Embed Size (px)
Citation preview

Journal of Visceral Surgery (2014) 151, 117—124
Available online at
ScienceDirectwww.sciencedirect.com
REVIEW
Indocyanine green fluorescence imaging inthe surgical management of liver cancers:Current facts and future implications
C. Lima,∗, E. Vibertb, D. Azoulaya, C. Sallouma,T. Ishizawac, R. Yoshiokac, Y. Misec, Y. Sakamotoc,T. Aokic, Y. Sugawarac, K. Hasegawac, N. Kokudoc
a
Service de Chirurgie Digestive, Hépatobiliaire, Pancréatique et Transplantation Hépatique,Hôpital Henri-Mondor, Assistance Publique—Hôpitaux de Paris, 51, avenue duMaréchal-de-Lattre-de-Tassigny, 94010 Créteil, Franceb Service de Chirurgie Hépatobiliaire, Pancréatique et Transplantation Hépatique, HôpitalPaul-Brousse, 12, avenue Paul-Vaillant-Couturier, 94804 Villejuif, Francec Hepato-Biliary-Pancreatic Surgery Division, Department of Surgery, Graduate School ofmedicine, University of Tokyo, Tokyo, JapanAvailable online 21 January 2014
KEYWORDSFluorescence;Indocyanine green;Hepatocellularcarcinoma;Liver metastases;Camera
Summary Imaging detection of liver cancers and identification of the bile ducts duringsurgery, based on the fluorescence properties of indocyanine green, has recently been devel-oped in liver surgery. The principle of this imaging technique relies on the intravenousadministration of indocyanine green before surgery and the illumination of the surface of theliver by an infrared camera that simultaneously induces and collects the fluorescence. Detec-tion by fluorescence is based on the contrast between the (fluorescent) tumoral or peri-tumoraltissues and the healthy (non-fluorescent) liver. Results suggest that indocyanine green fluores-cence imaging is capable of identification of new liver cancers and enables the characterizationof known hepatic lesions in real time during liver resection. The purpose of this paper is topresent the fundamental principles of fluorescence imaging detection, to describe successivelythe practical and technical aspects of its use and the appearance of hepatic lesions in fluores-cence, and to expose the diagnostic and therapeutic perspectives of this innovative imagingtechnique in liver surgery.© 2013 Elsevier Masson SAS. All rights reserved.
Introduction
During the last couple of years, medical imaging research has been rejuvenated bythe development of lesion detection with fluorescence. Several medico-surgical special-ties (dermatology [1], pulmonology [2], urology [3], neurosurgery [4], gastro-intestinalsurgery [5], as well as plastic and reconstructive surgery [6]) now use fluorescence imag-ing techniques to diagnose cancer or premalignant lesions, and/or lymph nodes draininga tumor. The principle behind this imaging technique relies on the administration of
∗ Corresponding author.E-mail address: [email protected] (C. Lim).
1878-7886/$ — see front matter © 2013 Elsevier Masson SAS. All rights reserved.http://dx.doi.org/10.1016/j.jviscsurg.2013.11.003

1
a‘pimccptI
sittttfi
C
Iiccabdosaohcc
afahaaditsaoiftanodh
I
Iriww
itpero
eiltwewi
wllT
wasrbaaic1
iba(lIcbb
18
fluorescent marker capable of specifically targeting‘fluorescent’’ cancer cells; this has opened one of the mostromising fields of tumor detection. Indocyanine green (IG)s a soluble dye, which emits a fluorescent light when illu-inated by an infrared laser source. In hepatic surgery, IG
learance is used to evaluate hepatic function before surgi-al procedures [7—9], but the application of the fluorescentroperties of IG is just beginning. The first application ofhis imaging technique in hepatic surgery was reported byshizawa et al. in 2009 [10].
The goal of this update was to report the experience ofeveral Asiatic teams with this innovating intra-operativemaging technique in hepatic surgery, and, after presentinghe concept and the technical bases of fluorescence imaging,o summarize the practical and technical aspects of its use,o describe the features of the images that can be obtained,o review the pathophysiologic mechanisms implicated, andnally to outline the limitations of its use in hepatic surgery.
oncept
ndocyanine green is a fluorescent dye that has been usedn ophthalmology to visualize the retinal and choroid vas-ularization for more than 20 years [11]. Its metabolicharacteristics (intravascular confinement enhanced by fix-tion to plasma proteins and rapid hepatic excretion intoile), the spectral proprieties of this molecule, and theevelopment of new imaging systems has extended the fieldsf application of IG fluorescence to several other surgicalpecialties (cardiac surgery [12], neurosurgery [13], plasticnd reconstructive surgery [6]). In oncologic surgery, IG flu-rescence has been tested to detect kidney tumors [3], andas been used for detection of sentinel lymph nodes in breastancer [14], malignant melanoma [15] and gastro-intestinalancers [16—18].
In hepatic surgery, this dye has been used to evalu-te hepatic function and outline hepatectomy strategiesor oncologic resections [19,20], and for living donor hep-tic transplantation [21]. More recently, teams from Asiaave improved imaging techniques based on IG fluorescence,
llowing the visualization of bile ducts [22—24], as wells hepatocellular carcinoma (HCC) and hepatic metastasesuring liver surgery [10,25]. Basically, IG is administeredntravenously 12 to 48 hours before surgery and lights uphe liver surface when illuminated with a near-infraredource. After injection, IG is rapidly taken up by tumoralnd non-tumoral hepatocytes. In the presence of normalr subnormal hepatic function and in the absence of bil-ary obstruction, IG is excreted in the bile and disappearsrom healthy liver parenchyma within a few hours [26]. Onhe other hand, IG remains fixed in tumoral hepatocytesnd in pathological areas of the liver, particularly aroundon-hepatocellular tumors. Thanks to particular featuresf the camera, the fluorescent light emitted by IG allowsetection of hepatocellular (tumor fluorescence) and non-epatocellular (peri-tumoral fluorescence) tumors.ndocyanine green
ndocyanine green is a hydrosoluble molecule that fixesapidly and intensely to plasma proteins after intravenousnjection. Also, 98—99% of IG molecules link to proteinsith a large proportion becoming fixed to high moleculareight proteins such as albumin. The mode of elimination
ric
T
A
TocuriTrritIitsfi
C. Lim et al.
s exclusively hepatobiliary. IG is selectively taken up byhe hepatocytes and excreted in bile via an active trans-ort system. IG is not metabolized and does not enter thenterohepatic circulation. Consequently, the disappearanceate of IG from plasma to bile reflects the excretory functionf the liver [27].
Schematically, all molecules can take on different lev-ls of electronic energy. In its basal state, molecular energys minimal. Under the action of light, depending on wave-engths, absorbed light can raise the level of energy. Ashe molecule returns to its basal state, light is emittedith a wavelength superior to the light responsible for thexcitation. The difference between excitation and emissionavelengths is exploited thanks to cameras equipped with
nterferential filters to obtain the images.When the IG-protein complex is excited by a light source
ith a wavelength between 750 and 810 nm, fluorescentight with a wavelength of approximately 830 nm (wave-ength situated in the infrared spectrum) [28] is emitted.he human eye cannot see these wavelengths.
Fluorescent light is largely attenuated by hemoglobin andater as it traverses biological tissues. Hemoglobin stronglyttenuates all wavelengths less than 700 nm (which corre-ponds in fact to the entire visible spectrum excepting deeped). Water is transparent in visible and near-infrared lightut attenuates wavelengths over 900 nm. There is therefore
‘‘window’’ of wavelengths at the limit between deep rednd near infrared (700—900 nm) where tissue transparencys maximal. This is one of the reasons why IG fluorescencean be detected in the near-infrared zone from as deep as0 mm from the surface of tissues.
In France, the only fluorescent molecules approved fornjection in man are fluorescein and IG and both cane administered intravenously. Indocyanine green has andvantage in that is absorbs light in the near infrared rangewhile the spectrum of fluorescein is in the range of visibleight) and can be detected much deeper in tissues. AlthoughG seems to be better tolerated than fluorescein, severalases of allergy (hives, nausea and anaphylactic shock) haveeen reported in ophthalmology. Some of these cases haveeen attributed to the iodide contained in certain prepa-
ations of IG. In case of recognized allergy to iodine, its necessary to use special preparations of IG that do notontain iodine [29].echnique
pparatus
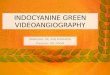
he device used is not specifically designed for intra-perative use, but the camera can be equipped with a sterileover that allows the operator to manipulate the apparatusnder sterile conditions. A portable imaging system provideseal time quantitative fluorescent imaging (Fig. 1). Thismaging system includes an infrared camera and amplifier.he camera simultaneously provides the functions of fluo-escence excitation with a laser (LED emitting an infraredadiance) diffused over the operative field and fluorescencemage acquisition is ensured by a captor (CCD), which filtershe light so that only near infrared wavelengths can be seen.n practice, the camera and cable do not need to be steril-zed. The length of the cable allows the screen and amplifiero be placed sufficiently far away so that a non-sterile per-on can hold the infrared camera above the sterile operativeeld. New imaging systems have been developed recently,

Indocyanine green fluorescence imaging 119
ncludfrare
can
rtesy
time, most clinical studies, especially in the domain of
Figure 1. Fluorescence imaging system. A. The imaging system ithe excitation of fluorescence thanks to a laser (LED emitting an in(CCD) which filters the light so that only near infrared wavelengthsPhotos published courtesy of Pr. Norihiro Kokudo, and photo 1C cou
measuring the fluorescence in the near infrared spectrumwhile the area under investigation is illuminated with whitelight.
Utilization
In Asia, the indications for liver resection and the type ofhepatectomy are determined according to a flow chart thattakes into account the presence or absence of controlledascites, total bilirubin, and IG clearance at 15 minutes [19].This test is performed three days before surgery on average(1 to 7 days for HCC and 1 to 14 days for metastases) [10,30].IG is injected intravenously at a dosage of 0.25 to 0.5 mg/kg,depending on the team. The exact optimal dosage remainsto be defined. The investigation is performed by placing theinfrared camera above the liver. The light in the operationroom should be decreased as much as possible to improvethe contrast of images seen on the screen.
The contrast between fluorescent (tumor) and non-fluorescent (non-tumoral parenchyma) areas dependsclosely on the interval between the time of IG injectionand the moment when the fluorescence is measured, aswell as on the liver function of the patient. IG should beinjected 12 to 48 hours before the operation, thus allow-ing a ‘‘wash-out’’ of IG from normally functioning liver tooccur, i.e. the lesions become fluorescent while the fluores-cence of the non-tumoral parenchyma is completely washedout (and therefore non-fluorescent). Of note, the greaterthe impairment of liver function (particularly in the caseof preoperative portal embolization), the more intense andpersistent is the parenchymal fluorescence [31].
es a camera and amplifier. B. The camera simultaneously inducesd radiance) and acquires fluorescence images ensured by a captorbe seen. C. Intra-operative use of fluorescence imaging.
of Dr Takeaki Ishizawa [30].
Cost and future perspectives
A fluorescence detection apparatus costs between 45,000and 50,000 euros in France. It is sold by a Japanese firm,Hamamatsu Photonics, and distributed by Pulsion Medi-cal Systems in France and in Europe. At the present
plastic and reconstructive surgery, use the apparatus com-mercialized by Hamamatsu Photonics (PDETM, HamamatsuPhotonics, Hamamatsu, Japan). Other systems avail-able include the SPYTM (Novadaq Technologies, Concord,Canada) and the FluobeamTM systems (Fluoptics, Grenoble,France).
Lastly, other applications of this new imaging tech-nique are under investigation in laparoscopic and roboticsurgery.
Detection of liver tumors
Aspect of fluorescent lesions
The fluorescent aspect of HCC is variable (Figs. 2—4) [10,25].Well-differentiated HCC are seen as intense and homoge-neous fluorescent spots whereas moderately differentiatedHCC are seen as partial and heterogeneous areas. Poorlydifferentiated HCC and liver colorectal (adenocarcinoma)metastases are not visible in fluorescence and the charac-teristic of these lesions is a fluorescent ring correspondingto the peri-tumoral parenchyma surrounding an empty zonecorresponding to the lesion.

120 C. Lim et al.
F minaV metapF
P
TciIh(tPvoacclct
mact
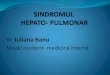
igure 2. Intra-operative view with and without liver surface illu. B. Hepatocellular carcinoma in segment VI. C. Subcapsular liver
alpable (arrow).
igures courtesy of Dr Takeaki Ishizawa [30].athophysiological mechanisms
he pathophysiological mechanisms underlying the fluores-ent anomalies are not totally elucidated but could possiblymplicate hepatocyte-to-bile duct secretion anomalies [32].t has been well established that IG selectively taken up byepatocytes via two membrane transport systems, OATP1B3transporter belonging to the family of OATP or organic anionransporters) and NTCP (Na+/Taurocholate Co-transportingolypeptide). The molecule is then excreted into the bileia other membrane transporters located on the membranesf the biliary canalicules (MRP2 or multidrug-resistance-ssociated protein 2) [33]. The fluorescence obtained in thease of well-differentiated HCC could be related to MRP2analicular transporter anomalies, which lead to intracel-ular accumulation of IG. This hypothesis implies that IG isaptured by tumor cells but cannot be excreted correctly inhe biliary canalicules.
Conversely, in poorly differentiated HCC and colorectaletastases, the lack of fluorescence could be interpreted
s the absence of capture of the molecule by the tumorells. Here again, the mechanism responsible for the peri-umoral fluorescence is not known but could imply impaired
h[oeolcbrdda
ofi
V
T
Is
tion by infrared camera. A. Hepatocellular carcinoma in segmentstases. Among the three nodules, only one was neither visible nor
epatocyte biliary secretion in immature hepatocytes34]. In a recently published Dutch study [34], the authorsbserved fluorescence in the cytoplasm and outside cellsxpressing the CK7 marker with a microscope. The presencef CK7+ cells was mostly detected at the periphery ofiver metastases. These cells expressing the CK7 markeran be identified as progenitor cells (dual hepatocyte andiliary potentiality) and attests to the presence of a ductaleaction associated with liver metastases. In addition, aecrease in membrane transporter expression leading toecreased excretion of several molecules, including IG, haslso been observed.
The rationale behind peri-tumoral fluorescence reposesn the hypothesis that IG accumulation in the CK7+ cellsound in the peripheral ductular reaction of liver metastasess largely responsible for this peri-tumoral fluorescence.
alue of the technique
umor localization
ntra-operative fluorescence could improve detection ofmall superficial lesions and help to determine the nature of

Indocyanine green fluorescence imaging 121
Figure 3. Fluorescent imaging on hepatectomy specimens. A. Total and homogeneous fluorescence imaging (well-differentiated HCC). B.Partial fluorescence imaging (moderately differentiated HCC). C. Peri-tumoral fluorescence (fluorescent ring, poorly differentiated HCC).D. Peri-tumoral fluorescence (colorectal liver metastasis).Figures courtesy of Dr Takeaki Ishizawa [30].
Figure 4. Schematic aspect of liver lesion seen in fluorescence.

1
te(swsl
spciaottlmceuaiPo
mtracss
S
Botuap
Fsd
22
hese lesions, especially when clinical examination, preop-rative imaging (CT, MRI), and intra-operative investigationsinspection, liver palpation and ultrasound) are inconclu-ive. Currently, fluorescence findings should be comparedith those obtained by inspection, liver palpation and ultra-
ound, in order to determine the existence of supplementaryesions.
The limits of this technique today are related to the sen-
itivity of the camera and the function of the underlyingarenchyma. In certain patients with cirrhosis, present-dayameras occasionally detect several hot spots correspond-ng to dysplastic and/or regeneration nodules rather than touthentical HCC. In the cirrhotic liver, thanks to the intensityf the fluorescence, this type of camera is especially usefulo detect one or more peripheral satellite nodules aroundhe main nodule. This technique is useful in the ‘‘healthyiver’’, particularly during the treatment of colorectal liveretastases, and has an impact on therapy in 5% to 8% ofases [31]. Another value of this technique is to visualizextra-hepatic metastases of HCC (sub-diaphragmatic nod-les, peritoneal carcinomatosis and lymph-nodes), but heregain the mechanism behind this extra-hepatic fluorescences unknown and comparative studies (fluorescence vs. CT andET-CT scans) are necessary to evaluate the true mechanismf action [35].
The most innovative concept consists of detection oficrometastases by multislice illumination of the opera-
ive specimen [36]. This type of investigation does notequire any complementary techniques (occult metastasesre usually detected by immunohistology). This techniqueould also allow intra-operative analysis of the quality ofurgical excision, by distinguishing between R0 and R1 exci-ions.
stp[etTlsb
fli••
tnc
fb
igure 5. Formal segment VI resection. A. Early images after ultrasouegment VI) of indocyanine green. B. Resection of segment VI. Note theivision.
C. Lim et al.
urgery of liver tumors
ased on the same principle as methylene blue tattooingf the liver segment to be resected (puncture of the por-al branch of the segment and injection of methylene bluender ultrasound guidance), intra-operative fluorescencellows outlining of the segment(s) to be resected, in order toerform a formal liver resection (Fig. 5) [37]. During laparo-
copic hepatectomies, difficulties in delimiting the territoryo resect may arise because the abilities to inspect and pal-ate are limited compared with conventional open surgery38]; this is also true for repeat hepatectomy where the pres-nce of adhesions on the surface of the liver make it difficulto visualize the tattooed territory or the limits of ischemia.he technique of IG injection is also useful in performingiver resections for biliary lesions that cause localized biliarytasis. Strong fluorescence can be detected in the stagnantiliary zone [39].
In sum, the most pertinent indications of the use of IGuorescence in the management of malignant liver tumors
nclude:detection of small superficial nodules;identification and characterization of HCC and colorectalliver metastases, distinguishing between these lesions andbenign lesions.
At the present time, there is not enough available datao justify the use of this technique to detect extra-hepaticodules or to find hepatic lesions that disappear underhemotherapy.
In the future, this technique should potentially be usefulor laparoscopic resections, not only to identify the lesionsut also to determine the resection margins, which are
nd-guided puncture and intraportal injection (in portal branch of presence of fluorescent parenchyma in segment VI in the plane of

Indocyanine green fluorescence imaging
often difficult to determine during atypical resection vialaparoscopy.
Limitations
The main limitation of this imaging technique is low sen-sitivity for the detection of deep nodules and the falsepositive results seen in the cirrhotic liver. These limi-tations are anatomical, but also related to the physicalproperties of IG because of the attenuation of fluores-cence as the proportion of light reaching the cameradecreases as it traverses tissues. Thus only superficialor fluorescent structures less than 10 mm deep can bevisualized. Ishizawa et al. reported a detection rate of65% (37/57 lesions) in a series of 26 patients with a totalof 57 lesions (41 HCC and 16 metastases) [10,30]. Lesionsnot identified by fluorescence were smaller (11 mm vs.18 mm) and deeper (10 mm vs. 2 mm) than those visibleunder fluorescence. Intra-operative ultrasound allowed thedetection of 33 HCC nodules and 16 metastases (86% detec-tion rate). Nonetheless, among the eight HCC undetectedby ultrasound, three nodules were found by fluorescence(sub-capsular located 1—2 mm below the surface of theliver).
Moreover, it is important to recognize that false posi-tive findings have been reported with this technique. Benignlesions such as regenerative nodules or biliary hamartomascan generate hyperfluorescence, indistinguishable from thatproduced by malignant lesions. Approximately 40 to 50% oflesions visualized by fluorescence in HCC resection speci-mens were false positives [10,25].
Lastly, there are no studies that allow confirmation of theabsence of tumor cells in the hyperfluorescent halo foundon the periphery of metastases; fluorescence measurementtherefore does not allow affirmation of the R0 character ofresection.
Conclusions and perspectives
Indocyanine green fluorescence imaging is a promising tech-nique in liver surgery. This technique provides additionalinformation in the localization and diagnosis of the moresuperficial lesions. The anatomical limits (loss of diagnos-tic sensitivity for deep nodules) of this imaging requirefurther optimization to improve the results. Additionalknowledge on hepatobiliary transport systems and patho-physiologic mechanisms should allow further progress withthis technique. In the future, this new imaging techniqueand navigation tool should allow detection of subclinicallesions and increase the safety and precision of hepatec-tomies.
ESSENTIAL POINTS
• Imaging based on the fluorescent proprietiesof indocyanine green allows simultaneous visua-lization of biliary canals and hepatic segments, aswell as liver cancer, during liver surgery.
123
• Detection of lesions by fluorescence is basedon the contrast between tumor or peri-tumoral(fluorescent) tissues and the rest of the (non-fluorescent) liver.
• The study of indocyanine green fluorescenceproperties is enhanced by the fact that injectionof the substance does not alter the usualmanagement of patients.
• Indocyanine green (potentially serving toevaluate the liver function before performinghepatectomy) is administered intravenously 12 to48 hours before the operation.
• At the present time, the most pertinentindications are the identification and charac-terization of HCC and colorectal liver metastasesas well as the differential diagnosis of benignlesions.
• The evaluation of the results of this imagingtechnique is still limited in the literature. Inparticular, there is no evidence that fluorescenceimproves the intra-operative detection of liverlesions compared with ultrasound.
• The mechanisms behind the fluorescence ano-malies could be related to faulty biliary excretion.
• An essential limitation of this imaging technique isits low sensitivity for detection of nodules deeperthan 10 mm.
• The use of fluorescence imaging with indocyaninegreen is currently under evaluation for roboticsurgery.
Disclosure of interest
The authors declare that they have no conflicts of interestconcerning this article.
References
[1] Morton CA, Brown SB, Collins S, et al. Guidelines for topicalphotodynamic therapy: report of a workshop of the BritishPhotodermatology Group. Br J Dermatol 2002;146(4):552—67.
[2] Lam B, Wong MP, Fung SL, et al. The clinical value of autoflu-orescence bronchoscopy for the diagnosis of lung cancer. EurRespir J 2006;28(5):915—9.
[3] Tobis S, Knopf JK, Silvers CR, et al. Near infrared fluorescenceimaging after intravenous indocyanine green: initial clinicalexperience with open partial nephrectomy for renal corticaltumors. Urology 2012;79(4):958—64.
[4] Stummer W, Stocker S, Wagner S, et al. Intraoperative detec-tion of malignant gliomas by 5-aminolevulinic acid-inducedporphyrin fluorescence. Neurosurgery 1998;42(3):518—25 [dis-cussion 525-6].
[5] Kusano M, Tajima Y, Yamazaki K, et al. Sentinel node map-ping guided by indocyanine green fluorescence imaging: a newmethod for sentinel node navigation surgery in gastrointestinalcancer. Dig Surg 2008;25(2):103—8.
[6] Ogata F, Narushima M, Mihara M, et al. Intraoperative lym-phography using indocyanine green dye for near-infraredfluorescence labeling in lymphedema. Ann Plast Surg2007;59(2):180—4.
[7] Hemming AW, Scudamore CH, Shackleton CR, et al. Indocyaninegreen clearance as a predictor of successful hepatic resectionin cirrhotic patients. Am J Surg 1992;163(5):515—8.

1
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
24
[8] Lau H, Man K, Fan ST, et al. Evaluation of preoperative hepaticfunction in patients with hepatocellular carcinoma undergoinghepatectomy. Br J Surg 1997;84(9):1255—9.
[9] Stockmann M, Lock JF, Riecke B, et al. Prediction of postoper-ative outcome after hepatectomy with a new bedside test formaximal liver function capacity. Ann Surg 2009;250(1):119—25.
10] Ishizawa T, Fukushima N, Shibahara J, et al. Real-time identifi-cation of liver cancers by using indocyanine green fluorescentimaging. Cancer 2009;115(11):2491—504.
11] Guyer DR, Puliafito CA, Mones JM, et al. Digital indocyanine-green angiography in chorioretinal disorders. Ophthalmology1992;99(2):287—91.
12] Rubens FD, Ruel M, Fremes SE. A new and simplified methodfor coronary and graft imaging during CABG. Heart Surg Forum2002;5(2):141—4.
13] Raabe A, Nakaji P, Beck J, et al. Prospective evaluationof surgical microscope-integrated intraoperative near-infraredindocyanine green videoangiography during aneurysm surgery.J Neurosurg 2005;103(6):982—9.
14] Kitai T, Inomoto T, Miwa M, et al. Fluorescence navigation withindocyanine green for detecting sentinel lymph nodes in breastcancer. Breast Cancer 2005;12(3):211—5.
15] Tanaka R, Nakashima K, Fujimoto W. Sentinel lymph nodedetection in skin cancer using fluorescence navigation withindocyanine green. J Dermatol 2009;36(8):468—70.
16] Miyashiro I, Hiratsuka M, Kishi K, et al. Intraoperative diag-nosis using sentinel node biopsy with indocyanine green dye
in gastric cancer surgery: an institutional trial by experiencedsurgeons. Ann Surg Oncol 2012;20(2):542—6.17] Miyashiro I, Miyoshi N, Hiratsuka M, et al. Detection of sentinelnode in gastric cancer surgery by indocyanine green fluores-cence imaging: comparison with infrared imaging. Ann SurgOncol 2008;15(6):1640—3.
18] Noura S, Ohue M, Seki Y, et al. Feasibility of a lateral regionsentinel node biopsy of lower rectal cancer guided by indo-cyanine green using a near-infrared camera system. Ann SurgOncol 2009;17(1):144—51.
19] Makuuchi M, Kosuge T, Takayama T, et al. Surgery for small livercancers. Semin Surg Oncol 1993;9(4):298—304.
20] Seyama Y, Kubota K, Sano K, et al. Long-term outcome ofextended hemihepatectomy for hilar bile duct cancer with nomortality and high survival rate. Ann Surg 2003;238(1):73—83.
21] Faybik P, Krenn CG, Baker A, et al. Comparison of invasiveand noninvasive measurement of plasma disappearance rateof indocyanine green in patients undergoing liver transplan-tation: a prospective investigator-blinded study. Liver Transpl2004;10(8):1060—4.
22] Ishizawa T, Bandai Y, Hasegawa K, et al. Fluorescentcholangiography during laparoscopic cholecystectomy: indo-cyanine green or new fluorescent agents? World J Surg2010;34(10):2505—6.
23] Ishizawa T, Bandai Y, Ijichi M, et al. Fluorescent cholan-giography illuminating the biliary tree during laparoscopiccholecystectomy. Br J Surg 2010;97(9):1369—77.
[
[
[
[
[
[
[
C. Lim et al.
24] Ishizawa T, Tamura S, Masuda K, et al. Intraoperative fluores-cent cholangiography using indocyanine green: a biliary roadmap for safe surgery. J Am Coll Surg 2009;208(1):e1—4.
25] Gotoh K, Yamada T, Ishikawa O, et al. A novel image-guidedsurgery of hepatocellular carcinoma by indocyanine green flu-orescence imaging navigation. J Surg Oncol 2009;100(1):75—9.
26] Branch RA. Drugs as indicators of hepatic function. Hepatology1982;2(1):97—105.
27] Cherrick GR, Stein SW, Leevy CM, et al. Indocyanine green:observations on its physical properties, plasma decay, and hep-atic extraction. J Clin Invest 1960;39:592—600.
28] Landsman ML, Kwant G, Mook GA, et al. Light-absorbing proper-ties, stability, and spectral stabilization of indocyanine green.J Appl Physiol 1976;40(4):575—83.
29] Desmettre T, Devoisselle JM, Soulie-Begu S, et al. [Fluores-cence properties and metabolic features of indocyanine green(ICG)]. J Fr Ophtalmol 1999;22(9):1003—16.
30] Ishizawa T. Scientific basis and clinical application of ICGfluorescence imaging: hepatobiliary cancer. Open Surg Oncol2010;2.
31] Kokudo N, Ishizawa T. Fluorescence imaging in the treatment ofhepatobiliary and pancreatic diseases: techniques and futureperpectives. Front Gastrointest Res 2013;31:1—7 [Epub aheadof print].
32] Kawaguchi Y, Ishizawa T, Miyata Y, et al. Portal uptakefunction in veno-occlusive regions evaluated by real-timefluorescent imaging using indocyanine green. J Hepatol
2012;58(2):247—53.33] de Graaf W, Hausler S, Heger M, et al. Transporters involvedin the hepatic uptake of (99m)Tc-mebrofenin and indocyaninegreen. J Hepatol 2010;54(4):738—45.
34] van der Vorst JR, Schaafsma BE, Hutteman M, et al. Near-infrared fluorescence-guided resection of colorectal livermetastases. Cancer 2013 [Epub ahead of print].
35] Satou S, Ishizawa T, Masuda K, et al. Indocyanine green flu-orescent imaging for detecting extrahepatic metastasis ofhepatocellular carcinoma. J Gastroenterol 2012 [Epub aheadof print].
36] Yokoyama N, Otani T, Hashidate H, et al. Real-time detection ofhepatic micrometastases from pancreatic cancer by intraoper-ative fluorescence imaging: preliminary results of a prospectivestudy. Cancer 2011;118(11):2813—9.
37] Aoki T, Yasuda D, Shimizu Y, et al. Image-guided livermapping using fluorescence navigation system with indocya-nine green for anatomical hepatic resection. World J Surg2008;32(8):1763—7.
38] Ishizawa T, Zuker NB, Kokudo N, et al. Positive and negativestaining of hepatic segments by use of fluorescent imag-ing techniques during laparoscopic hepatectomy. Arch Surg2012;147(4):393—4.
39] Harada N, Ishizawa T, Muraoka A, et al. Fluorescence navi-gation hepatectomy by visualization of localized cholestasisfrom bile duct tumor infiltration. J Am Coll Surg 2010;210(6):e2—6.