Embed Size (px)
Citation preview

A O S 1999
83
Indocyanine green angiography ofretinal pigment epithelial tearsA. Giovannini1, B. Scassellati-Sforzolini1,2, B. Lafaut2, J. Edeling2,E. D’Altobrando1 and J. J. De Laey2
1Department of Ophthalmology, University of Ancona, Italy2Department of Ophthalmology, Universitair Ziekenhuis Gent, Belgium
ABSTRACT.Purpose: To investigate the fluorescein and indocyanine green (ICG) featuresbefore and after retinal pigment epithelial tear.Methods: Fluorescein and ICG videoangiography were performed in 30 patientsaffected by age-related macular degeneration either complicated by tear of theretinal pigment epithelium (25 eyes) or by pigment epithelial detachment withpretear characteristics (5 eyes).Results: At the pretear stage fluorescein angiography (FA) showed in all casessigns of occult CNV associated with delayed, slow and uneven filling of thepigment epithelium detachment. In 2 eyes the ICG filling of the retinal pigmentepithelial detachment was seen. Progression to the tear stage was seen in 4 eyeswhere a CNV was evident on ICG angiography; in two eyes within one monthafter laser photocoagulation. At the tear stage FA showed an area of markedhyperfluorescence with well defined margins. Adjacent to the exposed area thetorn RPE was markedly hypofluorescent during all angiographic phases. Thebare choroid was always hypo or normofluorescent on ICG angiography. Thetorn retinal pigment epithelium showed moderate hypofluorescence. The exactseat and extension of CNVs could be visualized in 20 cases (67%; 95% C.I.,50–84%) with ICG angiography vs. 6 cases (20%; 95% C.I., 6–34%) with FA(p∞0.001).Conclusions: ICG angiography did not add anything substantial to the analysisof frank tears. The most useful application of ICG angiography in this diseaseis the visualization of the seat and extension of the associated CNV. In fact, itis well known that laser treatment of a pigment epithelial detachment at thepretear stage may facilitate the development of a tear of the RPE.
Key words: age-related macular degeneration – choroidal neovascularisation – fluorescein angio-graphy – indocyanine green angiography – retinal pigment epithelial tear – retinal pigment epi-thelial detachment.
Acta Ophthalmol. Scand. 1999: 77: 83–87Copyright c Acta Ophthalmol Scand 1999. ISSN 1395-3907
Age-related macular degeneration(AMD) is the leading cause of ac-
quired blindness among the elderly in thedeveloped countries (Leibowitz et al.1980; Klein & Klein 1982; Martinez et al.1982; Ferris 1983; Cullinan 1987; Ghaf-our et al. 1988; Thompson & Rosenthal1989; Grey et al. 1989). Tears of the reti-nal pigment epithelium (RPE) have beendescribed as a variance of presentation oras a complication of AMD (Hoskin et al.
1981; Coscas et al. 1982; Cantril et al.1983; Decker et al. 1983; De Laey & Ri-ems 1984; Green & Yarian 1983; TuteinNoltenius & Deutman 1985; Krishan etal. 1985; Giovannini et al. 1987; HallerYeo et al. 1988; Nisha et al. 1995). In1981 Hoskin et al. first described the clin-ical and angiographic characteristics ofthis clinical entity.
Tears of the RPE may present as anapparently primitive form, during the
spontaneous evolution of a pigment epi-thelial detachment (PED) of the elderlyor as a complication of the laser treat-ment of a PED (Hoskin et al. 1981; Co-scas et al. 1982; Green & Yarian 1983; DeLaey & Riems 1984; Gass 1984; TuteinNoltenius & Deutman 1985; Krishan etal. 1985; Giovannini et al. 1987; HallerYeo et al. 1988; Nisha et al. 1995; TheMoorfields Macular Study Group 1982).
A tear of the RPE is not uncommon:about 10% of vascularized PED may de-velop such a complication in the follow-up (Hoskin et al. 1981).
Hoskin et al. (1981), Gass (1984) andCoscas et al. (1990) schematized thenatural course of PED towards tear ofthe RPE into three stages:
1) pretear stage;2) tear stage;3) scarring or cicatricial stage.
There are probably two patterns of reti-nal pigment epithelial tear: rolling-up ofthe free flap of the torn RPE like a pa-pyrus and retraction of the torn RPE.
The fluorescein angiographic charac-teristics of these stages are well known. Onthe contrary, the contributions on indo-cyanine green (ICG) angiography of reti-nal pigment epithelial tear are limited (Co-scas et al. 1994; Colucciello et al. 1997; Ar-royo et al. 1997; Giovannini et al. 1997).
The purpose of this paper is to com-pare the fluorescein and ICG character-istics of retinal pigment epithelial tearand pretear.
Materials and Methods30 eyes of 30 patients (12 males and 18females; age: 59–84 years; mean age:72.3) who underwent fluorescein andICG angiography in the University Eye

A O S 1999
84
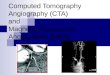
Fig. 1. PED at the pretear stage. a–b) Fluorescein angiography shows thedelayed filling of the PED with a notch and hot spot at its inferior mar-gin. c) The ICG angiography at 5:30 min. displays the exact seat andextension of the CNV, the PED is hypofluorescent. d) On the late framesof ICG angiography (34:10 min) a partial progressive filling of the PEDfrom the CNV can be observed. e) Less than two months after laserphotocoagulation of the CNV a tear of the RPE is evident on fluorescein angiography. f) The ICG angiographic sequence shows the hypofluorescenceof the exposed choroid and a large area of hyperfluorescence, probably corresponding to the still active CNV.

A O S 1999
85
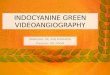
Fig. 2. Tear of the RPE. a) Fluorescein angiography shows a crescent shaped area of marked hyperfluorescence with well defined margins correspond-ing to the exposed choroid. The retracted and folded RPE is intensely hypofluorescent. Stippled hyperfluorescence is evident temporally to the tornRPE. b) The late phases of ICG angiography show the presence of a CNV that was almost completely masked by the torn RPE. The exposedchoroid is slightly hypofluorescent.
Fig. 3. Very large macular tear of the RPE. a) Marked hyperfluorescence in the area of the retinal pigment epithelial tear can be seen on fluoresceinangiography. Hyperfluorescence is evident underneath the area of hypofluorescent retracted RPE. b) A hyperfluorescent plaque can be observed inthe late phases of ICG angiography in the region of retracted RPE. The bare choroid is intensely hypofluorescent.
Clinics of Ancona and Gent between1992 and 1997 for AMD complicated byPED, with signs of tear or pretear of theRPE, were retrospectively analysed.
Five eyes were at the pretear stage, 25at the tear stage.
Patients were included in the pretearstage group if fundus examination re-vealed two or more of the followingcharacteristics:O uneven elevation of the PED often as-
sociated with an adjacent neuroepi-thelium detachment;
O signs of occult CNV (presence of splithaemorrhages and hard exudates);
O stretching of the margin of the PED.The tear stage group included patientswhere an area of exposed choroid, as a
consequence of the retraction or displace-ment of the torn RPE, was present at thefundus examination.
ICG angiography was performedusing 25–50 mg of ICG (Cardiogreen,Hynson, Westcott and Dunning, Inc.,Baltimore, MD, USA). The dye was in-jected into a peripheral arm vein andwas followed immediately by a 5 mlflush of sterile saline via a three-waystopcock.
The ICG angiographic phases were de-fined as follows (Yannuzzi et al. 1997):O early phase: from the choroidal blush
until 2–3 minutes;O middle phase: between 5 and 15 min-
utes;O late phase: more than 20 minutes.
The comparison between fluorescein andICG angiographic characteristics of thepretear and tear groups was performedusing the Mc Nemar’s test for dependentvariables.
ResultsPretear stage (5 eyes) (Table 1)
At this stage fluorescein angiography(Fig. 1a–b) displayed signs of occult CNVin all cases (notch of one of the marginsof the detachment, visualization of oneor more hot-spots). A delayed, slow anduneven filling of the PED with hypofluo-rescence of the center until the late phasesof the angiogram and progressively in-

A O S 1999
86
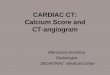
Fig. 4. Large temporal tear of the RPE. a) On fluorescein angiography the bare choroid is hyperfluorescent, while the torn RPE partially masks thechoroidal fluorescence. b) On the late frames of ICG angiography an area of hyperfluorescence consistent with a CNV can be observed. The barechoroid is slightly hypofluorescent.
creasing hyperfluorescence of the marginswas also evident (Fig. 1a–b).
On ICG angiography (Fig. 1c–d) thePED was always hypofluorescent in theearly phases. A progressive hyperfluor-escence of the PED from the middlephases of the angiogram with a partialor complete filling in the late phases, wasobserved in 2 eyes.
ICG angiography allowed to visualizea well defined CNV within the PED or atits margins in 4 of 5 eyes (Fig. 1c–d),while fluorescein angiography did notshow any classic CNV.
All 4 eyes with well defined CNV onICG angiography progressed to the tearstage (2 eyes with ICG filling of the PEDand two with no filling of the PED). In 2of the 4 eyes a laser photocoagulation ofthe CNV had been performed before thetear occurred (Fig. 1e–f). In 1 case no ripwas seen after 14 months of follow-up.
Tear stage (25 eyes)
Fluorescein angiography (Fig. 2a, 3a, 4a)showed from the early phases an area ofmarked hyperfluorescence with well de-fined margins corresponding to the barechoroid. The hyperfuorescence increasedin the late phases. Adjacent to the ex-
Table 1. Fluorescein and ICG angiography of CNVs in 30 patients affected by AMD at thepretear and tear stages.
Choroidal neovascularmembrane Fluorescein angiography ICG angiography Either method
Pretear stage 0/5 (0%) 4/5 (80%) 4/5 (80%)Tear stage 6/25 (24%) 16/25 (64%) 16/25 (64%)Total 6/30 (20%) 20/30 (67%) 20/30 (67%)
posed area, the torn RPE was markedlyhypofluorescent during all angiographicphases. In two cases a secondary PEDwas present.
On ICG angiography (Fig. 2b, 3b, 4b)hypo- or normal fluorescence was alwaysobserved in the area of exposed choroid.The torn retinal pigment epitheliumshowed a moderate hypofluorescence.
On fluorescein angiography a well de-fined CNV was observed in 6 of 25 eyes(24%; 95% CI, 7–41%). ICG angiographyrevealed the presence of the CNV in 16of 25 eyes (64%; 95% CI, 45–83%), in-cluding the 6 eyes where fluorescein an-giography was positive.
If we consider all 30 cases of tear andpretear, the exact seat and extension ofthe CNV was visualized in 20 cases (67%;95% CI, 50–84%) with ICG angiographycompared to only 6 cases (20%; 95% CI,6–34%) with fluorescein angiography(p∞0.001 Mc Nemar’s test).
DiscussionIn spite of the numerous biomicroscopicand fluorescein angiographic signs, thediagnosis of pretear of the RPE is often
difficult. Ophthalmoscopy shows an un-even elevation of the PED. On fluoresceinangiography the PED presents a delayedand non homogeneous filling: a markedhyperfluorescence of the margins with acentral hypofluorescence in the latephases. The shape of the detachment ischaracterized by the stretching of one ofthe edges. Sometimes a crescent-likehemorrhage is evident next to the mar-gins of the PED. The signs are often illdefined; it can be therefore not easy torecognize those PEDs at high risk of rip.
In our series, in 2 of the PEDs at thepretear stage, a progressive ICG leakagefrom the CNV into the detachment wasobserved. The marked hyperpermeabilityof the CNV could explain the ICG fillingof the PED, as ICG leaks abundantlyonly in the presence of an increased per-meability of the vessels’ walls.
The diagnosis of acute tear can be al-ready made with fluorescein angiography.In our series the area of exposed choroidwas always hyperfluorescent with well de-fined edges from the early phases into thelate phases of fluorescein angiography.An increased visualization of the cho-roidal vessels was evident. The torn RPEblocked choroidal fluorescence during allangiographic phases.
ICG angiography did not add any sub-stantial information to the fluoresceinangiographic picture at the acute stage.The area of exposed choroid was alwayshypo- or normofluorescent on ICG an-giography. The torn retinal pigment epi-thelial flap showed a variable degree ofhypofluorescence in the early and middlephases of ICG angiography. In the late

A O S 1999
87
phases such hypofluorescence was oftenmasked by the leakage of dye from theCNV.
ICG angiography at the pretear andtear stage allowed the diagnosis of CNVin a greater number of cases than fluor-escein angiography: in 20 cases (66.7%)the exact seat and extension of CNVscould be visualized with ICG angiogra-phy compared to only 6 cases (20%) withfluorescein angiography (p∞0.001).
Concerning those cases where no CNVwas seen with either technique, it can behypothesized that we are dealing with oc-cult new vessels on ICG angiography aswell. In many of these cases an ill definedlate leakage was observed on the latephases of ICG angiography. There is nogeneral agreement on the presence of theCNV at the acute stage of the retinal pig-ment epithelial tear. Some authors (Hos-kin et al. 1981; Green et al. 1985; HallerYeo et al. 1988), believe that a tear of theRPE could develop even in the absence ofchoroidal new vessels, but their work havebeen published in the pre-ICG angiogra-phy era. For Gass (1984) a CNV is alwayspresent and the rip occurs at the junctionbetween detached and adherent RPE. Ahistopathologic study on two eyes (Greenet al. 1985) showed that a rip can be associ-ated with atrophy of the RPE and may oc-cur even in the absence of CNV.
Retinal pigment epithelial tear is oneof the major causes of severe visual lossin AMD (Schoeppner et al. 1989). Pros-pective studies on larger series of patientswith PED at the pretear stage are necess-ary. It is important to assess the statisti-cal significance of the predictive value ofthe fluorescein and ICG angiographicsigns at this stage. It is, in fact, wellknown that laser treatment of a PED atthe pretear stage may precipitate the de-velopment of a tear of the RPE (Gass1984). Even in the ICG era, the photoco-agulation of the CNV within or at themargins of a PED is still challenging andtreatment is frequently unsuccessful; inour series the 2 cases of CNV at the pre-tear stage who underwent laser photoco-agulation developed a tear of the RPEwithin one month. This is due to eitherincomplete visualization of the CNV orto the fact that the density of the subreti-nal fluid or the elevation of the detach-ment prevents the delivery of sufficientlaser energy at the level of the CNV. An-other cause of disappointing results afterlaser photocoagulation can be the pres-ence of chorioretinal anastomoses associ-ated with the CNV (Kuhn et al. 1995).
AcknowledgementsThe authors thank Dr. Luigi Ferrante of theDepartment of Biomedical Sciences of theUniversity of Ancona, who provided all the as-sistance in the statistic elaboration of the data.
ReferencesArroyo JG, Schatz H, McDonald R & Johnson
RN (1997): Indocyanine green videoangio-graphy after acute retinal pigment epithelialtears in age-related macular degeneration.Am J Ophthalmol 123: 377–385.
Cantril HL, Ramsay RC & Knobloch WH(1983): Rips in the pigment epithelium. ArchOphthalmol 101: 1074–1079.
Colucciello M, Ginsburg LH & SammartinoJP (1997): Indocyanine green angiographicevaluation of retinal pigment epithelialtears. Retina 17: 23–27.
Coscas G, Quentel G & Soubrane G (1982):Dechirure spontanee de l’epithelium pig-mentaire dans la region maculaire. Bull SocOphtalmol Fr 82: 815–820.
Coscas G, Koenig F & Soubrane G (1990): Thepretear characteristics of pigment epithelialdetachments. A study of 40 eyes. ArchOphthalmol 108: 1687–1693.
Coscas G, Krott R, Quaranta M & SoubraneG (1994): Decollement de l’epithelium pig-me ithelium pigmentaire. Ophtalmologie 8:452–456.
Cullinan TM (1987): The epidemiology ofblindness. In, Miller S, ed. Clinical Ophthal-mology. Bristol, England: Wright 571–578.
Decker WL, Sanborn GE, Ridley M, AnnesleyWH & Sorr EM (1983): Retinal pigment epi-thelial tears. Ophthalmology 90: 507–512.
De Laey JJ & Riems D (1984): Ripping of de-tached retinal pigment epithelium in senilemacular degeneration. Bull Soc Belge Opht-almol 207: 27–35.
Ferris FL III (1983): Senile macular degenera-tion: review of epidemiologic features. Am JEpidemiol 118: 132–151.
Gass JDM (1984): Pathogenesis of tears of theretinal pigment epithelium. Br J Ophthalmol68: 513–519.
Gass JDM (1984): Retinal pigment epithelialrip during krypton red laser photocoagu-lation. Br J Ophthalmol 98: 700–706.
Ghafour M, Allan D & Foulds WS (1988):Common causes of blindness and visualhandicap in the west of Scotland. Br JOphthalmol 167: 209.
Giovannini A, Sperti F & Volanti S (1987): De-chirure de l’epithelium pigmentaire. Evolu-tion naturelle de l’affection. Ophtalmologie2: 187–189.
Giovannini A, Scassellati-Sforzolini B, D’Alto-brando E, Mariotti C & Tittarelli R (1997):Indocyanine green videoangiography ofidiopathic serous pigment epithelium de-tachment. Retina 17: 286–293.
Green SN & Yarian D (1983): Acute tear ofretinal pigment epithelium. Retina 3: 16–20
Green WR, McDonnel PJ & Yeo JH (1985):
Pathologic features of senile macular de-generation. Ophthalmology 92: 615–627.
Grey RHB, Burns-Cox CJ & Hughes A (1989):Blind and partial sighted registration inAvon. Br J Ophthalmol 73: 988.
Haller Yeo J, Marcus S & Murphy RP (1988):Retinal pigment epithelial tears. Pattern andprognosis. Ophthalmology 95: 8–13.
Hoskin A, Bird AC & Sehmi K (1981): Tearsof detached retinal pigment epithelium. Br JOphthalmol 65: 417–422.
Klein BE & Klein R (1982): Cataracts andmacular degeneration in older Americans.Arch Ophthalmol 100: 571–573.
Krishan NR, Chandra SR & Stevens TS(1985): Diagnosis and pathogenesis of reti-nal pigment epithelial tears. Am J Ophthal-mol 100: 698–707.
Kuhn D, Meunier I, Soubrane G & Coscas G(1995): Imaging of chorioretinal anastom-oses in vascularized retinal pigment epithel-ium detachments. Arch Ophthalmol 413:1392–1398.
Leibowitz HM, Krueger DE, Maunder LR etal. (1980): The Framingham Eye Studymonograph. An ophthalmological and epi-demiological study of cataract, glaucoma,diabetic retinopathy, macular degenerationand visual acuity in a general population of2631 adults, 1973–1975. Surv Ophthalmol24 (suppl): 335–610.
Martinez GS, Campbell AJ, Reinken J & AllanBC (1982): Prevalence of ocular disease in apopulation study of subjects 65 years oldand older. Am J Ophthalmol 94: 181–189.
The Moorfields Macular Study Group (1982):Retinal pigment epithelial detachment in theelderly. A controlled trial of argon laserphotocoagulation. Br J Ophthalmol 66: 1.
Nisha RK, Suresh RC & Thomas SS (1995):Diagnosis and pathogenesis of retinal pig-ment epithelial tears. Am J Ophthalmol 100:698–707.
Schoeppner G, Chuang EL & Bird AC (1989):The risk of fellow eye visual loss with unilat-eral retinal pigment epithelial tears. Am JOphthalmol 108: 683–685.
Thompson JR & Rosenthal AR (1989): Recenttrends in the registration of blindness andpartial sight in Leicester. Br J Ophthalmol73: 95.
Tutein Noltenius PA & Deutman AF (1985):Rips of the retinal pigment epithelium. IntOphthalmol 8: 19–23.
Yannuzzi LA, Flower RW & Slakter JS (1997):Indocyanine green angiography. Mosby-Year Book, St Louis.
Received on February 16th, 1998.Accepted on August 13th, 1998.
Corresponding author:
Alfonso Giovannini, MDDepartment of OphthalmologyUniversity of AnconaOspedale di Torrette60020 Ancona, ItalyTel. 39 071 5964384. Fax 39 071 5964377