Embed Size (px)
Citation preview

Infectious triggers of pediatric asthma
James E. Gern, MDa,*, Robert F. Lemanske, Jr., MDa,b
aDepartment of Pediatrics, University of Wisconsin Medical School, Madison, WI 53792, USAbDepartment of Medicine, University of Wisconsin Medical School, Madison, WI 53792, USA
Respiratory infections can cause wheezing illnesses in children of all ages and
also can influence the causation and disease activity of asthma. For years it has been
recognized that respiratory syncytial virus (RSV) infections often produce the first
episode of wheezing in children who go on to develop chronic asthma. More re-
cently, it has been proposed that repeated infections with other common childhood
viral pathogens might help the immune system develop in such a way as to prevent
the onset of allergic diseases and possibly asthma. In addition to the effects of viral
infections, infections with certain intracellular pathogens, such as Chlamydia and
Mycoplasma, may cause acute and chronic wheezing in some individuals, whereas
common cold and acute sinus infections can trigger acute symptoms of asthma. In
this article, the epidemiologic, mechanistic, and treatment implications of the
association between respiratory infections and asthma are discussed.
Epidemiology
Can infections cause asthma?
Asthma is a multifactorial disease that is likely to be the result of interactions
between a genetically determined predisposition to allergic diseases and envi-
ronmental factors that serve to enhance allergic inflammation and target inflam-
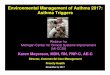
mation to the lower airway (Fig. 1). Genetic factors may include regulation of
cytokines that control the generation of IgE and eosinophilic inflammation, along
with polymorphisms in genes that regulate airway tone (eg, b-adrenergicreceptors) and repair mechanisms for acute injuries. Recent epidemiologic studies
suggest that environmental factors, and especially exposures in early infancy,
0031-3955/03/$ – see front matter D 2003 Elsevier Inc. All rights reserved.
doi:10.1016/S0031-3955(03)00040-3
This work was supported by NIH Grants AI34891, HL56396, 1RO1HL61879, and P01HL070831.
* Corresponding author. University of Wisconsin Hospital, 600 Highland Avenue, K4/918,
Madison, WI 53792–9988.
E-mail address: [email protected] (J.E. Gern).
Pediatr Clin N Am 50 (2003) 555–575

may play a major role in the development of the immune system. In this regard,
exposure to microbial products, allergens, stress, and perhaps even certain
infections may help the immune system to mature so that allergies are less likely
to occur. If allergy is present, severe lower respiratory infections (eg, RSV
bronchiolitis, and perhaps chronic infections with Mycoplasma, Chlamydia, and
Adenovirus) may damage the lungs or target allergic inflammatory responses to
the lower airway and thus promote the development of asthma.
Respiratory syncytial virus, lower respiratory illness, and bronchiolitis
Infection with RSV is the most common cause of bronchiolitis, which parallels
many of the features of childhood asthma [1]. From 1980 to 1996, rates of
hospitalization of infants with bronchiolitis increased substantially [2]; from this
report among others, RSV was found to cause about 70% of these episodes,
whereas Parainfluenza, Influenza, and Metapneumoviruses are less frequent
causes of wheezing. Although nearly all children are infected with RSV by
age 2 years [3], and only a subset of these infections cause wheezing, it is clear
that there are specific host risk factors that may predispose a child to lower
respiratory manifestations of infection. Some of the identified risk factors for
wheezing with respiratory infections in infancy include young age, small lung
size, passive exposure to smoke, and virus-induced immune responses [3,4].
Fig. 1. Role of viral infections in the pathogenesis of asthma. LRI = lower respiratory infection;
RSV = respiratory syncytial virus; PIV = parainfluenzavirus.
J.E. Gern, R.F. Lemanske, Jr. / Pediatr Clin N Am 50 (2003) 555–575556

Recently, additional insight into these areas has been provided by the results of
an 11-year prospective study involving 880 children who were enrolled at birth,
followed for the development of lower respiratory tract illnesses in the first
3 years of life and then evaluated for the presence or absence of physician-
diagnosed asthma or a history of current wheezing at ages 6 and 11 years [5].
Respiratory syncytial virus bronchiolitis increased the risk for both frequent
episodes of wheezing (> 3/year) and infrequent episodes of wheezing (< 3/year);
however, the risk decreased gradually with age and was not significant by age
13 years [6]. A decrease in the frequency of wheezing with increasing age
following documented RSV infections has been observed by other investigators
as well [7,8]. These data suggest that, although RSV infections contribute
substantially to the expression of the asthmatic phenotype, other cofactors (eg,
genetic, environmental, developmental) also seem to contribute, either in the
initial expression or the modification of the phenotype over time.
From a number of epidemiologic observations, it seems that other viral
infections during infancy and early childhood that have a predisposition for
lower airway involvement (eg, Parainfluenza, Influenza A) can also be associated
with chronic lower respiratory tract symptoms including asthma. [5,9–11].
Prospective measurements of lung function before the infection demonstrated
that children with reduced levels of lung function in infancy seem to be at
increased risk for the development of chronic lower respiratory tract sequelae
following viral infections. [5]. Whether this defect is alone responsible for these
developments is presently unknown. Further, the ability of one virus (ie, RSV) to
be more likely responsible for these outcomes (because of either virus- or host-
specific factors) has also not been well defined [8]. Indeed, recent data indicate
that bronchiolitis induced by viruses other than RSV may be associated with an
even greater risk for childhood asthma [12].
Chronic respiratory infections and asthma
It has been proposed that chronic viral and bacterial infections cause some
cases of recurrent wheezing and asthma. Organisms that have been implicated in
this process include Adenovirus [13], Chlamydia pneumoniae [14], and Myco-
plasma pneumoniae [15,16].
Historically, the first potential association between asthma and C. pneumoniae
was reported in 1991 in a study in which 9 of 19 wheezing adult asthmatic
patients were found to have serologic evidence of current or recent infection
with this organism [17]. Further, in school-aged children with asthma, titers of
C. pneumoniae–specific secretory IgA antibodies were greater in persons who
reported four or more exacerbations in the study than in those who reported only
one. Although there was no evidence linking acute Chlamydia infection and acute
exacerbations of asthma, these findings suggest that chronic infection with
Chlamydia was more common in children with higher rates of exacerbations.
Chronic chlamydial infection may possibly promote ongoing airway inflam-
mation that increases susceptibility to other exacerbating stimuli such as viruses,
allergens, or both.
J.E. Gern, R.F. Lemanske, Jr. / Pediatr Clin N Am 50 (2003) 555–575 557

Thus far the most comprehensive evaluation of the role of both Chlamydia and
Mycloplasma infections in chronic asthma was recently reported by Martin et al
[15]. This group of investigators evaluated 55 adult patients with chronic asthma
(percent of predicted forced expiratory volume at 1 second [FEV1] = 69.3 ± 2.1%)
and 11 controls for infection with Mycoplasma, Chlamydia, and viruses. Fifty-six
percent of the asthmatic patients had a positive polymerase chain reaction (PCR)
assay for Mycoplasma (n = 25) or Chlamydia (n = 7), which were mainly found in
lavage fluid or biopsy samples. Only 1 of 11 control subjects had a positive PCR
for Mycoplasma. Cultures for both organisms were negative in all patients,
and serologic confirmation correlated poorly with PCR results. Although these
intriguing findings suggest that these organisms may play a role in the patho-
physiology of asthma in some patients, the specificity of these findings to asthma
and the phenotypic and genotypic characteristics of the at-risk patient need
further delineation.
There have been several attempts to test the role of chronic infection in
patients with asthma through therapeutic trials of antibiotics. Although some of
these studies have had promising results [18], the data are difficult to interpret
because of the difficulty in eradicating Chlamydia and Mycoplasma infection,
nonblinded study designs, and the fact that many of the macrolide antibiotics
have anti-inflammatory effects in addition to serving as antimicrobials [19].
One additional mechanism implicated in the pathogenesis of chronic
asthmatic symptoms is latent Adenovirus infection [13]. A latent infection
occurs when a virus incorporates itself into the host cell DNA and continues to
express viral genes periodically. Respiratory disease caused by adenoviruses
can be followed by latent infection that persists for many years [20]. A
Slovenic study demonstrated that 94% of children with steroid-resistant asthma
had detectable Adenovirus antigens, compared with 0% of controls [21]. In
adults both with and without asthma, as many as 50% of the individuals tested
showed evidence of adenoviral infection [15]. Although these preliminary
results are intriguing, additional studies are needed to establish the causality
and the specificity of these observations to asthma pathogenesis and to define
the immunoinflammatory mechanisms contributing to these associations in
adult and pediatric patients.
Infections and acute exacerbations of asthma
Viral respiratory infections
The relationship between viral infections and wheezing illnesses in older
children and adults has been clarified by the advent of sensitive diagnostic tests,
based on PCR, for picornaviruses such as Rhinovirus (RV). With the devel-
opment of these more sensitive diagnostic tools, information linking common
cold infections with exacerbations of asthma has come from a number of sources.
Prospective studies of persons with asthma have demonstrated that up to 85% of
exacerbations of asthma in children and nearly half of such episodes in adults are
caused by viral infections [22]. Although many respiratory viruses can provoke
J.E. Gern, R.F. Lemanske, Jr. / Pediatr Clin N Am 50 (2003) 555–575558

acute asthma symptoms, RV is most often detected, especially during the spring
and fall RV seasons. In fact, the spring and fall peaks in hospitalizations caused
by asthma closely coincide with patterns of RV isolation within the community
[23]. Influenza and RSV are somewhat more likely to trigger acute asthma
symptoms in the wintertime but seem to account for a smaller fraction of asthma
flares. Furthermore, RV infections are frequently detected in children over the age
of 2 years who present to emergency departments with acute wheezing [24,25]
and in adults account for approximately one half of asthma-related acute care
visits [26]. Together, these studies provide evidence of a strong relationship
between viral infections, particularly those caused by RV, and acute exacerbations
of asthma.
Individuals with asthma do not necessarily have more colds, and neither the
severity nor duration of virus-induced upper respiratory symptoms is enhanced
by respiratory allergies or asthma [27,28]. In contrast to findings in the upper
airway, a prospective study of colds in couples consisting of one asthmatic and
one nonasthmatic individual demonstrated that colds cause greater duration and
severity of lower respiratory symptoms in persons with asthma [28]. These
findings suggest that there are fundamental differences in the lower airway effects
of respiratory viral infections related to asthma.
Although viral infections alone can promote lower airway symptoms, there is
evidence that viral infections may exert synergistic effects with other known
triggers for asthma. For example, the effects of colds on asthma may be amplified
by exposure to allergens [29] and possibly by exposure to greater levels of air
pollutants [30].
In addition to provoking asthma, RV infections can also increase lower airway
obstruction in individuals with other chronic airway diseases (eg, chronic
obstructive lung disease, cystic fibrosis) [31,32], and in infants [33] and elderly
persons [34]. Thus, common cold viruses that produce relatively mild illnesses in
most people can cause severe pulmonary problems in selected individuals.
Bacterial sinusitis
The nature of the association between asthma and sinusitis in children has
been the subject of debate for many years. Much of the difficulty in defining this
relationship results from the uncertainties in making the clinical diagnosis of
sinusitis, because the signs and symptoms of sinusitis in children overlap with
many common childhood respiratory disorders, including the common cold,
allergic rhinitis, and asthma.
Asthma and sinusitis are frequent comorbidities in children [35], and clinical
signs and symptoms compatible with sinusitis often occur during acute exacer-
bations of asthma, raising the possibility that bacterial sinusitis causes increased
lower respiratory symptoms. This hypothesis was the subject of a study
conducted by Rachelefsky and colleagues [36], who prospectively identified
48 children ages 4 to 13 years who had daily coughing and wheezing for at least
3 months, abnormal sinus radiographs (more than 6 mm maxillary sinus mucosal
edema on the Water’s view), and evidence of airway obstruction on pulmonary
J.E. Gern, R.F. Lemanske, Jr. / Pediatr Clin N Am 50 (2003) 555–575 559

function tests (decreased FEV1 and decreased forced expiratory flow in the
midexpiratory phase [FEF25%–75%]). These children were treated with 2 to
5 weeks of antibiotics, and 9 of the children with persistent symptoms and
radiographic evidence of sinusitis were subsequently referred to an otolaryngol-
ogist for antral lavage. Posttreatment evaluation revealed substantial improve-
ment in upper and lower respiratory symptoms, reduced use of bronchodilators,
and improved radiographic appearance of the sinuses. Although this study did not
include a control group, the findings suggest that children with chronic lower
respiratory symptoms that are refractory to usual asthma therapy may be at
increased risk of having concomitant bacterial sinusitis and that this infection
may contribute to the production of both upper and lower respiratory symptoms.
Two additional studies have expanded on these findings by correlating
respiratory symptoms, findings on sinus radiographs, and results of sinus aspirate
cultures in children with asthma and clinical evidence of sinusitis. Friedman and
colleagues [37] evaluated eight children with abnormal maxillary sinus radio-
graphs (opacification of at least one maxillary sinus) and acute asthma that was
unresponsive to bronchodilator therapy. Cultures of the sinus aspirate were
positive in five of these patients, and each patient improved after 2 weeks of
combined antibiotic and asthma therapy, including short courses of oral cortico-
steroid in four individuals. Goldenhersh et al [38] evaluated 12 children with
respiratory allergy and chronic sinusitis, including 9 asthmatic children between
the ages of 3 and 9 years who had nasal congestion or cough of more than
30 days’ duration, and abnormal sinus radiographs (8 of the 9 children had
opacification of at least one maxillary sinus). Pathogens, most commonly
Moraxella catarrhalis, were cultured from aspirates from 7 of the 9 asthmatic
subjects. Together, these studies suggest that children with asthma, chronic or
bronchodilator-resistant cough or wheeze, and chronic nasal congestion should be
evaluated for sinusitis, and that under these conditions, a sinus radiograph
revealing complete opacification of a maxillary sinus is usually indicative of
bacterial sinusitis. These studies also suggest that the combination of nasal lavage
and antibiotic therapy improves upper airway symptoms and may improve
asthma control as well. Finally, the limited data available regarding culture of
sinus content in children with asthma indicate that the microbiology of sinusitis is
similar in children with or without asthma [37–40].
Several mechanisms have been proposed to explain how infections of the
paranasal sinuses could cause bronchospasm and exacerbate asthma [41–43]. It
has been suggested that chronic aspiration of the contents of inflamed sinuses
could aggravate asthma [43,44]. Another hypothesis is that there are reflexes that
connect upper and lower respiratory function, although significant sinobronchial
reflexes are difficult to demonstrate in humans [45,46]. It has also been suggested
that pharyngobronchial reflexes can be triggered by postnasal drip of neutrophils
and inflammatory mediators to provoke acute lower airway symptoms [47,48].
There is clinical evidence that most patients with sinusitis develop a hyper-
responsiveness of the upper airway and that this upper airway hyperresponsive-
ness is often accompanied by bronchial hyperresponsiveness [47]. Furthermore,
J.E. Gern, R.F. Lemanske, Jr. / Pediatr Clin N Am 50 (2003) 555–575560

treatment of the chronic sinusitis with antibiotics and nasal corticosteroids can
improve both upper and lower airway hyperresponsiveness. These findings
suggest that postnasal drip associated with sinusitis might trigger upper airway
hyperresponsiveness and subsequently affect the lower airway through a pha-
ryngeal-pulmonary reflex. This hypothesis is consistent with reports that dem-
onstrate that treatment with intranasal corticosteroids can reduce the likelihood of
acute exacerbations of asthma [49].
Finally, some data indicate that chronic sinusitis and asthma may both be mani-
festations of a generalized inflammatory disorder of the respiratory mucosa, thus
explaining their frequent coexistence. Although there are few published studies
involving children, it is clear that the mucosal inflammation associated with
chronic sinusitis in adults resembles that of asthma. The mucosa in chronic sinus-
itis is infiltrated by eosinophils, mast cells, and T cells [50], and mucosal eosino-
philia is particularly striking in patients with asthma [51]. Other features of asthma,
such as mucosal thickening, epithelial cell damage, and increased histamine and
leukotriene levels are also found in chronic sinusitis, suggesting that common
pathogenic mechanisms underlie these two frequently associated disorders.
Can certain infections reduce the risk of developing allergies and asthma?
It has been suggested that some viral or bacterial infections might actually
protect against the subsequent development of allergies and asthma. This contro-
versial theory, termed the hygiene hypothesis, was first suggested by David
Strachan [52], who noted that the risk of developing allergies and asthma is
inversely related to the number of children in the family, an observation that has
been duplicated in a number of subsequent studies [53,54]. This finding has led to
speculation that infectious diseases, which are more likely to be transmitted in large
families, could modulate the development of the immune system in a manner to
reduce the chances of developing allergies. This hypothesis suggests that the
immune system is immature at birth; in support of this concept, experimental
evidence shows that Th1-like interferon (IFN) responses are depressed in cells from
umbilical cord blood [55]. According to the theory, each infection would provide a
stimulus for the development or activation of Th1-like immune responses. This
repetitive stimulation would lead to the development of balanced Th1-like and
Th2-like cytokine responses and, as a result, to a low risk of developing allergies. In
the absence of exposure to infectious diseases in infancy, the immune system is
skewed toward Th2-like responses, and on exposure to environmental allergens,
the risk of allergic sensitization would be increased.
During the past decade, a number of epidemiologic variables have been
evaluated in relation to the hygiene hypothesis. Presently, the evidence most
strongly supports a reduction in the incidence of allergic sensitization in
individuals from large families, particularly the youngest in the family (birth-
order effect), and in those living in a less affluent environment [56]. These
relationships are stronger for allergic sensitization than for asthma [57,58].
Whether the effects of being in a large family result from increased exposure
J.E. Gern, R.F. Lemanske, Jr. / Pediatr Clin N Am 50 (2003) 555–575 561

to infectious diseases has been evaluated in two types of studies. First, the
influence of specific infections has been related to the subsequent development of
atopic diseases. Some of the first studies suggested that infections with specific
pathogens such as measles [59] or Mycobacteria [60] were associated with lower
rates of allergen sensitization and asthma; however, these results have not been
verified in more recent studies [61,62]. There is better evidence that repeated
exposure to infectious diseases during early infancy in settings such as day care
centers may reduce the risk of allergen sensitization [63,64].
The route of infection may be important in determining long-term effects on
allergies and asthma. For example, RSV bronchiolitis seems to be a risk factor for
the development of asthma but in most studies does not promote allergic
sensitization. In contrast, infections acquired by oro-fecal transmission (eg,
hepatitis A), are associated with lower rates of allergy and asthma [65]. These
findings suggest that foodborne and fecal-oral rather than respiratory tract
transmission of infection may be a more likely determinant of the risk of allergic
sensitization during childhood.
Other epidemiologic and biologic factors that have been considered to
influence the development of allergic sensitization or asthma include early
exposure to a farming lifestyle [66,67], alterations in bacterial flora of the gut
[68], and increased antibiotic usage [69]. Furthermore, it has recently been
demonstrated that high levels of exposure to endotoxin in the home, as occurs in
farmhouses and homes with furred pets, is associated with reduced rates of
allergy and an enhanced number of IFN-producing cells in peripheral blood
[70,71]. Collectively, these studies suggest that exposure to microbes, in addition
to infections per se, may affect immune development to reduce the risk of atopy
and asthma. This concept has led to efforts to use oral administration of probiotics
(live cultures of Lactobacillus) to try to reduce the incidence of atopic diseases,
and early results look promising [72,73].
In summary, the effects of infections on the incidence of allergic disorders and
asthma are complex and are likely to depend on the specific pathogen, route of
infection or exposure, cumulative number of infections, and the age of the child
and stage of immunologic development. One other factor to consider is the
genetic makeup of the child, because polymorphisms in genes related to either the
innate or adaptive immune systems could strongly influence the immune
response to microbial products or infections and, potentially, the incidence of
allergies and asthma [74].
Mechanisms of virus-induced wheezing and asthma
Respiratory symptoms are likely to be the result of two factors: destruction of
normal airway tissue because of the direct effects of the virus, and pro-
inflammatory immune responses to the infection. For viruses such as RV, which
infect relatively few cells in the airway, the proinflammatory response may be the
primary mechanism for airway symptoms and lower airway dysfunction [75].
J.E. Gern, R.F. Lemanske, Jr. / Pediatr Clin N Am 50 (2003) 555–575562

The various components of the immune response, both antiviral and proinflam-
matory, are reviewed in the following sections.
Inflammation
Epithelial cells
The epithelial cell serves as the host cell for viral replication and also helps to
initiate antiviral responses. Damage to the epithelial cells can disturb airway
physiology through a number of different pathways. For example, epithelial
edema and shedding together with mucus production can cause airway obstruc-
tion and wheezing. Virus-induced epithelial damage can also increase the
permeability of the mucosal layer [76,77], perhaps facilitating allergen contact
with immune cells and leaving neural elements exposed.
The processes associated with viral replication trigger both innate and adaptive
immune responses within the epithelial cell. Virus attachment to cell surface
receptors may initiate some immune responses. For example, RSV infection
activates signaling pathways in airway epithelial cells through the surface
molecule toll-like receptor 4 (TLR-4) [78]. There is also evidence of receptor-
independent pathways for virus activation of epithelial cells, such as the
generation of oxidative stress [79].
Replication of viral RNA can also stimulate antiviral responses in epithelial
cells. Double-stranded RNA (dsRNA) that is synthesized in virus-infected cells
can bind to cell surface receptors and also directly activates intracellular enzymes,
such as the dsRNA-dependent protein kinase (PKR) and 2–5 oligoadenylate
synthase, which are important components of the innate antiviral immune
response [80]. Through this mechanism, viral replication induces innate antiviral
activity through the generation of nitric oxide, activation of RNase L, and
inhibition of protein synthesis within infected cells. In addition, dsRNA gen-
erated during viral infections promotes the activation of chemokine genes such
as interleukin (IL)-8 and RANTES (Regulated by Activation, Normal T cell
Expressed and Secreted), which recruit inflammatory cells into the airway [81].
Thus, host cell recognition of dsRNA is an important pathway for the initiation of
multiple and antiviral and proinflammatory pathways within the cell.
Granulocytes and mononuclear cells
During natural infection, the initial inoculum that transmits the illness is
assumed to be quite small; however, viral titers in respiratory secretions can attain
106 infectious units/mL, even after dilution by nasal lavage [82]. At this point, it
is likely that mononuclear cells are activated by these high titers of virus. As a
result, monocytes, macrophages, and, presumably, dendritic cells secrete proin-
flammatory cytokines such as IL-1, IL-8, tumor necrosis factor-alpha (TNF-a),IL-10, and IFN-a [83–85]. These cytokines activate other cells in the envir-
onment and are potent inducers of adhesion molecules. Together with chemo-
kines generated by epithelial cells, this response provides a potent stimulus for
inflammatory cell recruitment.
J.E. Gern, R.F. Lemanske, Jr. / Pediatr Clin N Am 50 (2003) 555–575 563

Acute respiratory viral infections are often accompanied by neutrophilia in
airway secretions, and products of neutrophil activation are probably involved in
obstructing the airway and causing lower airway symptoms [86,87]. Of particular
interest is evidence that activated neutrophils, through the release of the potent
secretagogue elastase, can increase goblet cell secretion of mucus [88]. In
addition, changes in IL-8 levels in nasal secretions have been related to res-
piratory symptoms and virus-induced increases in airway hyperresponsiveness
[89,90]. These findings suggest that neutrophils and neutrophil activation
products contribute to airway obstruction and symptoms during viral infections
and exacerbations of asthma.
Lymphocytes are recruited into the upper and lower airways during the early
stages of a viral respiratory infection, and it is assumed that innate and adaptive
immune responses serve to limit the extent of infection and to clear virus-infected
epithelial cells. This process is consistent with reports of severe viral lower
respiratory infections in immunocompromised patients [91].
For RSV, the G (attachment) and F (fusion) proteins are the major surface
glycoproteins against which neutralizing antibody is directed. In both murine [92]
and human [93] in vitro experiments, it has been noted that the G protein elicits a
predominant Th2 immune response, whereas the F protein and infectious RSV pro-
duce a predominant Th1 response. This property of the G protein has led to
speculation that this may be a mechanism by which RSV promotes allergen
sensitization. In murine models, RSV infections are associated with the devel-
opment of airway hyperresponsiveness [94] and an augmented allergic airway
response [95]. Some [96], but not all [97], investigators have demonstrated that
these alterations are related to increased production of the Th2-like cytokine IL-13
in the airway.
These and other animal models of respiratory viral infection suggest that
cellular immune responses and patterns of cytokine production may be related to
the outcome of respiratory infections. This same concept has been tested in a
limited number of studies involving humans. For example, reduced peripheral
blood mononuclear cell production of IFN-g both during and months following
RSV infection has been observed in only those children who develop subsequent
asthma [98]. In contrast, concentrations of IFN-g in upper airway secretions are
increased during episodes of viral-induced wheezing compared with upper
respiratory infections [99].
Additional information has been obtained by evaluating immune responses in
volunteers inoculated with a strain of RV. In these studies, strong IFN-g responsesto virus in blood mononuclear cells were associated with reduced viral shedding
[100]. In addition, stronger Th1-like response in sputum cells (higher IFNg/IL-5mRNA ratio) during induced colds was associated with milder cold symptoms and
also with more rapid clearance of the virus [82]. There is evidence that production
of IFN-g in response to viruses may be impaired in asthma [101]. Together, these
experimental findings suggest that the impaired cellular immune responses to
respiratory viruses, and reduced IFN-g production in particular, could promote
more severe clinical manifestations of viral respiratory infections in asthma.
J.E. Gern, R.F. Lemanske, Jr. / Pediatr Clin N Am 50 (2003) 555–575564

Effects of allergy
Several studies have addressed the possibility that allergic individuals may
have impaired antiviral responses and, as a result, develop more severe mani-
festations of viral respiratory infections, particularly in relationship to airway
obstruction and wheezing. In infants, several studies have evaluated whether
allergy, atopic dermatitis, or a family history of allergy increase the risk of acute
bronchiolitis during RSV epidemics [102–106]; however, these studies have
yielded conflicting results. In addition, it seems unlikely that infections with RSV
in infancy cause allergy [6,106], although this possibility, too, is a matter of
controversy [107].
Despite these uncertainties, more convincing evidence implicates respiratory
allergy as a risk factor for wheezing with common cold infections later in
childhood. In studies conducted in an emergency department, risk factors for
developing acute wheezing episodes were ascertained [25,108]. Individual risk
factors for developing wheezing included detection of a respiratory virus, most
commonly RV, positive allergen-specific IgE as detected by radioallergosorbent
testing (RAST), and evidence of eosinophilic inflammation. Viral infections and
allergic inflammation synergistically enhanced the risk of wheezing [25].
Furthermore, other studies have shown that experimental inoculation with RV
is more likely to increase airway responsiveness in allergic individuals than in
non-allergic individuals [109]. Finally, the risk of hospitalization among virus-
infected individuals is increased in patients who are both sensitized and exposed
to respiratory allergens [29]. Considered together, these findings provide strong
evidence that individuals with either respiratory allergies or eosinophilic airway
inflammation have an increased risk for wheezing with viral infections.
Viral infections may interact with allergic inflammation to promote airway
dysfunction through several mechanisms [110]. First, it has been suggested that
viruses capable of infecting lower airway epithelium may lead to enhanced
absorption of aeroallergens across the airway wall predisposing to subsequent
sensitization [111,112]. Second, viral infections may lead to mast cell mediator
release within the airway, resulting in the development of bronchospasm and
the ingress of eosinophils [113–118]. Third, airway resident and inflammatory
cell generation of various cytokines (TNF-1b, IL-1-, IL-1b IL-6) [119–122],
chemokines (macrophage inflammatory protein [MIP]-1a, RANTES, monocyte
chemotactic protein [MCP]-1, IL-8) [123,124], leukotrienes [99], and adhesion
molecules (intercellular adhesion molecule-1 [ICAM-1]) [119] may further
increase the ongoing inflammatory response.
Studies have been performed using bronchoscopy and experimental viral
inoculation to try to understand RV-induced inflammation in the lower airway
and interactions with allergen-induced inflammation. These studies have dem-
onstrated that RV infections can enhance lower airway histamine responses and
eosinophil recruitment in response to allergen challenge [125,126]. In addition,
during a RV infection, study subjects had enhanced immediate responses to
allergen and were more likely to have a late asthmatic response after allergen
J.E. Gern, R.F. Lemanske, Jr. / Pediatr Clin N Am 50 (2003) 555–575 565

challenge [127]. These findings suggest that RV can enhance both the immediate
and the late-phase response to allergen.
How do common cold infections disturb lower airway physiology?
Rhinovirus has traditionally been considered to be an upper airway pathogen
because of its association with common cold symptoms and the observation that
RV replicates best at 33� to 35�C, which approximates temperatures in the upper
airway. There is evidence to indicate that lower airway temperatures may also be
conducive to RV replication. Lower airway temperatures have been directly
mapped using a bronchoscope equipped with a thermister [128]. During quiet
breathing of air at room temperature, airway temperatures are generally lower
than 35�C down to the level of fourth generation bronchi. Moreover, RV seems to
replicate equally well in cultured epithelial cells derived from either upper or
lower airway epithelium [129]. Finally, although RV has been difficult to culture
from the lower airway, it has been detected in lower airway cells and secretions
both by reverse transcription polymerase chain reaction (RT-PCR) and in situ
hybridization of mucosal biopsies after experimental inoculation [130,131].
These findings establish that RV can replicate in the lower airway epithelium
at temperatures found in the large airway of the lung. This concept is further
supported by evidence that RV infections can produce lower airway inflam-
mation, including increased neutrophils in bronchial lavage fluid [132], influx of
T cells and eosinophils into lower airway epithelium [133], and enhanced
epithelial expression of ICAM-1 [134].
Remaining challenges include determining how much virus is present in the
lower airway and establishing whether viral replication in the lower airway is a
sufficient stimulus to provoke exacerbations of asthma. Alternate mechanisms to
explain the link between colds and increased asthma include virus-induced
systemic immune activation, the existence of reflex bronchospasm triggered by
upper airway inflammation, and the aspiration of inflammatory cells and
mediators that are generated in the upper airway [135].
Effects of viral infections on airway hyperresponsiveness
Information derived from animal models, as well as clinical studies of natural
or experimentally induced viral infections, indicate that viruses can enhance
airway hyperresponsiveness, which is one of the key features of asthma [136].
Clinical studies have generally shown that viral infections cause mild increases in
airway responsiveness during the time of peak cold symptoms and that these
changes can sometimes last for several weeks. A heightened sensitivity to inhaled
irritants and greater maximum bronchoconstriction in response to these stimuli
have been observed. The mechanism of virus-induced airway responsiveness is
likely to be multifactorial, and contributing factors are likely to include impair-
ment in the inactivation of tachykinins, virus effects on nitric oxide production,
and virus-induced changes in neural control of the airway [137].
J.E. Gern, R.F. Lemanske, Jr. / Pediatr Clin N Am 50 (2003) 555–575566

Treatment
Wheezing infants
One of the biggest challenges in treating infants who present with wheezing is to
try to differentiate RSV bronchiolitis from wheezing that is caused by early-onset
asthma. This differentiation is important, because bronchodilators produce at best
only modest short-term improvements in clinical features of mild or moderately
severe bronchiolitis and do not affect the rate or duration of hospitalization [138].
Given the high costs and uncertain benefit of this therapy, bronchodilators are not
recommended for routine management of first-time wheezers.
A meta-analysis of studies involving therapy of bronchiolitis with either oral
or parenteral corticosteroids concluded that this approach produced modest
benefits [139]. Of 12 relevant publications, 6 met the selection criteria and had
relevant data available. Corticosteroid therapy (prednisone, prednisolone, methyl-
prednisone, hydrocortisone, dexamethasone given orally, intramuscularly, or
intravenously in dose ranges of 0.6 to 6.3 mg/kg/day of prednisone equivalents)
was associated with a statistically significant reduction in clinical symptom
scores and length of hospital stay (0.4 day difference). The analysis suggested
that corticosteroid treatment might have its greatest effects in more severe cases,
and that clinical benefits are noticeable in the first 24 hours.
Several placebo-controlled trials [140–149] have addressed the question as to
whether corticosteroid treatment can prevent respiratory sequelae after RSV
bronchiolitis [8]. Seven of 10 of these trials did not show any long-term effects
(follow-up time from 6 months to 5 years) on postbronchiolitic wheezing, the
development of various wheezing phenotypes (transient, persistent, or late onset),
or a subsequent diagnosis of asthma. In the three trials that did show some
benefit, the positive effects observed were mainly over shorter time intervals
following infection.
Because elevated levels of leukotrienes have been reported in respiratory tract
secretions of infants who develop recurrent wheezing following RSV bronchiol-
itis [150,151], the effect of a leukotriene receptor antagonist in modulating these
developments recently has been evaluated. In a prospective, placebo-controlled
trial, a 28-day treatment course of montelukast significantly reduced lower
respiratory tract symptoms in infants who were hospitalized for RSV bronchiol-
itis [152]. These preliminary observations suggest a potential role of this class of
compounds in improving short-term symptom control and also in preventing
long-term lower respiratory tract sequelae.
Role of oral and inhaled corticosteroids in acute exacerbations of asthma
Numerous studies have been conducted to assess the role of systemic cortico-
steroid therapy in acute episodes of asthma in children and adults, and it is assumed
that many of these episodes are caused by viral respiratory infections. A meta-
analysis of these studies supports the early use of systemic corticosteroids in acute
J.E. Gern, R.F. Lemanske, Jr. / Pediatr Clin N Am 50 (2003) 555–575 567

exacerbations based on a reduction in the admission rate for asthma and prevention
of relapse in the outpatient treatment of exacerbations [153]. As a reflection of such
information, the most recent National Heart, Lung, and Blood Institute guidelines
for the diagnosis and management of asthma recommend the addition of cortico-
steroids for asthma exacerbations unresponsive to bronchodilators [154].
Children who experience frequent exacerbations of asthma may receive
several short courses of systemic corticosteroids during each viral season. The
potential toxicity of repeated courses of oral corticosteroids is a significant
clinical concern and has prompted studies to determine whether high doses of an
inhaled corticosteriod might be just as effective with a lower potential for side
effects. Standard treatment doses of inhaled corticosteroid do not seem to prevent
virus-induced exacerbations of asthma [155]. In contrast, treatment of at-risk
children with early signs of viral upper respiratory infection with high doses of
inhaled corticosteroid (eg, 800 to 3200 mg budesonide per day) may help prevent
acute asthma attacks [156,157]. In addition, some [158], but not all [159], studies
suggest that high-dose inhaled corticosteroids compare favorably with systemic
preparations for the treatment of acute asthma in children who present to an
emergency department. Collectively, these studies suggest that inhaled cortico-
steroids can be useful in preventing asthma symptoms induced by viral infections
under some conditions. Although they provide useful information, all these
studies are limited by small numbers of patients and do not delineate features
predictive of patients who would be expected to respond to a given therapy. In
addition, the ideal drug, dosage, delivery system, and duration of therapy remain
unclear. Improved delivery of a potent drug to the lower airway may be
associated with a more favorable clinical response.
Antiviral strategies and future directions
Influenza vaccine has been used for years as a means of preventing virus-
induced exacerbations of asthma in the winter. For RSV and RV, which are more
frequently associated with wheezing illnesses, there are still no proven and cost-
effective antiviral strategies. Several antiviral agents are in development, and a
number of antirhinovirus compounds have been tested in clinical trials. These
compounds include molecules such as soluble ICAM and capsid-binding agents
(eg, pleconaril), which either hinder RV binding to cellular receptors or inhibit
uncoating of the virus to release RNA inside the cell [160–163], and inhibitors of
RV 3C protease [164]. Whether these antiviral agents can prevent asthma
exacerbations if given at the first sign of a cold has not yet been tested.
The other potential therapeutic approach for respiratory viral infections would
be to inhibit specific proinflammatory immune responses induced by the virus.
Although glucocorticoid therapy can be effective in this regard, future studies
will determine whether more focused inhibition of specific components of virus-
induced inflammation, such as proinflammatory cytokines (eg, IL-8) or mediators
(leukotrienes, bradykinin), will be able to provide safe and effective relief from
virus-induced wheezing and asthma.
J.E. Gern, R.F. Lemanske, Jr. / Pediatr Clin N Am 50 (2003) 555–575568

References
[1] Landau LI. Bronchiolitis and asthma: are they related? Thorax 1994;49:293–6.
[2] Shay DK, Holman RC, Newman RD, et al. Bronchiolitis-associated hospitalizations among US
children, 1980–1996. JAMA 1999;282:1440–6.
[3] Openshaw PJM. Immunological mechanisms in respiratory syncytial virus disease. Springer
Semin Immunopathol 1995;17:187–201.
[4] Martinez FD, Wright AL, Taussig LM, et al. Asthma and wheezing in the first six years of life.
N Engl J Med 1995;332:133–8.
[5] Castro-Rodrıguez JA, Holberg CJ, Wright AL, et al. Association of radiologically ascertained
pneumonia before age 3 yr with asthmalike symptoms and pulmonary function during child-
hood: a prospective study. Am J Respir Crit Care Med 1999;159(6):1891–7.
[6] Stein RT, Sherrill D, Morgan WJ, et al. Respiratory syncytial virus in early life and risk of
wheeze and allergy by age 13 years. Lancet 1999;354:541–5.
[7] Kneyber MCJ, Steyerberg EW, De Groot R, et al. Long-term effects of respiratory syncytial
virus (RSV) bronchiolitis in infants and young children: a quantitative review. Acta Paediatr
2000;89(6):654–60.
[8] Wennergren G, Kristjansson S. Relationship between respiratory syncytial virus bronchiolitis
and future obstructive airway diseases. Eur Respir J 2001;18(6):1044–58.
[9] Eriksson M, Bennet R, Nilsson A. Wheezing following lower respiratory tract infections with
respiratory syncytial virus and influenza A in infancy. Pediatr Allergy Immunol 2000;11(3):
193–7.
[10] Korppi M, Reijonen T, Poysa L, et al. A 2- to 3-year outcome after bronchiolitis. Am J Dis
Child 1993;147(6):628–31.
[11] Wennergren G, Amark M, Amark K, et al. Wheezing bronchitis reinvestigated at the age of
10 years. Acta Paediatr 1997;86(4):351–5.
[12] Reijonen TM, Kotaniemi-Syrjanen A, Korhonen K, et al. Predictors of asthma three years after
hospital admission for wheezing in infancy. Pediatrics 2000;106(6):1406–12.
[13] Hogg JC. Role of latent viral infections in chronic obstructive pulmonary disease and asthma.
Am J Respir Crit Care Med 2001;164(10 Pt 2):S71–5.
[14] Von Hertzen LC. Role of persistent infection in the control and severity of asthma: focus on
Chlamydia pneumoniae. Eur Respir J 2002;19:546–56.
[15] Martin RJ, Kraft M, Chu HW, et al. A link between chronic asthma and chronic infection.
J Allergy Clin Immunol 2001;107(4):595–601.
[16] Kraft M, Cassell GH, Henson JE, et al. Detection of Mycoplasma pneumoniae in the airways of
adults with chronic asthma. Am J Respir Crit Care Med 1998;158:998–1001.
[17] Hahn DL, Dodge RW, Golubjatnikov R. Association of Chlamydia pneumoniae (strain TWAR)
infection with wheezing, asthmatic bronchitis, and adult-onset asthma. JAMA 1991;266(2):
225–30.
[18] Black PN, Blasi F, Jenkins CR, et al. Trial of Roxithromycin in subjects with asthma and
serological evidence of infection with Chlamydia pneumoniae. Am J Respir Crit Care Med
2001;164(4):536–41.
[19] Avila PC, Boushey HA. Macrolides, asthma, inflammation, and infection. Ann Allergy Asthma
Immunol 2000;84(6):565–8.
[20] Matsuse T, Hayashi S, Kuwano K, et al. Latent adenoviral infection in the pathogenesis of
chronic obstructive pulmonary disease. Am Rev Respir Dis 1992;146(1):177–84.
[21] Macek V, Sorli J, Kopriva S, et al. Persistent adenoviral infection and chronic airway obstruc-
tion in children. Am J Respir Crit Care Med 1994;150:7–10.
[22] Johnston SL, Pattemore PK, Sanderson G, et al. Community study of role of viral infections in
exacerbations of asthma in 9–11 year old children. BMJ 1995;310(6989):1225–9.
[23] Johnston SL, Pattemore PK, Sanderson G, et al. The relationship between upper respiratory
infections and hospital admissions for asthma: a time-trend analysis. Am J Respir Crit Care
Med 1996;154(3 Pt 1):654–60.
J.E. Gern, R.F. Lemanske, Jr. / Pediatr Clin N Am 50 (2003) 555–575 569

[24] Ingram JM, Rakes GP, Hoover GE, et al. Eosinophil cationic protein in serum and nasal washes
from wheezing infants and children. J Pediatr 1995;127:558–64.
[25] Rakes GP, Arruda E, Ingram JM, et al. Rhinovirus and respiratory syncytial virus in wheezing
children requiring emergency care. IgE and eosinophil analyses. Am J Respir Crit Care Med
1999;159(3):785–90.
[26] Atmar RL, Guy E, Guntupalli KK, et al. Respiratory tract viral infections in inner city asthmatic
adults. Arch Intern Med 1998;158:2453–9.
[27] Skoner DP, Doyle WJ, Seroky J, et al. Lower airway responses to rhinovirus 39 in healthy
allergic and nonallergic subjects. Eur Respir J 1996;9:1402–6.
[28] Corne JM, Marshall C, Smith S, et al. Frequency, severity, and duration of rhinovirus infections
in asthmatic and non-asthmatic individuals: a longitudinal cohort study. Lancet 2002;
359(9309):831–4.
[29] Green RM, Custovic A, Sanderson G, et al. Synergism between allergens and viruses and risk
of hospital admission with asthma: case-control study. BMJ 2002;324(7340):763.
[30] Tarlo SM, Broder I, Corey P, et al. The role of symptomatic colds in asthma exacerbations:
influence of outdoor allergens and air pollutants. J Allergy Clin Immunol 2001;108(1):52–8.
[31] Smyth AR, Smyth RL, Tong CYW, et al. Effect of respiratory virus infections including
rhinovirus on clinical status in cystic fibrosis. Arch Dis Child 1995;73:117–20.
[32] Seemungal T, Harper-Owen R, Bhowmik A, et al. Respiratory viruses, symptoms, and inflam-
matory markers in acute exacerbations and stable chronic obstructive pulmonary disease. Am J
Respir Crit Care Med 2001;164(9):1618–23.
[33] Hegele RG, Ahmad HY, Becker AB, et al. The association between respiratory viruses and
symptoms in 2-week-old infants at high risk for asthma and allergy. J Pediatr 2001;138(6):
831–7.
[34] Nicholson KG, Kent J, Hammersley V, et al. Risk factors for lower respiratory complications of
rhinovirus infections in elderly people living in the community: prospective cohort study. BMJ
1996;313:1119–23.
[35] Grupp-Phelan J, Lozano P, Fishman P. Health care utilization and cost in children with asthma
and selected comorbidities. J Asthma 2001;38(4):363–73.
[36] Rachelefsky GS, Katz RM, Siegel SC. Chronic sinus disease with associated reactive airway
disease in children. Pediatr 1984;73:526–9.
[37] Friedman R, Ackerman M, Wald E, et al. Asthma and bacterial sinusitis in children. J Allergy
Clin Immunol 1984;74(2):185–9.
[38] Goldenhersh MJ, Rachelefsky GS, Dudley J, et al. The microbiology of chronic sinus disease in
children with respiratory allergy. J Allergy Clin Immunol 1990;85:1030–9.
[39] Wald ER. Microbiology of acute and chronic sinusitis in children. J Allergy Clin Immunol
1992;90(3 Pt 2):452–6.
[40] Wald ER, Milmoe GJ, Bowen A, et al. Acute maxillary sinusitis in children. N Engl J Med
1981;304:749–54.
[41] Hamilos DL. Gastroesophageal reflux and sinusitis in asthma. Clin Chest Med 1995;16:683–97.
[42] McFadden Jr. ER. Nasal-sinus-pulmonary reflexes and bronchial asthma [editorial]. J Allergy
1986;78:1–3.
[43] Irvin CG. Sinusitis and asthma: an animal model. J Allergy Clin Immunol 1992;90:521–33.
[44] Brugman SM, Larsen GL, Henson PM, et al. Increased lower airways responsiveness associated
with sinusitis in a rabbit model. Am Rev Respir Dis 1993;147:314–20.
[45] Littell NT, Carlisle CC, Millman RP, et al. Changes in airway resistance following nasal
provocation. Am Rev Respir Dis 1990;141:580–3.
[46] Sato T. Effect of nasal mucosal irritation on airway resistance. Auris Nasus Larynx 1980;7:
39–50.
[47] Bucca C, Rolla G, Scappaticci E, et al. Extrathoracic and intrathoracic airway responsiveness in
sinusitis. J Allergy Clin Immunol 1995;95(1 Pt 1):52–9.
[48] Bucca C, Rolla G, Brussino L, et al. Are asthma-like symptoms due to bronchial or extra-
thoracic airway dysfunction? [see comments]. Lancet 1995;346(8978):791–5.
J.E. Gern, R.F. Lemanske, Jr. / Pediatr Clin N Am 50 (2003) 555–575570

[49] Adams RJ, Fuhlbrigge AL, Finkelstein JA, et al. Intranasal steroids and the risk of emergency
department visits for asthma. J Allergy Clin Immunol 2002;109(4):636–42.
[50] Demoly P, Crampette L, Mondain M, et al. Assessment of inflammation in noninfectious
chronic maxillary sinusitis. J Allergy Clin Immunol 1994;94:95–108.
[51] Harlin SL, Ansel DG, Lane SR, et al. A clinical and pathologic study of chronic sinusitis: the
role of the eosinophil. J Allergy Clin Immunol 1988;81:867–75.
[52] Strachan DP. Hay fever, hygiene, and household size. BMJ 1989;299:1259–60.
[53] von Mutius E, Martinez FD, Fritzsch C, et al. Skin test reactivity and number of siblings. BMJ
1994;308:692–5.
[54] von Mutius E. The influence of birth order on the expression of atopy in families: a gene-
environment interaction? Clin Exp Allergy 1998;28(12):1454–6.
[55] Prescott SL, Macaubas C, Smallacombe T, et al. Development of allergen-specific T-cell
memory in atopic and normal children. Lancet 1999;353(9148):196–200.
[56] Strachan DP. Family size, infection and atopy: the first decade of the ‘‘hygiene hypothesis’’.
Thorax 2000;55(Suppl 1):S2–10.
[57] Lewis S, Butland B, Strachan D, et al. Study of the aetiology of wheezing illness at age 16 in
two national British birth cohorts. Thorax 1996;51(7):670–6.
[58] Butland BK, Strachan DP, Lewis S, et al. Investigation into the increase in hay fever and eczema
at age 16 observed between the 1958 and 1970 British birth cohorts. BMJ 1997;315(7110):
717–21.
[59] Shaheen SO, Aaby P, Hall AJ, et al. Measles and atopy in Guinea-Bissau. Lancet 1996;347:
1792–6.
[60] Shirakawa T, Enomoto T, Shimazu S, et al. The inverse association between tuberculin re-
sponses and atopic disorder. Science 1997;275:77–9.
[61] Strannegard IL, Larsson LO, Wennergren G, et al. Prevalence of allergy in children in relation to
prior BCG vaccination and infection with atypical mycobacteria. Allergy 1998;53(3):249–54.
[62] Paunio M, Heinonen OP, Virtanen M, et al. Measles history and atopic diseases: a population-
based cross-sectional study [see comments]. JAMA 2000;283(3):343–6.
[63] Ball TM, Castro-Rodrıguez JA, Griffith KA, et al. Siblings, day-care attendance, and the risk of
asthma and wheezing during childhood. N Engl J Med 2000;343:538–43.
[64] Oddy WH, de Klerk NH, Sly PD, et al. The effects of respiratory infections, atopy, and
breastfeeding on childhood asthma. Eur Respir J 2002;19(5):899–905.
[65] Matricardi PM, Rosmini F, Ferrigno L, et al. Cross sectional retrospective study of prevalence
of atopy among Italian military students with antibodies against hepatitis A virus. BMJ 1997;
314(7086):999–1003.
[66] von Mutius E. The increase in asthma can be ascribed to cleanliness. Am J Respir Crit Care
Med 2001;164(7):1106–7.
[67] von Mutius E. Infection: friend or foe in the development of atopy and asthma? The epidemio-
logical evidence. Eur Respir J 2001;18(5):872–81.
[68] Bjorksten B, Naaber P, Sepp E, et al. The intestinal microflora in allergic Estonian and Swedish
2-year-old children. Clin Exp Allergy 1999;29(3):342–6.
[69] Hopkin JM. Early life receipt of antibiotics and atopic disorder. Clin Exp Allergy 1999;
29(6):733–4.
[70] Gereda JE, Leung DY, Liu AH. Levels of environmental endotoxin and prevalence of atopic
disease. JAMA 2000;284(13):1652–3.
[71] Gereda JE, Leung DY, Thatayatikom A, et al. Relation between house-dust endotoxin exposure,
type 1 T-cell development, and allergen sensitisation in infants at high risk of asthma. Lancet
2000;355(9216):1680–3.
[72] Rautava S, Kalliomaki M, Isolauri E. Probiotics during pregnancy and breast-feeding might
confer immunomodulatory protection against atopic disease in the infant. J Allergy Clin Im-
munol 2002;109(1 Pt 1):119–21.
[73] Kalliomaki M, Salminen S, Arvilommi H, et al. Probiotics in primary prevention of atopic
disease: a randomised placebo-controlled trial. Lancet 2001;357(9262):1076–9.
J.E. Gern, R.F. Lemanske, Jr. / Pediatr Clin N Am 50 (2003) 555–575 571

[74] Vercelli D. The functional genomics of CD14 and its role in IgE responses: an integrated view.
J Allergy Clin Immunol 2002;109(1 Pt 1):14–21.
[75] Hendley JO. The host response, not the virus, causes the symptoms of the common cold. Clin
Infect Dis 1998;26(4):847–8.
[76] Igarashi Y, Skoner DP, Doyle WJ, et al. Analysis of nasal secretions during experimental
rhinovirus upper respiratory infections. J Allergy Clin Immunol 1993;92:722–31.
[77] Ohrui T, Yamaya M, Sekizawa K, et al. Effects of rhinovirus infection on hydrogen peroxide-
induced alterations of barrier function in the cultured human tracheal epithelium. Am J Respir
Crit Care Med 1998;158(1):241–8.
[78] Kurt-Jones EA, Popova L, Kwinn L, et al. Pattern recognition receptors TLR4 and CD14
mediate response to respiratory syncytial virus. Nat Immunol 2000;1(5):398–401.
[79] Kaul P, Biagioli MC, Singh I, et al. Rhinovirus-induced oxidative stress and interleukin-8
elaboration involves p47-phox but is independent of attachment to intercellular adhesion mol-
ecule-1 and viral replication. J Infect Dis 2000;181:1885–90.
[80] Williams BRG. PKR: a sentinel kinase for cellular stress. Oncogene 1999;18:6112–20.
[81] Konno S, Grindle KA, Lee WM, et al. Interferon-gamma enhances rhinovirus-induced
RANTES secretion by airway epithelial cells. Am J Respir Cell Mol Biol 2002;26(5):594–601.
[82] Gern JE, Vrtis R, Grindle KA, et al. Relationship of upper and lower airway cytokines to
outcome of experimental rhinovirus infection. Am J Respir Crit Care Med 2000;162:2226–31.
[83] Gern JE, Vrtis R, Kelly EAB, et al. Rhinovirus produces nonspecific activation of lymphocytes
through a monocyte-dependent mechanism. J Immunol 1996;157:1605–12.
[84] Panuska JR, Merolla R, Rebert NA, et al. Respiratory syncytial virus induces interleukin-10 by
human alveolar macrophages. Suppression of early cytokine production and implications for
incomplete immunity. J Clin Invest 1995;96:2445–53.
[85] Johnston SL, Papi A, Monick MM, et al. Rhinoviruses induce interleukin-8 mRNA and protein
production in human monocytes. J Infect Dis 1997;175(2):323–9.
[86] Gern JE, Busse WW. Relationship of viral infections to wheezing illnesses and asthma. Nat Rev
Immunol 2002;2(2):132–8.
[87] McNamara PS, Smyth RL. The pathogenesis of respiratory syncytial virus disease in childhood.
Br Med Bull 2002;61:13–28.
[88] Cardell LO, Agusti C, Takeyama K, et al. LTB(4)-induced nasal gland serous cell secretion
mediated by neutrophil elastase. Am J Respir Crit Care Med 1999;160(2):411–4.
[89] Grunberg K, Timmers MC, Smits HH, et al. Effect of experimental rhinovirus 16 colds on
airway hyperresponsiveness to histamine and interleukin-8 in nasal lavage in asthmatic subjects
in vivo. Clin Exp Allergy 1997;27:36–45.
[90] Gern JE, Martin MS, Anklam KA, et al. Relationships among specific viral pathogens, virus-
induced interleukin-8, and respiratory symptoms in infancy. Pediatr Allergy Immunol 2002;13:
386–93.
[91] Malcolm E, Arruda E, Hayden FG, et al. Clinical features of patients with acute respiratory
illness and rhinovirus in their bronchoalveolar lavages. J Clin Virol 2001;21(1):9–16.
[92] Alwan WH, Record FM, Openshaw PJM. Phenotypic and functional characterization of T cell
lines specific for individual respiratory syncytial virus proteins. J Immunol 1993;150:5211–8.
[93] Jackson M, Scott R. Different patterns of cytokine induction in cultures of respiratory syncytial
(RS) virus-specific human TH cell lines following stimulation with RS virus and RS virus
proteins. J Med Virol 1996;49:161–9.
[94] Peebles Jr. RS, Sheller JR, Johnson JE, et al. Respiratory syncytial virus infection prolongs
methacholine-induced airway hyperresponsiveness in ovalbumin-sensitized mice. J Med Virol
1999;57:186–92.
[95] Lukacs NW, Tekkanat KK, Berlin A, et al. Respiratory syncytial virus predisposes mice to
augmented allergic airway responses via il-13-mediated mechanisms. J Immunol 2001;
167(2):1060–5.
[96] Tekkanat KK, Maassab HF, Cho DS, et al. IL-13-induced airway hyperreactivity during respi-
ratory syncytial virus infection is STAT6 dependent. J Immunol 2001;166(5):3542–8.
J.E. Gern, R.F. Lemanske, Jr. / Pediatr Clin N Am 50 (2003) 555–575572

[97] Peebles Jr. RS, Sheller JR, Collins RD, et al. Respiratory syncytial virus infection does not
increase allergen-induced type 2 cytokine production, yet increases airway hyperresponsiveness
in mice. J Med Virol 2001;63(2):178–88.
[98] Renzi PM, Turgeon JP, Marcotte JE, et al. Reduced interferon-g production in infants with
bronchiolitis and asthma. Am J Respir Crit Care Med 1999;159:1417–22.
[99] van Schaik SM, Tristram DA, Nagpal IS, et al. Increased production of IFN-g and cysteinyl
leukotrienes in virus-induced wheezing. J Allergy Clin Immunol 1999;103:630–6.
[100] Parry DE, Busse WW, Sukow KA, et al. Rhinovirus-induced PBMC responses and outcome of
experimental infection in allergic subjects. J Allergy Clin Immunol 2000;105:692–8.
[101] Papadopoulos NG, Stanciu LA, Papi A, et al. A defective type 1 response to rhinovirus in
atopic asthma. Thorax 2002;57(4):328–32.
[102] Laing I, Riedel F, Yap PL, et al. Atopy predisposing to acute bronchiolitis during an epidemic
of respiratory syncytial virus. B Med J 1982;284:1070–2.
[103] Rooney JC, Williams HE. The relationship between proved viral bronchiolitis and subsequent
wheezing. J Pediatr 1971;79:744–7.
[104] Zweiman B, Schoenwetter WF, Pappano JE, et al. Patterns of allergic respiratory disease in
children with a past history of bronchiolitis. J Allergy Clin Immunol 1971;48:283–9.
[105] Pullan CR, Hey EN. Wheezing, asthma, and pulmonary dysfunction 10 years after infection
with respiratory syncytial virus in infancy. BMJ 1982;284:1665–9.
[106] Murray M, Webb MS, O’Callaghan C, et al. Respiratory status and allergy after bronchiolitis.
Arch Dis Child 1992;67:482–7.
[107] Sigurs N, Bjarnason R, Sigurbergsson F, et al. Asthma and immunoglobulin E antibodies after
respiratory syncytial virus bronchiolitis: a prospective cohort study with matched controls.
Pediatrics 1995;95:500–5.
[108] Duff AL, Pomeranz ES, Gelber LE, et al. Risk factors for acute wheezing in infants and children:
viruses, passive smoke, and IgE antibodies to inhalant allergens. Pediatrics 1993;92:535–40.
[109] Gern JE, Calhoun W, Swenson C, et al. Rhinovirus infection preferentially increases lower
airway responsiveness in allergic subjects. Am J Respir Crit Care Med 1997;155:1872–6.
[110] Welliver RC. Immunologic mechanisms of virus-induced wheezing and asthma. J Pediatr 1999;
135:S14–20.
[111] Sakamoto M, Ida S, Takishima T. Effect of influenza virus infection on allergic sensitization to
aerosolized ovalbumin in mice. J Immunol 1984;132(5):2614–7.
[112] Freihorst J, Piedra PA, Okamoto Y, et al. Effect of respiratory syncytial virus infection on the
uptake of and immune response to other inhaled antigens. Proc Soc Exp Biol Med 1988;
188:191–7.
[113] Garofalo R, Kimpen JLL, Welliver RC, et al. Eosinophil degranulation in the respiratory tract
during naturally acquired respiratory syncytial virus infection. J Pediatr 1992;120:28–32.
[114] Kimpen JLL, Garofalo R, Welliver RC, et al. Activation of human eosinophils in vitro by
respiratory syncytial virus. Pediatr Res 1992;32:160–4.
[115] Volovitz B, Welliver RC, De Castro G, et al. The release of leukotrienes in the respiratory tract
during infection with respiratory syncytial virus: role in obstructive airway disease. Pediatr Res
1988;24:504–7.
[116] Welliver RC, Sun M, Rinaldo D, et al. Predictive value of respiratory syncytial virus-specific
IgE responses for recurrent wheezing following bronchiolitis. J Pediatr 1986;109:776–80.
[117] Welliver RC, Wong DT, Sun M, et al. The development of respiratory syncytial virus-specific
IgE and the release of histamine in nasopharyngeal secretions after infection. N Engl J Med
1981;305:841–6.
[118] Rabatic S, Gagro A, Lokar-Kolbas R, et al. Increase in CD23 + cells in infants with bronchio-
litis is accompanied by appearance of IgE and IgG4 antibodies specific for respiratory syncytial
virus. J Infect Dis 1997;175(1):32–7.
[119] Patel JA, Kunimoto M, Sim TC, et al. Interleukin-1a mediates the enhanced expression of
intercellular adhesion molecule-1 in pulmonary epithelial cells infected with respiratory syn-
cytial virus. Am J Respir Cell Mol Biol 1995;13:602–9.
J.E. Gern, R.F. Lemanske, Jr. / Pediatr Clin N Am 50 (2003) 555–575 573

[120] Arnold R, Konig B, Galatti H, et al. Cytokine (IL-8, IL-6, TNF-a) and soluble TNF receptor-I
release from human peripheral blood mononuclear cells after respiratory syncytial virus infec-
tion. Immunology 1995;85:364–72.
[121] Tsutsumi H, Matsuda K, Sone S, et al. Respiratory syncytial virus-induced cytokine production
by neonatal macrophages. Clin Exp Immunol 1996;106(3):442–6.
[122] Takeuchi R, Tsutsumi H, Osaki M, et al. Respiratory syncytial virus infection of neonatal
monocytes stimulates synthesis of interferon regulatory factor 1 and interleukin-1b (IL-1b)-converting enzyme and secretion of IL-1b. J Virol 1998;72:837–40.
[123] Olszewska-Pazdrak B, Casola A, Saito T, et al. Cell-specific expression of RANTES, MCP-1,
and MIP-1a by lower airway epithelial cells and eosinophils infected with respiratory syncytial
virus. J Virol 1998;72(6):4756–64.
[124] Harrison AM, Bonville CA, Rosenberg HF, et al. Respiratory syncytial virus-induced chemo-
kine expression in the lower airways: eosinophil recruitment and degranulation. Am J Respir
Crit Care Med 1999;159:1918–24.
[125] Calhoun WJ, Swenson CA, Dick EC, et al. Experimental rhinovirus 16 infection potentiates
histamine release after antigen bronchoprovocation in allergic subjects. Am Rev Respir Dis
1991;144:1267–73.
[126] Calhoun WJ, Dick EC, Schwartz LB, et al. A common cold virus, rhinovirus 16, potentiates
airway inflammation after segmental antigen bronchoprovocation in allergic subjects. J Clin
Invest 1994;94:2200–8.
[127] Lemanske Jr. RF, Dick EC, Swenson CA, et al. Rhinovirus upper respiratory infection increases
airway hyperreactivity and late asthmatic reactions. J Clin Invest 1989;83:1–10.
[128] McFadden Jr. ER. Improper patient techniques with metered dose inhalers: clinical conse-
quences and solutions to misuse. J Allergy Clin Immunol 1995;96:278–83.
[129] Mosser AG, Brockman-Schneider RA, Amineva SP, et al. Similar frequency of rhinovirus-
infectable cells in upper and lower airway epithelium. J Infect Dis 2002;185:734–43.
[130] Gern JE, Galagan DM, Jarjour NN, et al. Detection of rhinovirus RNA in lower airway cells
during experimentally induced infection. Am J Respir Crit Care Med 1997;155:1159–61.
[131] Papadopoulos NG, Bates PJ, Bardin PG, et al. Rhinoviruses infect the lower airways. J Infect
Dis 2000;181(6):1875–84.
[132] Jarjour NN, Gern JE, Kelly EAB, et al. The effect of an experimental rhinovirus 16 infection on
bronchial lavage neutrophils. J Allergy Clin Immunol 2000;105(6):1169–77.
[133] Fraenkel DJ, Bardin PG, Sanderson G, et al. Lower airways inflammation during rhi-
novirus colds in normal and asthmatic subjects. Am J Respir Crit Care Med 1995;151:
879–86.
[134] Grunberg K, Sharon RF, Hiltermann TJN, et al. Experimental rhinovirus 16 infection increases
intercellular adhesion molecule-1 expression in bronchial epithelium of asthmatics regardless of
inhaled steroid treatment. Clin Exp Allergy 2000;30(7):1015–23.
[135] Bardin PG, Johnston SL, Pattemore PK. Viruses as precipitants of asthma symptoms. II.
Physiology and mechanisms. Clin Exp Allergy 1992;22:809–22.
[136] Folkerts G, Busse WW, Nijkamp FP, et al. State of the art: virus-induced airway hyperrespon-
siveness and asthma. Am J Respir Crit Care Med 1998;157:1708–20.
[137] Jacoby DB. Virus-induced asthma attacks. JAMA 2002;287(6):755–61.
[138] Kellner JD, Ohlsson A, Gadomski AM, et al. Bronchodilators for bronchiolitis. Cochrane
Database Syst Rev 2000;(2):CD001266.
[139] Garrison MM, Christakis DA, Harvey E, et al. Systemic corticosteroids in infant bronchiolitis:
a meta-analysis. Pediatrics 2000;105(4):E44.
[140] Bulow SM, Nir M, Levin E, et al. Prednisolone treatment of respiratory syncytial virus in-
fection: a randomized controlled trial of 147 infants. Pediatrics 1999;104(6):e77.
[141] van Woensel JB, Kimpen JL, Sprikkelman AB, et al. Long-term effects of prednisolone in the
acute phase of bronchiolitis caused by respiratory syncytial virus. Pediatr Pulmonol 2000;30(2):
92–6.
[142] Cade A, Brownlee KG, Conway SP, et al. Randomised placebo controlled trial of nebulised
J.E. Gern, R.F. Lemanske, Jr. / Pediatr Clin N Am 50 (2003) 555–575574

corticosteroids in acute respiratory syncytial viral bronchiolitis. Arch Dis Child 2000;82(2):
126–30.
[143] Richter H, Seddon P. Early nebulized budesonide in the treatment of bronchiolitis and the
prevention of postbronchiolitic wheezing. J Pediatr 1998;132(5):849–53.
[144] Fox GF, Everard ML, Marsh MJ, et al. Randomized controlled trial of budesonide for the
prevention of post-bronchiolitis wheezing. Arch Dis Child 1999;30:343–7.
[145] Reijonen TM, Korppi M. One-year follow-up of young children hospitalized for wheezing: the
influence of early anti-inflammatory therapy and risk factors for subsequent wheezing and
asthma. Pediatr Pulmonol 1998;26(2):113–9.
[146] Reijonen TM, Kotaniemi-Syrjanen A, Korhonen K, et al. Predictors of asthma three years after
hospital admission for wheezing in infancy. Pediatrics 2000;106:1406–12.
[147] Kajosaari M, Syvanen P, Forars M, et al. Inhaled corticosteroids during and after respiratory
syncytial virus-bronchiolitis may decrease subsequent asthma. Pediatr Allergy Immunol 2000;
11(3):198–202.
[148] Carlsen KH, Leegaard J, Larsen S, et al. Nebulised beclomethasone dipropionate in recurrent
obstructive episodes after acute bronchiolitis. Arch Dis Child 1988;63(12):1428–33.
[149] Reijonen T, Korppi M, Kuikka L, et al. Anti-inflammatory therapy reduces wheezing after
bronchiolitis. Arch Pediatr Adolesc Med 1996;150(5):512–7.
[150] Garofalo R, Welliver RC, Ogra PL. Concentrations of LTB4, LTC4, LTD4, and LTE4 in bron-
chiolitis due to respiratory syncytial virus. Allergy 1991;2:30–7.
[151] van Schaik SM, Tristram DA, Nagpal IS, et al. Increased production of IFN-g and cysteinyl
leukotrienes in virus-induced wheezing. J Allergy Clin Immunol 1999;103:630–6.
[152] Bisgaard H. A randomized trial of montelukast in respiratory syncytial virus post-bronchiolitis.
Am J Respir Crit Care Med 2003:167:379–83.
[153] Rowe BH, Keller JL, Oxman AD. Effectiveness of steroid therapy in acute exacerbations of
asthma: a meta-analysis. Am J Emerg Med 1992;10(4):301–10.
[154] National Asthma Education and Prevention Program, National Heart, Lung and Blood Institute,
National Institutes of Health. Guidelines for the diagnosis and management of asthma. Update
on selected topics 2002. J Allergy Clin Immunol 2002;110:S141–209.
[155] Doull IJM, Lampe FC, Smith S, et al. Effect of inhaled corticosteroids on episodes of wheezing
associated with viral infection in school age children: randomized double blind placebo con-
trolled trial. BMJ 1997;315:858–62.
[156] Connett G, Lenney W. Prevention of viral induced asthma attacks using inhaled budesonide.
Arch Dis Child 1993;68(1):85–7.
[157] Svedmyr J, Nyberg E, Asbrink-Nilsson E, et al. Intermittent treatment with inhaled steroids for
deterioration of asthma due to upper respiratory tract infections. Acta Paediatr 1995;84(8):884–8.
[158] Volovitz B, Bentur L, Finkelstein Y, et al. Effectiveness and safety of inhaled corticosteroids in
controlling acute asthma attacks in children who were treated in the emergency department: a
controlled comparative study with oral prednisone. J Allergy Clin Immunol 1998;102:605–9.
[159] Schuh S, Reisman J, Alshehri M, et al. A comparison of inhaled fluticasone and oral prednisone
for children with severe acute asthma. N Engl J Med 2000;343(10):689–94.
[160] Rotbart HA. Pleconaril treatment of enterovirus and rhinovirus infections. Infect Med
2000;17(7):488–94.
[161] Rotbart HA. Treatment of picornavirus infections. Antiviral Res 2002;53:83–98.
[162] Turner RB, Dutko FJ, Goldstein NH, et al. Efficacy of oral WIN 54954 for prophylaxis of
experimental rhinovirus infection. Antimicrob Agents Chemother 1993;37:297–300.
[163] Turner RB, Wecker MT, Pohl G, et al. Efficacy of tremacamra, a soluble intercellular adhesion
molecule 1, for experimental rhinovirus infection–a randomized clinical trial. JAMA 1999;
281(19):1797–804.
[164] Patick AK, Binford SL, Brothers MA, et al. In vitro antiviral activity of AG7088, a potent
inhibitor of human rhinovirus 3C protease. Antimicrob Agents Chemother 1999;43(10):
2444–50.
J.E. Gern, R.F. Lemanske, Jr. / Pediatr Clin N Am 50 (2003) 555–575 575