Embed Size (px)
Citation preview
Infants admitted to neonatal units – interventions toimprove breastfeeding outcomes: a systematic review1990–2007
Rhona J. McInnes* and Julie Chambers†
*NMAHP Research Unit, and †Department of Psychology, University of Stirling, Stirling, UK
Abstract
This review aimed to identify interventions to promote breastfeeding or breast milk feeding forinfants admitted to the neonatal unit.
The medical electronic databases were searched for papers listed between 1990 and June 2005which had breastfeeding or breast milk as an outcome and which targeted infants who had beenadmitted to a neonatal unit, thus including the infant and/or their parents and/or neonatal unitstaff. Only papers culturally relevant to the UK were included resulting in studies from the USA,Canada, Europe, Australia and New Zealand. This search was updated in December 2007 toinclude publications up to this date.
We assessed 86 papers in full, of which 27 ultimately fulfilled the inclusion criteria.The studiesemployed a range of methods and targeted different aspects of breastfeeding in the neonatalunit.Variations in study type and outcomes meant that there was no clear message of what worksbest but skin-to-skin contact and additional postnatal support seemed to offer greater advantagefor the infant in terms of breastfeeding outcome. Galactogogues for mothers who are unable tomeet their infants’ needs may also help to increase milk supply. Evidence of an effect from otherpractices, such as cup-feeding on breastfeeding was limited; mainly because of a lack of researchbut also because few studies followed up the population beyond discharge from the unit.
Further research is required to explore the barriers to breastfeeding in this vulnerable popu-lation and to identify appropriate interventions to improve breastfeeding outcomes.
Keywords: breastfeeding, breast milk, premature infant, low-birthweight infant, systematicreview.
Corresponding: Dr Rhona J. McInnes, NMAHP Research Unit, Iris Murdoch Building, University of Stirling, Stirling FK9 4LA, UK.
E-mail: [email protected]
Review Article
235© 2008 The Authors. Journal compilation © 2008 Blackwell Publishing Ltd. Maternal and Child Nutrition (2008), 4, pp. 235–263

Introduction
Infants born prematurely and those of low-birthweight (LBW), who form the bulk of admissionsto neonatal units (NU), are at greater risk of pooreroutcomes than term or normal birthweight infantsand continue to be disadvantaged into adult life(Bhutta et al. 2002;Anderson et al. 2003; Klassen et al.
2004; Stein et al. 2006). These infants are also over-represented by those from less affluent backgrounds,thus increasing the likelihood of social and healthdisadvantage (Spencer et al. 1999; Moser et al. 2003).Health professionals caring for preterm/LBW infantsshould, therefore, aim to provide opportunities to givethese infants a better start in life. Breastfeeding isrecognized as the optimal method of feeding suchnewborns by providing protection from infection,enabling appropriate digestion and absorption ofnutrients, and optimizing neurological development(Schanler et al. 1999). However, infant feedingchoices continue to reflect socio-economic disadvan-tage with younger less affluent women tending to optto bottle-feed their babies (Bolling et al. 2007). In theNU, mothers are frequently encouraged to providebreast milk, which is often recognized as being crucialto their infant’s survival and well-being. The evidencethat many mothers will provide breast milk for theirinfant following admission to the NU (Jaeger et al.
1997; Miracle et al. 2004) suggests a unique opportu-nity to promote breastfeeding. However, there issome evidence that few infants are breastfed (i.e. fedat the breast rather than fed breast milk) at the timeof discharge from the unit (Buckley & Charles 2006).Furthermore mothers often feel excluded from theunit and from providing care for their infant (Lupton& Fenwick 2001; Flacking et al. 2006) and speakof distress at being separated from their babies(Hedberg Nyqvist et al. 1994). Mothers who expressbreast milk or breastfeed their infant speak of theimportant bond that this creates with their infant, theincreased opportunities for them to interact with theirinfant and the importance for them of this maternalrole (Lupton & Fenwick 2001; Miracle et al. 2004).Breastfeeding success is affected by the clinical well-being of the infant, the support the mother receivesand by the separation of the mother from her infant,
which in itself can act as a barrier to breastfeeding.There are a number of clinical practices and decisionswhich affect the ability of the mother to maintain hersupply of breast milk and to establish breastfeeding.Some practices have been identified as beneficial forhealthy, term infants (Renfrew et al. 2005), such asavoiding supplements and/or artificial teats. However,as preterm infants and infants admitted to the NUexperience different feeding challenges (such asdelayed oral feeding) and have different needs (suchas supplemental feeding and/or the need to be fedduring the mothers absence from the unit), it may notbe helpful to extrapolate those findings to this group.
Given the importance of breast milk for thepreterm/LBW or sick infant and the mother, it iscrucial that we identify the processes that can supportthe mother to provide breast milk for her infant andto enable breastfeeding. This systematic review aimsto identify interventions that affect breastfeedingand/or breast milk feeding in NU.
Methods
Search strategy
A search of the electronic databases CDSR, DARE,AMED, BNI, CINAHL, EMBASE, MEDLINE,PsycINFO and the reference lists of published articlesfor papers published between 1990 and 2005 was con-ducted. This search was updated in December 2007 toinclude any further publications since 2005 (Fig. 1).
Inclusion
Studies were included if they were experimental, pub-lished in English, had breastfeeding or breast milk asan outcome and targeted infants admitted to NU, thusincluding infants and/or their parents and/or NU staff.To identify papers, we searched for studies which tar-geted preterm (<37 weeks) or LBW infants (<2.5 kg)and for interventions within NU. In our originalsearch we included studies from developing coun-tries; however, these studies are not included in thispaper as it was unclear whether their outcomesreflected an impact of the intervention or were a con-sequence of poorly resourced care often provided to
R.J. McInnes and J. Chambers236
© 2008 The Authors. Journal compilation © 2008 Blackwell Publishing Ltd. Maternal and Child Nutrition (2008), 4, pp. 235–263
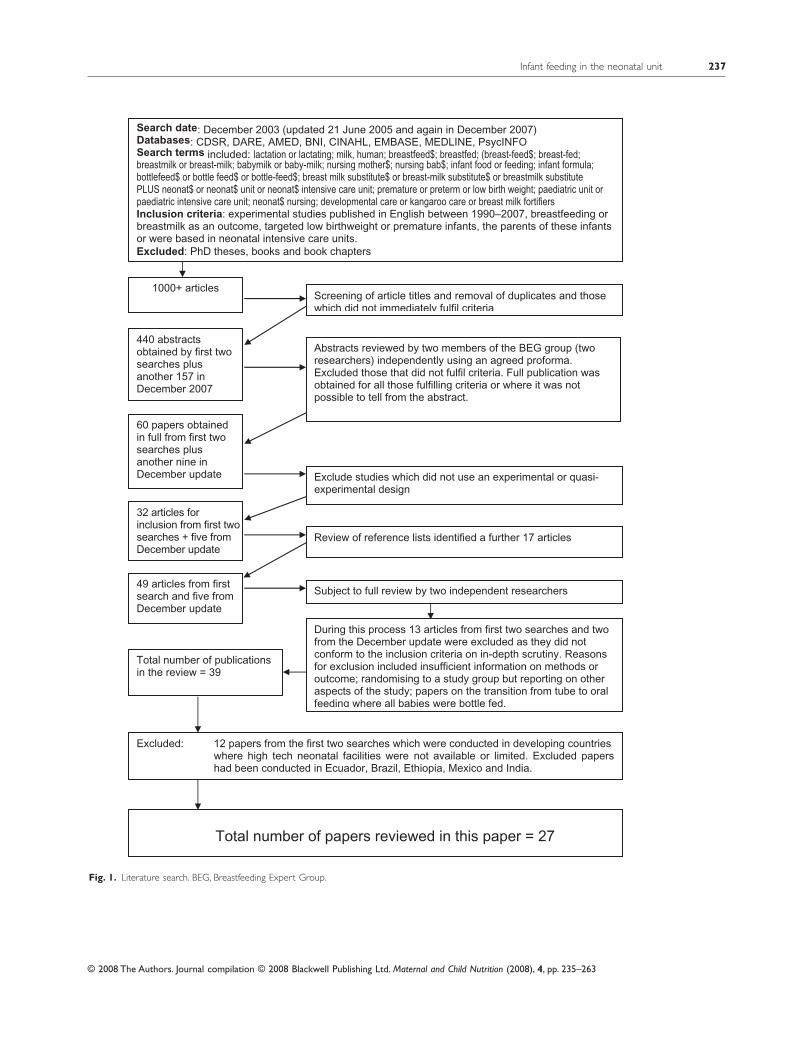
Search date: December 2003 (updated 21 June 2005 and again in December 2007)Databases: CDSR, DARE, AMED, BNI, CINAHL, EMBASE, MEDLINE, PsycINFO Search terms included: lactation or lactating; milk, human; breastfeed$; breastfed; (breast-feed$; breast-fed; breastmilk or breast-milk; babymilk or baby-milk; nursing mother$; nursing bab$; infant food or feeding; infant formula; bottlefeed$ or bottle feed$ or bottle-feed$; breast milk substitute$ or breast-milk substitute$ or breastmilk substitute PLUS neonat$ or neonat$ unit or neonat$ intensive care unit; premature or preterm or low birth weight; paediatric unit or paediatric intensive care unit; neonat$ nursing; developmental care or kangaroo care or breast milk fortifiers Inclusion criteria: experimental studies published in English between 1990–2007, breastfeeding or breastmilk as an outcome, targeted low birthweight or premature infants, the parents of these infantsor were based in neonatal intensive care units.
Excluded: PhD theses, books and book chapters
1000+ articles Screening of article titles and removal of duplicates and those which did not immediately fulfil criteria
440 abstracts obtained by first twosearches plus another 157 in December 2007
Abstracts reviewed by two members of the BEG group (two researchers) independently using an agreed proforma. Excluded those that did not fulfil criteria. Full publication was obtained for all those fulfilling criteria or where it was not possible to tell from the abstract.
60 papers obtained in full from first twosearches plus another nine in December update Exclude studies which did not use an experimental or quasi-
experimental design
32 articles for inclusion from first twosearches + five from December update
Review of reference lists identified a further 17 articles
49 articles from firstsearch and five from December update
Subject to full review by two independent researchers
During this process 13 articles from first two searches and two from the December update were excluded as they did not conform to the inclusion criteria on in-depth scrutiny. Reasons for exclusion included insufficient information on methods or outcome; randomising to a study group but reporting on other aspects of the study; papers on the transition from tube to oral feeding where all babies were bottle fed.
Total number of papers reviewed in this paper = 27
Total number of publications in the review = 39
Excluded: 12 papers from the first two searches which were conducted in developing countries where high tech neonatal facilities were not available or limited. Excluded papers had been conducted in Ecuador, Brazil, Ethiopia, Mexico and India.
Fig. 1. Literature search. BEG, Breastfeeding Expert Group.
Infant feeding in the neonatal unit 237
© 2008 The Authors. Journal compilation © 2008 Blackwell Publishing Ltd. Maternal and Child Nutrition (2008), 4, pp. 235–263

control group infants in these countries. Furthermorethe breastfeeding and parenting culture apparent inmany developing countries may affect the generaliz-ability of such studies to high technology NU in coun-tries with generally lower rates of breastfeeding. Afuller report, which includes papers (from 1990 to2005) from developing countries, is available from theauthors on request. Excluded papers are listed inAppendix 1.
Screening and data extraction
Abstracts were independently screened for inclusionby the reviewers (RM and JC) who also indepen-dently appraised each of the included papers using atool developed from critical appraisal publications(Centre for Reviews and Dissemination 2001; SIGN2004; Higgins et al. 2006) and from previous work bythe researchers. In the updated search for papers pub-lished between 2005 and 2007, papers were screenedby the first author (RM) and reviewed for agreementby the second (JC).
Quality assessment
All papers were scored according to methodologicalrigour (see Appendix 2 for more details on how thiswas calculated). The quality rating for each paper isgiven in column 1 of Table 3. Papers scoring �70%were defined as good, those scoring 50–69% as inter-mediate and those <50% as poor quality. Authorswere contacted to discuss ‘gaps’ in reporting that mayimpact upon the quality rating. Agreement betweenthe reviewers was high and minor disagreements wereresolved through discussion.
Evidence statements
Grouping papers with similar interventions enabledidentification of a number of statements about theevidence. The strength of these statements could beassessed using a process of comparative judgement(SIGN 2004).Assessments were based on the numberand quality of studies, consistency of evidencebetween studies and clinical usefulness of the findings.Statements were graded as: A: more than one good
quality study; B: one good quality study plus morethan one lesser quality; C: one good quality study plusone of lesser quality OR more than one lesser qualitystudy; and D: insufficient evidence to form a judge-ment. Evidence statements are given in the resultssection where possible. Because of the heterogeneityof the interventions conducting a meta-analysis wasnot thought appropriate.
Results
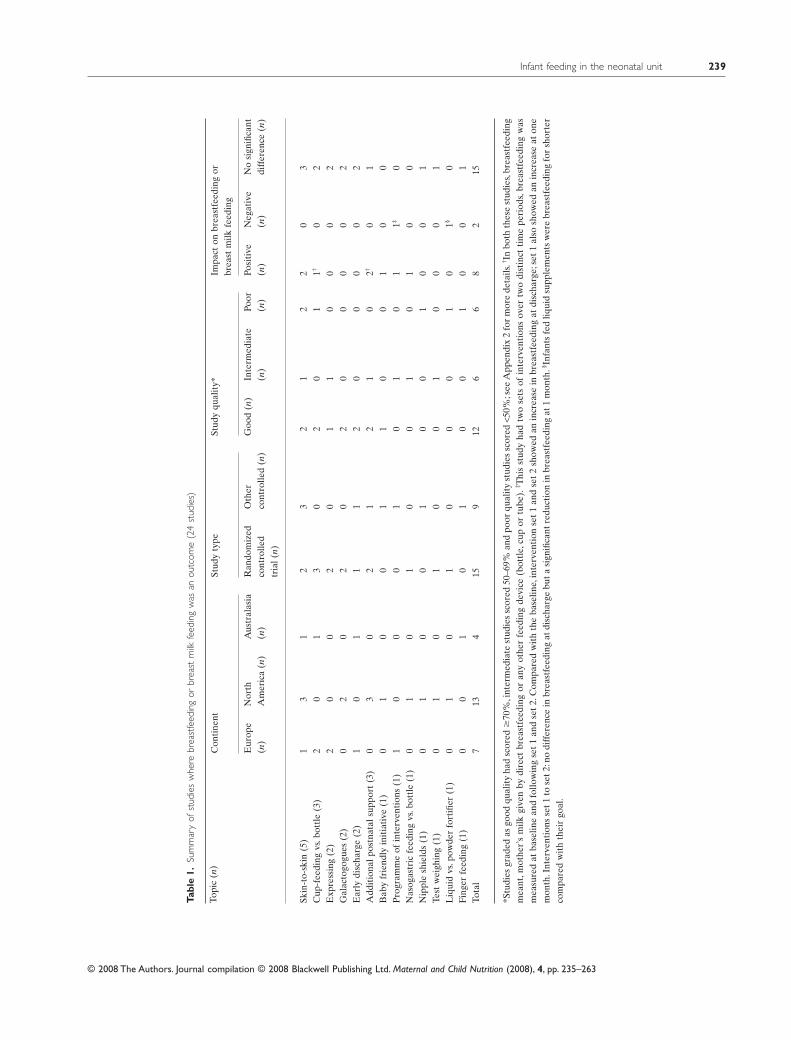
Overall 27 studies fullfiled the inclusion criteria.Twenty-four studies included breastfeeding as anoutcome, of which seven also included a measure-ment of milk volume/supply. In the remaining threestudies, breast milk volume/supply but not breast-feeding was an outcome. It should be noted that manyof the studies used ‘breastfeeding’ to indicate that thebaby was fed breast milk but often did not differen-tiate how this was given (i.e. breast, bottle or cup).Where information is available this has been noted inthe relevant tables. Twenty-one studies recruited pre-mature infants, three recruited LBW infants and threerecruited all infants admitted to the NU during thestudy period.
Study characteristics
Tables 1 and 2 sumarize the general characteristics ofthe 27 studies grouped by outcome measured, i.e.breastfeeding or breast milk volume. The studiesvaried widely in terms of the structure of the inter-vention and there were seven topics where only onepaper was identified; thus, a consistent impact onbreastfeeding/breast milk volume could not bedetermined. These were nasogastric tube feeding(Kliethermes et al. 1999), nipple shields (Meier et al.
2000), test weighing (Hurst et al. 2004), fortifiers(Fenton et al. 2000), finger feeding (Oddy & Glenn2003), the Baby Friendly Hospital Initiative (Mere-wood et al. 2003) and a series of interventions, aimingto promote breastfeeding (Dall’Oglio et al. 2007).Planned early discharge with good home support wasevaluated in two studies and was not shown to signifi-cantly affect breastfeeding outcomes, but furtherresearch is recommended particularly in countrieswith lower rates of breastfeeding (Örtenstrand et al.
R.J. McInnes and J. Chambers238
© 2008 The Authors. Journal compilation © 2008 Blackwell Publishing Ltd. Maternal and Child Nutrition (2008), 4, pp. 235–263
Tabl
e1.
Sum
mar
yof
stud
ies
whe
rebr
east
feed
ing
orbr
east
milk
feed
ing
was
anou
tcom
e(2
4st
udie
s)
Con
tine
ntSt
udy
type
Stud
yqu
alit
y*Im
pact
onbr
east
feed
ing
orbr
east
milk
feed
ing
Topi
c(n
)
Eur
ope
(n)
Nor
thA
mer
ica
(n)
Aus
tral
asia
(n)
Ran
dom
ized
cont
rolle
dtr
ial(
n)
Oth
erco
ntro
lled
(n)
Goo
d(n
)In
term
edia
te(n
)Po
or(n
)Po
siti
ve(n
)N
egat
ive
(n)
No
sign
ifica
ntdi
ffer
ence
(n)
Skin
-to-
skin
(5)
13
12
32
12
20
3C
up-f
eedi
ngvs
.bot
tle
(3)
20
13
02
01
1†0
2E
xpre
ssin
g(2
)2
00
20
11
00
02
Gal
acto
gogu
es(2
)0
20
20
20
00
02
Ear
lydi
scha
rge
(2)
10
11
12
00
00
2A
ddit
iona
lpos
tnat
alsu
ppor
t(3
)0
30
21
21
02†
01
Bab
yfr
iend
lyin
itia
tive
(1)
01
00
11
00
10
0P
rogr
amm
eof
inte
rven
tion
s(1
)1
00
01
01
01
1‡0
Nas
ogas
tric
feed
ing
vs.b
ottl
e(1
)0
10
10
01
01
00
Nip
ple
shie
lds
(1)
01
00
10
01
00
1Te
stw
eigh
ing
(1)
01
01
00
10
00
1L
iqui
dvs
.pow
der
fort
ifier
(1)
01
01
00
01
01§
0Fi
nger
feed
ing
(1)
00
10
10
01
00
1To
tal
713
415
912
66
82
15
*Stu
dies
grad
edas
good
qual
ity
had
scor
ed�
70%
,int
erm
edia
test
udie
ssc
ored
50–6
9%an
dpo
orqu
alit
yst
udie
ssc
ored
<50%
;see
App
endi
x2
for
mor
ede
tails
.† Inbo
thth
ese
stud
ies,
brea
stfe
edin
gm
eant
,mot
her’
sm
ilkgi
ven
bydi
rect
brea
stfe
edin
gor
any
othe
rfe
edin
gde
vice
(bot
tle,
cup
ortu
be).
‡ Thi
sst
udy
had
two
sets
ofin
terv
enti
ons
over
two
dist
inct
tim
epe
riod
s,br
east
feed
ing
was
mea
sure
dat
base
line
and
follo
win
gse
t1
and
set
2.C
ompa
red
wit
hth
eba
selin
e,in
terv
enti
onse
t1
and
set
2sh
owed
anin
crea
sein
brea
stfe
edin
gat
disc
harg
e;se
t1
also
show
edan
incr
ease
aton
em
onth
.Int
erve
ntio
nsse
t1to
set2
:no
diff
eren
cein
brea
stfe
edin
gat
disc
harg
ebu
tasi
gnifi
cant
redu
ctio
nin
brea
stfe
edin
gat
1m
onth
.§ Infa
nts
fed
liqui
dsu
pple
men
tsw
ere
brea
stfe
edin
gfo
rsh
orte
rco
mpa
red
wit
hth
eir
goal
.
Infant feeding in the neonatal unit 239
© 2008 The Authors. Journal compilation © 2008 Blackwell Publishing Ltd. Maternal and Child Nutrition (2008), 4, pp. 235–263

1999; Gunn et al. 2000). Two of the single-paperstudies showed a positive impact on breastfeedingoutcome, i.e. use of nasogastric tube-feeding in pref-erence to bottle-feeding for supplements for preterminfants (Kliethermes et al. 1999) and implementationof the Baby Friendly Hospital Initiative policies(Merewood et al. 2003). We have given more detailsof the single papers and the two on early discharge inAppendix 3 as this may highlight knowledge gaps forfuture research and will also enable updating of theevidence base. We have not included these papers inthis review as they do not offer any consistent evi-dence for effective practice.
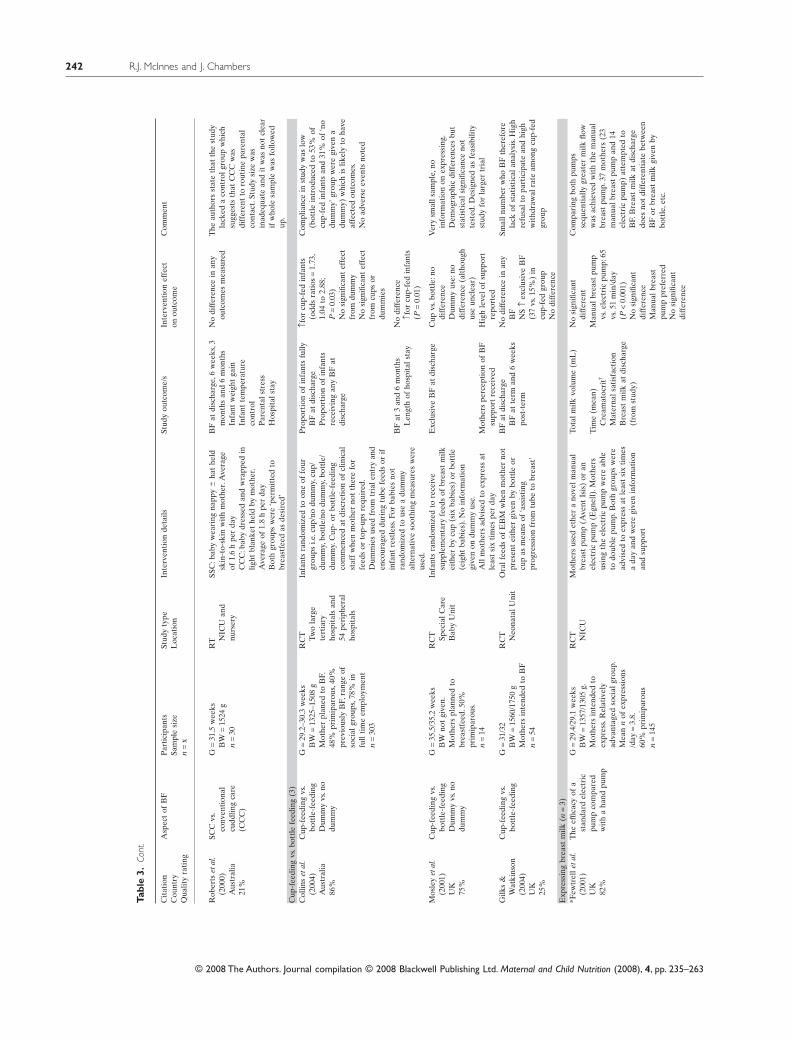
The five topics with the most accumulated evidencewere skin-to-skin contact (SSC) (five papers), cup-feeding (three papers), expressing breast milk (threepapers), galactogogues (four papers) and postnatalsupport (three papers). These 18 studies are reviewedhere and are summarized in Table 3.
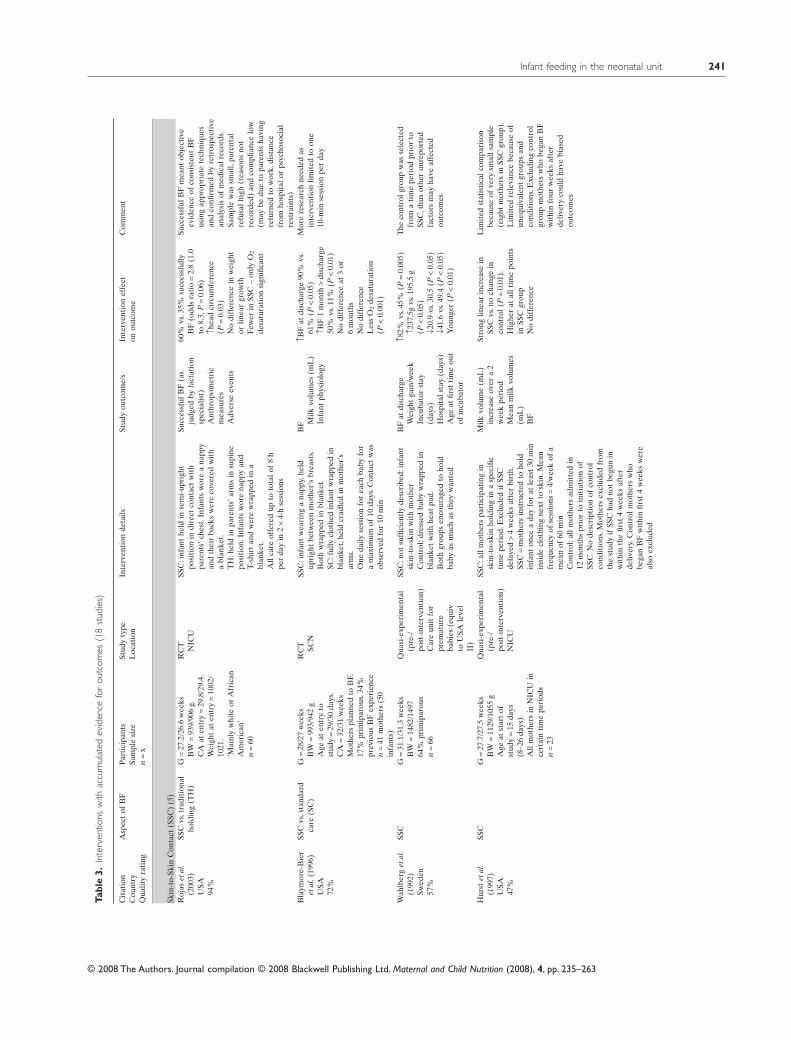
Skin-to-skin contact
In studies using SSC, the baby, wearing only a nappy(and a hat if required), is held vertically against themothers breasts (skin-to-skin) for varying periods oftime. In this review, contact times ranged from 10-minsession to 4-h sessions per day. This process is oftendescribed as Kangaroo Mother Care (KMC), which isa relatively standard intervention developed inColumbia in response to the lack of incubators (Rey& Martinez 1983). In KMC, the baby has free accessto the breast and will be nursed like this continuously(up to 24 h). Because contact times were so restrictedin the reviewed studies, none of them could be con-sidered to have used KMC as originally described;therefore, we have used the term skin-to-skin contact(SSC) to cover these interventions. In industrializedcountries, the terms KMC and SSC appear to be usedinterchangeably, but KMC as originally described iseither not well implemented or not understood. SSCas described in this section is different from ‘earlySSC’ which is encouraged in the first 24 h after birthand was the subject of a recent Cochrane Review(Moore et al. 2007).
Five studies evaluated SSC (Wahlberg et al. 1992;Blaymore Bier et al. 1996; Hurst et al. 1997; RobertsTa
ble
2.Su
mm
ary
ofst
udie
sw
here
brea
stm
ilkvo
lum
ew
asan
outc
ome
(10
stud
ies)
Con
tine
ntSt
udy
type
*Stu
dyqu
alit
yIm
pact
onbr
east
milk
volu
me
Topi
c(n
)
Eur
ope
(n)
Nor
thA
mer
ica
(n)
Aus
tral
asia
(n)
Ran
dom
ized
cont
rolle
dtr
ial(
n)
Oth
erco
ntro
lled
(n)
Goo
d(n
)In
ter-
med
iate
(n)
Poor
(n)
Posi
tive
(n)
Neg
ativ
e(n
)N
osi
gnifi
cant
diff
eren
ce(n
)
Skin
-to-
skin
cont
act
(2)
02
01
11
01
10
1E
xpre
ssin
g(3
)2
10
30
12
01
02
Gal
acto
gogu
es(4
)1
21
40
31
02
02
Add
itio
nalp
ostn
atal
supp
ort
(1)
01
01
00
10
00
1To
tal
36
19
15
41
40
6
*Stu
dies
grad
edas
good
qual
ity
had
scor
ed�
70%
,int
erm
edia
test
udie
ssc
ored
50–6
9%an
dpo
orqu
alit
yst
udie
ssc
ored
<50%
,see
App
endi
x2.
Stud
ies
incl
uded
inth
ista
ble
wer
eth
ose
that
mea
sure
dac
tual
brea
stm
ilkvo
lum
ew
hich
may
beth
eon
lyou
tcom
eor
may
bein
addi
tion
toot
her
feed
ing
outc
omes
such
asbr
east
feed
ing.
Bre
astm
ilkvo
lum
eco
uld
bem
easu
red
afte
rex
pres
sing
(gor
mL
)or
byte
stw
eigh
ing.
R.J. McInnes and J. Chambers240
© 2008 The Authors. Journal compilation © 2008 Blackwell Publishing Ltd. Maternal and Child Nutrition (2008), 4, pp. 235–263
Tabl
e3.
Inte
rven
tions
with
accu
mul
ated
evid
ence
for
outc
omes
(18
stud
ies)
Cit
atio
nC
ount
ryQ
ualit
yra
ting
Asp
ect
ofB
FP
arti
cipa
nts
Sam
ple
size
n=
x
Stud
yty
peL
ocat
ion
Inte
rven
tion
deta
ilsSt
udy
outc
ome/
sIn
terv
enti
onef
fect
onou
tcom
eC
omm
ent
Skin
-to-
Skin
Con
tact
(SSC
)(5
)R
ojas
etal
.(2
003)
USA
94%
SSC
vs.t
radi
tion
alho
ldin
g(T
H)
G=
27.2
/26.
6w
eeks
BW
=93
9/90
6g.
CA
aten
try
=29
.8/2
9.4.
Wei
ght
aten
try
=10
02/
1021
.’M
ainl
yw
hite
orA
fric
anA
mer
ican
’n
=60
RC
T NIC
USS
C:i
nfan
the
ldin
sem
i-up
righ
tpo
siti
onin
dire
ctco
ntac
tw
ith
pare
nts’
ches
t.In
fant
sw
ore
ana
ppy
and
thei
rba
cks
wer
eco
vere
dw
ith
abl
anke
t.T
H:h
eld
inpa
rent
s’ar
ms
insu
pine
posi
tion
.Inf
ants
wor
ena
ppy
and
T-sh
irt
and
wer
ew
rapp
edin
abl
anke
t.A
llca
reof
fere
dup
toto
talo
f8
hpe
rda
yin
2¥
4-h
sess
ions
Succ
essf
ulB
F(a
sju
dged
byla
ctat
ion
spec
ialis
t)A
nthr
opom
etri
cm
easu
res
Adv
erse
even
ts
60%
vs.3
5%su
cces
sful
lyB
F(o
dds
rati
o=
2.8
(1.0
to8.
3,P
=0.
06)
↑hea
dci
rcum
fere
nce
(P=
0.03
)N
odi
ffer
ence
inw
eigh
tor
linea
rgr
owth
Few
erin
SSC
–on
lyO
2
desa
tura
tion
sign
ifica
nt
Succ
essf
ulB
Fm
eant
obje
ctiv
eev
iden
ceof
cons
iste
ntB
Fus
ing
appr
opri
ate
tech
niqu
esan
dco
nfirm
edby
retr
ospe
ctiv
ean
alys
isof
med
ical
reco
rds.
Sam
ple
was
smal
l,pa
rent
alre
fusa
lhig
h(r
easo
nsno
tre
cord
ed)
and
com
plia
nce
low
(may
bedu
eto
pare
nts
havi
ngre
turn
edto
wor
k,di
stan
cefr
omho
spit
alor
psyc
hoso
cial
rest
rain
ts)
Bla
ymor
e-B
ier
etal
.(19
96)
USA
72%
SSC
vs.s
tand
ard
care
(SC
)G
=28
/27
wee
ksB
W=
993/
942
gA
geat
entr
yto
stud
y=
29/3
0da
ys.
CA
=32
/31
wee
ksM
othe
rspl
anne
dto
BF.
17%
prim
ipar
ous.
34%
prev
ious
BF
expe
rien
cen
=41
mot
hers
(50
infa
nts)
RC
T SCN
SSC
:inf
ant
wea
ring
ana
ppy,
held
upri
ght
betw
een
mot
her’
sbr
east
s.B
oth
wra
pped
inbl
anke
t.SC
:ful
lycl
othe
din
fant
wra
pped
inbl
anke
t,he
ldcr
adle
din
mot
her’
sar
ms.
One
daily
sess
ion
for
each
baby
for
am
axim
umof
10da
ys.C
onta
ctw
asob
serv
edfo
r10
min
BF M
ilkvo
lum
es(m
L)
Infa
ntph
ysio
logy
↑BF
atdi
scha
rge
90%
vs.
61%
(P<
0.05
)↑B
F1
mon
th>
disc
harg
e50
%vs
.11%
(P<
0.01
)N
odi
ffer
ence
at3
or6
mon
ths
No
diff
eren
ceL
ess
O2
desa
tura
tion
(P<
0.00
1)
Mor
ere
sear
chne
eded
asin
terv
enti
onlim
ited
toon
e10
-min
sess
ion
per
day
Wah
lber
get
al.
(199
2)Sw
eden
57%
SSC
G=
31.1
/31.
3w
eeks
BW
=14
82/1
497
64%
prim
ipar
ous
n=
66
Qua
si-e
xper
imen
tal
(pre
-/po
st-i
nter
vent
ion)
Car
eun
itfo
rpr
emat
ure
babi
es(e
quiv
toU
SAle
vel
II)
SSC
:not
suffi
cien
tly
desc
ribe
d:in
fant
skin
-to-
skin
wit
hm
othe
rC
ontr
ol:d
ress
edba
byw
rapp
edin
blan
ket
wit
hhe
atpa
d.B
oth
grou
psen
cour
aged
toho
ldba
byas
muc
has
they
wan
ted
BF
atdi
scha
rge
Wei
ght
gain
/wee
kIn
cuba
tor
stay
(day
s)H
ospi
tals
tay
(day
s)A
geat
first
tim
eou
tof
incu
bato
r
↑82%
vs.4
5%(P
=0.
005)
↑237
.5g
vs.1
95.5
g(P
<0.
05)
↓20.
9vs
.30.
5(P
<0.
05)
↓41.
6vs
.49.
4(P
<0.
05)
You
nger
(P<
0.01
)
The
cont
rolg
roup
was
sele
cted
from
ati
me
peri
odpr
ior
toSS
C,t
hus
othe
run
repo
rted
fact
ors
may
have
affe
cted
outc
omes
Hur
stet
al.
(199
7)U
SA47
%
SSC
G=
27.7
/27.
5w
eeks
BW
=11
29/1
055
gA
geat
star
tof
stud
y=
15da
ys(8
–26
days
)A
llm
othe
rsin
NIC
Uin
cert
ain
tim
epe
riod
sn
=23
Qua
si-e
xper
imen
tal
(pre
-/po
st-i
nter
vent
ion)
NIC
U
SSC
:all
mot
hers
part
icip
atin
gin
skin
-to-
skin
hold
ing
ina
spec
ific
tim
epe
riod
.Exc
lude
dif
SSC
dela
yed
>4
wee
ksaf
ter
birt
h.SS
C=
mot
hers
inst
ruct
edto
hold
infa
nton
cea
day
for
atle
ast
30m
inin
side
clot
hing
next
tosk
in.M
ean
freq
uenc
yof
sess
ions
=4/
wee
kof
am
ean
of60
min
Con
trol
:all
mot
hers
adm
itte
din
12m
onth
spr
ior
toin
itia
tion
ofSS
C.N
ode
scri
ptio
nof
cont
rol
cond
itio
ns.M
othe
rsex
clud
edfr
omth
est
udy
ifSS
Cha
dno
tbe
gun
inw
ithi
nth
efir
st4
wee
ksaf
ter
deliv
ery.
Con
trol
mot
hers
who
bega
nB
Fw
ithi
nfir
st4
wee
ksw
ere
also
excl
uded
Milk
volu
me
(mL
)in
crea
seov
era
2w
eek
peri
odM
ean
milk
volu
mes
(mL
)B
F
Stro
nglin
ear
incr
ease
inSS
Cvs
.no
chan
gein
cont
rol(
P=
0.01
).H
ighe
rat
allt
ime
poin
tsin
SSC
grou
pN
odi
ffer
ence
Lim
ited
stat
isti
calc
ompa
riso
nbe
caus
eof
very
smal
lsam
ple
(eig
htm
othe
rsin
SSC
grou
p).
Lim
ited
rele
vanc
ebe
caus
eof
uneq
uiva
lent
grou
psan
dco
ndit
ions
.Exc
ludi
ngco
ntro
lgr
oup
mot
hers
who
bega
nB
Fw
ithi
nfo
urw
eeks
afte
rde
liver
yco
uld
have
bias
edou
tcom
es
Infant feeding in the neonatal unit 241
© 2008 The Authors. Journal compilation © 2008 Blackwell Publishing Ltd. Maternal and Child Nutrition (2008), 4, pp. 235–263
Tabl
e3.
Cont
.
Cit
atio
nC
ount
ryQ
ualit
yra
ting
Asp
ect
ofB
FP
arti
cipa
nts
Sam
ple
size
n=
x
Stud
yty
peL
ocat
ion
Inte
rven
tion
deta
ilsSt
udy
outc
ome/
sIn
terv
enti
onef
fect
onou
tcom
eC
omm
ent
Rob
erts
etal
.(2
000)
Aus
tral
ia21
%
SCC
vs.
conv
enti
onal
cudd
ling
care
(CC
C)
G=
31.5
wee
ksB
W=
1524
gn
=30
RT N
ICU
and
nurs
ery
SSC
:bab
yw
eari
ngna
ppy
�ha
the
ldsk
in-t
o-sk
inw
ith
mot
her.
Ave
rage
of1.
6h
per
day
CC
C:b
aby
dres
sed
and
wra
pped
inlig
htbl
anke
the
ldby
mot
her.
Ave
rage
of1.
8h
per
day
Bot
hgr
oups
wer
e‘p
erm
itte
dto
brea
stfe
edas
desi
red’
BF
atdi
scha
rge,
6w
eeks
,3m
onth
san
d6
mon
ths
Infa
ntw
eigh
tga
inIn
fant
tem
pera
ture
cont
rol
Par
enta
lstr
ess
Hos
pita
lsta
y
No
diff
eren
cein
any
outc
omes
mea
sure
dT
heau
thor
sst
ate
that
the
stud
yla
cked
aco
ntro
lgro
upw
hich
sugg
ests
that
CC
Cw
asdi
ffer
ent
toro
utin
epa
rent
alco
ntac
t.St
udy
size
was
inad
equa
tean
dit
was
not
clea
rif
who
lesa
mpl
ew
asfo
llow
edup
.C
up-f
eedi
ngvs
.bot
tle
feed
ing
(3)
Col
lins
etal
.(2
004)
Aus
tral
ia86
%
Cup
-fee
ding
vs.
bott
le-f
eedi
ngD
umm
yvs
.no
dum
my
G=
29.2
–30.
3w
eeks
BW
=13
25–1
508
gM
othe
rpl
aned
toB
F.48
%pr
imip
arou
s,40
%pr
evio
usly
BF,
rang
eof
soci
algr
oups
,78%
infu
llti
me
empl
oym
ent
n=
303
RC
T Two
larg
ete
rtia
ryho
spit
als
and
54pe
riph
eral
hosp
ital
s
Infa
nts
rand
omiz
edto
one
offo
urgr
oups
i.e.c
up/n
odu
mm
y,cu
p/du
mm
y,bo
ttle
/no
dum
my,
bott
le/
dum
my.
Cup
-or
bott
le-f
eedi
ngco
mm
ence
dat
disc
reti
onof
clin
ical
staf
fw
hen
mot
her
not
ther
efo
rfe
eds
orto
p-up
sre
quir
ed.
Dum
mie
sus
edfr
omtr
iale
ntry
and
enco
urag
eddu
ring
tube
feed
sor
ifin
fant
rest
less
.For
babi
esno
tra
ndom
ized
tous
ea
dum
my
alte
rnat
ive
soot
hing
mea
sure
sw
ere
used
.
Pro
port
ion
ofin
fant
sfu
llyB
Fat
disc
harg
eP
ropo
rtio
nof
infa
nts
rece
ivin
gan
yB
Fat
disc
harg
e
↑for
cup-
fed
infa
nts
(odd
sra
tios
=1.
73,
1.04
to2.
88;
P=
0.03
)N
osi
gnifi
cant
effe
ctfr
omdu
mm
yN
osi
gnifi
cant
effe
ctfr
omcu
psor
dum
mie
s
Com
plia
nce
inst
udy
was
low
(bot
tle
intr
oduc
edto
53%
ofcu
p-fe
din
fant
san
d31
%of
‘no
dum
my’
grou
pw
ere
give
na
dum
my)
whi
chis
likel
yto
have
affe
cted
outc
omes
.N
oad
vers
eev
ents
note
d
BF
at3
and
6m
onth
sL
engt
hof
hosp
ital
stay
No
diff
eren
ce↑f
orcu
p-fe
din
fant
s(P
=0.
01)
Mos
ley
etal
.(2
001)
UK
75%
Cup
-fee
ding
vs.
bott
le-f
eedi
ngD
umm
yvs
.no
dum
my
G=
35.5
/35.
2w
eeks
BW
not
give
n.M
othe
rspl
anne
dto
brea
stfe
ed.5
0%pr
imip
arou
s.n
=14
RC
T Spec
ialC
are
Bab
yU
nit
Infa
nts
rand
omiz
edto
rece
ive
supp
lem
enta
ryfe
eds
ofbr
east
milk
eith
erby
cup
(six
babi
es)
orbo
ttle
(eig
htba
bies
).N
oin
form
atio
ngi
ven
ondu
mm
yus
e.A
llm
othe
rsad
vise
dto
expr
ess
atle
ast
six
tim
espe
rda
y
Exc
lusi
veB
Fat
disc
harg
eC
upvs
.bot
tle:
nodi
ffer
ence
Dum
my
use:
nodi
ffer
ence
(alt
houg
hus
eun
clea
r)
Ver
ysm
alls
ampl
e,no
info
rmat
ion
onex
pres
sing
.D
emog
raph
icdi
ffer
ence
sbu
tst
atis
tica
lsig
nific
ance
not
test
ed.D
esig
ned
asfe
asib
ility
stud
yfo
rla
rger
tria
lM
othe
rspe
rcep
tion
ofB
Fsu
ppor
tre
ceiv
edH
igh
leve
lof
supp
ort
repo
rted
Gilk
s&
Wat
kins
on(2
004)
UK
25%
Cup
-fee
ding
vs.
bott
le-f
eedi
ngG
=31
/32
BW
=15
60/1
750
gM
othe
rsin
tend
edto
BF
n=
54
RC
T Neo
nata
lUni
tO
ralf
eeds
ofE
BM
whe
nm
othe
rno
tpr
esen
tei
ther
give
nby
bott
leor
cup
asm
eans
of‘a
ssis
ting
prog
ress
ion
from
tube
tobr
east
’
BF
atdi
scha
rge
BF
atte
rman
d6
wee
kspo
st-t
erm
No
diff
eren
cein
any
BF
NS
↑ex
clus
ive
BF
(37
vs.1
5%)
incu
p-fe
dgr
oup
No
diff
eren
ce
Smal
lnum
ber
who
BF
ther
efor
ela
ckof
stat
isti
cala
naly
sis.
Hig
hre
fusa
lto
part
icip
ate
and
high
wit
hdra
wal
rate
amon
gcu
p-fe
dgr
oup
Exp
ress
ing
brea
stm
ilk(n
=3)
*Few
trel
leta
l.(2
001)
UK
82%
The
effic
acy
ofa
stan
dard
elec
tric
pum
pco
mpa
red
wit
ha
hand
pum
p
G=
29.4
/29.
1w
eeks
BW
=13
57/1
305
g.M
othe
rsin
tend
edto
expr
ess.
Rel
ativ
ely
adva
ntag
edso
cial
grou
p.M
ean
nof
expr
essi
ons
/day
=3.
8.60
%pr
imip
arou
sn
=14
5
RC
T NIC
UM
othe
rsus
edet
her
ano
velm
anua
lbr
east
pum
p(A
vent
Isis
)or
anel
ectr
icpu
mp
(Egn
ell)
.Mot
hers
usin
gth
eel
ectr
icpu
mp
wer
eab
leto
doub
lepu
mp.
Bot
hgr
oups
wer
ead
vise
dto
expr
ess
atle
ast
six
tim
esa
day
and
wer
egi
ven
info
rmat
ion
and
supp
ort
Tota
lmilk
volu
me
(mL
)N
osi
gnifi
cant
diff
eren
tC
ompa
ring
both
pum
psse
quen
tial
lygr
eate
rm
ilkflo
ww
asac
hiev
edw
ith
the
man
ual
brea
stpu
mp.
37m
othe
rs(2
3m
anua
lbre
ast
pum
pan
d14
elec
tric
pum
p)at
tem
pted
toB
F.B
reas
tm
ilkat
disc
harg
edo
esno
tdi
ffer
enti
ate
betw
een
BF
orbr
east
milk
give
nby
bott
le,e
tc.
Tim
e(m
ean)
Cre
amat
ocri
t†
Mat
erna
lsat
isfa
ctio
nB
reas
tm
ilkat
disc
harg
e(f
rom
stud
y)
Man
ualb
reas
tpu
mp
vs.e
lect
ric
pum
p:65
vs.5
1m
in/d
ay(P
<0.
001)
No
sign
ifica
ntdi
ffer
ence
Man
ualb
reas
tpu
mp
pref
erre
dN
osi
gnifi
cant
diff
eren
ce
R.J. McInnes and J. Chambers242
© 2008 The Authors. Journal compilation © 2008 Blackwell Publishing Ltd. Maternal and Child Nutrition (2008), 4, pp. 235–263
Tabl
e3.
Cont
.
Cit
atio
nC
ount
ryQ
ualit
yra
ting
Asp
ect
ofB
FP
arti
cipa
nts
Sam
ple
size
n=
x
Stud
yty
peL
ocat
ion
Inte
rven
tion
deta
ilsSt
udy
outc
ome/
sIn
terv
enti
onef
fect
onou
tcom
eC
omm
ent
Jone
set
al.
(200
1)U
K66
%
Sequ
enti
alvs
.si
mul
tane
ous
brea
stm
ilkex
pres
sing
wit
hor
wit
hout
mas
sage
G=
29.7
wee
ksB
W=
1535
gA
geat
star
tof
stud
y=
5–7
days
post
part
um.
33%
prim
ipar
ous.
n=
36
RT N
ICU
Mot
hers
allo
cate
dto
expr
ess
eith
ersi
mul
tane
ousl
yor
sequ
enti
ally
.All
part
icip
ants
also
rand
omiz
edto
2da
ysof
brea
stm
assa
gei.e
.day
s1–
2or
days
3–4.
Mot
hers
inst
ruct
edto
expr
ess
atle
ast
eigh
tti
mes
ada
yan
dex
pres
sun
tilm
ilkno
long
eren
tere
dth
eco
llect
ing
set.
The
Egn
ellA
med
aE
lect
ric
Elit
epu
mp
was
used
�si
last
icin
sert
s.St
udy
peri
od=
4da
ys.
Milk
volu
me
(g)
Fat
cont
ent
BF
dura
tion
(ter
m)
↑Milk
wei
ght
Sim
ulta
neou
s+
mas
sage
:12
5g
Sim
ulta
neou
s+
nom
assa
ge:8
8g
Sequ
enti
al+
mas
sage
:79
gSe
quen
tial
+no
mas
sage
:51
g(P
<0.
01)
Fat
conc
entr
atio
nsi
mila
rbu
tto
talf
atvo
lum
ew
assi
gnifi
cant
lyhi
gher
for
sim
ulta
neou
spu
mpi
ng(P
<0.
01).
Mas
sage
NS
No
diff
eren
ce
BF
:15
of17
sequ
enti
algr
oup
mot
hers
and
15of
16si
mul
tane
ous
grou
pm
othe
rsw
ere
fully
BF
orex
pres
sing
atte
rm.1
3%of
stud
ypo
pula
tion
eith
erfa
iled
tola
ctat
eor
supp
ress
edla
ctat
ion.
Wom
enfe
ltst
rong
lyth
atex
pres
sing
wit
hout
mas
sage
was
mor
edi
fficu
lt.
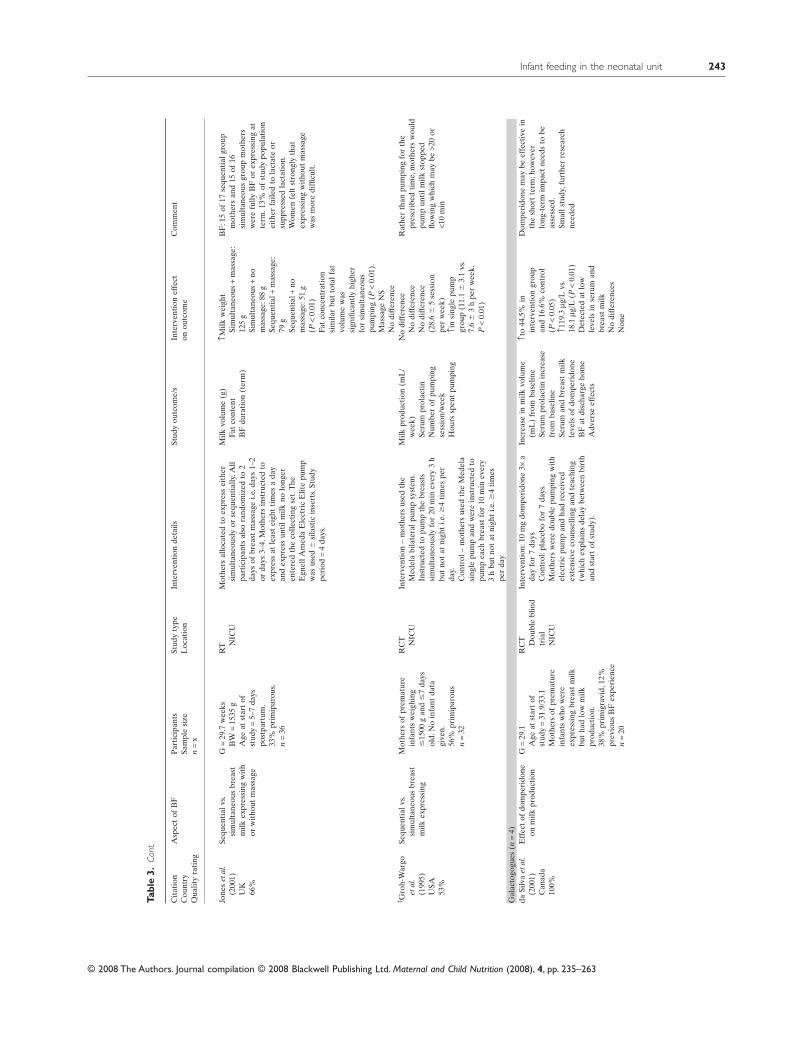
‡ Gro
h-W
argo
etal
.(1
995)
USA
53%
Sequ
enti
alvs
.si
mul
tane
ous
brea
stm
ilkex
pres
sing
Mot
hers
ofpr
emat
ure
infa
nts
wei
ghin
g�
1500
gan
d�
7da
ysol
d.N
oin
fant
data
give
n.56
%pr
imip
arou
sn
=32
RC
T NIC
UIn
terv
enti
on–
mot
hers
used
the
Med
ela
bila
tera
lpum
psy
stem
.In
stru
cted
topu
mp
the
brea
sts
sim
ulta
neou
sly
for
20m
inev
ery
3h
but
not
atni
ght
i.e.�
4ti
mes
per
day.
Con
trol
–m
othe
rsus
edth
eM
edel
asi
ngle
pum
pan
dw
ere
inst
ruct
edto
pum
pea
chbr
east
for
10m
inev
ery
3h
but
not
atni
ght
i.e.�
4ti
mes
per
day
Milk
prod
ucti
on(m
L/
wee
k)Se
rum
prol
acti
nN
umbe
rof
pum
ping
sess
ion/
wee
kH
ours
spen
tpu
mpi
ng
No
diff
eren
ceN
odi
ffer
ence
No
diff
eren
ce(2
8.6
�5
sess
ion
per
wee
k)↑i
nsi
ngle
pum
pgr
oup
(11.
1�
3.1
vs.
7.6
�3
hpe
rw
eek,
P<
0.01
)
Rat
her
than
pum
ping
for
the
pres
crib
edti
me,
mot
hers
wou
ldpu
mp
unti
lmilk
stop
ped
flow
ing
whi
chm
aybe
>20
or<1
0m
in
Gal
acto
gogu
es(n
=4)
daSi
lva
etal
.(2
001)
Can
ada
100%
Eff
ect
ofdo
mpe
rido
neon
milk
prod
ucti
onG
=29
.1A
geat
star
tof
stud
y=
31.9
/33.
1M
othe
rsof
prem
atur
ein
fant
sw
how
ere
expr
essi
ngbr
east
milk
but
had
low
milk
prod
ucti
on.
38%
prim
igra
vid,
12%
prev
ious
BF
expe
rien
cen
=20
RC
T Dou
ble
blin
dtr
ial
NIC
U
Inte
rven
tion
:10
mg
dom
peri
done
3¥a
day
for
7da
ysC
ontr
ol:p
lace
bofo
r7
days
.M
othe
rsw
ere
doub
lepu
mpi
ngw
ith
elec
tric
pum
pan
dha
dre
ceiv
edex
tens
ive
coun
selli
ngan
dte
achi
ng(w
hich
expl
ains
dela
ybe
twee
nbi
rth
and
star
tof
stud
y).
Incr
ease
inm
ilkvo
lum
e(m
L)
from
base
line
Seru
mpr
olac
tin
incr
ease
from
base
line
Seru
man
dbr
east
milk
leve
lsof
dom
peri
done
BF
atdi
scha
rge
hom
eA
dver
seef
fect
s
↑to
44.5
%in
inte
rven
tion
grou
pan
d16
.6%
cont
rol
(P<
0.05
)↑1
19.3
mg/L
vs.
18.1
mg/L
(P<
0.01
)D
etec
ted
atlo
wle
vels
inse
rum
and
brea
stm
ilkN
odi
ffer
ence
sN
one
Dom
peri
done
may
beef
fect
ive
inth
esh
ort
term
;how
ever
long
-ter
mim
pact
need
sto
beas
sess
ed.
Smal
lstu
dy,f
urth
erre
sear
chne
eded
Infant feeding in the neonatal unit 243
© 2008 The Authors. Journal compilation © 2008 Blackwell Publishing Ltd. Maternal and Child Nutrition (2008), 4, pp. 235–263
Tabl
e3.
Cont
.
Cit
atio
nC
ount
ryQ
ualit
yra
ting
Asp
ect
ofB
FP
arti
cipa
nts
Sam
ple
size
n=
x
Stud
yty
peL
ocat
ion
Inte
rven
tion
deta
ilsSt
udy
outc
ome/
sIn
terv
enti
onef
fect
onou
tcom
eC
omm
ent
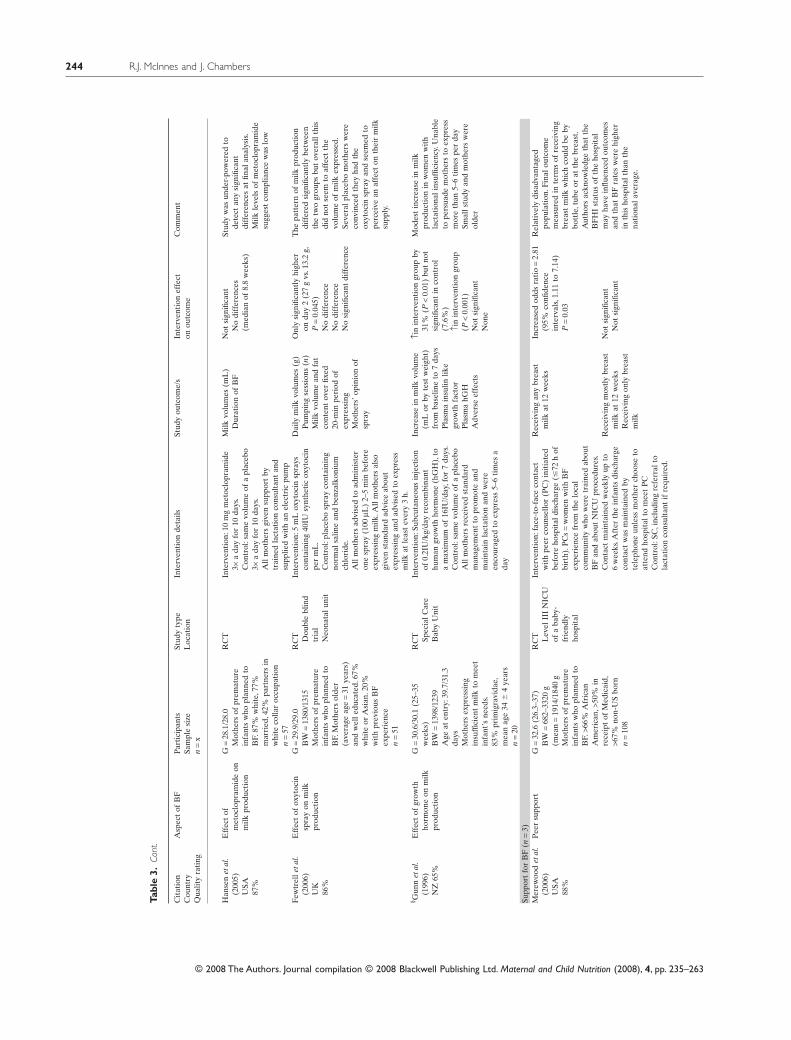
Han
sen
etal
.(2
005)
USA
87%
Eff
ect
ofm
etoc
lopr
amid
eon
milk
prod
ucti
on
G=
28.1
/28.
0M
othe
rsof
prem
atur
ein
fant
sw
hopl
anne
dto
BF.
87%
whi
te,7
7%m
arri
ed,4
2%pa
rtne
rsin
whi
teco
llar
occu
pati
onn
=57
RC
TIn
terv
enti
on:1
0m
gm
etoc
lopr
amid
e3¥
ada
yfo
r10
days
.C
ontr
ol:s
ame
volu
me
ofa
plac
ebo
3¥a
day
for
10da
ys.
All
mot
hers
give
nsu
ppor
tby
trai
ned
lact
atio
nco
nsul
tant
and
supp
lied
wit
han
elec
tric
pum
p
Milk
volu
mes
(mL
)D
urat
ion
ofB
FN
otsi
gnifi
cant
No
diff
eren
ces
(med
ian
of8.
8w
eeks
)
Stud
yw
asun
der-
pow
ered
tode
tect
any
sign
ifica
ntdi
ffer
ence
sat
final
anal
ysis
.M
ilkle
vels
ofm
etoc
lopr
amid
esu
gges
tco
mpl
ianc
ew
aslo
w
Few
trel
leta
l.(2
006)
UK
86%
Eff
ect
ofox
ytoc
insp
ray
onm
ilkpr
oduc
tion
G=
29.9
/29.
0B
W=
1380
/131
5M
othe
rsof
prem
atur
ein
fant
sw
hopl
anne
dto
BF.
Mot
hers
olde
r(a
vera
geag
e=
31ye
ars)
and
wel
ledu
cate
d.67
%w
hite
orA
sian
.20%
wit
hpr
evio
usB
Fex
peri
ence
n=
51
RC
T Dou
ble
blin
dtr
ial
Neo
nata
luni
t
Inte
rven
tion
:5m
Lox
ytoc
insp
rays
cont
aini
ng40
IUsy
nthe
tic
oxyt
ocin
per
mL
.C
ontr
ol:p
lace
bosp
ray
cont
aini
ngno
rmal
salin
ean
dbe
nzal
koni
umch
lori
de.
All
mot
hers
advi
sed
toad
min
iste
ron
esp
ray
(100
mL)
2–5
min
befo
reex
pres
sing
milk
.All
mot
hers
also
give
nst
anda
rdad
vice
abou
tex
pres
sing
and
advi
sed
toex
pres
sm
ilkat
leas
tev
ery
3h.
Dai
lym
ilkvo
lum
es(g
)P
umpi
ngse
ssio
ns(n
)M
ilkvo
lum
ean
dfa
tco
nten
tov
erfix
ed20
-min
peri
odof
expr
essi
ngM
othe
rs’o
pini
onof
spra
y
Onl
ysi
gnifi
cant
lyhi
gher
onda
y2
(27
gvs
.13.
2g,
P=
0.04
5)N
odi
ffer
ence
No
diff
eren
ceN
osi
gnifi
cant
diff
eren
ce
The
patt
ern
ofm
ilkpr
oduc
tion
diff
ered
sign
ifica
ntly
betw
een
the
two
grou
psbu
tov
eral
lthi
sdi
dno
tse
emto
affe
ctth
evo
lum
eof
milk
expr
esse
d.Se
vera
lpla
cebo
mot
hers
wer
eco
nvin
ced
they
had
the
oxyt
ocin
spra
yan
dse
emed
tope
rcei
vean
affe
cton
thei
rm
ilksu
pply
.
§ Gun
net
al.
(199
6)N
Z65
%
Eff
ect
ofgr
owth
horm
one
onm
ilkpr
oduc
tion
G=
30.6
/30.
1(2
5–35
wee
ks)
BW
=13
98/1
239
Age
aten
try:
39.7
/31.
3da
ysM
othe
rsex
pres
sing
insu
ffici
ent
milk
tom
eet
infa
nt’s
need
s.83
%pr
imig
ravi
dae,
mea
nag
e34
�4
year
sn
=20
RC
T Spec
ialC
are
Bab
yU
nit
Inte
rven
tion
:Sub
cuta
neou
sin
ject
ion
of0.
2IU
/kg/
day
reco
mbi
nant
hum
angr
owth
horm
one
(hG
H),
toa
max
imum
of16
IU/d
ay,f
or7
days
.C
ontr
ol:s
ame
volu
me
ofa
plac
ebo
All
mot
hers
rece
ived
stan
dard
man
agem
ent
topr
omot
ean
dm
aint
ain
lact
atio
nan
dw
ere
enco
urag
edto
expr
ess
5–6
tim
esa
day
Incr
ease
inm
ilkvo
lum
e(m
Lor
byte
stw
eigh
t)fr
omba
selin
eto
7da
ysP
lasm
ain
sulin
like
grow
thfa
ctor
Pla
sma
hGH
Adv
erse
effe
cts
↑in
inte
rven
tion
grou
pby
31%
(P<
0.01
)bu
tno
tsi
gnifi
cant
inco
ntro
l(7
.6%
)↑i
nin
terv
enti
ongr
oup
(P<
0.00
1)N
otsi
gnifi
cant
Non
e
Mod
est
incr
ease
inm
ilkpr
oduc
tion
inw
omen
wit
hla
ctat
iona
lins
uffic
ienc
y.U
nabl
eto
pers
uade
mot
hers
toex
pres
sm
ore
than
5–6
tim
espe
rda
ySm
alls
tudy
and
mot
hers
wer
eol
der
Supp
ort
for
BF
(n=
3)M
erew
ood
etal
.(2
006)
USA
88%
Pee
rsu
ppor
tG
=32
.6(2
6.3–
37)
BW
=68
2–33
20g
(mea
n=
1914
/184
0g
Mot
hers
ofpr
emat
ure
infa
nts
who
plan
ned
toB
F.>6
6%A
fric
anA
mer
ican
,>50
%in
rece
ipt
ofM
edic
aid,
>67%
non-
US
born
n=
108
RC
T Lev
elII
IN
ICU
ofa
baby
-fr
iend
lyho
spit
al
Inte
rven
tion
:fac
e-to
-fac
eco
ntac
tw
ith
peer
coun
sello
r(P
C)
init
iate
dbe
fore
hosp
ital
disc
harg
e(�
72h
ofbi
rth)
.PC
s=
wom
enw
ith
BF
expe
rien
cefr
omth
elo
cal
com
mun
ity
who
wer
etr
aine
dab
out
BF
and
abou
tN
ICU
proc
edur
es.
Con
tact
mai
ntai
ned
wee
kly
upto
6w
eeks
.Aft
erth
ein
fant
sdi
scha
rge
cont
act
was
mai
ntai
ned
byte
leph
one
unle
ssm
othe
rch
oose
toat
tend
hosp
ital
tom
eet
PC
Con
trol
:SC
,inc
ludi
ngre
ferr
alto
lact
atio
nco
nsul
tant
ifre
quir
ed.
Rec
eivi
ngan
ybr
east
milk
at12
wee
ksIn
crea
sed
odds
rati
o=
2.81
(95%
confi
denc
ein
terv
als,
1.11
to7.
14)
P=
0.03
Rel
ativ
ely
disa
dvan
tage
dpo
pula
tion
.Fin
alou
tcom
em
easu
red
inte
rms
ofre
ceiv
ing
brea
stm
ilkw
hich
coul
dbe
bybo
ttle
,tub
eor
atth
ebr
east
.A
utho
rsac
know
ledg
eth
atth
eB
FH
Ist
atus
ofth
eho
spit
alm
ayha
vein
fluen
ced
outc
omes
and
that
BF
rate
sw
ere
high
erin
this
hosp
ital
than
the
nati
onal
aver
age.
Rec
eivi
ngm
ostl
ybr
east
milk
at12
wee
ksR
ecei
ving
only
brea
stm
ilk
Not
sign
ifica
ntN
otsi
gnifi
cant
R.J. McInnes and J. Chambers244
© 2008 The Authors. Journal compilation © 2008 Blackwell Publishing Ltd. Maternal and Child Nutrition (2008), 4, pp. 235–263
Tabl
e3.
Cont
.
Cit
atio
nC
ount
ryQ
ualit
yra
ting
Asp
ect
ofB
FP
arti
cipa
nts
Sam
ple
size
n=
x
Stud
yty
peL
ocat
ion
Inte
rven
tion
deta
ilsSt
udy
outc
ome/
sIn
terv
enti
onef
fect
onou
tcom
eC
omm
ent
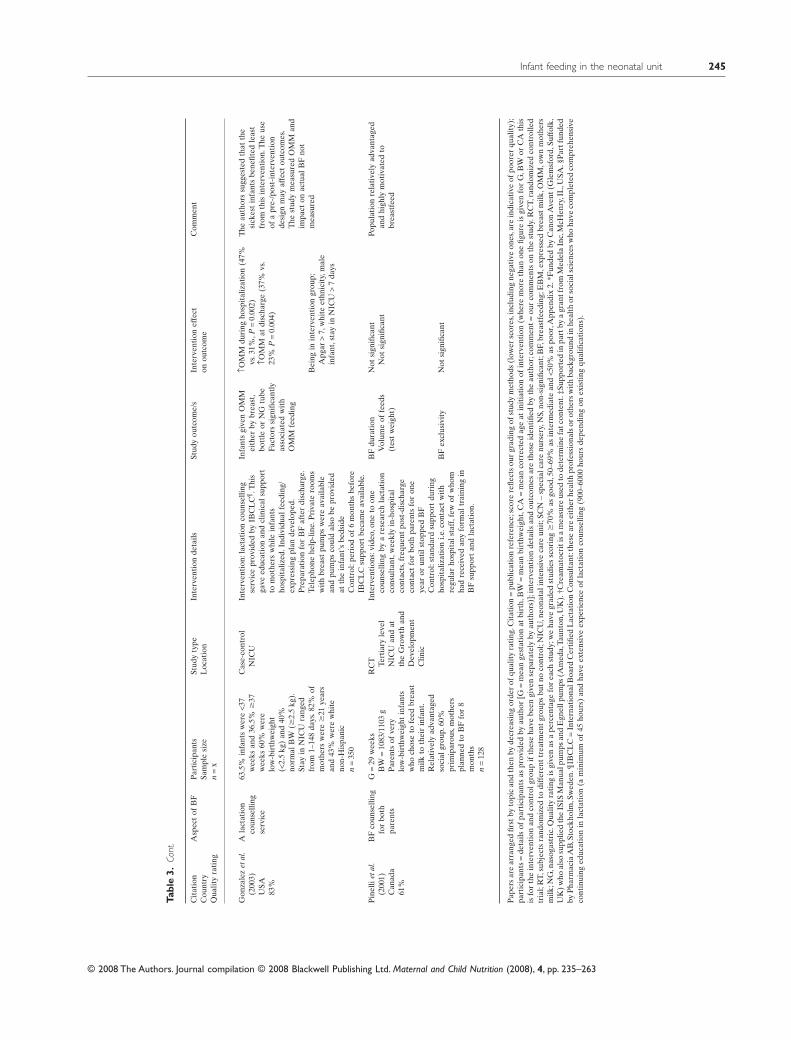
Gon
zale
zet
al.
(200
3)U
SA83
%
Ala
ctat
ion
coun
selli
ngse
rvic
e
63.5
%in
fant
sw
ere
<37
wee
ksan
d36
.5%
�37
wee
ks60
%w
ere
low
-bir
thw
eigh
t(<
2.5
kg)
and
40%
norm
alB
W(�
2.5
kg).
Stay
inN
ICU
rang
edfr
om1–
148
days
.82%
ofm
othe
rsw
ere
�21
year
san
d43
%w
ere
whi
teno
n-H
ispa
nic
n=
350
Cas
e-co
ntro
lN
ICU
Inte
rven
tion
:lac
tati
onco
unse
lling
serv
ice
prov
ided
byIB
CL
C¶.T
his
gave
educ
atio
nan
dcl
inic
alsu
ppor
tto
mot
hers
whi
lein
fant
sho
spit
aliz
ed.I
ndiv
idua
lfee
ding
/ex
pres
sing
plan
deve
lope
d.P
repa
rati
onfo
rB
Faf
ter
disc
harg
e.Te
leph
one
help
-lin
e.P
riva
tero
oms
wit
hbr
east
pum
psw
ere
avai
labl
ean
dpu
mps
coul
dal
sobe
prov
ided
atth
ein
fant
’sbe
dsid
eC
ontr
ol:p
erio
dof
6m
onth
sbe
fore
IBC
LC
supp
ort
beca
me
avai
labl
e.
Infa
nts
give
nO
MM
eith
erby
brea
st,
bott
leor
NG
tube
Fact
ors
sign
ifica
ntly
asso
ciat
edw
ith
OM
Mfe
edin
g
↑OM
Mdu
ring
hosp
ital
izat
ion
(47%
vs.3
1%,P
=0.
002)
↑OM
Mat
disc
harg
e(3
7%vs
.23
%P
=0.
004)
The
auth
ors
sugg
este
dth
atth
esi
ckes
tin
fant
sbe
nefit
edle
ast
from
this
inte
rven
tion
.The
use
ofa
pre-
/pos
t-in
terv
enti
onde
sign
may
affe
ctou
tcom
es.
The
stud
ym
easu
red
OM
Man
dim
pact
onac
tual
BF
not
mea
sure
dB
eing
inin
terv
enti
ongr
oup;
Apg
ar>
7,w
hite
ethn
icit
y,m
ale
infa
nt,s
tay
inN
ICU
>7
days
Pin
elli
etal
.(2
001)
Can
ada
61%
BF
coun
selli
ngfo
rbo
thpa
rent
s
G=
29w
eeks
BW
=10
83/1
103
gP
aren
tsof
very
low
-bir
thw
eigh
tin
fant
sw
hoch
ose
tofe
edbr
east
milk
toth
eir
infa
nt.
Rel
ativ
ely
adva
ntag
edso
cial
grou
p.60
%pr
imip
arou
s,m
othe
rspl
anne
dto
BF
for
8m
onth
sn
=12
8
RC
T Tert
iary
leve
lN
ICU
and
atth
eG
row
than
dD
evel
opm
ent
Clin
ic
Inte
rven
tion
s:vi
deo,
one
toon
eco
unse
lling
bya
rese
arch
lact
atio
nco
nsul
tant
,wee
kly
in-h
ospi
tal
cont
acts
,fre
quen
tpo
st-d
isch
arge
cont
act
for
both
pare
nts
for
one
year
orun
tils
topp
edB
FC
ontr
ol:s
tand
ard
supp
ort
duri
ngho
spit
aliz
atio
ni.e
.con
tact
wit
hre
gula
rho
spit
alst
aff,
few
ofw
hom
had
rece
ived
any
form
altr
aini
ngin
BF
supp
ort
and
lact
atio
n.
BF
dura
tion
Vol
ume
offe
eds
(tes
tw
eigh
t)
Not
sign
ifica
ntN
otsi
gnifi
cant
Popu
lati
onre
lati
vely
adva
ntag
edan
dhi
ghly
mot
ivat
edto
brea
stfe
ed
BF
excl
usiv
ity
Not
sign
ifica
nt
Pap
ers
are
arra
nged
first
byto
pic
and
then
byde
crea
sing
orde
rof
qual
ity
rati
ng.C
itat
ion
=pu
blic
atio
nre
fere
nce;
scor
ere
flect
sou
rgr
adin
gof
stud
ym
etho
ds(l
ower
scor
es,i
nclu
ding
nega
tive
ones
,are
indi
cati
veof
poor
erqu
alit
y);
part
icip
ants
=de
tails
ofpa
rtic
ipan
tsas
prov
ided
byau
thor
[G=
mea
nge
stat
ion
atbi
rth,
BW
=m
ean
birt
hwei
ght,
CA
=m
ean
corr
ecte
dag
eat
init
iati
onof
inte
rven
tion
(whe
rem
ore
than
one
figur
eis
give
nfo
rG
,BW
orC
Ath
isis
for
the
inte
rven
tion
and
cont
rolg
roup
ifth
ese
have
been
give
nse
para
tely
byau
thor
s)];
inte
rven
tion
deta
ilsan
dou
tcom
esar
eth
ose
iden
tifie
dby
the
auth
or;c
omm
ent=
our
com
men
tson
the
stud
y.R
CT,
rand
omiz
edco
ntro
lled
tria
l;R
T,su
bjec
tsra
ndom
ized
todi
ffer
ent
trea
tmen
tgr
oups
but
noco
ntro
l;N
ICU
,neo
nata
lint
ensi
veca
reun
it;S
CN
–sp
ecia
lcar
enu
rser
y,N
S,no
n-si
gnifi
cant
;BF,
brea
stfe
edin
g;E
BM
,exp
ress
edbr
east
milk
,OM
M,o
wn
mot
hers
milk
;NG
,nas
ogas
tric
.Qua
lity
rati
ngis
give
nas
ape
rcen
tage
for
each
stud
y;w
eha
vegr
aded
stud
ies
scor
ing
�70
%as
good
,50–
69%
asin
term
edia
tean
d<5
0%as
poor
,App
endi
x2.
*Fun
ded
byC
anon
Ave
nt(G
lem
sfor
d,Su
ffol
k,U
K)
who
also
supp
lied
the
ISIS
Man
ualp
umps
and
Egn
ellp
umps
(Am
eda,
Taun
ton,
UK
).†C
ream
atoc
riti
sa
mea
sure
used
tode
term
ine
fatc
onte
nt.‡
Supp
orte
din
part
bya
gran
tfro
mM
edel
aIn
c,M
cHen
ry,I
L,U
SA.§
Par
tfun
ded
byP
harm
acia
AB
,Sto
ckho
lm,S
wed
en.¶
IBC
LC
=In
tern
atio
nalB
oard
Cer
tifie
dL
acta
tion
Con
sult
ant:
thes
ear
eei
ther
heal
thpr
ofes
sion
als
orot
hers
wit
hba
ckgr
ound
inhe
alth
orso
cial
scie
nces
who
have
com
plet
edco
mpr
ehen
sive
cont
inui
nged
ucat
ion
inla
ctat
ion
(am
inim
umof
45ho
urs)
and
have
exte
nsiv
eex
peri
ence
ofla
ctat
ion
coun
selli
ng(9
00–6
000
hour
sde
pend
ing
onex
isti
ngqu
alifi
cati
ons)
.
Infant feeding in the neonatal unit 245
© 2008 The Authors. Journal compilation © 2008 Blackwell Publishing Ltd. Maternal and Child Nutrition (2008), 4, pp. 235–263

et al. 2000; Rojas et al. 2003). Three studies comparedSSC during specified parental visits with traditionalcontact (fully clothed and wrapped infant held supinein parents’ arms) (Wahlberg et al. 1992; BlaymoreBier et al. 1996; Rojas et al. 2003); one other studycompared SSC with control infants but did notdescribe the intervention (SSC) conditions (Hurstet al. 1997). In the remaining study (Roberts et al.
2000), a programme of SSC was implemented follow-ing a 12-month control period which was notdescribed.The gestational ages of the infants includedin the studies ranged from 26 to 31 weeks with birth-weight ranging from just over 900 g to over 1500 g.Allstudies comprised very small samples; thus, the totalnumber of infants included in this section is 220. Noadverse outcomes were reported. Box 1 summarizesthe evidence.
Two of the four studies measuring breastfeedingoutcomes showed statistically significant increases inbreastfeeding at discharge from the NU (Wahlberget al. 1992; Blaymore Bier et al. 1996). One of thesealso showed an increase at 1-month following dis-charge (Blaymore Bier et al. 1996). One further studyshowed a borderline-significant increase in successfulbreastfeeding (odds ratios = 1.0 to 8.3, P = 0.06) asjudged by a lactation specialist (Rojas et al. 2003).Thetwo other studies which measured breastfeedingshowed no difference between the SSC group and thecontrol. Both of these were poor quality studies and inone (Roberts et al. 2000) the average daily contactbetween mother and baby was longer for comparisonmothers than for SSC mothers. Breast milk volumewas measured in two studies with one (Blaymore Bieret al. 1996) showing no difference and the other
(Hurst et al. 1997) demonstrating a significantincrease in milk volumes over 2 weeks.
In two studies, SSC was associated with significantlyfewer episodes of oxygen desaturation (BlaymoreBier et al. 1996; Rojas et al. 2003). There was no con-sistent impact of SSC interventions on infant growthin terms of weight gain and/or head circumference.
Cup-feeding
Some preterm or sick infants are initially fed enterallyvia a naso-gastric (NG) or oro-gastric (OG) tube untilthey are mature or well enough to take oral feeds.During the transition from ‘tube’ feeds to breastfeed-ing, the infant may be given supplements (’top-ups’)by tube, bottle or cup in addition to breastfeeds. Indeciding how to give supplements, or to feed theinfant during the mother’s absence from the unit,health professionals must consider what methodwill best support the successful establishment ofbreastfeeding.
For mothers planning to breastfeed or who werebreastfeeding, supplements given by cups were com-pared with the use of bottles (Mosley et al. 2001;Collins et al. 2004; Gilks & Watkinson 2004). Cupswere used with babies born at 29–35 weeks, althoughage at use of cups was not given. One of the studies(Collins et al. 2004) was large (303 infants); however,the other two were both very small, giving a totalof 374 infants in this section. Box 2 summarizes theevidence.
The impact of cup-feeding on breastfeeding dura-tion was inconclusive. The largest and best qualitystudy (Collins et al. 2004) indicated higher breastfeed-ing rates in cup-fed infants at discharge; however,compliance with the study protocol was low withbottles introduced to over 50% of cup-fed infants.Thereasons for introducing bottles included mothers notliking or having problems with the cup (e.g. spillage,infant not satisfied) or staff refusing to cup-feed.Although this study was large, participants were
Box 1. Summary of evidence for use of SSCImpact on breastfeeding and breast milk volume:
• SSC was associated with increased breastfeeding at hospitaldischarge C
Other outcomes:
• SSC was associated with fewer episodes of oxygendesaturation A
Box 2. Summary of evidence for cup-feedingImpact on breastfeeding:The effects of cup use on breastfeeding/breast milk feeding D
R.J. McInnes and J. Chambers246
© 2008 The Authors. Journal compilation © 2008 Blackwell Publishing Ltd. Maternal and Child Nutrition (2008), 4, pp. 235–263

recruited over 3.5 years in two large tertiary hospitalsand included infants (59% of the sample) who weretransferred out to one of the 54 participating periph-eral hospitals where potential variations in practice,staff training and unit ethos may have affected theresults. The two other studies (Mosley et al. 2001;Gilks & Watkinson 2004) did not show any overalleffect on breastfeeding. In most studies, few mothersmade the transition to full breastfeeding; thus,numbers were small in later stages of data collection.One good quality study monitored adverse eventsand noted no significant physiological adverse eventsbut did find that cup-fed infants had increased hospi-tal stay (Collins et al. 2004).
Expressing breast milk
Three studies evaluated techniques and types of pumpfor expressing breast milk on a range of outcomes.Theinfants in this section were all premature (29–30 weeks, although one study did not supply demo-graphic data). Two of the studies were small; thus, thetotal number of infants in this section was 213. Twostudies (Groh-Wargo et al. 1995; Jones et al. 2001)compared sequential expressing with simultaneousexpressing using an electric pump, while the third(Fewtrell et al. 2001) compared a hand pump with anelectric pump. One study also compared the use ofbreast massage with not using massage (Jones et al.
2001). Breastfeeding was an outcome of one study(Jones et al. 2001) with no difference in numbers ofmothers’ breastfeeding or fully expressing at term.Milk volume was measured in all three studies withonly one, showing an increase in volume associatedwith simultaneous pumping and also with massage(Jones et al. 2001). Both studies comparing sequentialvs. simultaneous pumping had small numbers (n = 32and 36 respectively);however,one of these (Jones et al.
2001) was stopped early as interim data analysis clearlyidentified a significant effect in the simultaneouspumping group. Mothers also found that expressingwithout the use of breast massage was more difficult(Jones et al. 2001) (Box 3). A manual (hand) pumpcompared with an electric pump demonstrated nodifference in total volume of milk expressed, despitethe electric pump users being able to pump simulta-
neously (Fewtrell et al. 2001) and when compared insimilar conditions, i.e. breasts expressed sequentially,the manual pump users expressed greater volumes ofmilk and expressed a given volume more quickly. Fatcontent was not affected by pump type. Mothers alsoscored the manual pump more highly in terms of easeof use, amount of suction, comfort, pleasant to use and‘overall opinion’.
Galactogogues
Four small intervention studies were identified, two ofwhich measured both milk volume and breastfeeding(da Silva et al. 2001; Hansen et al. 2005), and twowhich measured milk volume only (Gunn et al. 1996;Fewtrell et al. 2006). The gestation at birth for infantsin this section ranged from 25 to 35 weeks althoughthe infants were older at the time of trial entry wasolder, e.g. 31.9/33.1 weeks (da Silva et al. 2001) or over31 days (Gunn et al. 1996). All the studies in thissection were very small with a total of 148 infants.Twostudies recruited women who had inadequate milksupply, (Gunn et al. 1996; da Silva et al. 2001) whilethe other two included all women who had given birthto a premature infant (Hansen et al. 2005; Fewtrellet al. 2006). One well-designed trial explored theshort-term use of domperidone for women with lowmilk production and showed increased milk volumesfrom baseline (da Silva et al. 2001). Growth hormone,used with mothers with poor milk supply, achieved amodest increase in milk volume from baseline to7 days (Gunn et al. 1996); however, neither metoclo-pramide nor oxytocin used with mothers of preterminfants had an effect on milk volume and/or breast-feeding duration (Hansen et al. 2005; Fewtrell et al.
2006). It is possible that the lack of effect from bothmetoclopramide and oxytocin was due to the fact that
Box 3. Summary of evidence for expressingImpact on milk volume:
• Simultaneous pumping was associated with increased breastmilk volume D• Breast massage was associated with increased breast milkvolume D
Infant feeding in the neonatal unit 247
© 2008 The Authors. Journal compilation © 2008 Blackwell Publishing Ltd. Maternal and Child Nutrition (2008), 4, pp. 235–263

both the studies were small; none of the women par-ticipating had identifiable milk inadequacy and thenumbers who could potentially have developed clini-cally significant milk inadequacy would have beensmaller still. Overall, none of the studies showedan increase in duration of breastfeeding; however,increasing milk volume may be a more important goalthan duration for mothers who are unable to achievesatisfactory volumes of breast milk (Box 4).
Postnatal support for breastfeeding
The interventions in this section varied considerablyfrom the provision of structured breastfeeding coun-selling programme delivered by a ‘research lactationconsultant’ (Pinelli et al. 2001); support and assistancefrom an International Board Certified Lactation Con-sultant (Gonzalez et al. 2003) and peer support deliv-ered by women with breastfeeding experience fromthe local community (Merewood et al. 2006). Thestudies also measured different outcomes includingbreastfeeding duration (Pinelli et al. 2001), breast-feeding at 12 weeks (Merewood et al. 2006), exclusiv-ity of breastfeeding (Pinelli et al. 2001; Merewoodet al. 2006), volume of breast milk feeds as measuredby test-weighing (Pinelli et al. 2001) and whether theinfant received breast milk feeds by any means(breast, bottle or tube) during hospitalisation and atdischarge (Gonzalez et al. 2003). They targeted differ-ent audiences with support being provided to bothparents (Pinelli et al. 2001) or to mothers only(Gonzalez et al. 2003; Merewood et al. 2006). Further-more, the mothers in two studies planned to breast-feed (Pinelli et al. 2001; Merewood et al. 2006)compared with the other study where feeding inten-tion was not solicited (Gonzalez et al. 2003). Thepopulation recruited by Pinelli et al. was relativelyadvantaged, highly motivated to breastfeed and had
good community support. The populations in theother two studies (Gonzalez et al. 2003; Merewoodet al. 2006) appeared more mixed and included a highpercentage of African American women who tend tohave lower rates of breastfeeding (Ryan et al. 1997).The age of the infants varied; 36% of infants in onetrial were born after 37 weeks (Gonzalez et al. 2003)while the gestational range for the other studies was26–37 weeks. The studies had larger numbers than inthe other sections involving a total of 586 infants.
Because of differences in the type of intervention,population recruited and outcomes measured anyconclusions in this section must be interpreted withcaution; however, in the two higher quality studies(Gonzalez et al. 2003; Merewood et al. 2006) addi-tional postnatal support was associated withincreased provision of breast milk feeding (Box 5).
Discussion and recommendations
Considering the value, i.e.placed on breast milk for thepreterm or LBW infant, there is very little well-designed research into practices which might supportor improve breastfeeding or breast milk feeding.Overall, the evidence for effective interventions waslimited with only SSC and additional postnatalsupport showing an effect on breastfeeding or breastmilk feeding at discharge [SSC and postnatal (PN)support], 1 month (SSC) or 12 weeks (PN support)(Box 6).
The majority of papers in this review targeted thepreterm or LBW infant. Our selection procedureaimed to identify interventions that evaluatedfeeding in other infant groups which might be admit-ted to the NU but we did not identify any such
Box 4. Summary of evidence for use of galactogoguesImpact on breastfeeding and breast milk volume:
• Domperidone or growth hormone may increase milkvolume in women who are expressing insufficient amounts C• Effect of galactagogues on breastfeeding D
Box 5. Summary of evidence for additional PN supportImpact on breast milk feeding:
• Postnatal support is associated with increased likelihood ofbreast milk feeding A*
*This grading should be considered with caution as although twogood quality studies showed an effect on breastfeeding the out-comes were measured at different times (discharge and12 weeks) and the interventions differed greatly (InternationalBoard Certified Lactation Consultant support vs. peer support)
R.J. McInnes and J. Chambers248
© 2008 The Authors. Journal compilation © 2008 Blackwell Publishing Ltd. Maternal and Child Nutrition (2008), 4, pp. 235–263

studies. Indeed, many of the studies included in thisreview excluded infants with congenital abnormali-ties or mothers who had a history of illicit drug use.Most of the studies reviewed in full (14) recruitedonly preterm infants. Three studies (Blaymore Bieret al. 1996; Hurst et al. 1997; Pinelli et al. 2001)recruited LBW infants but these infants alsoappeared to be preterm. One study (Gonzalez et al.
2003) included all infants in the unit during the studytime period of which over 60% were either LBW orpremature. This study, which showed a significantincrease in breast milk feeding during hospital stayand at discharge, did not identify an associationbetween gestational age and outcome by multivariateanalysis. Premature infants and infants, who are LBWbecause of foetal growth restriction, are likely torespond differently to feeding interventions but anydifference between these two groups was notadequately evaluated in the reviewed articles.
Skin-to-skin contact was associated with increasedbreastfeeding in two out of the four studies that mea-sured this outcome, and a tendency towards moresuccessful breastfeeding in a further study. However,there was no consistent effect on breastfeeding ratesfollowing discharge from the unit. A CochraneReview of the use of KMC for LBW infants (Conde-Agudelo et al. 2003) also noted some improvement inbreastfeeding but the authors expressed concernsabout study methods and could not recommendroutine use of KMC for LBW infants.The four papersin the Cochrane review were based in countries withnon-westernized healthcare systems and were noteligible for inclusion here; however, neither theCochrane Review nor the papers reviewed herereported any adverse effects. Following preterm birth,the separation of mother and infant can cause distress(Roller 2005) and despair for the mother (Nyström &Axelsson 2002) who wants to get to know her infantby seeing, holding and touching him (Roller 2005).Mothers have described KMC as calming and posi-tive, providing comfort for themselves and theirinfant (Roller 2005). In a qualitative study, the imple-mentation of KMC guidelines in Sweden was associ-ated with improved parental and infant well-being(Wallin et al. 2005). However, resistance to imple-menting KMC has been noted in both developed
(Wallin et al. 2005) and developing countries(Charpak & Ruiz-Paláez 2006) often because ofKMC being considered as substandard care, improperor unusual and resulting in extra work for staff. Lackof privacy and space in some units can also be prob-lematical and continuous KMC contact is not alwaysencouraged (Charpak & Ruiz-Paláez 2006). The evi-dence reviewed here and elsewhere suggests thatKMC or SSC is beneficial for both infant and motherand, given its recent systematic application in NU inSweden, can be used successfully in high-tech NU.From the research already completed, it is not clearwhich components of KMC/SSC (i.e. is it SSC per se,or length of contact or stimulation of the breast)affect breastfeeding and/or breast milk volume andfurther research is, therefore, needed.
Additional postnatal support was associated withan increased likelihood of the infant receiving somebreast milk by any means in two out of three studies.Postnatal support from a trained person (peer or pro-fessional) is associated with increased breastfeedingamong mothers of healthy term infants who wantsupport and/or who want to breastfeed, although out-comes differed according to population demographicsand/or intentions (Renfrew et al. 2005). Additionalsupport has received little attention for infants admit-ted to NU but it is possible that it might prove ben-eficial for a mother trying to feed her infant in thismore difficult environment. The studies in this reviewvaried considerably in their approach to providingsupport; thus, further research is needed to evaluatethe impact of postnatal support and to determine themost effective and acceptable method of delivery.Peer support is one such method of delivering addi-tional support and such initiatives have been increas-ing in number and popularity in the UK (Dykes 2005;Britten et al. 2006). The evidence for the effectivenessof peer support varies with some showing increases insome breastfeeding where offered proactively towomen who want to breastfeed (Renfrew et al. 2005)or increases in exclusive breastfeeding but not in anybreastfeeding (Britton et al. 2006). We identified onlyone eligible study using peer support in the NU(Merewood et al. 2006), which showed increasedbreast milk feeding by any means at 12 weeks follow-ing discharge. However, we identified one other study
Infant feeding in the neonatal unit 249
© 2008 The Authors. Journal compilation © 2008 Blackwell Publishing Ltd. Maternal and Child Nutrition (2008), 4, pp. 235–263

(Agrasada et al. 2005) based in the Philippines whichused peer support for term LBW infants, some ofwhom were admitted to the NU for 12–24 h. Breast-feeding support was provided by village women whohad had personal positive experience of breastfeedingand had received additional training. Compared withcomparison and a control group mothers, those whohad received peer breastfeeding counselling were sig-nificantly more like to be exclusively breastfeeding at2 weeks and 6 months, to continue to breastfeed andto be breastfeeding at 6 months. The peer supportstudy (Merewood et al. 2006) is one of only twostudies which demonstrated an impact on feedingbeyond discharge from the NU (the other being anincrease in breastfeeding at 1 month associated withSSC) (Blaymore Bier et al. 1996). Thus, furtherresearch is recommended to identify how best peersupport might be delivered in this environment in amanner that is both acceptable and accessible toparents and staff.
Neonatal staff frequently require to give supple-mental feeds to infants within the NU or to providefeeds when the mother is absent. These feeds shouldbe given in a manner which supports the transition tosuccessful breastfeeding, if this is the mothers wish,but the choice of method is limited by what is cur-rently available. The evidence that the skills used tofeed from a bottle differ from those used at the breast,has led to concerns about ‘nipple confusion’ where abreastfed infant may become confused if given abottle (Neifert et al. 1995). Therefore, there is nowa tendency to offer breast milk either by cup or tube(NG/OG). However, it is likely that the skills used forcup-feeding also differ from breastfeeding as sug-gested by Dowling and colleagues in a study of eightpreterm infants, in which the authors also had con-cerns about the small volumes of milk actuallyingested by cup-feeding (Dowling et al. 2002). ACochrane review of cupfeeding for infants unable tofully breastfeed (Flint et al. 2007) reviewed fourstudies and could not recommend cup-feeding overbottle-feeding as it conferred no significant benefitsand was associated a longer hospital stay. In ourreview, which included three of the four studies in theCochrane review, cup-feeding was associated withincreased breastfeeding at discharge in one of the
three studies reviewed but overall there was no accu-mulated evidence of an effect from cup-feeding. Thismay be due in part to few mothers making the tran-sition to breastfeeding; however, protocol violationsindicate a need for further exploration of the accept-ability of cup-feeding. While the evidence for nippleconfusion and cup-feeding is limited, there may be arisk in removing cups from this environment alto-gether as this may reinforce a culture of bottle-feeding. Neonatal staff have expressed concernsabout the psychological impact supplementing bybottle may have on the mother especially if she ishaving difficulty with breastfeeding (McInnes, unpub-lished) and while this may be the case, it has notreceived any attention in the research literature. Thepossibility that cup-feeding unnecessarily complicatesbreastfeeding should also be considered. The evi-dence from this review suggests that it is essential toexplore the use of cup-feeding in more detail from theperspective of both the mother and NU staff.
Dummy use is part of the ‘nipple confusion’ debate;however, none of the studies reviewed provideduseful evidence on the impact of dummies on breast-feeding in the NU because of study design, protocolviolations and very few mothers achieving full breast-feeding and/or maintaining breastfeeding once home(Mosley et al. 2001; Collins et al. 2004). Dummy usehas not been consistently associated with breastfeed-ing duration in healthy term babies (Renfrew et al.
2005); however, comparison between dummy use interm healthy infants and their use for preterm orLBW babies may be unhelpful. In NU, dummies areoften used to enable non-nutritive sucking (NNS),and a review of this practice (Pinelli & Symington2005) demonstrated that NNS was associated withsignificantly reduced hospital stay and improved tran-sition to bottle-feeding but did not include breast-feeding as an outcome. Further research is needed toidentify potential effects on breastfeeding of pretermNNS devices for ill or ventilated babies.
Given that expressing breast milk may be the mostimportant thing a mother can do for her pre-terminfant, there has been very little research into thisarea. Mothers speak of frustration and lack of supportwhen expressing (Jaeger et al. 1997) but those whosucceed experience a sense of satisfaction or reward
R.J. McInnes and J. Chambers250
© 2008 The Authors. Journal compilation © 2008 Blackwell Publishing Ltd. Maternal and Child Nutrition (2008), 4, pp. 235–263

(Miracle et al. 2004; Bernaix et al. 2006). In the studiesin this review, however, the authors reported thatalthough mothers appeared motivated to express,they rarely did so at the level recommended in thestudy protocol, which warrants further investigation.The frequency of expressing recommended by healthprofessionals in these studies varied from four toeight times per day. There also appears to be littleconsensus in the published literature regarding fre-quency of expressing, e.g. at least five times per day(Furman et al. 2002), at least eight times a day (Jones& Spencer 2007) or every 3 h (Meier et al. 2004).Possible variation in storage capacity of the breastsuggests that frequency of expressing may not beabsolute (Hartmann et al. 2003) and although 8–10times per day may be required to initiate lactationonce milk supply is established (a few days to2 weeks), frequency may then depend on breaststorage capacity (Spatz 2006). In addition, there wasno consensus on whether individual pumping sessionsshould be for a set period of time or until milk stopsflowing, or whether short-frequent pumping is prefer-able to longer less frequent sessions. Interventions,such as relaxation, visualization and back massage arethought to increase milk supply but were not identi-fied in this literature search. Neither were any studieswhich evaluated the use of hand expression a methodsometimes favoured by mothers especially whenexpressing very small amounts of milk in the earlydays.
The production of sufficient breast milk is impor-tant for all mothers expressing breast milk for theirinfant in the NU. However, the stressful environmentof the NU, separation of the mother from her infantand the need to stimulate and maintain lactationsolely by milk expression can cause milk supply prob-lems. For mothers who are unable to meet theirinfant’s needs, even small increases in expressed milkare important. For those mothers pharmacologicalintervention may be required and there is some evi-dence that short-term use of Domperidone orGrowth Hormone may be beneficial. However, long-term use of these or their impact on breastfeeding wasnot evaluated. Milk supply is affected by the fre-quency and efficiency of milk removal (Knight et al.
1998; Wilde et al. 1998). In the studies reviewed here
the advice on milk expression was at least every 3hours (Fewtrell et al. 2006) or 5–6 times a day, (Gunnet al. 1996) although two studies did not give anyinformation. A comparison of the effectiveness ofgalactogogues with other techniques to increase milksupply, such as increasing the frequency of expressingand/or additional support, is recommended.
Limitations
This review is restricted to experimental studies thatevaluated the impact of an intervention on breast-feeding or breast milk supply; thus, non-experimentalstudies and those which did not have breastfeeding orbreast milk as an outcome were not included. Quali-tative studies which explore the beliefs and experi-ences of parents and staff, were included in aqualitative synthesis published elsewhere (McInnes& Chambers 2006). This review was one of series ofreviews conducted concurrently and in order to beconsistent this dictated a number of limitations to oursearch strategy. Thus, we only included published lit-erature, the search commenced from 1990, and weincluded only papers published in English. When weupdated our search in December 2007, we did notidentify any non-English publications (from 1990 to2007) which fulfilled our inclusion criteria. The popu-
Box 6. Summary of results (consistent evidence of an effect).Interventions which may help the mother with expressing breast
milk:
• None identified
Interventions which may increase breast milk supply:
• Galactogogues where clinical insufficiency has beenestablished C
Interventions which may increase breast milk feeding:
• Additional postnatal support A• Skin-to-skin contact C
Interventions which may help establish successful breastfeeding:
• Skin-to-skin contact C
Infant feeding in the neonatal unit 251
© 2008 The Authors. Journal compilation © 2008 Blackwell Publishing Ltd. Maternal and Child Nutrition (2008), 4, pp. 235–263

lation group of mainly preterm infants may limit thegeneralizability to other infant groups in the NU.
The studies varied widely in intervention type,duration (of intervention and of data collection) andoutcomes (type of outcome and time of collection),and many studies did not examine potential con-founding variables, such as population demographics.All of this makes it difficult to draw any firm conclu-sions about effective practice. Of the papers reviewedin full the majority (13 out of 18) of the studies hadsmall sample sizes (<100), making the results less gen-eralizable. Finally, because of the specific nature ofsome of the interventions, the results may not be gen-eralizable to other populations or cultures.
Fourteen of the 18 papers in this review reported‘breastfeeding’ as an outcome although only twopapers (Pinelli et al. 2001; Collins et al. 2004) used aninternationally recognized definition for breastfeed-ing (Labbok & Krasovec 1990; World Health Organi-zation 1991). Only six studies differentiated betweenexclusive and partial breastfeeding; however, it wasalso not clear in many of the studies whether breast-feeding meant feeding at the breast or being fedbreast milk by other means. Future research requiresmore useful definitions of breastfeeding. Simply usingthe definitions applied to healthy term infants maynot be helpful for the preterm/sick infant as it isimportant to differentiate between whether an infantwas fed breast milk by bottle, tube or cup andat-breast breastfeeding. It is accepted that manypreterm/sick infants will receive some breast milkduring their hospitalization but it is also clear that fewgo on to breastfeed despite the known advantages ofbreastfeeding (at the breast) over breast milk feeding(by bottle, cup or tube) (Buckley & Charles 2006).
Conclusion
Current recommendations for increasing breastfeed-ing among term healthy infants suggest that effectiveinterventions should be identified and that each area(geographical and clinical) should consider the bestpackage of interventions for their population groupand that this should be informed by the views ofpractitioners and users (Dyson et al. 2006).The ad hoc
nature of the interventions identified in this review
suggests a need to work with mothers and staff toidentify the best approach to supporting mothers infeeding their infants. In the environment of the NU, itmay be necessary to consider feeding alongside theother aspects of parenting a small, sick or preterminfant. Given the physical and emotional benefits ofexpressing and breastfeeding for both the infant andthe mother, future interventions should work towardssupporting mothers to express milk where requiredand should identify ways to maximize milk produc-tion in terms of both volume and duration. Once theinfant is able to feed at the breast, effective strategiesneed to be developed to support the mother in thisimportant step to ensure effective breastfeeding andthe mother’s confidence in her role.
Conflicts of interest
None declared.
References
Agrasada G.V., Gustafsson J., Kylberg E. & Ewald U.(2005) Postnatal peer counselling on exclusive breast-feeding of low-birthweight infants: a randomized, con-trolled trial. Acta Paediatrica 94, 1109–1115.
Key messages
• Human milk is the optimal form of nutritionfor the preterm or LBW neonate and althoughmany mothers will express breast milk fortheir infant few go on to breastfeed.• Interventions to promote breastfeeding inthe NU appear to be task orientated and lackconsistency.• There are substantial gaps in our knowledgeof what aids breastfeeding in the NU and moreresearch is needed to identify what practicesare effective in supporting breastfeeding in theNU.• Currently skin-to-skin and/or postnatalsupport offers the most promise for increasingbreastfeeding for the preterm/LBW infant.
R.J. McInnes and J. Chambers252
© 2008 The Authors. Journal compilation © 2008 Blackwell Publishing Ltd. Maternal and Child Nutrition (2008), 4, pp. 235–263
Anderson P., Doyle L. & the Victoria Infant CollaborativeStudy Group. (2003) Neurobehavioural outcomes ofschool-age children born extremely low birthweight orvery preterm in the 1990s. Journal of the AmericanMedical Association 289, 3264–3272.
Bernaix L.W., Schmidt C.A., Jamerson P.A., Seiter L. &Smith J. (2006) The NICU experience of lactation andits relation to family management style. Maternal ChildNursing 31, 95–100.
Bhutta A.T., Cleves M.A., Casey P.H., Cradock M. &Anand K.J.S. (2002) Cognitive and behavioural outcomesof school-aged children who were born preterm. Journalof the American Medical Association 288, 728–737.
Blaymore Bier J-A, Ferguson A.E., Morales Y., LieblingJ.A., Archer D., Oh W. et al. (1996) Comparison of skin-to-skin contact with standard contact in low-birth-weightinfants who are breastfed. Archives of Pediatric andAdolescent Medicine 150, 1265–1269.
Bolling K., Grant C., Hamlyn B. & Thornton A. (2007)Infant Feeding Survey 2005, The Information Centre.Available at: http://www.ic.nhs.uk/webfiles/publications/breastfeed2005/InfantFeedingSurvey190506_PDF.pdf
Britten J., Hoddinott P. & McInnes R. (2006) Breastfeed-ing peer support: health service programmes in Scot-land. British Journal of Midwifery 14, 12–19.
Britton C., McCormick F.M., Renfrew M.J., Wade A. &King S.E. (2006) Support for breastfeeding mothers.Cochrane Database of Systematic Reviews, Issue 1. Art.No.: CD001141. doi: 10:1002/14651858.CD001141.pub3
Buckley K.M. & Charles G.E. (2006) Benefits and chal-lenges of transitioning preterm infants to at-breast feed-ings. International Breastfeeding Journal 1, Issue 13. doi:10.1186/1746-4358-1-13
Centre for Reviews and Dissemination (2001) UndertakingSystematic Reviews of Research on Effectiveness: CRD’sGuidance for Those Carrying out or CommissioningReviews. University of York. Available at: http://www.york.ac.uk/inst/crd/pdf/crd4_ph5.pd
Charpak N. & Ruiz-Paláez J.G. (2006) Resistance toimplementing Kangaroo Mother Care in developingcountries and proposed solutions. Acta Paediatrica 95,529–534.
Collins C.T., Ryan P., Crowther C.A., McPhee A.J.,Paterson S. & Hiller J.E. (2004) Effects of bottles,cups, and dummies on breastfeeding in preterm infants:a randomised controlled trial. British Medical Journal329, 193–198.
Conde-Agudelo A., Diaz-Rossello J.L. & Belizan J.M.(2003) Kangaroo mother care to reduce morbidity andmortality in low birthweight infants. Cochrane Databaseof Systematic Reviews, Issue 2. Art. No: CD002771. doi:10.1002/14651858.CD002771
Dall’Oglio I., Salvatori G., Bonci E., Nantini B.,D’Agostino G. & Dotta A. (2007) Breastfeeding promo-
tion in neonatal intensive care unit: impact of a newprogram toward a BFH1 for high-risk infants. Acta Pae-diatrica 96, 1626–1631.
Dowling D.A., Meier P.P., DiFore J.M., Blatz M. & MartinR.J. (2002) Cup-feeding for preterm infants: mechanicsand safety. Journal of Human Lactation 18, 13–20.
Dykes F. (2005) Government funded breastfeeding peersupport projects: implications for practice. Maternal andChild Nutrition 1, 21–31.
Dyson L., Renfrew M.J., McFadden A., McCormick F.,Herbert G. & Thomas J. (2006) Promotion of Breast-feeding Initiation and Duration. Evidence into practicebriefing, National Institute for Clinical Excellence, UK.Available at: http://www.nice.org.uk
Fenton T.R., Tough S.C. & Belik J. (2000) Breast milksupplementation for preterm infants: parental prefer-ences and post-discharge lactation duration. AmericanJournal of Perintology 17, 329–333.
Fewtrell M.S., Lucas P., Collier S., Singhal A., AhluwaliaJ.S. & Lucas A. (2001) Randomised trial comparing theefficacy of a novel manual breast pump with a standardelectric breast pump in mothers who delivered preterminfants. Pediatrics 107, 1291–1297.
Fewtrell M.S., Loh K.L., Blake A., Ridout D.A. &Hawdon J.M. (2006) Randomised double blindtrial of oxytocin nasal spray in mothers expressingbreast milk for preterm infants. Archives of Disease inChildhood Fetal Neonatal Edition 91, F169–F174.
Flacking R., Ewald U., Hedberg Nyqvist K. & Starrin B.(2006) Trustful bonds: a key to ‘becoming a mother’ andto reciprocal breastfeeding. Stories of mothers of verypreterm infants at a neonatal unit. Social Science andMedicine 62, 70–80.
Flint A., New K. & Davies M.W. (2007) Cup feedingversus other forms of supplemental enteral feeding fornewborn infants unable to fully breastfeed (Review).Cochrane Database of Systematic Reviews, Issue 2. Art.No. CD005092. doi: 10.1002/14651858
Furman L., Minich N. & Hack M. (2002) Correlates of lac-tation in mothers of very low birthweight infants. Pediat-rics 109, e57.
Gilks J. & Watkinson M. (2004) Improving breastfeedingrates in preterm babies: cup feeding versus bottlefeeding. Journal of Neonatal Nursing 10, 118–120.
Gonzalez K.A., Meinzen-Derr J., Burke B.L., Hibler A.J.,Kavinsky B., Hess S. et al. (2003) Evaluation of a lactationsupport service in a children’s hospital neonatal intensivecare unit. Journal of Human Lactation 19, 286–292.
Groh-Wargo S., Toth A., Mahoney K., Simonian S., WasserT. & Rose S. (1995) The utility of a bilateral breastpumping system for mothers of premature infants. Neo-natal Network 14, 31–36.
Gunn A.J., Gunn T.R., Rabone D.L., Breier B.H., BlumW.F. & Gluckman P.D. (1996) Growth hormone
Infant feeding in the neonatal unit 253
© 2008 The Authors. Journal compilation © 2008 Blackwell Publishing Ltd. Maternal and Child Nutrition (2008), 4, pp. 235–263

increases breast milk volumes in mothers of preterminfants. Pediatrics 98, 279–282.
Gunn T.R., Thompson J.M.D., Jackson H., McKnight S.,Buckthought G. & Gunn A.J. (2000) Does early hospitaldischarge with home support of families with preterminfants affect breastfeeding success? A randomised trial.Acta Paediatrica 89, 1358–1363.
Hansen W.H., McAndrew S., Harris K. & ZimmermanM.B. (2005) Metoclopramide effect on breastfeeding thepreterm infant: a randomised trial. Obstetrics and Gyne-cology 105, 383–389.
Hartmann P.E., Cregan M.D., Ramsay D.T., Simmer K. &Kent J.C. (2003) Physiology of lactation in pretermmothers: initiation and maintenance. Pediatric Annals 32,351–355.
Hedberg Nyqvist K., Sjoden P. & Ewald U. (1994) Mothersadvice about facilitating breastfeeding in a NeonatalIntensive Care Unit. Journal of Human Lactation 10,237–243.
Higgins J.P.T. & Green S. (eds) (2006) Cochrane Hand-book for Systematic Reviews of Interventions 4.2.6. JohnWiley & Sons: Chichester, UK. Available at: http://www.cochrane.org/resources/handbook/Handbook4.2.6Sep2006.pdf
Hurst N.M., Valentine C.J., Renfro L., Burns P. & Ferlic L.(1997) Skin-to-skin holding in the neonatal intensivecare unit influences maternal milk volume. Journal ofPerinatology 17, 213–217.
Hurst N.M., Meier P.P., Engstrom J.L. & Myatt A. (2004)Mothers performing in-home measurement of milkintake during breastfeeding of their preterm infants:maternal reactions and feeding outcomes. Journal ofHuman Lactation 20, 178–187.
Jaeger M.C., Lawson M. & Filteau S. (1997) The impact ofprematurity and neonatal illness on the decision tobreastfeed. Journal of Advanced Nursing 25, 729–737.
Jones E. & Spencer S.A. (2007) Optimising theprovision of human milk for preterm infants. Archives ofDisease in Childhood Fetal and Neonatal Edition 92,236–238.
Jones E., Dimmock P.W. & Spencer S.A. (2001) A ran-domised controlled trial to compare methods of milkexpression after preterm delivery. Archives of Disease inChildhood Fetal Neonatal Edition 85, F91–F95.
Klassen A.F., Lee S.K., Raina P., Chan H.W.P., Mathew D.& Brabyn D. (2004) Health status and health-related quality of life in a population-based sample ofneonatal intensive care graduates. Pediatrics 113, 594–600.
Kliethermes P.A., Cross M., Lanese M.G., Johnson K.M. &Simon S.D. (1999) Transitioning preterm infants withnasogastric tube supplementation: increased likelihoodof breastfeeding. Journal of Obstetrics, Gynecology andNeonatal Nursing 28, 264–273.
Knight C.H., Peaker M. & Wilde C.J. (1998) Local controlof mammary development and function. Reviews ofReproduction 3, 104–112.
Labbok M. & Krasovec K. (1990) Toward consistency inbreastfeeding definitions. Family Planning 21, 226–230.
Lupton D. & Fenwick J. (2001) They’ve forgotten that I’ma mum: constructing and practising motherhood inspecial care nurseries. Social Science and Medicine 53,1011–1021.
McInnes R.J. & Chambers J.A. (2006) A Synthesis ofQualitative Studies Exploring Psychosocial Factors Relat-ing to Infant Feeding and the Breastfeeding of Babies inNeonatal Units 1990–2005. NHS Health Scotland: Edin-burgh. Available at: http://www.healthscotland.com/documents/1701.aspx
Meier P.P., Brown L.P., Hurst N.M., Spatz D.L., EngstromJ.L., Borucki L.C. et al. (2000) Nipple shields for preterminfants: effect on milk transfer and duration of breast-feeding. Journal of Human Lactation 16, 106–114.
Meier P.P., Engstrom J.L., Mingolelli S.S., Miracle D.J. &Kiesling S. (2004) The Rush Mothers’ Milk Club: breast-feeding interventions for mothers with very-low-birth-weight infants. Journal of Obstetrics, Gynecology andNeonatal Nursing 33, 164–174.
Merewood A., Philipp B.L., Chawla N. & Cimo S. (2003)The Baby Friendly Hospital Initiative increases breast-feeding rates in a US neonatal intensive care unit.Journal of Human Lactation 19, 166–171.
Merewood A., Chamberlain L.B., Cook J.T., Philipp B.L.,Malone K. & Bauchner H. (2006) The effect of peercounselors on breastfeeding rates in the neonatal inten-sive care unit. Archives of Pediatric and AdolescentMedicine 160, 681–685.
Miracle D.J., Meier P.P. & Bennett P.A. (2004) Mothers’decisions to change from formula to mothers’ milk forVLBW babies. Journal of Gynecology and NeonatalNursing 33, 692–703.
Moore E.R., Anderson G.C. & Bergamn N. (2007). Earlyskin-to-skin contact for mothers and their healthynewborn infants. Cochrane Database of SystematicReviews, Issue 2. Art. No. CD003519. doi: 10.1002/14651858
Moser K., Power C. & Li L. (2003) Social inequalities inlow birthweight in England and Wales: trends and impli-cations for future population health. Journal of Epidemi-ology and Community Health 57, 687–691.
Mosley C., Whittle C. & Hicks C. (2001) A pilot study toassess the viabiity of a randomised controlled trial ofmethods of supplementary feeding of breast-fed pre-term babies. Midwifery 17, 150–157.
Neifert M., Lawrence R.A. & Seacat J. (1995) Nipple con-fusion: toward a formal definition. Journal of Pediatrics126, S125–S129.
R.J. McInnes and J. Chambers254
© 2008 The Authors. Journal compilation © 2008 Blackwell Publishing Ltd. Maternal and Child Nutrition (2008), 4, pp. 235–263
Nyström K. & Axelsson K. (2002) Mothers’ experienceof being separated from their newborn. Journal ofObstetrics, Gynecology and Neonatal Nursing 31, 275–282.
Oddy W.H. & Glenn K. (2003) Implementing the BabyFriendly Hospital Initiative: the role of finger feeding.Breastfeeding Review 11, 5–9.
Örtenstrand A., Waldenström U. & Winbladh B. (1999)Early discharge of preterm infants needing limitedspecial care, followed by domiciliary nursing care. ActaPaediatrica 88, 1024–1030.
Örtenstrand A., Winbladh B., Nordström G. & Walden-ström U. (2001) Early discharge of preterm infants fol-lowed by domiciliary nursing care: patients’ anxiety,assessment of infant health and breastfeeding. ActaPaediatrica 90, 1190–1195.
Pinelli J. & Symington A. (2005) Non-nutritive sucking forpromoting physiologic stability and nutrition in preterminfants. Cochrane Database of Systematic Reviews, Issue4. Art. No. CD001071. doi: 10.1002/14651858.CD001071.pub2.
Pinelli J., Atkinson S.A. & Saigal S. (2001) Randomisedtrial of breastfeeding support in very low birth weightinfants. Archives of Pediatric and Adolescent Medicine155, 548–553.
Renfrew M.J., Dyson L., Wallace L.M., D’Souza L.,McCormick F. & Spiby H. (2005) The Effectiveness ofPublic Health Interventions to Promote the Duration ofBreastfeeding: Systematic Reviews of the Evidence.National Institute for Health and Clinical Excellence:London. Available at: http://www.nice.org.uk.
Rey E. & Martinez H. (1983) Manejo Racional del ninoPremature. Universidad Nacional: Bogota.
Roberts K.L., Paynter C. & McEwan B. (2000) A compari-son of Kangaroo Mother Care and conventional cud-dling care. Neonatal Network 19, 31–35.
Rojas M.A., Kaplan M., Quevedo M., Sherwonit E., FosterL.B., Ehrenkranz R.A. et al. (2003) Somatic growth ofpreterm infants during skin-to-skin care versus tradi-tional holding: a randomised controlled trial. Develop-mental and Behavioural Pediatrics 24, 163–168.
Roller C.G. (2005) Getting to know you: mothers’ experi-ences of Kangaroo Care. Journal of Obstetrics, Gynecol-ogy and Neonatal Nursing 34, 210–217.
Ryan A.S. (1997) Resurgence of breastfeeding in theUnited States. Pediatrics 99, e12.
SIGN (2004) Scottish Intercollegiate Network Guidelines(SIGN), Scotland. Available at: http://www.sign.ac.uk/guidelines/fulltext/50/section6.html
Schanler R.J., Hurst N.M. & Lau C. (1999) The use ofhuman milk and breastfeeding in premature infants.Clinical Perinatology 25, 379–397.
Spatz D.L. (2006) State of the science: use of human milkand breast-feeding for vulnerable infants. Journal ofPerinatal and Neonatal Nursing 20, 51–55.
Spencer N., Bambang S., Logan S. & Leicester G. (1999)Socioeconomic status and birth weight: comparison ofan area-based measure with the Registrar General’ssocial class. Journal of Epidemiology and CommunityHealth 53, 495–498.
Stein R.E.K., Siegel M.J. & Bauman L.J. (2006) Are chil-dren of moderately low birth weight at increased risk forpoor health? A new look at an old question. Pediatrics118, 217–223.
Wahlberg V., Affonso D.D. & Persson B. (1992) A retro-spective, comparative study using the Kangaroo Methodas a complement to the standard incubator care. Euro-pean Journal of Public Health 2, 34–37.
Wallin L., Rudberg A. & Gunningberg L. (2005) Staffexperiences in implementing guidelines for KangarooMother Care – a qualitative study. International Journalof Nursing Studies 42, 61–73.
Wilde C.J., Addey C.C., Bryson J.M., Finch L.M., KnightC.H. & Peaker M. (1998) Autocrine regulation of milksecretion. Biochemical Society of Symposium 63, 81–90.
World Health Organization (1991) Indicators for AssessingBreast-Feeding Practice. WHO: Geneva.
da Silva O.P., Knoppert D.C., Angelini M.M. & Forret P.A.(2001) Effect of domperidone on milk production inmothers of premature newborns: a randomised, double-blind, placebo-controlled trial. Canadian Medical Asso-ciation Journal 164, 17–21.
Infant feeding in the neonatal unit 255
© 2008 The Authors. Journal compilation © 2008 Blackwell Publishing Ltd. Maternal and Child Nutrition (2008), 4, pp. 235–263
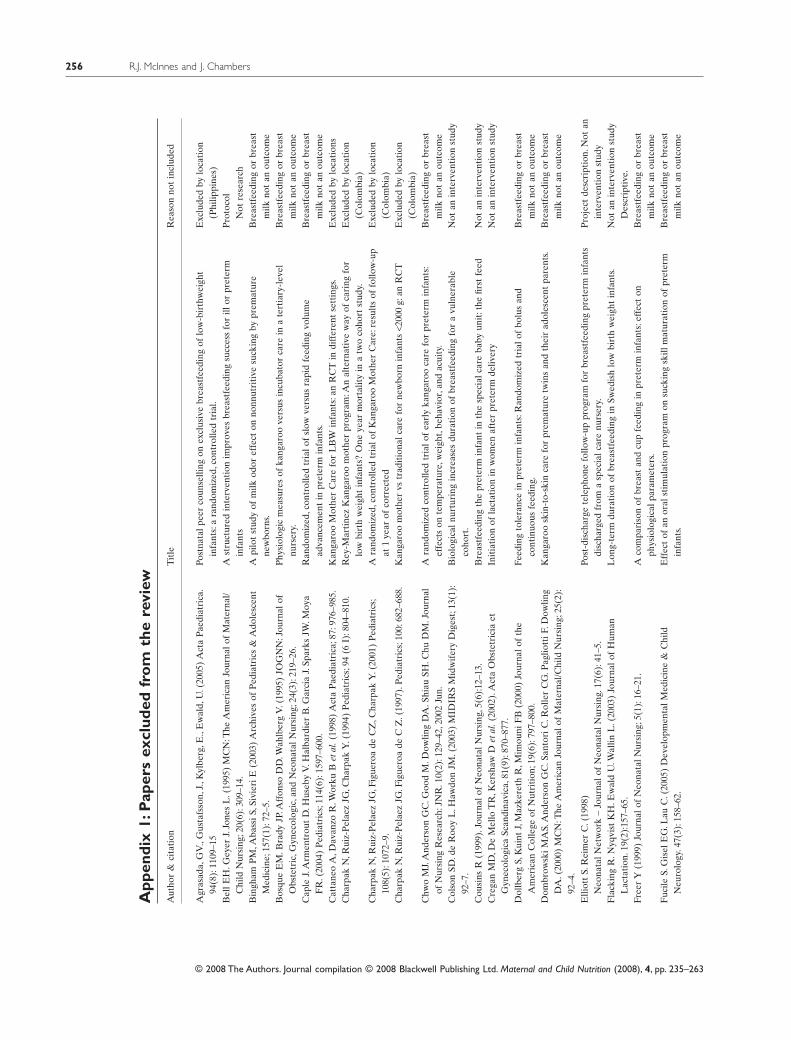
App
endi
x1:
Pap
ers
excl
uded
fro
mth
ere
view
Aut
hor
&ci
tati
onT
itle
Rea
son
not
incl
uded
Agr
asad
a,G
V.,
Gus
tafs
son,
J.,K
ylbe
rg,E
.,E
wal
d,U
.(20
05)
Act
aP
aedi
atri
ca.
94(8
):11
09–1
5Po
stna
talp
eer
coun
selli
ngon
excl
usiv
ebr
east
feed
ing
oflo
w-b
irth
wei
ght
infa
nts:
ara
ndom
ized
,con
trol
led
tria
l.E
xclu
ded
bylo
cati
on(P
hilip
pine
s)B
ellE
H.G
eyer
J.Jo
nes
L.(
1995
)M
CN
:The
Am
eric
anJo
urna
lof
Mat
erna
l/C
hild
Nur
sing
;20(
6):3
09–1
4.A
stru
ctur
edin
terv
enti
onim
prov
esbr
east
feed
ing
succ
ess
for
illor
pret
erm
infa
nts
Pro
toco
lN
otre
sear
chB
ingh
amP
M,A
bass
iS,S
ivie
riE
(200
3)A
rchi
ves
ofP
edia
tric
s&
Ado
lesc
ent
Med
icin
e;15
7(1)
:72–
5.A
pilo
tst
udy
ofm
ilkod
oref
fect
onno
nnut
riti
vesu
ckin
gby
prem
atur
ene
wbo
rns.
Bre
astf
eedi
ngor
brea
stm
ilkno
tan
outc
ome
Bos
que
EM
.Bra
dyJP
.Aff
onso
DD
.Wah
lber
gV
.(19
95)
JOG
NN
:Jou
rnal
ofO
bste
tric
,Gyn
ecol
ogic
,and
Neo
nata
lNur
sing
;24(
3):2
19–2
6.P
hysi
olog
icm
easu
res
ofka
ngar
oove
rsus
incu
bato
rca
rein
ate
rtia
ry-l
evel
nurs
ery.
Bre
astf
eedi
ngor
brea
stm
ilkno
tan
outc
ome
Cap
leJ.
Arm
entr
out
D.H
useb
yV
.Hal
bard
ier
B.G
arci
aJ.
Spar
ksJW
.Moy
aF
R.(
2004
)P
edia
tric
s;11
4(6)
:159
7–60
0.R
ando
miz
ed,c
ontr
olle
dtr
ialo
fsl
owve
rsus
rapi
dfe
edin
gvo
lum
ead
vanc
emen
tin
pret
erm
infa
nts.
Bre
astf
eedi
ngor
brea
stm
ilkno
tan
outc
ome
Cat
tane
oA
,Dav
anzo
R.W
orku
Bet
al.(
1998
)A
cta
Pae
diat
rica
;87:
976–
985.
Kan
garo
oM
othe
rC
are
for
LB
Win
fant
s:an
RC
Tin
diff
eren
tse
ttin
gs.
Exc
lude
dby
loca
tion
sC
harp
akN
,Rui
z-P
elae
zJG
,Cha
rpak
Y.(
1994
)P
edia
tric
s;94
(6I)
:804
–810
.R
ey-M
arti
nez
Kan
garo
om
othe
rpr
ogra
m:A
nal
tern
ativ
ew
ayof
cari
ngfo
rlo
wbi
rth
wei
ght
infa
nts?
One
year
mor
talit
yin
atw
oco
hort
stud
y.E
xclu
ded
bylo
cati
on(C
olom
bia)
Cha
rpak
N,R
uiz-
Pel
aez
JG,F
igue
roa
deC
Z,C
harp
akY
.(20
01)
Ped
iatr
ics;
108(
5):1
072–
9.A
rand
omiz
ed,c
ontr
olle
dtr
ialo
fK
anga
roo
Mot
her
Car
e:re
sult
sof
follo
w-u
pat
1ye
arof
corr
ecte
dE
xclu
ded
bylo
cati
on(C
olom
bia)
Cha
rpak
N,R
uiz-
Pel
aez
JG.F
igue
roa
deC
Z.(
1997
).P
edia
tric
s;10
0:68
2–68
8.K
anga
roo
mot
her
vstr
adit
iona
lcar
efo
rne
wbo
rnin
fant
s<2
000
g:an
RC
TE
xclu
ded
bylo
cati
on(C
olom
bia)
Chw
oM
J.A
nder
son
GC
.Goo
dM
.Dow
ling
DA
.Shi
auSH
.Chu
DM
.Jou
rnal
ofN
ursi
ngR
esea
rch:
JNR
.10(
2):1
29–4
2,20
02Ju
n.A
rand
omiz
edco
ntro
lled
tria
lof
earl
yka
ngar
ooca
refo
rpr
eter
min
fant
s:ef
fect
son
tem
pera
ture
,wei
ght,
beha
vior
,and
acui
ty.
Bre
astf
eedi
ngor
brea
stm
ilkno
tan
outc
ome
Col
son
SD.d
eR
ooy
L.H
awdo
nJM
.(20
03)
MID
IRS
Mid
wif
ery
Dig
est;
13(1
):92
–7.
Bio
logi
caln
urtu
ring
incr
ease
sdu
rati
onof
brea
stfe
edin
gfo
ra
vuln
erab
leco
hort
.N
otan
inte
rven
tion
stud
y
Cou
sins
R(1
999)
.Jou
rnal
ofN
eona
talN
ursi
ng,5
(6):
12–1
3.B
reas
tfee
ding
the
pret
erm
infa
ntin
the
spec
ialc
are
baby
unit
:the
first
feed
Not
anin
terv
enti
onst
udy
Cre
gan
MD
,De
Mel
loT
R,K
ersh
awD
etal
.(20
02).
Act
aO
bste
tric
iaet
Gyn
ecol
ogic
aSc
andi
navi
ca,8
1(9)
:870
–877
.In
itia
tion
ofla
ctat
ion
inw
omen
afte
rpr
eter
mde
liver
yN
otan
inte
rven
tion
stud
y
Dol
lber
gS,
Kui
ntJ,
Maz
kere
thR
,Mim
ouni
FB
(200
0)Jo
urna
lof
the
Am
eric
anC
olle
geof
Nut
riti
on;1
9(6)
:797
–800
.Fe
edin
gto
lera
nce
inpr
eter
min
fant
s:R
ando
miz
edtr
ialo
fbo
lus
and
cont
inuo
usfe
edin
g.B
reas
tfee
ding
orbr
east
milk
not
anou
tcom
eD
ombr
owsk
iMA
S.A
nder
son
GC
.San
tori
C.R
olle
rC
G.P
aglio
ttiF
.Dow
ling
DA
.(20
00)
MC
N:T
heA
mer
ican
Jour
nalo
fM
ater
nal/C
hild
Nur
sing
;25(
2):
92–4
.
Kan
garo
osk
in-t
o-sk
inca
refo
rpr
emat
ure
twin
san
dth
eir
adol
esce
ntpa
rent
s.B
reas
tfee
ding
orbr
east
milk
not
anou
tcom
e
Elli
ott
S.R
eim
erC
.(19
98)
Neo
nata
lNet
wor
k–
Jour
nalo
fN
eona
talN
ursi
ng.1
7(6)
:41–
5.Po
st-d
isch
arge
tele
phon
efo
llow
-up
prog
ram
for
brea
stfe
edin
gpr
eter
min
fant
sdi
scha
rged
from
asp
ecia
lcar
enu
rser
y.P
roje
ctde
scri
ptio
n.N
otan
inte
rven
tion
stud
yF
lack
ing
R.N
yqvi
stK
H.E
wal
dU
.Wal
linL
.(20
03)
Jour
nalo
fH
uman
Lac
tati
on.1
9(2)
:157
–65.
Lon
g-te
rmdu
rati
onof
brea
stfe
edin
gin
Swed
ish
low
birt
hw
eigh
tin
fant
s.N
otan
inte
rven
tion
stud
yD
escr
ipti
ve.
Free
rY
(199
9)Jo
urna
lof
Neo
nata
lNur
sing
;5(1
):16
–21.
Aco
mpa
riso
nof
brea
stan
dcu
pfe
edin
gin
pret
erm
infa
nts:
effe
cton
phys
iolo
gica
lpar
amet
ers.
Bre
astf
eedi
ngor
brea
stm
ilkno
tan
outc
ome
Fuc
ileS.
Gis
elE
G.L
auC
.(20
05)
Dev
elop
men
talM
edic
ine
&C
hild
Neu
rolo
gy.4
7(3)
:158
–62.
Eff
ect
ofan
oral
stim
ulat
ion
prog
ram
onsu
ckin
gsk
illm
atur
atio
nof
pret
erm
infa
nts.
Bre
astf
eedi
ngor
brea
stm
ilkno
tan
outc
ome
R.J. McInnes and J. Chambers256
© 2008 The Authors. Journal compilation © 2008 Blackwell Publishing Ltd. Maternal and Child Nutrition (2008), 4, pp. 235–263
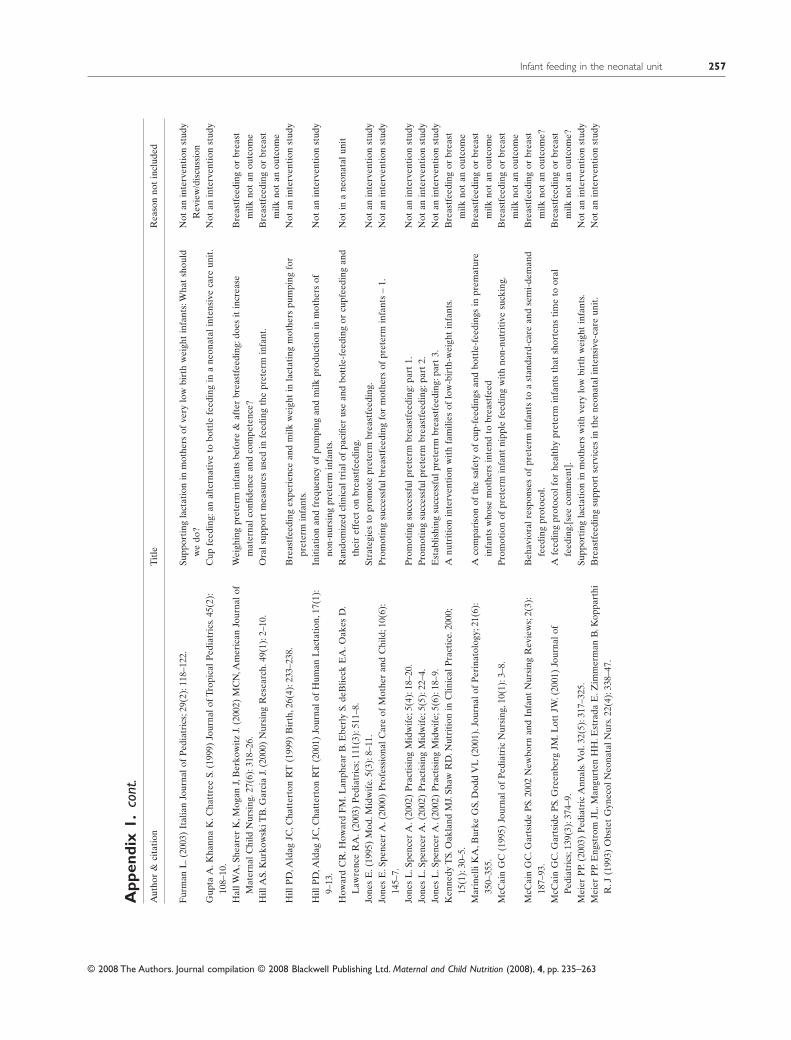
App
endi
x1.
cont
.A
utho
r&
cita
tion
Tit
leR
easo
nno
tin
clud
ed
Fur
man
L.(
2003
)It
alia
nJo
urna
lof
Ped
iatr
ics;
29(2
):11
8–12
2.Su
ppor
ting
lact
atio
nin
mot
hers
ofve
rylo
wbi
rth
wei
ght
infa
nts:
Wha
tsh
ould
we
do?
Not
anin
terv
enti
onst
udy
Rev
iew
/dis
cuss
ion
Gup
taA
.Kha
nna
K.C
hatt
ree
S.(1
999)
Jour
nalo
fTro
pica
lPed
iatr
ics.
45(2
):10
8–10
.C
upfe
edin
g:an
alte
rnat
ive
tobo
ttle
feed
ing
ina
neon
atal
inte
nsiv
eca
reun
it.
Not
anin
terv
enti
onst
udy
Hal
lWA
,She
arer
K,M
ogan
J,B
erko
wit
zJ.
(200
2)M
CN
,Am
eric
anJo
urna
lof
Mat
erna
lChi
ldN
ursi
ng.2
7(6)
:318
–26.
Wei
ghin
gpr
eter
min
fant
sbe
fore
&af
ter
brea
stfe
edin
g:do
esit
incr
ease
mat
erna
lcon
fiden
cean
dco
mpe
tenc
e?B
reas
tfee
ding
orbr
east
milk
not
anou
tcom
eH
illA
S.K
urko
wsk
iTB
.Gar
cia
J.(2
000)
Nur
sing
Res
earc
h.49
(1):
2–10
.O
rals
uppo
rtm
easu
res
used
infe
edin
gth
epr
eter
min
fant
.B
reas
tfee
ding
orbr
east
milk
not
anou
tcom
eH
illP
D,A
ldag
JC,C
hatt
erto
nR
T(1
999)
Bir
th,2
6(4)
:233
–238
.B
reas
tfee
ding
expe
rien
cean
dm
ilkw
eigh
tin
lact
atin
gm
othe
rspu
mpi
ngfo
rpr
eter
min
fant
s.N
otan
inte
rven
tion
stud
y
Hill
PD
,Ald
agJC
,Cha
tter
ton
RT
(200
1)Jo
urna
lof
Hum
anL
acta
tion
,17(
1):
9–13
.In
itia
tion
and
freq
uenc
yof
pum
ping
and
milk
prod
ucti
onin
mot
hers
ofno
n-nu
rsin
gpr
eter
min
fant
s.N
otan
inte
rven
tion
stud
y
How
ard
CR
.How
ard
FM
.Lan
phea
rB
.Ebe
rly
S.de
Blie
ckE
A.O
akes
D.
Law
renc
eR
A.(
2003
)P
edia
tric
s;11
1(3)
:511
–8.
Ran
dom
ized
clin
ical
tria
lof
paci
fier
use
and
bott
le-f
eedi
ngor
cupf
eedi
ngan
dth
eir
effe
cton
brea
stfe
edin
g.N
otin
ane
onat
alun
it
Jone
sE
.(19
95)
Mod
.Mid
wif
e.5(
3):8
–11.
Stra
tegi
esto
prom
ote
pret
erm
brea
stfe
edin
g.N
otan
inte
rven
tion
stud
yJo
nes
E.S
penc
erA
.(20
00)
Pro
fess
iona
lCar
eof
Mot
her
and
Chi
ld;1
0(6)
:14
5–7.
Pro
mot
ing
succ
essf
ulbr
east
feed
ing
for
mot
hers
ofpr
eter
min
fant
s–
1.N
otan
inte
rven
tion
stud
y
Jone
sL
.Spe
ncer
A.(
2002
)P
ract
isin
gM
idw
ife;
5(4)
:18–
20.
Pro
mot
ing
succ
essf
ulpr
eter
mbr
east
feed
ing:
part
1.N
otan
inte
rven
tion
stud
yJo
nes
L.S
penc
erA
.(20
02)
Pra
ctis
ing
Mid
wif
e;5(
5):2
2–4.
Pro
mot
ing
succ
essf
ulpr
eter
mbr
east
feed
ing:
part
2.N
otan
inte
rven
tion
stud
yJo
nes
L.S
penc
erA
.(20
02)
Pra
ctis
ing
Mid
wif
e;5(
6):1
8–9.
Est
ablis
hing
succ
essf
ulpr
eter
mbr
east
feed
ing:
part
3.N
otan
inte
rven
tion
stud
yK
enne
dyT
S.O
akla
ndM
J.Sh
awR
D.N
utri
tion
inC
linic
alP
ract
ice.
2000
;15
(1):
30–5
.A
nutr
itio
nin
terv
enti
onw
ith
fam
ilies
oflo
w-b
irth
-wei
ght
infa
nts.
Bre
astf
eedi
ngor
brea
stm
ilkno
tan
outc
ome
Mar
inel
liK
A,B
urke
GS,
Dod
dV
L(2
001)
.Jou
rnal
ofP
erin
atol
ogy;
21(6
):35
0–35
5.A
com
pari
son
ofth
esa
fety
ofcu
p-fe
edin
gsan
dbo
ttle
-fee
ding
sin
prem
atur
ein
fant
sw
hose
mot
hers
inte
ndto
brea
stfe
edB
reas
tfee
ding
orbr
east
milk
not
anou
tcom
eM
cCai
nG
C(1
995)
Jour
nalo
fP
edia
tric
Nur
sing
,10(
1):3
–8.
Pro
mot
ion
ofpr
eter
min
fant
nipp
lefe
edin
gw
ith
non-
nutr
itiv
esu
ckin
g.B
reas
tfee
ding
orbr
east
milk
not
anou
tcom
eM
cCai
nG
C.G
arts
ide
PS.
2002
New
born
and
Infa
ntN
ursi
ngR
evie
ws;
2(3)
:18
7–93
.B
ehav
iora
lres
pons
esof
pret
erm
infa
nts
toa
stan
dard
-car
ean
dse
mi-
dem
and
feed
ing
prot
ocol
.B
reas
tfee
ding
orbr
east
milk
not
anou
tcom
e?M
cCai
nG
C.G
arts
ide
PS.
Gre
enbe
rgJM
.Lot
tJW
.(20
01)
Jour
nalo
fP
edia
tric
s;13
9(3)
:374
–9.
Afe
edin
gpr
otoc
olfo
rhe
alth
ypr
eter
min
fant
sth
atsh
orte
nsti
me
toor
alfe
edin
g.[s
eeco
mm
ent]
.B
reas
tfee
ding
orbr
east
milk
not
anou
tcom
e?M
eier
PP.
(200
3)P
edia
tric
Ann
als.
Vol
.32(
5):3
17–3
25.
Supp
orti
ngla
ctat
ion
inm
othe
rsw
ith
very
low
birt
hw
eigh
tin
fant
s.N
otan
inte
rven
tion
stud
yM
eier
PP.
Eng
stro
mJL
.Man
gurt
enH
H.E
stra
daE
.Zim
mer
man
B.K
oppa
rthi
R.J
(199
3)O
bste
tG
ynec
olN
eona
talN
urs.
22(4
):33
8–47
.B
reas
tfee
ding
supp
ort
serv
ices
inth
ene
onat
alin
tens
ive-
care
unit
.N
otan
inte
rven
tion
stud
y
Infant feeding in the neonatal unit 257
© 2008 The Authors. Journal compilation © 2008 Blackwell Publishing Ltd. Maternal and Child Nutrition (2008), 4, pp. 235–263
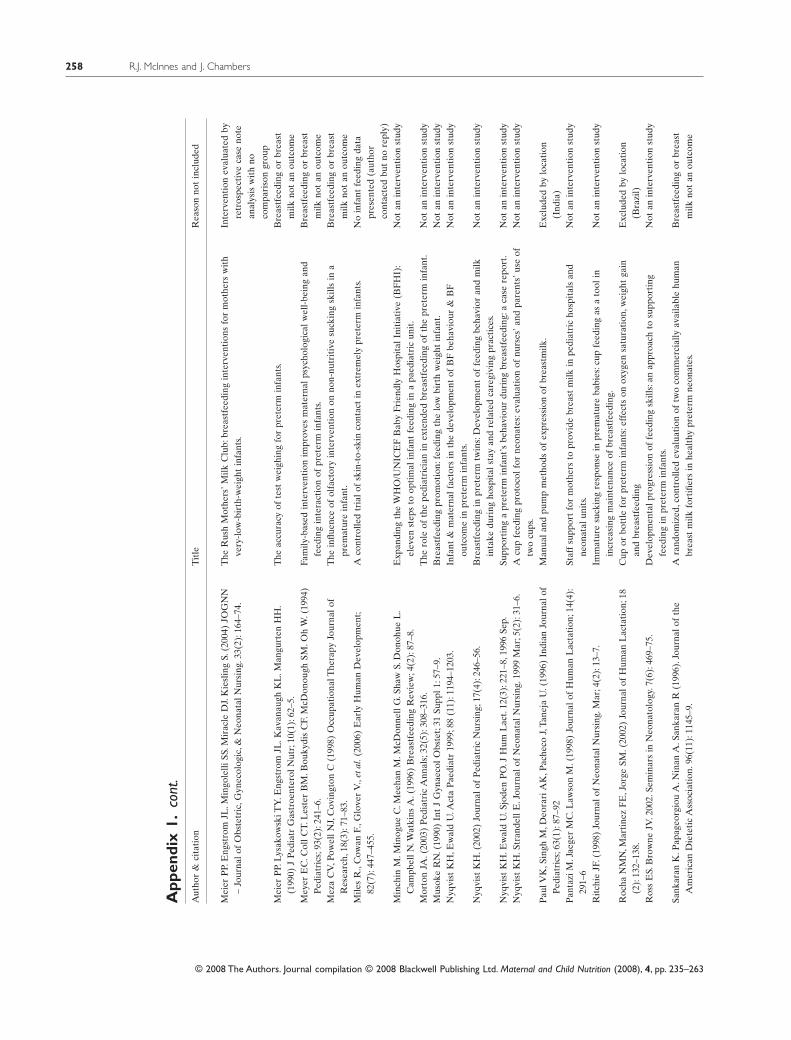
App
endi
x1.
cont
.A
utho
r&
cita
tion
Tit
leR
easo
nno
tin
clud
ed
Mei
erP
P.E
ngst
rom
JL.M
ingo
lelli
SS.M
irac
leD
J.K
iesl
ing
S.(2
004)
JOG
NN
–Jo
urna
lof
Obs
tetr
ic,G
ynec
olog
ic,&
Neo
nata
lNur
sing
.33(
2):1
64–7
4.T
heR
ush
Mot
hers
’Milk
Clu
b:br
east
feed
ing
inte
rven
tion
sfo
rm
othe
rsw
ith
very
-low
-bir
th-w
eigh
tin
fant
s.In
terv
enti
onev
alua
ted
byre
tros
pect
ive
case
note
anal
ysis
wit
hno
com
pari
son
grou
pM
eier
PP.
Lys
akow
skiT
Y.E
ngst
rom
JL.K
avan
augh
KL
.Man
gurt
enH
H.
(199
0)J
Ped
iatr
Gas
troe
nter
olN
utr;
10(1
):62
–5.
The
accu
racy
ofte
stw
eigh
ing
for
pret
erm
infa
nts.
Bre
astf
eedi
ngor
brea
stm
ilkno
tan
outc
ome
Mey
erE
C.C
ollC
T.L
este
rB
M.B
ouky
dis
CF.
McD
onou
ghSM
.Oh
W.(
1994
)P
edia
tric
s;93
(2):
241–
6.Fa
mily
-bas
edin
terv
enti
onim
prov
esm
ater
nalp
sych
olog
ical
wel
l-be
ing
and
feed
ing
inte
ract
ion
ofpr
eter
min
fant
s.B
reas
tfee
ding
orbr
east
milk
not
anou
tcom
eM
eza
CV
,Pow
ellN
J,C
ovin
gton
C(1
998)
Occ
upat
iona
lThe
rapy
Jour
nalo
fR
esea
rch,
18(3
):71
–83.
The
influ
ence
ofol
fact
ory
inte
rven
tion
onno
n-nu
trit
ive
suck
ing
skill
sin
apr
emat
ure
infa
nt.
Bre
astf
eedi
ngor
brea
stm
ilkno
tan
outc
ome
Mile
sR
.,C
owan
F.,G
love
rV
.,et
al.(
2006
)E
arly
Hum
anD
evel
opm
ent;
82(7
):44
7–45
5.A
cont
rolle
dtr
ialo
fsk
in-t
o-sk
inco
ntac
tin
extr
emel
ypr
eter
min
fant
s.N
oin
fant
feed
ing
data
pres
ente
d(a
utho
rco
ntac
ted
but
nore
ply)
Min
chin
M.M
inog
ueC
.Mee
han
M.M
cDon
nell
G.S
haw
S.D
onoh
ueL
.C
ampb
ellN
.Wat
kins
A.(
1996
)B
reas
tfee
ding
Rev
iew
;4(2
):87
–8.
Exp
andi
ngth
eW
HO
/UN
ICE
FB
aby
Frie
ndly
Hos
pita
lIni
tiat
ive
(BF
HI)
:el
even
step
sto
opti
mal
infa
ntfe
edin
gin
apa
edia
tric
unit
.N
otan
inte
rven
tion
stud
y
Mor
ton
JA.(
2003
)P
edia
tric
Ann
als;
32(5
):30
8–31
6.T
hero
leof
the
pedi
atri
cian
inex
tend
edbr
east
feed
ing
ofth
epr
eter
min
fant
.N
otan
inte
rven
tion
stud
yM
usok
eR
N.(
1990
)In
tJ
Gyn
aeco
lObs
tet;
31Su
ppl1
:57–
9.B
reas
tfee
ding
prom
otio
n:fe
edin
gth
elo
wbi
rth
wei
ght
infa
nt.
Not
anin
terv
enti
onst
udy
Nyq
vist
KH
,Ew
ald
U.A
cta
Pae
diat
r19
99;8
8(1
1):1
194–
1203
.In
fant
&m
ater
nalf
acto
rsin
the
deve
lopm
ent
ofB
Fbe
havi
our
&B
Fou
tcom
ein
pret
erm
infa
nts.
Not
anin
terv
enti
onst
udy
Nyq
vist
KH
.(20
02)
Jour
nalo
fP
edia
tric
Nur
sing
;17(
4):2
46–5
6.B
reas
tfee
ding
inpr
eter
mtw
ins:
Dev
elop
men
tof
feed
ing
beha
vior
and
milk
inta
kedu
ring
hosp
ital
stay
and
rela
ted
care
givi
ngpr
acti
ces.
Not
anin
terv
enti
onst
udy
Nyq
vist
KH
.Ew
ald
U.S
jode
nP
O.J
Hum
Lac
t.12
(3):
221–
8,19
96Se
p.Su
ppor
ting
apr
eter
min
fant
’sbe
havi
our
duri
ngbr
east
feed
ing:
aca
sere
port
.N
otan
inte
rven
tion
stud
yN
yqvi
stK
H.S
tran
dell
E.J
ourn
alof
Neo
nata
lNur
sing
.199
9M
ar;5
(2):
31–6
.A
cup
feed
ing
prot
ocol
for
neon
ates
:eva
luat
ion
ofnu
rses
’and
pare
nts’
use
oftw
ocu
ps.
Not
anin
terv
enti
onst
udy
Pau
lVK
,Sin
ghM
,Deo
rari
AK
,Pac
heco
J,Ta
neja
U.(
1996
)In
dian
Jour
nalo
fP
edia
tric
s;63
(1):
87–9
2M
anua
land
pum
pm
etho
dsof
expr
essi
onof
brea
stm
ilk.
Exc
lude
dby
loca
tion
(Ind
ia)
Pan
tazi
M.J
aege
rM
C.L
awso
nM
.(19
98)
Jour
nalo
fH
uman
Lac
tati
on;1
4(4)
:29
1–6
Staf
fsu
ppor
tfo
rm
othe
rsto
prov
ide
brea
stm
ilkin
pedi
atri
cho
spit
als
and
neon
atal
unit
s.N
otan
inte
rven
tion
stud
y
Rit
chie
JF.(
1998
)Jo
urna
lof
Neo
nata
lNur
sing
.Mar
;4(2
):13
–7.
Imm
atur
esu
ckin
gre
spon
sein
prem
atur
eba
bies
:cup
feed
ing
asa
tool
inin
crea
sing
mai
nten
ance
ofbr
east
feed
ing.
Not
anin
terv
enti
onst
udy
Roc
haN
MN
,Mar
tine
zF
E,J
orge
SM.(
2002
)Jo
urna
lof
Hum
anL
acta
tion
;18
(2):
132–
138.
Cup
orbo
ttle
for
pret
erm
infa
nts:
effe
cts
onox
ygen
satu
rati
on,w
eigh
tga
inan
dbr
east
feed
ing
Exc
lude
dby
loca
tion
(Bra
zil)
Ros
sE
S.B
row
neJV
.200
2.Se
min
ars
inN
eona
tolo
gy.7
(6):
469–
75.
Dev
elop
men
talp
rogr
essi
onof
feed
ing
skill
s:an
appr
oach
tosu
ppor
ting
feed
ing
inpr
eter
min
fant
s.N
otan
inte
rven
tion
stud
y
Sank
aran
K.P
apag
eorg
iou
A.N
inan
A.S
anka
ran
R(1
996)
.Jou
rnal
ofth
eA
mer
ican
Die
teti
cA
ssoc
iati
on.9
6(11
):11
45–9
.A
rand
omiz
ed,c
ontr
olle
dev
alua
tion
oftw
oco
mm
erci
ally
avai
labl
ehu
man
brea
stm
ilkfo
rtifi
ers
inhe
alth
ypr
eter
mne
onat
es.
Bre
astf
eedi
ngor
brea
stm
ilkno
tan
outc
ome
R.J. McInnes and J. Chambers258
© 2008 The Authors. Journal compilation © 2008 Blackwell Publishing Ltd. Maternal and Child Nutrition (2008), 4, pp. 235–263
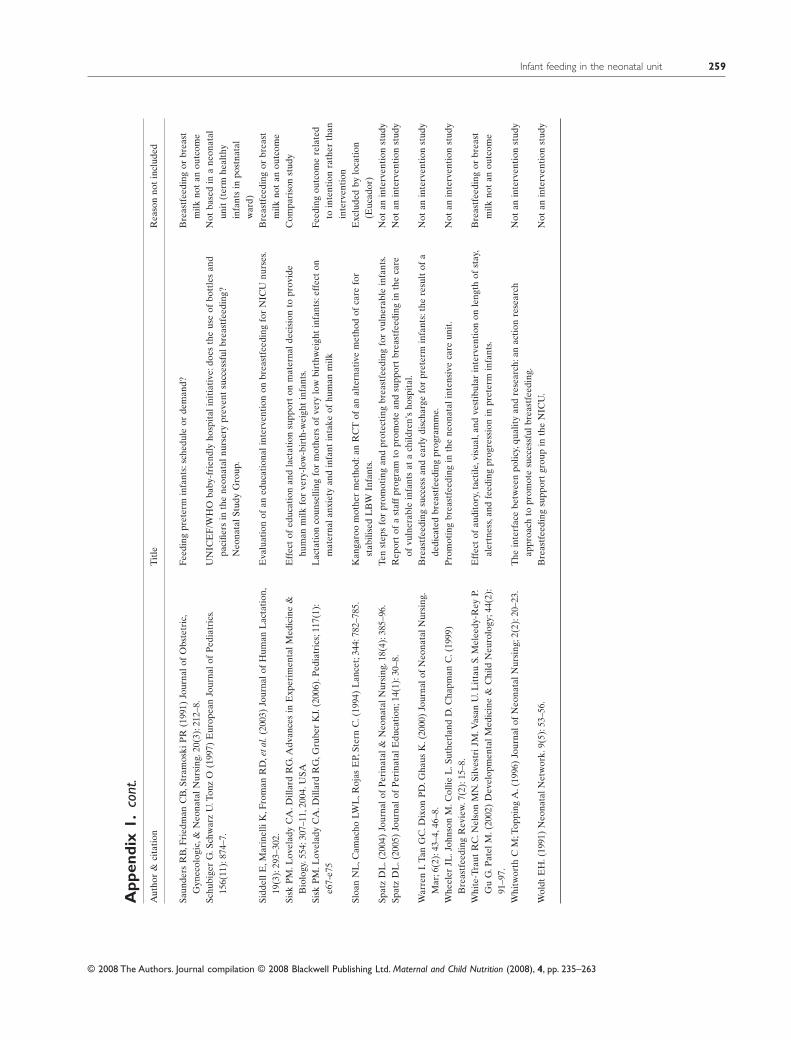
App
endi
x1.
cont
.A
utho
r&
cita
tion
Tit
leR
easo
nno
tin
clud
ed
Saun
ders
RB
,Fri
edm
anC
B,S
tram
oski
PR
(199
1)Jo
urna
lof
Obs
tetr
ic,
Gyn
ecol
ogic
,&N
eona
talN
ursi
ng.2
0(3)
:212
–8.
Feed
ing
pret
erm
infa
nts:
sche
dule
orde
man
d?B
reas
tfee
ding
orbr
east
milk
not
anou
tcom
eSc
hubi
ger
G.S
chw
arz
U.T
onz
O(1
997)
Eur
opea
nJo
urna
lof
Ped
iatr
ics.
156(
11):
874–
7.U
NIC
EF
/WH
Oba
by-f
rien
dly
hosp
ital
init
iati
ve:d
oes
the
use
ofbo
ttle
san
dpa
cifie
rsin
the
neon
atal
nurs
ery
prev
ent
succ
essf
ulbr
east
feed
ing?
Neo
nata
lStu
dyG
roup
.
Not
base
din
ane
onat
alun
it(t
erm
heal
thy
infa
nts
inpo
stna
tal
war
d)Si
ddel
lE,M
arin
elli
K,F
rom
anR
D,e
tal.
(200
3)Jo
urna
lof
Hum
anL
acta
tion
,19
(3):
293–
302.
Eva
luat
ion
ofan
educ
atio
nali
nter
vent
ion
onbr
east
feed
ing
for
NIC
Unu
rses
.B
reas
tfee
ding
orbr
east
milk
not
anou
tcom
eSi
skP
M.L
ovel
ady
CA
.Dill
ard
RG
.Adv
ance
sin
Exp
erim
enta
lMed
icin
e&
Bio
logy
.554
:307
–11,
2004
.USA
Eff
ect
ofed
ucat
ion
and
lact
atio
nsu
ppor
ton
mat
erna
ldec
isio
nto
prov
ide
hum
anm
ilkfo
rve
ry-l
ow-b
irth
-wei
ght
infa
nts.
Com
pari
son
stud
y
Sisk
PM
.Lov
elad
yC
A.D
illar
dR
G,G
rube
rK
J.(2
006)
.Ped
iatr
ics;
117(
1):
e67-
e75
Lac
tati
onco
unse
lling
for
mot
hers
ofve
rylo
wbi
rthw
eigh
tin
fant
s:ef
fect
onm
ater
nala
nxie
tyan
din
fant
inta
keof
hum
anm
ilkFe
edin
gou
tcom
ere
late
dto
inte
ntio
nra
ther
than
inte
rven
tion
Sloa
nN
L,C
amac
hoLW
L,R
ojas
EP,
Ster
nC
.(19
94)
Lan
cet;
344:
782–
785.
Kan
garo
om
othe
rm
etho
d:an
RC
Tof
anal
tern
ativ
em
etho
dof
care
for
stab
ilise
dL
BW
Infa
nts.
Exc
lude
dby
loca
tion
(Euc
ador
)Sp
atz
DL
.(20
04)
Jour
nalo
fP
erin
atal
&N
eona
talN
ursi
ng.1
8(4)
:385
–96.
Ten
step
sfo
rpr
omot
ing
and
prot
ecti
ngbr
east
feed
ing
for
vuln
erab
lein
fant
s.N
otan
inte
rven
tion
stud
ySp
atz
DL
.(20
05)
Jour
nalo
fP
erin
atal
Edu
cati
on;1
4(1)
:30–
8.R
epor
tof
ast
aff
prog
ram
topr
omot
ean
dsu
ppor
tbr
east
feed
ing
inth
eca
reof
vuln
erab
lein
fant
sat
ach
ildre
n’s
hosp
ital
.N
otan
inte
rven
tion
stud
y
War
ren
I.Ta
nG
C.D
ixon
PD
.Gha
usK
.(20
00)
Jour
nalo
fN
eona
talN
ursi
ng.
Mar
;6(2
):43
–4,4
6–8.
Bre
astf
eedi
ngsu
cces
san
dea
rly
disc
harg
efo
rpr
eter
min
fant
s:th
ere
sult
ofa
dedi
cate
dbr
east
feed
ing
prog
ram
me.
Not
anin
terv
enti
onst
udy
Whe
eler
JL.J
ohns
onM
.Col
lieL
.Sut
herl
and
D.C
hapm
anC
.(19
99)
Bre
astf
eedi
ngR
evie
w.7
(2):
15–8
.P
rom
otin
gbr
east
feed
ing
inth
ene
onat
alin
tens
ive
care
unit
.N
otan
inte
rven
tion
stud
y
Whi
te-T
raut
RC
.Nel
son
MN
.Silv
estr
iJM
.Vas
anU
.Lit
tau
S.M
elee
dy-R
eyP.
Gu
G.P
atel
M.(
2002
)D
evel
opm
enta
lMed
icin
e&
Chi
ldN
euro
logy
;44(
2):
91–9
7.
Eff
ect
ofau
dito
ry,t
acti
le,v
isua
l,an
dve
stib
ular
inte
rven
tion
onle
ngth
ofst
ay,
aler
tnes
s,an
dfe
edin
gpr
ogre
ssio
nin
pret
erm
infa
nts.
Bre
astf
eedi
ngor
brea
stm
ilkno
tan
outc
ome
Whi
twor
thC
M;T
oppi
ngA
.(19
96)
Jour
nalo
fN
eona
talN
ursi
ng;2
(2):
20–2
3.T
hein
terf
ace
betw
een
polic
y,qu
alit
yan
dre
sear
ch:a
nac
tion
rese
arch
appr
oach
topr
omot
esu
cces
sful
brea
stfe
edin
g.N
otan
inte
rven
tion
stud
y
Wol
dtE
H.(
1991
)N
eona
talN
etw
ork.
9(5)
:53–
56.
Bre
astf
eedi
ngsu
ppor
tgr
oup
inth
eN
ICU
.N
otan
inte
rven
tion
stud
y
Infant feeding in the neonatal unit 259
© 2008 The Authors. Journal compilation © 2008 Blackwell Publishing Ltd. Maternal and Child Nutrition (2008), 4, pp. 235–263
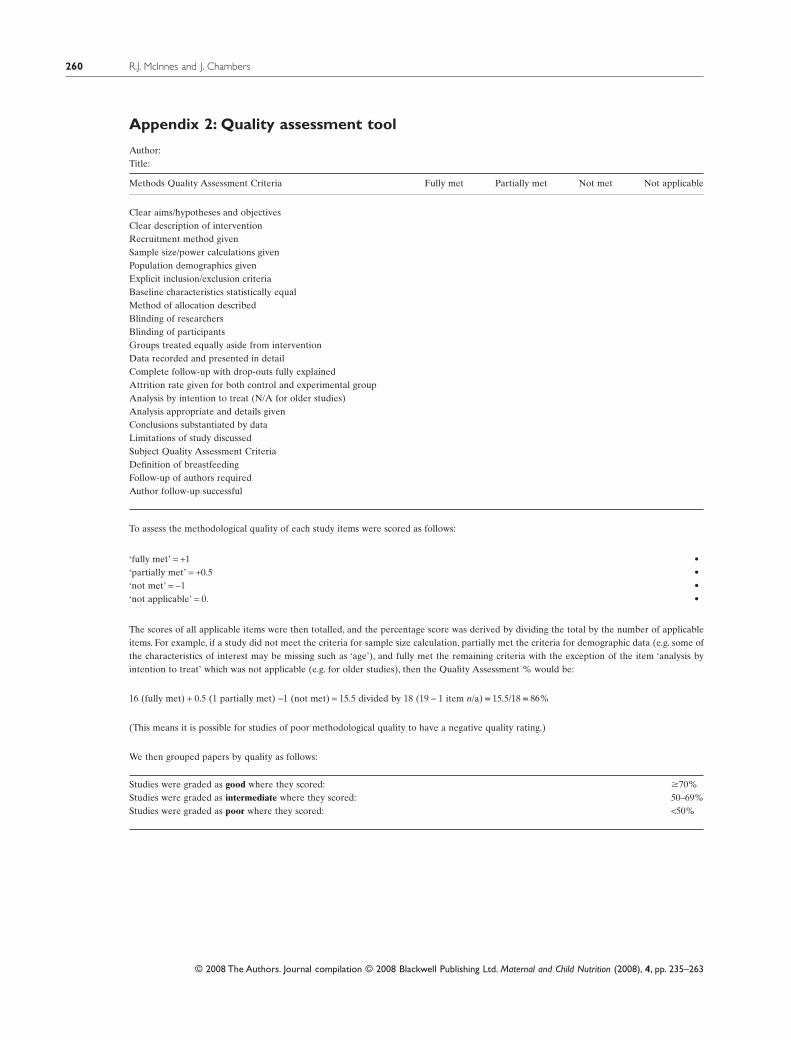
Appendix 2: Quality assessment tool
Author:Title:
Methods Quality Assessment Criteria Fully met Partially met Not met Not applicable
Clear aims/hypotheses and objectivesClear description of interventionRecruitment method givenSample size/power calculations givenPopulation demographics givenExplicit inclusion/exclusion criteriaBaseline characteristics statistically equalMethod of allocation describedBlinding of researchersBlinding of participantsGroups treated equally aside from interventionData recorded and presented in detailComplete follow-up with drop-outs fully explainedAttrition rate given for both control and experimental groupAnalysis by intention to treat (N/A for older studies)Analysis appropriate and details givenConclusions substantiated by dataLimitations of study discussedSubject Quality Assessment CriteriaDefinition of breastfeedingFollow-up of authors requiredAuthor follow-up successful
To assess the methodological quality of each study items were scored as follows:
•‘fully met’ = +1•‘partially met’ = +0.5•‘not met’ = -1•‘not applicable’ = 0.
The scores of all applicable items were then totalled, and the percentage score was derived by dividing the total by the number of applicableitems. For example, if a study did not meet the criteria for sample size calculation, partially met the criteria for demographic data (e.g. some ofthe characteristics of interest may be missing such as ‘age’), and fully met the remaining criteria with the exception of the item ‘analysis byintention to treat’ which was not applicable (e.g. for older studies), then the Quality Assessment % would be:
16 (fully met) + 0.5 (1 partially met) -1 (not met) = 15.5 divided by 18 (19 - 1 item n/a) = 15.5/18 = 86%
(This means it is possible for studies of poor methodological quality to have a negative quality rating.)
We then grouped papers by quality as follows:
Studies were graded as good where they scored: �70%Studies were graded as intermediate where they scored: 50–69%Studies were graded as poor where they scored: <50%
R.J. McInnes and J. Chambers260
© 2008 The Authors. Journal compilation © 2008 Blackwell Publishing Ltd. Maternal and Child Nutrition (2008), 4, pp. 235–263
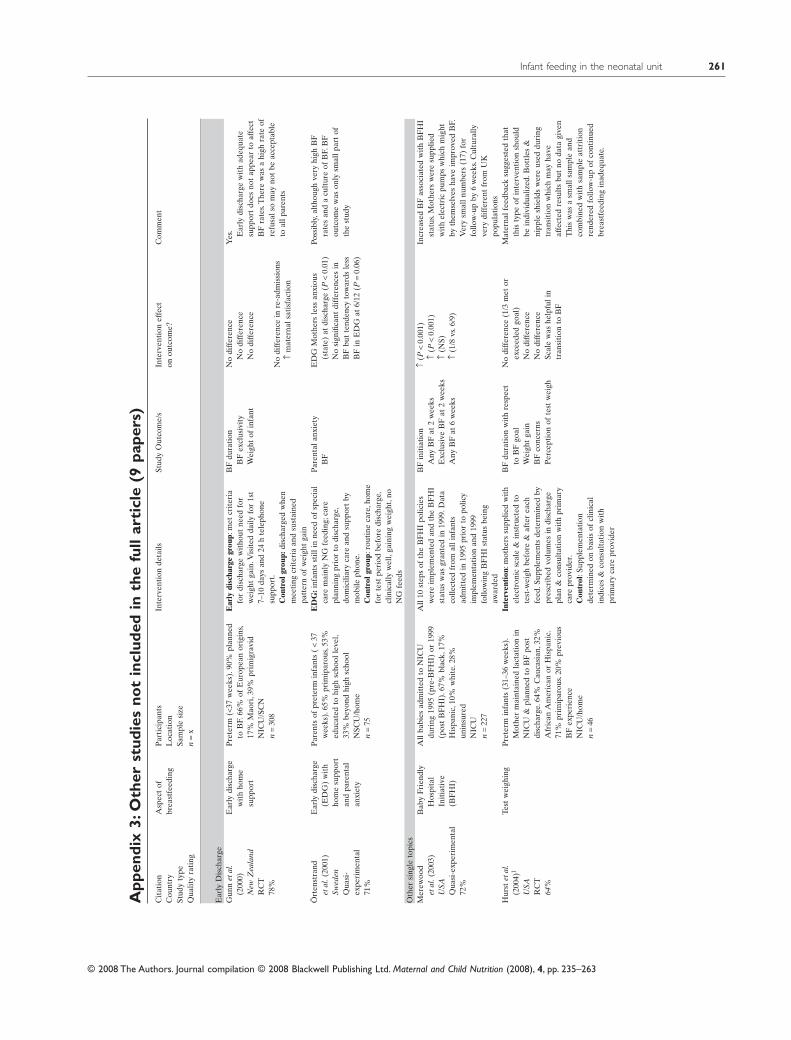
App
endi
x3:
Oth
erst
udie
sno
tin
clud
edin
the
full
arti
cle
(9pa
pers
)C
itat
ion
Cou
ntry
Stud
yty
peQ
ualit
yra
ting
Asp
ect
ofbr
east
feed
ing
Par
tici
pant
sL
ocat
ion
Sam
ple
size
n=
x
Inte
rven
tion
deta
ilsSt
udy
Out
com
e/s
Inte
rven
tion
effe
cton
outc
ome?
Com
men
t
Ear
lyD
isch
arge
Gun
net
al.
(200
0)N
ewZ
eala
ndR
CT
78%
Ear
lydi
scha
rge
wit
hho
me
supp
ort
Pre
term
(<37
wee
ks).
90%
plan
ned
toB
F.66
%of
Eur
opea
nor
igin
s,17
%M
aori
,39%
prim
igra
vid
NIC
U/S
CN
n=
308
Ear
lydi
scha
rge
grou
p:m
etcr
iter
iafo
rdi
scha
rge
wit
hout
need
for
wei
ght
gain
.Vis
ited
daily
for
1st
7–10
days
and
24h
tele
phon
esu
ppor
t.C
ontr
olgr
oup:
disc
harg
edw
hen
mee
ting
crit
eria
and
sust
aine
dpa
tter
nof
wei
ght
gain
BF
dura
tion
BF
excl
usiv
ity
Wei
ght
ofin
fant
No
diff
eren
ceN
odi
ffer
ence
No
diff
eren
ce
Yes
. Ear
lydi
scha
rge
wit
had
equa
tesu
ppor
tdo
esno
tap
pear
toaf
fect
BF
rate
s.T
here
was
ahi
ghra
teof
refu
sals
om
ayno
tbe
acce
ptab
leto
allp
aren
tsN
odi
ffer
ence
inre
-adm
issi
ons
↑m
ater
nals
atis
fact
ion
Ört
enst
rand
etal
.(20
01)
Swed
enQ
uasi
-ex
peri
men
tal
71%
Ear
lydi
scha
rge
(ED
G)
wit
hho
me
supp
ort
and
pare
ntal
anxi
ety
Par
ents
ofpr
eter
min
fant
s(
<37
wee
ks).
65%
prim
ipar
ous,
53%
educ
ated
tohi
ghsc
hool
leve
l,33
%be
yond
high
scho
olN
SCU
/hom
en
=75
ED
G:i
nfan
tsst
illin
need
ofsp
ecia
lca
rem
ainl
yN
Gfe
edin
g;ca
repl
anni
ngpr
ior
todi
scha
rge,
dom
icili
ary
care
and
supp
ort
bym
obile
phon
e.C
ontr
olgr
oup:
rout
ine
care
,hom
efo
rte
stpe
riod
befo
redi
scha
rge,
clin
ical
lyw
ell,
gain
ing
wei
ght,
noN
Gfe
eds
Par
enta
lanx
iety
BF
ED
GM
othe
rsle
ssan
xiou
s(s
tate
)at
disc
harg
e(P
<0.
01)
No
sign
ifica
ntdi
ffer
ence
sin
BF
but
tend
ency
tow
ards
less
BF
inE
DG
at6/
12(P
=0.
06)
Poss
ibly
,alt
houg
hve
ryhi
ghB
Fra
tes
and
acu
ltur
eof
BF.
BF
outc
ome
was
only
smal
lpar
tof
the
stud
y
Oth
ersi
ngle
topi
csM
erew
ood
etal
.(20
03)
USA
Qua
si-e
xper
imen
tal
72%
Bab
yFr
iend
lyH
ospi
tal
Init
iati
ve(B
FH
I)
All
babi
esad
mit
ted
toN
ICU
duri
ng19
95(p
re-B
FH
I)or
1999
(pos
tB
FH
I).6
7%bl
ack,
17%
His
pani
c,10
%w
hite
.28%
unin
sure
dN
ICU
n=
227
All
10st
eps
ofth
eB
FH
Ipo
licie
sw
ere
impl
emen
ted
and
the
BF
HI
stat
usw
asgr
ante
din
1999
.Dat
aco
llect
edfr
omal
linf
ants
adm
itte
din
1995
prio
rto
polic
yim
plem
enta
tion
and
1999
follo
win
gB
FH
Ist
atus
bein
gaw
arde
d
BF
init
iati
onA
nyB
Fat
2w
eeks
Exc
lusi
veB
Fat
2w
eeks
Any
BF
at6
wee
ks
↑(P
<0.
001)
↑(P
<0.
001)
↑(N
S)↑
(1/8
vs.6
/9)
Incr
ease
dB
Fas
soci
ated
wit
hB
FH
Ist
atus
.Mot
hers
wer
esu
pplie
dw
ith
elec
tric
pum
psw
hich
mig
htby
them
selv
esha
veim
prov
edB
F.V
ery
smal
lnum
bers
(17)
for
follo
w-u
pby
6w
eeks
.Cul
tura
llyve
rydi
ffer
ent
from
UK
popu
lati
ons
Hur
stet
al.
(200
4)1
USA
RC
T64
%
Test
wei
ghin
gP
rete
rmin
fant
s(3
1–36
wee
ks).
Mot
her
mai
ntai
ned
lact
atio
nin
NIC
U&
plan
ned
toB
Fpo
stdi
scha
rge.
64%
Cau
casi
an,3
2%A
fric
anA
mer
ican
orH
ispa
nic.
71%
prim
ipar
ous.
20%
prev
ious
BF
expe
rien
ceN
ICU
/hom
en
=46
Inte
rven
tion
:mot
hers
supp
lied
wit
hel
ectr
onic
scal
e&
inst
ruct
edto
test
-wei
ghbe
fore
&af
ter
each
feed
.Sup
plem
ents
dete
rmin
edby
pres
crib
edvo
lum
esin
disc
harg
epl
an&
cons
ulta
tion
wit
hpr
imar
yca
repr
ovid
er.
Con
trol
:Sup
plem
enta
tion
dete
rmin
edon
basi
sof
clin
ical
indi
ces
&co
nsul
tati
onw
ith
prim
ary
care
prov
ider
BF
dura
tion
wit
hre
spec
tto
BF
goal
Wei
ght
gain
BF
conc
erns
Per
cept
ion
ofte
stw
eigh
No
diff
eren
ce(1
/3m
etor
exce
eded
goal
)N
odi
ffer
ence
No
diff
eren
ceSc
ale
was
help
fuli
ntr
ansi
tion
toB
F
Mat
erna
lfee
dbac
ksu
gges
ted
that
this
type
ofin
terv
enti
onsh
ould
bein
divi
dual
ized
.Bot
tles
&ni
pple
shie
lds
wer
eus
eddu
ring
tran
siti
onw
hich
may
have
affe
cted
resu
lts
but
noda
tagi
ven
Thi
sw
asa
smal
lsam
ple
and
com
bine
dw
ith
sam
ple
attr
itio
nre
nder
edfo
llow
-up
ofco
ntin
ued
brea
stfe
edin
gin
adeq
uate
.
Infant feeding in the neonatal unit 261
© 2008 The Authors. Journal compilation © 2008 Blackwell Publishing Ltd. Maternal and Child Nutrition (2008), 4, pp. 235–263
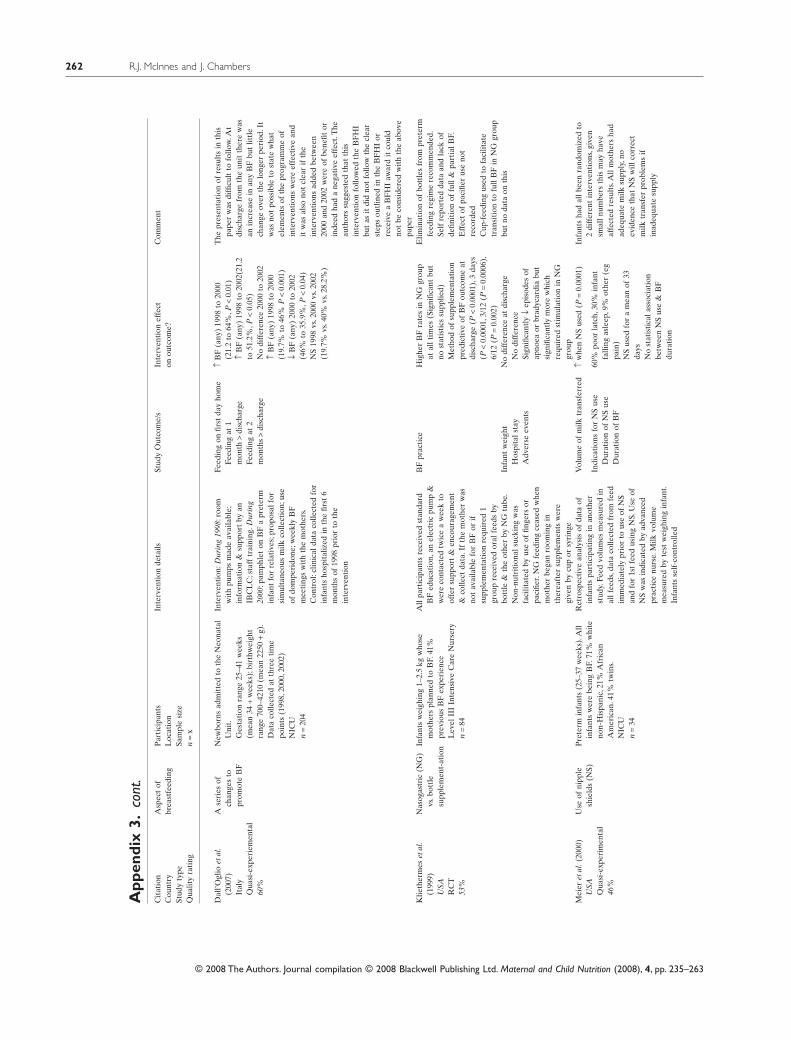
App
endi
x3.
cont
.C
itat
ion
Cou
ntry
Stud
yty
peQ
ualit
yra
ting
Asp
ect
ofbr
east
feed
ing
Par
tici
pant
sL
ocat
ion
Sam
ple
size
n=
x
Inte
rven
tion
deta
ilsSt
udy
Out
com
e/s
Inte
rven
tion
effe
cton
outc
ome?
Com
men
t
Dal
l’Ogl
ioet
al.
(200
7)It
aly
Qua
si-e
xper
iem
enta
l60
%
Ase
ries
ofch
ange
sto
prom
ote
BF
New
born
sad
mit
ted
toth
eN
eona
tal
Uni
t.G
esta
tion
rang
e25
–41
wee
ks(m
ean
34+
wee
ks);
birt
hwei
ght
rang
e70
0–42
10(m
ean
2250
+g)
.D
ata
colle
cted
atth
ree
tim
epo
ints
(199
8,20
00,2
002)
NIC
Un
=20
4
Inte
rven
tion
:Dur
ing
1998
:roo
mw
ith
pum
psm
ade
avai
labl
e;in
form
atio
n&
supp
ort
byan
IBC
LC
;sta
fftr
aini
ng.D
urin
g20
00:p
amph
let
onB
Fa
pret
erm
infa
ntfo
rre
lati
ves;
prop
osal
for
sim
ulta
neou
sm
ilkco
llect
ion;
use
ofdo
mpe
rido
ne;w
eekl
yB
Fm
eeti
ngs
wit
hth
em
othe
rs.
Con
trol
:clin
ical
data
colle
cted
for
infa
nts
hosp
ital
ized
inth
efir
st6
mon
ths
of19
98pr
ior
toth
ein
terv
enti
on
Feed
ing
onfir
stda
yho
me
Feed
ing
at1
mon
th>
disc
harg
eFe
edin
gat
2m
onth
s>
disc
harg
e
↑B
F(a
ny)
1998
to20
00(2
1.2
to64
%,P
<0.
01)
↑B
F(a
ny)
1998
to20
02(2
1.2
to51
.2%
,P<
0.05
)N
odi
ffer
ence
2000
to20
02↑
BF
(any
)19
98to
2000
(19.
7%to
46%
P<
0.00
1)↓
BF
(any
)20
00to
2002
(46%
to35
.9%
,P<
0.04
)N
S19
98vs
.200
0vs
.200
2(1
9.7%
vs.4
0%vs
.28.
2%)
The
pres
enta
tion
ofre
sult
sin
this
pape
rw
asdi
fficu
ltto
follo
w.A
tdi
scha
rge
from
the
unit
ther
ew
asan
incr
ease
inan
yB
Fbu
tlit
tle
chan
geov
erth
elo
nger
peri
od.I
tw
asno
tpo
ssib
leto
stat
ew
hat
elem
ents
ofth
epr
ogra
mm
eof
inte
rven
tion
sw
ere
effe
ctiv
ean
dit
was
also
not
clea
rif
the
inte
rven
tion
sad
ded
betw
een
2000
and
2002
wer
eof
bene
fitor
inde
edha
da
nega
tive
effe
ct.T
heau
thor
ssu
gges
ted
that
this
inte
rven
tion
follo
wed
the
BF
HI
but
asit
did
not
follo
wth
ecl
ear
step
sou
tlin
edin
the
BF
HI
orre
ceiv
ea
BF
HI
awar
dit
coul
dno
tbe
cons
ider
edw
ith
the
abov
epa
per
Klie
ther
mes
etal
.(1
999)
USA
RC
T53
%
Nas
ogas
tric
(NG
)vs
.bot
tle
supp
lem
ent-
atio
nInfa
nts
wei
ghin
g1–
2.5
kgw
hose
mot
hers
plan
ned
toB
F.41
%pr
evio
usB
Fex
peri
ence
Lev
elII
IIn
tens
ive
Car
eN
urse
ryn
=84
All
part
icip
ants
rece
ived
stan
dard
BF
educ
atio
n,an
elec
tric
pum
p&
wer
eco
ntac
ted
twic
ea
wee
kto
offe
rsu
ppor
t&
enco
urag
emen
t&
colle
ctda
ta.I
fth
em
othe
rw
asno
tav
aila
ble
for
BF
orif
supp
lem
enta
tion
requ
ired
1gr
oup
rece
ived
oral
feed
sby
bott
le&
the
othe
rby
NG
tube
.N
on-n
utri
tion
alsu
ckin
gw
asfa
cilit
ated
byus
eof
finge
rsor
paci
fier.
NG
feed
ing
ceas
edw
hen
mot
her
bega
nro
omin
gin
ther
eaft
ersu
pple
men
tsw
ere
give
nby
cup
orsy
ring
e
BF
prac
tice
Hig
her
BF
rate
sin
NG
grou
pat
allt
imes
(Sig
nific
ant
but
nost
atis
tics
supp
lied)
Met
hod
ofsu
pple
men
tati
onpr
edic
tive
ofB
Fou
tcom
eat
disc
harg
e(P
<0.
0001
),3
days
(P<
0.00
01,3
/12
(P=
0.00
06),
6/12
(P=
0.00
2)
Elim
inat
ion
ofbo
ttle
sfr
ompr
eter
mfe
edin
gre
gim
ere
com
men
ded.
Self
repo
rted
data
and
lack
ofde
finit
ion
offu
ll&
part
ialB
F.E
ffec
tof
paci
fier
use
not
reco
rded
Cup
-fee
ding
used
tofa
cilit
ate
tran
siti
onto
full
BF
inN
Ggr
oup
but
noda
taon
this
Infa
ntw
eigh
tH
ospi
tals
tay
Adv
erse
even
ts
No
diff
eren
ceat
disc
harg
eN
odi
ffer
ence
Sign
ifica
ntly
↓ep
isod
esof
apno
eaor
brad
ycar
dia
but
sign
ifica
ntly
mor
ew
hich
requ
ired
stim
ulat
ion
inN
Ggr
oup
Mei
eret
al.(
2000
)U
SAQ
uasi
-exp
erim
enta
l46
%
Use
ofni
pple
shie
lds
(NS)
Pre
term
infa
nts
(25–
37w
eeks
).A
llin
fant
sw
ere
bein
gB
F.71
%w
hite
non-
His
pani
c,21
%A
fric
anA
mer
ican
.41%
twin
s.N
ICU
n=
34
Ret
rosp
ecti
vean
alys
isof
data
ofin
fant
spa
rtic
ipat
ing
inan
othe
rst
udy.
Feed
volu
mes
mea
sure
din
allf
eeds
,dat
aco
llect
edfr
omfe
edim
med
iate
lypr
ior
tous
eof
NS
and
for
1st
feed
usin
gN
S.U
seof
NS
was
indi
cate
dby
adva
nced
prac
tice
nurs
e.M
ilkvo
lum
em
easu
red
byte
stw
eigh
ing
infa
nt.
Infa
nts
self
-con
trol
led
Vol
ume
ofm
ilktr
ansf
erre
d↑
whe
nN
Sus
ed(P
=0.
0001
)In
fant
sha
dal
lbee
nra
ndom
ized
to2
diff
eren
tin
terv
enti
ons,
give
nsm
alln
umbe
rsth
ism
ayha
veaf
fect
edre
sult
s.A
llm
othe
rsha
dad
equa
tem
ilksu
pply
,no
evid
ence
that
NS
will
corr
ect
milk
tran
sfer
prob
lem
sif
inad
equa
tesu
pply
Indi
cati
ons
for
NS
use
Dur
atio
nof
NS
use
Dur
atio
nof
BF
60%
poor
latc
h,30
%in
fant
falli
ngas
leep
,9%
othe
r(e
gpa
in)
NS
used
for
am
ean
of33
days
No
stat
isti
cala
ssoc
iati
onbe
twee
nN
Sus
e&
BF
dura
tion
R.J. McInnes and J. Chambers262
© 2008 The Authors. Journal compilation © 2008 Blackwell Publishing Ltd. Maternal and Child Nutrition (2008), 4, pp. 235–263
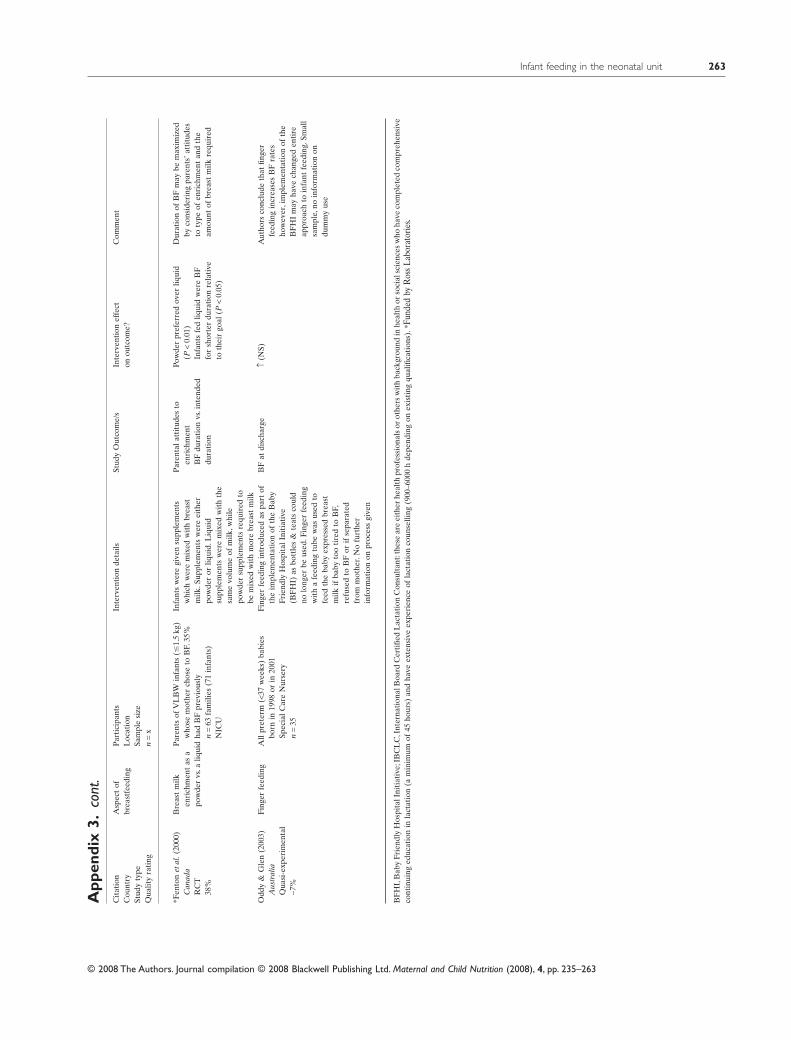
App
endi
x3.
cont
.C
itat
ion
Cou
ntry
Stud
yty
peQ
ualit
yra
ting
Asp
ect
ofbr
east
feed
ing
Par
tici
pant
sL
ocat
ion
Sam
ple
size
n=
x
Inte
rven
tion
deta
ilsSt
udy
Out
com
e/s
Inte
rven
tion
effe
cton
outc
ome?
Com
men
t
*Fen
ton
etal
.(20
00)
Can
ada
RC
T38
%
Bre
ast
milk
enri
chm
ent
asa
pow
der
vs.a
liqui
dPar
ents
ofV
LB
Win
fant
s(�
1.5
kg)
who
sem
othe
rch
ose
toB
F.35
%ha
dB
Fpr
evio
usly
n=
63fa
mili
es(7
1in
fant
s)N
ICU
Infa
nts
wer
egi
ven
supp
lem
ents
whi
chw
ere
mix
edw
ith
brea
stm
ilk.S
uppl
emen
tsw
ere
eith
erpo
wde
ror
liqui
d.L
iqui
dsu
pple
men
tsw
ere
mix
edw
ith
the
sam
evo
lum
eof
milk
,whi
lepo
wde
rsu
pple
men
tsre
quir
edto
bem
ixed
wit
hm
ore
brea
stm
ilk
Par
enta
latt
itud
esto
enri
chm
ent
BF
dura
tion
vs.i
nten
ded
dura
tion
Pow
der
pref
erre
dov
erliq
uid
(P<
0.01
)In
fant
sfe
dliq
uid
wer
eB
Ffo
rsh
orte
rdu
rati
onre
lati
veto
thei
rgo
al(P
<0.
05)
Dur
atio
nof
BF
may
bem
axim
ized
byco
nsid
erin
gpa
rent
s’at
titu
des
toty
peof
enri
chm
ent
and
the
amou
ntof
brea
stm
ilkre
quir
ed
Odd
y&
Gle
n(2
003)
Aus
tral
iaQ
uasi
-exp
erim
enta
l-7
%
Fing
erfe
edin
gA
llpr
eter
m(<
37w
eeks
)ba
bies
born
in19
98or
in20
01Sp
ecia
lCar
eN
urse
ryn
=35
Fing
erfe
edin
gin
trod
uced
aspa
rtof
the
impl
emen
tati
onof
the
Bab
yFr
iend
lyH
ospi
talI
niti
ativ
e(B
FH
I)as
bott
les
&te
ats
coul
dno
long
erbe
used
.Fin
ger
feed
ing
wit
ha
feed
ing
tube
was
used
tofe
edth
eba
byex
pres
sed
brea
stm
ilkif
baby
too
tire
dto
BF,
refu
sed
toB
For
ifse
para
ted
from
mot
her.
No
furt
her
info
rmat
ion
onpr
oces
sgi
ven
BF
atdi
scha
rge
↑(N
S)A
utho
rsco
nclu
deth
atfin
ger
feed
ing
incr
ease
sB
Fra
tes
how
ever
,im
plem
enta
tion
ofth
eB
FH
Im
ayha
vech
ange
den
tire
appr
oach
toin
fant
feed
ing.
Smal
lsa
mpl
e,no
info
rmat
ion
ondu
mm
yus
e
BF
HI,
Bab
yFr
iend
lyH
ospi
talI
niti
ativ
e;IB
CL
C,I
nter
nati
onal
Boa
rdC
erti
fied
Lac
tati
onC
onsu
ltan
t:th
ese
are
eith
erhe
alth
prof
essi
onal
sor
othe
rsw
ith
back
grou
ndin
heal
thor
soci
alsc
ienc
esw
hoha
veco
mpl
eted
com
preh
ensi
veco
ntin
uing
educ
atio
nin
lact
atio
n(a
min
imum
of45
hour
s)an
dha
veex
tens
ive
expe
rien
ceof
lact
atio
nco
unse
lling
(900
–600
0h
depe
ndin
gon
exis
ting
qual
ifica
tion
s).*
Fund
edby
Ros
sLa
bora
torie
s.
Infant feeding in the neonatal unit 263
© 2008 The Authors. Journal compilation © 2008 Blackwell Publishing Ltd. Maternal and Child Nutrition (2008), 4, pp. 235–263





























