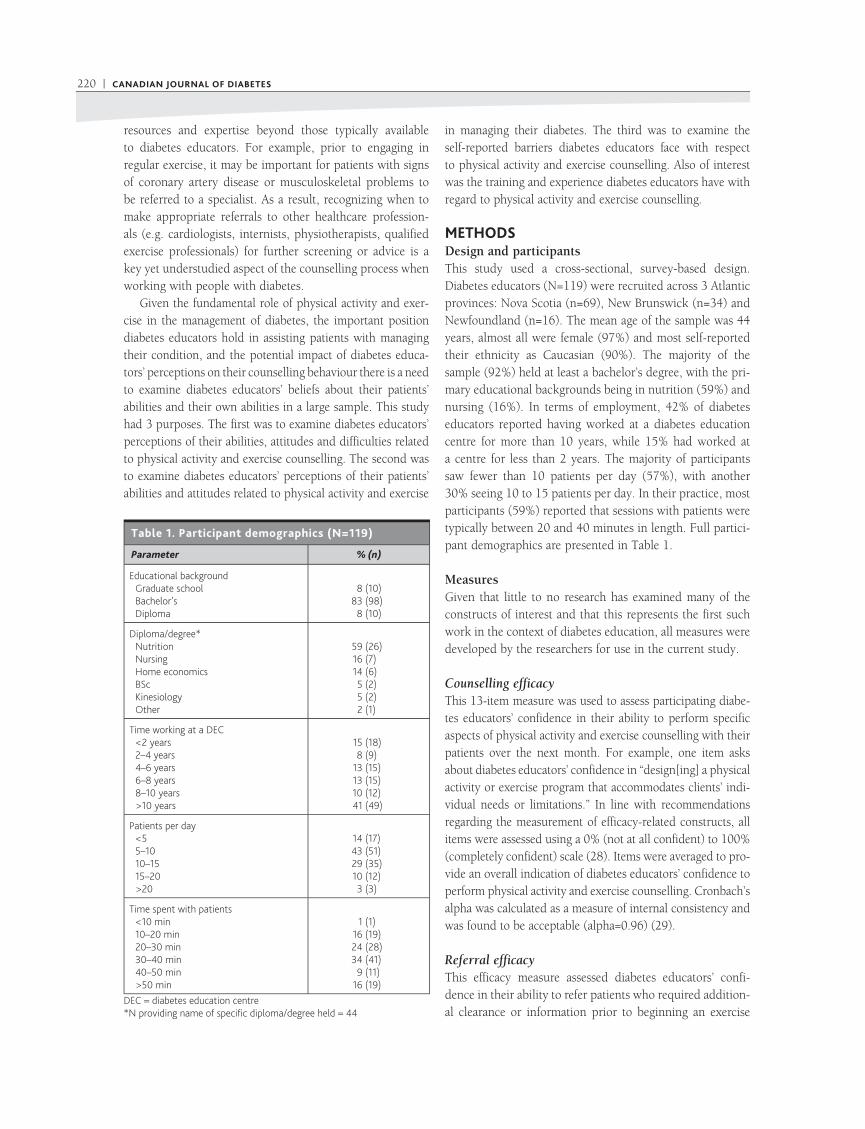
BarriersOn average, diabetes educators provided more than 2 responses to the open-ended questions concerning barriers to incorporating physical activity and exercise counselling into their practice. In order to assess distinct barriers report-ed, 2 separate researchers grouped barriers and synonyms or phrases that reflected a given barrier (e.g. lack of time, time, appointments too short). These statements were then counted to quantify how many times a given barrier was mentioned. This resulted in 6 distinct categories of barriers: lack of time (e.g. not enough time in sessions to cover physical activity and exercise), lack of interest on the part of the patient (e.g. patient not interested or resistant), lack of resources (e.g. lack of access to exercise professionals), diabetes educators’ lack of ability/confidence/knowledge (e.g. lack of knowledge/training), patient comorbidities (e.g. physical conditions that may limit exercise) and lack of access to facilities (e.g. lack of physical activity space and facilities in rural areas). Lack of time was the barrier most often noted, with 65% of diabetes educators identifying it as a challenge to incorporating more physical activity and exercise counselling into their practice. On average, for those who reported barriers, these were seen as occurring relatively frequently and were reported to have a moderate impact on counselling practices. See Table 3 for full results of the analysis of reported barriers.
Training and practiceFrequency analysis of the degree to which diabetes educa-tors incorporated physical activity and exercise counselling into their practice revealed that while 62% of diabetes educators reported addressing physical activity and exercise in more than half of their sessions, 83% of participants indicated that they spent less than 25% of their time dis-cussing this topic (Table 4). In terms of training in physical activity and exercise counselling, 40% of diabetes educators reported having received no formal training with respect to physical activity and exercise, and an additional 40% had received only 1 form of training (e.g., workshops, as a part of degree, conference presentations, certifications). The remaining 20% of participants reported having received more than 2 forms of training specific to physical activity and exercise counselling.
Differences in social cognitions across physical activity and exercise counsellingIn order to explore whether diabetes educators’ perceptions of themselves and their patients differed depending on the
standardized script to solicit participation. Diabetes educa-tors recruited through a chapter chair were sent a standard-ized letter via e-mail to solicit participation. At the time of recruitment, all potential participants were provided with an information letter outlining the purpose and procedures of the study, and all participants provided informed con-sent. Diabetes educators recruited at annual meetings were given the option of completing the questionnaires onsite and returning them to the researcher in a sealed envelope or by mail using a self-addressed stamped envelope. Diabetes educators recruited through their chapter chair completed questionnaires online via a secure website designed specifi-cally for this purpose. In addition to the main variables of interest, demographic variables and variables concerning employment history were also collected.
RESULTSSocial cognitions Baseline descriptive analyses (Table 2) revealed that dia-betes educators lacked confidence in both their ability to prescribe physical activity and exercise and their ability to make appropriate physical activity and exercise-related referrals, with both averages being below the midpoint of the scale (i.e. 50%). Diabetes educators reported positive attitudes about physical activity and exercise, viewing it as an important aspect of diabetes management and they were highly receptive to including more counselling in their sessions. However, they indicated that their knowledge of physical activity and exercise was moderate. In terms of per-ceived difficulty, diabetes educators reported that including more in-depth physical activity and exercise counselling would be only somewhat difficult.
With respect to perceptions of their patients’ abilities, diabetes educators reported low confidence in their patients’
Table 2. Mean social cognitions (N=119)
Variables (scale anchors) Mean±SD
Diabetes educator perceptions of themselves
Counselling efficacy (0–100) 46.5±21.6
Referral efficacy (0–100) 48.2±28.5
Attitudes: perceived importance (1–5) 4.9±0.3
Attitudes: how receptive (1–5) 4.5±0.6
Attitudes: knowledge (1–5) 3.1±0.9
Perceived difficulty (1–5) 2.7±0.9
Diabetes educator perceptions of their patients
Confidence in patient (0–100) 37.6±17.8
Attitudes: perceived importance (1–5) 2.8±0.7
Attitudes: how receptive (1–5) 3.2±0.7
Attitudes: knowledge (1–5) 2.5±0.7
CANADIAN JOURNAL OF DIABETES. 2010;34(3):218-226.
DIABETES EDUCATORS’ PERCEPTIONS OF PHYSICAL ACTIVITY COUNSELLING | 223
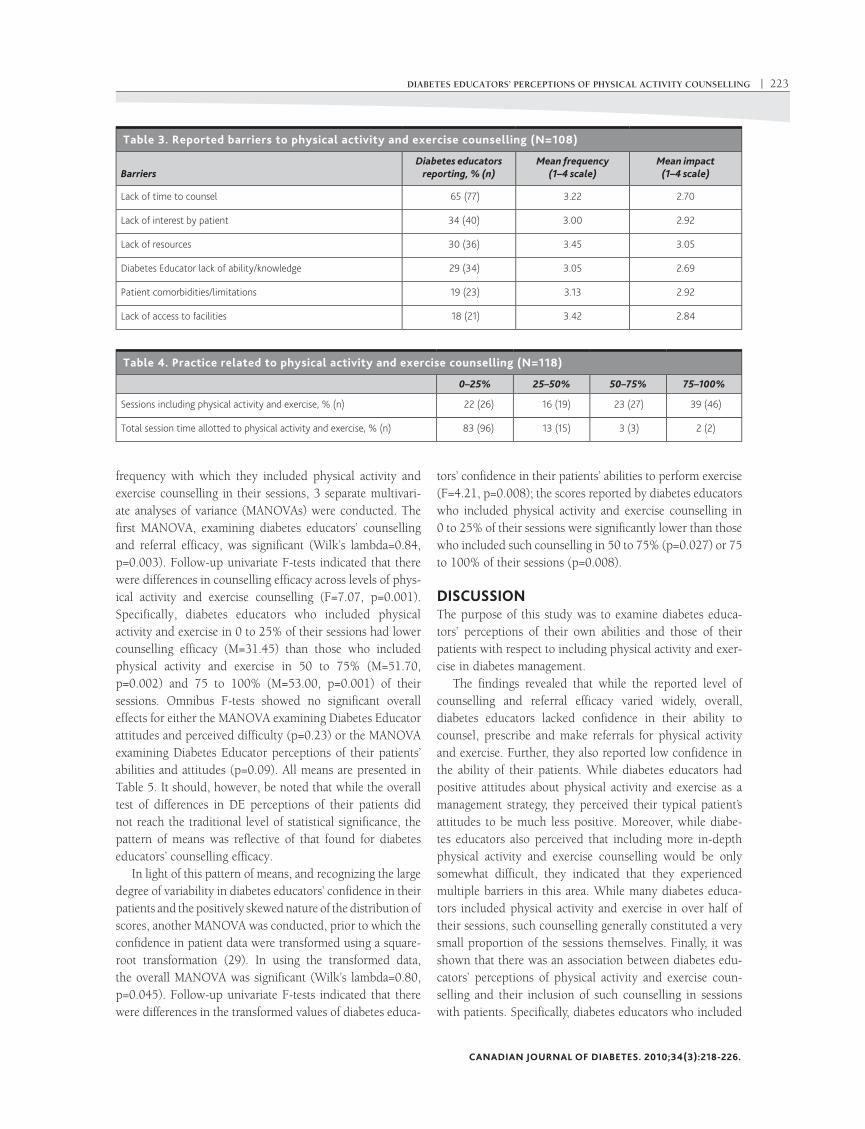
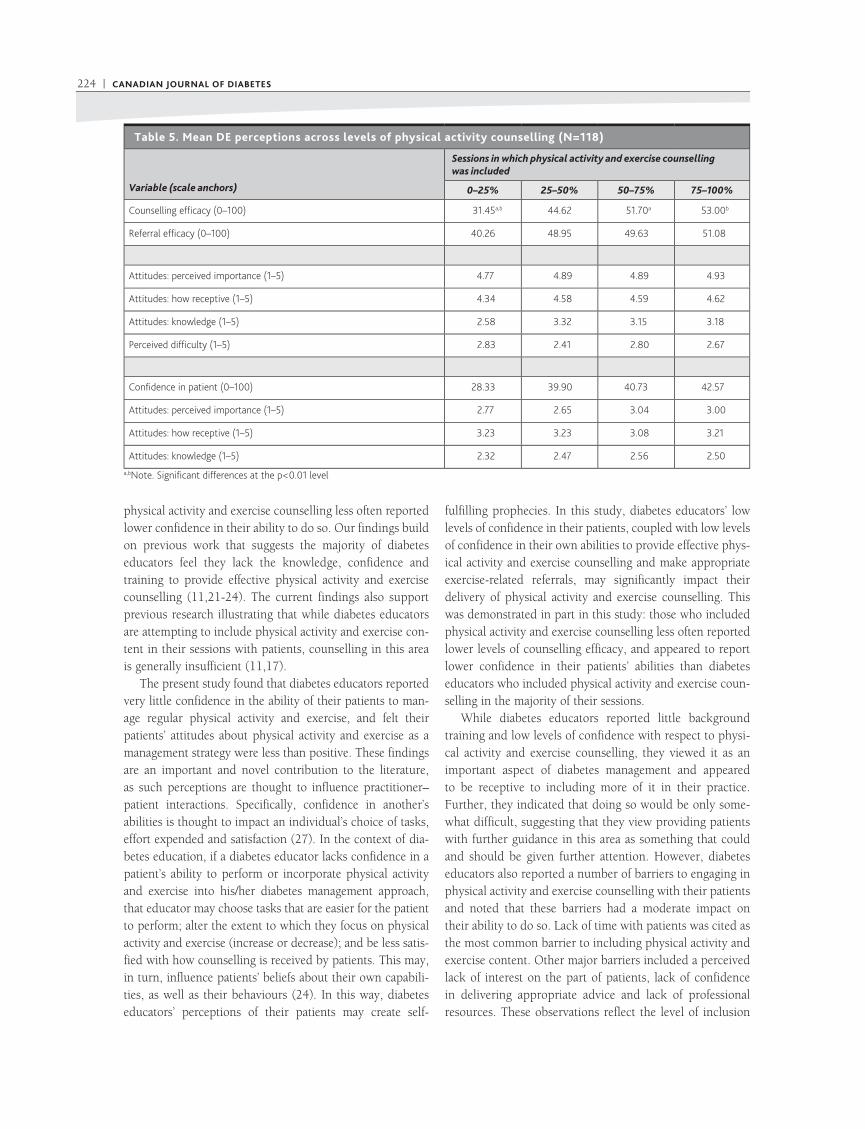
frequency with which they included physical activity and exercise counselling in their sessions, 3 separate multivari-ate analyses of variance (MANOVAs) were conducted. The first MANOVA, examining diabetes educators’ counselling and referral efficacy, was significant (Wilk’s lambda=0.84, p=0.003). Follow-up univariate F-tests indicated that there were differences in counselling efficacy across levels of phys-ical activity and exercise counselling (F=7.07, p=0.001). Specifically, diabetes educators who included physical activity and exercise in 0 to 25% of their sessions had lower counselling efficacy (M=31.45) than those who included physical activity and exercise in 50 to 75% (M=51.70, p=0.002) and 75 to 100% (M=53.00, p=0.001) of their sessions. Omnibus F-tests showed no significant overall effects for either the MANOVA examining Diabetes Educator attitudes and perceived difficulty (p=0.23) or the MANOVA examining Diabetes Educator perceptions of their patients’ abilities and attitudes (p=0.09). All means are presented in Table 5. It should, however, be noted that while the overall test of differences in DE perceptions of their patients did not reach the traditional level of statistical significance, the pattern of means was reflective of that found for diabetes educators’ counselling efficacy.
In light of this pattern of means, and recognizing the large degree of variability in diabetes educators’ confidence in their patients and the positively skewed nature of the distribution of scores, another MANOVA was conducted, prior to which the confidence in patient data were transformed using a square-root transformation (29). In using the transformed data, the overall MANOVA was significant (Wilk’s lambda=0.80, p=0.045). Follow-up univariate F-tests indicated that there were differences in the transformed values of diabetes educa-
tors’ confidence in their patients’ abilities to perform exercise (F=4.21, p=0.008); the scores reported by diabetes educators who included physical activity and exercise counselling in 0 to 25% of their sessions were significantly lower than those who included such counselling in 50 to 75% (p=0.027) or 75 to 100% of their sessions (p=0.008).
DISCUSSIONThe purpose of this study was to examine diabetes educa-tors’ perceptions of their own abilities and those of their patients with respect to including physical activity and exer-cise in diabetes management.
The findings revealed that while the reported level of counselling and referral efficacy varied widely, overall, diabetes educators lacked confidence in their ability to counsel, prescribe and make referrals for physical activity and exercise. Further, they also reported low confidence in the ability of their patients. While diabetes educators had positive attitudes about physical activity and exercise as a management strategy, they perceived their typical patient’s attitudes to be much less positive. Moreover, while diabe-tes educators also perceived that including more in-depth physical activity and exercise counselling would be only somewhat difficult, they indicated that they experienced multiple barriers in this area. While many diabetes educa-tors included physical activity and exercise in over half of their sessions, such counselling generally constituted a very small proportion of the sessions themselves. Finally, it was shown that there was an association between diabetes edu-cators’ perceptions of physical activity and exercise coun-selling and their inclusion of such counselling in sessions with patients. Specifically, diabetes educators who included
Table 3. Reported barriers to physical activity and exercise counselling (N=108)
Barriers
Diabetes educators reporting, % (n)
Mean frequency (1–4 scale)
Mean impact (1–4 scale)
Lack of time to counsel 65 (77) 3.22 2.70
Lack of interest by patient 34 (40) 3.00 2.92
Lack of resources 30 (36) 3.45 3.05
Diabetes Educator lack of ability/knowledge 29 (34) 3.05 2.69
Patient comorbidities/limitations 19 (23) 3.13 2.92
Lack of access to facilities 18 (21) 3.42 2.84
Table 4. Practice related to physical activity and exercise counselling (N=118)
0–25% 25–50% 50–75% 75–100%
Sessions including physical activity and exercise, % (n) 22 (26) 16 (19) 23 (27) 39 (46)
Total session time allotted to physical activity and exercise, % (n) 83 (96) 13 (15) 3 (3) 2 (2)
224 | CANADIAN JOURNAL OF DIABETES
physical activity and exercise counselling less often reported lower confidence in their ability to do so. Our findings build on previous work that suggests the majority of diabetes educators feel they lack the knowledge, confidence and training to provide effective physical activity and exercise counselling (11,21-24). The current findings also support previous research illustrating that while diabetes educators are attempting to include physical activity and exercise con-tent in their sessions with patients, counselling in this area is generally insufficient (11,17).
The present study found that diabetes educators reported very little confidence in the ability of their patients to man-age regular physical activity and exercise, and felt their patients’ attitudes about physical activity and exercise as a management strategy were less than positive. These findings are an important and novel contribution to the literature, as such perceptions are thought to influence practitioner–patient interactions. Specifically, confidence in another’s abilities is thought to impact an individual’s choice of tasks, effort expended and satisfaction (27). In the context of dia-betes education, if a diabetes educator lacks confidence in a patient’s ability to perform or incorporate physical activity and exercise into his/her diabetes management approach, that educator may choose tasks that are easier for the patient to perform; alter the extent to which they focus on physical activity and exercise (increase or decrease); and be less satis-fied with how counselling is received by patients. This may, in turn, influence patients’ beliefs about their own capabili-ties, as well as their behaviours (24). In this way, diabetes educators’ perceptions of their patients may create self-
fulfilling prophecies. In this study, diabetes educators’ low levels of confidence in their patients, coupled with low levels of confidence in their own abilities to provide effective phys-ical activity and exercise counselling and make appropriate exercise-related referrals, may significantly impact their delivery of physical activity and exercise counselling. This was demonstrated in part in this study: those who included physical activity and exercise counselling less often reported lower levels of counselling efficacy, and appeared to report lower confidence in their patients’ abilities than diabetes educators who included physical activity and exercise coun-selling in the majority of their sessions.
While diabetes educators reported little background training and low levels of confidence with respect to physi-cal activity and exercise counselling, they viewed it as an important aspect of diabetes management and appeared to be receptive to including more of it in their practice. Further, they indicated that doing so would be only some-what difficult, suggesting that they view providing patients with further guidance in this area as something that could and should be given further attention. However, diabetes educators also reported a number of barriers to engaging in physical activity and exercise counselling with their patients and noted that these barriers had a moderate impact on their ability to do so. Lack of time with patients was cited as the most common barrier to including physical activity and exercise content. Other major barriers included a perceived lack of interest on the part of patients, lack of confidence in delivering appropriate advice and lack of professional resources. These observations reflect the level of inclusion
Table 5. Mean DE perceptions across levels of physical activity counselling (N=118)
Variable (scale anchors)
Sessions in which physical activity and exercise counselling was included
0–25% 25–50% 50–75% 75–100%
Counselling efficacy (0–100) 31.45a,b 44.62 51.70a 53.00b
Referral efficacy (0–100) 40.26 48.95 49.63 51.08
Attitudes: perceived importance (1–5) 4.77 4.89 4.89 4.93
Attitudes: how receptive (1–5) 4.34 4.58 4.59 4.62
Attitudes: knowledge (1–5) 2.58 3.32 3.15 3.18
Perceived difficulty (1–5) 2.83 2.41 2.80 2.67
Confidence in patient (0–100) 28.33 39.90 40.73 42.57
Attitudes: perceived importance (1–5) 2.77 2.65 3.04 3.00
Attitudes: how receptive (1–5) 3.23 3.23 3.08 3.21
Attitudes: knowledge (1–5) 2.32 2.47 2.56 2.50a,bNote. Significant differences at the p<0.01 level

CANADIAN JOURNAL OF DIABETES. 2010;34(3):218-226.
DIABETES EDUCATORS’ PERCEPTIONS OF PHYSICAL ACTIVITY COUNSELLING | 225
ConclusionsPhysical activity and exercise are important means of pre-venting and managing diabetes, and diabetes educators are in a key position to promote and encourage these behav-iours. However, lack of confidence, multiple barriers and insufficient training in delivering physical activity and exer-cise counselling may limit their ability to do so. This study is the first to take into account diabetes educators’ perceptions of both their own ability and their patients’ ability, and it further supports the identified need to provide theory-based training on physical activity and exercise specific to the con-cerns and barriers that diabetes educators face. Recognizing the importance of the referral process in counselling those with diabetes (and other related comorbidities) is also an essential yet understudied area in the exercise/diabetes lit-erature, and we observed that more support is also required in this area.
This study was conducted on a large scale in Atlantic Canada, a region where the responsibility of diabetes edu-cators to provide all aspects of quality diabetes care may be particularly important, given that a large proportion of residents live in rural areas (34), where access to other healthcare resources may be limited. This study represents a step forward in providing the evidence-based framework for systematic, structured and uniform physical activity and exercise counselling in diabetes care (11). This work also identifies a need for longitudinal, intervention-based research to examine the impact of training aimed at improv-ing diabetes educators’ abilities in physical activity and exercise counselling, and whether any changes in their per-ceptions impact patients’ perceptions and behaviour.
ACKNOwLEDgMENTSFunding provided by the Lawson Foundation.
REFERENCES1. Bassuk SS, Manson JE. Epidemiological evidence for the role of physi-
cal activity in reducing risk of type 2 diabetes and cardiovascular dis-ease. J Applied Physiol. 2005;99:1193-1204.
2. Grace SL, Barry-Bianchi S, Stewart DE, et al. Physical activity behavior, motivational readiness and self-efficacy among Ontarians with cardio-vascular disease and diabetes. J Behav Med. 2007;30:21-29.
3. Lindstrom J, Ilanne-Parikka P, Peltonen M, et al. Sustained reduction in the incidence of type 2 diabetes by lifestyle intervention: follow-up of the Finnish Diabetes Prevention Study. Lancet. 2006;368:1673-1679.
4. American Diabetes Association. Standards of medical care in diabe-tes—2007. Diabetes Care. 2007;30(suppl 1):S4-S41.
5. Donahue KE, Mielenz TJ, Sloane PD, et al. Identifying supports and barriers to physical activity in patients at risk for diabetes. Prev Chronic Dis. 2006;3:A119.
6. Sigal RJ, Kenny GP, Wasserman DH, et al. Physical activity/exercise and type 2 diabetes: a consensus statement from the American Diabetes Association. Diabetes Care. 2006;29:1433-1438.
7. Diabetes in Canada: National Statistics and Opportunities for Improved Surveillance, Prevention and Control. Ottawa, ON: Health Canada; 1999.
8. Balducci S, Leonetti F, Di Mario U, et al. Is a long-term aerobic plus resistance training program feasible for and effective on metabolic
of physical activity and exercise counselling reported in the patient sessions in this study. Specifically, this study found that while the majority of diabetes educators included physical activity and exercise content in most of their ses-sions, such counselling was a relatively minor component.
Given the importance of physical activity and exercise in the management of diabetes (19), solutions need to be explored to allow for additional guidance in physical activ-ity and exercise during education sessions. Either more time needs to be allocated in practice to physical activity counsel-ling or resources need to be provided to help make physical activity and exercise counselling more achievable. While physical activity and exercise are recognized as high-priority components of quality diabetes care, it appears that this understanding does not entirely translate into practice. This may be due to the fact that most diabetes educators have less training in the area of physical activity and exercise, potentially resulting in a tendency to provide counselling priority to the areas that are more in line with their educa-tion and training (e.g. nutrition). For diabetes educators, greater support for physical activity and exercise counselling could come in the form of training workshops to help build knowledge and confidence, or in the form of educational tools to help streamline the counselling process.
Taken together, our results further highlight the need to provide diabetes educators with additional training in: (a) providing effective physical activity and exercise counsel-ling, including conveying a sense that the patient has the ability to be successful; (b) making appropriate exercise-related referrals; and (c) more effectively incorporating physical activity and exercise counselling into their sessions, given the time constraints in which they work. Indeed, it has been shown that training increases both knowledge and confidence (32,33), and that diabetes educators who receive training in exercise counselling are more comfortable with distributing physical activity and exercise advice (21).
LimitationsThis study provides important new insights into diabetes educators’ perceptions of and experience with physical activ-ity and exercise counselling; however, it is not without its limitations. While diabetes educators’ perceptions of their own abilities were shown to be associated with the delivery of physical activity and exercise counselling, the cross-sectional design of this study did not allow for causal inferences with respect to this relationship. Further, while diabetes educators’ inclusion of physical activity and exercise counselling would be expected to be related to patient physical activity, no direct patient outcomes were assessed. There is a clear need for longitudinal, intervention-based research to examine the impact of training aimed at improving diabetes educators’ abilities in physical activity and exercise counselling.

226 | CANADIAN JOURNAL OF DIABETES
profiles in type 2 diabetic patients? Diabetes Care. 2004;27:841-842.9. Albright A, Franz M, Hornsby G, et al. American College of Sports
Medicine position stand. Exercise and type 2 diabetes. Med Sci Sports Exerc. 2000;32:1345-1360.
10. LaMonte MJ, Blair SM, Church TS. Physical activity and diabetes pre-vention. J Appl Physiol. 2005;99:1205-1213.
11. Gornall A, Lévesque L, Sigal RJ. A pilot study of physical activity educa-tion delivery in diabetes education centres in Ontario. Can J Diabetes. 2008;32:123-130.
12. Responding to the Challenge of Diabetes in Canada: First Report of the National Diabetes Surveillance System (NDSS). Ottawa, ON: Health Canada; 2003.
13. Dubbert PM. Physical activity and exercise: recent advances and current challenges. J Consult Clin Psychol. 2002;70:526-536.
14. McManus RM, Stitt LW, Bargh GJM. Population survey of diabe-tes knowledge and protective behaviours. Can J Diabetes. 2006;30: 256-263.
15. Plotnikoff RC. Physical activity in the management of diabetes: popula-tion-based perspectives and strategies. Can J Diabetes. 2006;30:52-62.
16. Wilson W, Ary DV, Biglan A, et al. Psychosocial predictors of self-care behaviors (compliance) and glycemic control in non-insulin-dependent diabetes mellitus. Diabetes Care. 1986;9:614-622.
17. Kirk AF, Barnett J, Mutrie N. Physical activity consultation for people with type 2 diabetes: evidence and guidelines. Diabetic Med. 2007; 24:809-816.
18. Gleeson-Kreig JM. Self-monitoring of physical activity: effects on self-efficacy and behavior in people with type 2 diabetes. Diabetes Educ. 2006;32:69-77.
19. Canadian Diabetes Association Clinical Practice Guidelines Expert Committee. Canadian Diabetes Association 2008 clinical practice guidelines for the prevention and management of diabetes in Canada. Can J Diabetes. 2008;32(suppl 1):1-201.
20. Praet E, van Loon LJ. Optimizing the therapeutic benefits of exercise in type 2 diabetes. J Appl Physiol. 2007;103:1113-1120.
21. George VA, Stevenson J, Harris CL, et al. CDE and non-CDE dietitians’ knowledge of exercise and content of exercise programs for older adults with type 2 diabetes. J Nutr Educ Behav. 2006;38:157-162.
22. Bowman A, Foster C. Physical activity advisement practices in diabetes education centres across Canada. Can J Diabetes. 2007; 31:131-139.
23. Tudor-Locke CE, Myers AM, Rodger NW, et al. Towards acceptable exercise guidelines in type 2 diabetes: an examination of current stan-dards and practices. Can J Diabetes Care. 1998;22:47-53.
24. Bandura A. Psychological aspects of prognostic judgments. In: Evans RW, Baskin DS, Yatsu FM, eds. Prognosis of Neurological Disorders, 2nd ed. New York, NY: Oxford University Press; 1992:11-27.
25. Hill-Briggs F, Batts-Turner M, Gary TL, et al. Training community health workers as diabetes educators for urban African Americans: value added using participatory methods. Prog Community Health Partnersh. 2007;1:185-194.
26. Gross R, Tabenkin H, Heymann A, et al. Physicians’ ability to influence the life-style behaviors of diabetic patients: implications for social work. Soc Work Health Care. 2007;44:191-204.
27. Lent RW, Lopez FG. Cognitive ties that bind: a tripartite view of efficacy beliefs in growth promoting relationships. J Soc Clin Psychol. 2002;21:256-283.
28. McAuley L, Mihalko SL. Measuring exercise-related self-efficacy. In: Duda JL, ed. Advances in Sport and Exercise Psychology Measurement. Morgantown, WV: Fitness Information Technology; 1998: 371-390.
29. Tabachnick BG, Fidell LS. Using Multivariate Statistics, 4th ed. New York, NY: HarperCollins College; 2001.
30. Culos-Reed SN, Shields C, Brawley LR. Breast cancer survivors involved in vigorous team physical activity: psychosocial correlates of mainte-nance participation. Psycho-oncology. 2005;14:594-605.
31. Brawley LR, Martin KA, Gyurcsik NC. Problems assessing perceived barriers to exercise: confusing obstacles with attributions and excuses. In: Duda JL, ed. Advances in Sport and Exercise Psychology Measurement. Morgantown, WV: Fitness Information Technology Inc; 1998: 337-350.
32. Hearnshaw H, Hughes N, Dale J, et al. Warwick Certificate in Diabetes Care: an evaluation. Diabetes Prim Care. 2005;7:197-204.
33. Hearnshaw H, Hopkins J, Dale J. A model of effective distributed deliv-ery to healthcare professionals of education in diabetes care. Educ Prim Care. 2004;15:596-605.
34. Population urban and rural, by province and territory, 2001. Statistics Canada website. Available at: http://www40.statcan.gc.ca/l01/cst01/demo62d-eng.htm. Accessed July 15, 2010.