Embed Size (px)
Citation preview
40 ostomy wound management® july 2012 www.o-wm.com
Feature
the management of Intravenous Infiltration Injuries in Infants and ChildrenTerry Treadwell, MD, FACS
abstractThe intravenous administration of fluids and medications is critical for the treatment of seriously ill patients. Unfortu-nately, especially in infants and children, fluid infiltration into the surrounding tissue can occur. Early recognition and prompt treatment usually limits the extent of tissue damage. Early treatment may include the injection or application of medication (eg, hyaluronidase, phentolamine, or nitroglycerin ointment) and appropriate dressings. Research to guide the care of more extensive extravasation injury remains limited. At the author’s institution, the protocol of care for chil-dren and infants with extensive tissue damage and necrotic tissue consists of careful debridement followed by the use of oxidized regenerative cellulose (ORC)/collagen dressings and skin replacement if needed. Research to help clinicians develop evidence-based protocols of care for both minor and more severe intravenous fluid infiltration or extravasation injury is needed.
Keywords: IV infiltration, infants, children, wounds, extravasation
Index: Ostomy Wound Management 2012;58(7):40–44
Potential Conflicts of Interest: none disclosed
Dr. Treadwell is Medical Director, Institute for Advanced Wound Care, Baptist Medical Center, Montgomery, AL. Please address correspondence to: Terry Treadwell, MD, FACS, Institute for Advanced Wound Care, Baptist Medical Center, 2167 Normandie Drive, Montgomery, AL 36111; email: [email protected].
the intravenous route of administering blood, fluid, and medications to patients is a relatively recent
phenomenon that provides rapid effect of the fluid or medication without the problems of absorption from the gastrointestinal tract and the uncertainty of giving medi-cation via the intramuscular route.1 the first recorded intravenous administration of blood to man was done by jean-Baptiste denis on june 15, 1667.2,3 due to political issues and the fact that the different blood types and an-ticoagulation were not well understood, the transfusion of blood did not become acceptable until the early 20th century. the first intravenous administration of saline was performed in the 1830s, but it did not become com-mon practice until the early 1900s.4 not until medication was sufficiently pure was intravenous administration considered reasonable.1 unfortunately, complications soon followed; most were found to be related to delivery of the fluid and/or medication into the subcutaneous tis-sues instead of the vein.
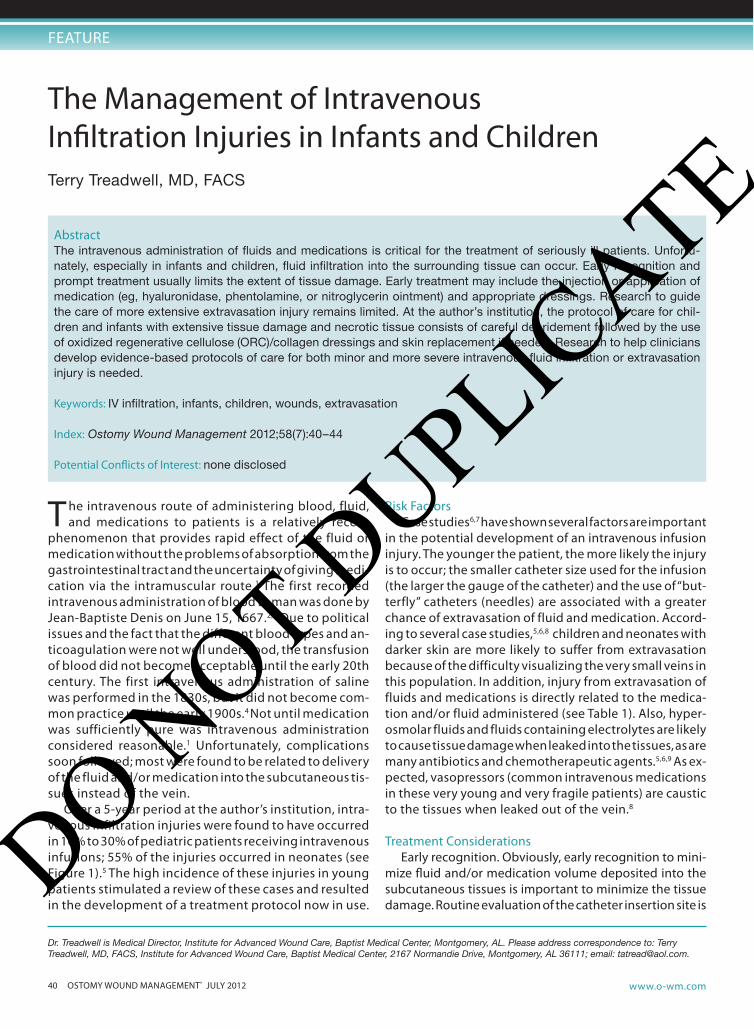
over a 5-year period at the author’s institution, intra-venous infiltration injuries were found to have occurred in 10% to 30% of pediatric patients receiving intravenous infusions; 55% of the injuries occurred in neonates (see Figure 1).5 the high incidence of these injuries in young patients stimulated a review of these cases and resulted in the development of a treatment protocol now in use.
risk FactorsCase studies6,7 have shown several factors are important
in the potential development of an intravenous infusion injury. the younger the patient, the more likely the injury is to occur; the smaller catheter size used for the infusion (the larger the gauge of the catheter) and the use of “but-terfly” catheters (needles) are associated with a greater chance of extravasation of fluid and medication. accord-ing to several case studies,5,6,8 children and neonates with darker skin are more likely to suffer from extravasation because of the difficulty visualizing the very small veins in this population. In addition, injury from extravasation of fluids and medications is directly related to the medica-tion and/or fluid administered (see table 1). also, hyper-osmolar fluids and fluids containing electrolytes are likely to cause tissue damage when leaked into the tissues, as are many antibiotics and chemotherapeutic agents.5,6,9 as ex-pected, vasopressors (common intravenous medications in these very young and very fragile patients) are caustic to the tissues when leaked out of the vein.8
treatment Considerationsearly recognition. obviously, early recognition to mini-
mize fluid and/or medication volume deposited into the subcutaneous tissues is important to minimize the tissue damage. routine evaluation of the catheter insertion site is
DO NOT D
UPLICATE
july 2012 ostomy wound management® 41www.o-wm.com
Intravenous InFIltratIon InjurIes
critical for the early recognition of the problem. once the prob-lem is noted, the infusion should be discontinued immediately and moved to another site if needed. If the catheter is still in the sub-cutaneous tissues, the author rec-ommends aspirating through the catheter to remove as much resid-ual fluid as possible. the catheter then is removed.
elevation. elevating the limb can result in more exten-sive spreading of the toxic mate-rial through the tissue and is not recommended.8 although this approach goes against current thinking, the author has observed less tissue damage.
temperature. Case studies7 have shown the use of warm or cold compresses to be controver-sial. the conventional idea is that warm compresses cause vasodila-tation in the tissues, increasing the blood flow and thus resulting in faster removal of the toxic mate-rial. Heat actually may cause more injury to the damaged tissues by increasing the tissue demands for oxygen. Heat is beneficial only for the treatment of extravasation of hypertonic saline solutions. Cold
• All intravenously administered medications and fluids• Hyperosmolar solutions (total parenteral nutrition
solutions, hypertonic glucose, hypertonic saline)• Blood• Electrolytes (calcium, potassium)• Vasopressors (dopamine, dobutamine, norepineph-
rine, epinephrine)• Mannitol• Digoxin• All antibiotics (especially tetracyclines, penicillin,
vancomycin)• Aminophylline• Phenytoin • All sedative-type medications (sodiumthiopental,
diazepam, chlordiazepoxide)• All chemotherapeutic agents
table 1. medications and fluids likely to cause tissue damage following extravasation5,6,8
Figure 1. Intravenous infiltration injuries in infants. A. Intravenous infiltration of saline on the scalp; B Intravenous infiltration of dopamine infusion.
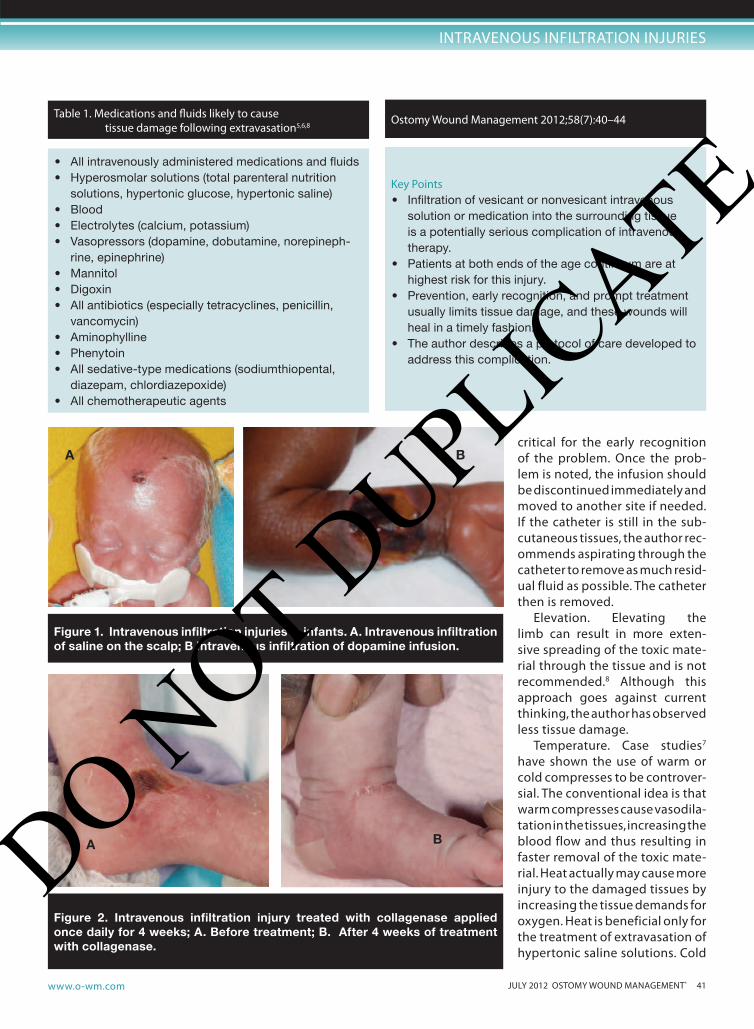
Figure 2. Intravenous infiltration injury treated with collagenase applied once daily for 4 weeks; A. Before treatment; B. After 4 weeks of treatment with collagenase.
A B
BA
Key Points• Infiltration of vesicant or nonvesicant intravenous
solution or medication into the surrounding tissue is a potentially serious complication of intravenous therapy.
• Patients at both ends of the age continuum are at highest risk for this injury.
• Prevention, early recognition, and prompt treatment usually limits tissue damage, and these wounds will heal in a timely fashion.
• The author describes a protocol of care developed to address this complication.
ostomy wound management 2012;58(7):40–44
DO NOT D
UPLICATE
42 ostomy wound management® july 2012 www.o-wm.com
Feature
compresses often are thought beneficial by causing vaso-constriction and preventing the spread of the toxic ma-terial. However, the vasoconstrictive effect of cold causes the tissue to become ischemic and makes most infusion injuries worse.10
medications. according to a review of the literature,11
certain medications have been found beneficial in extrav-asation injuries.11 one is hyaluronidase, an enzyme that allows the infiltrated fluid to diffuse through the tissues. Its effects last 24 to 48 hours. the medication should be diluted to 15 units/ml; 1 ml is injected into the tissues either through the catheter, if still present, or subcutane-ously. It is most effective if used within the first 2 hours
post-infiltration, but has been found beneficial if given up to 12 hours after infiltration.7,11 the injuries that re-spond well to hyaluronidase are listed in table 2.
Phentolamine is beneficial for use following infiltra-tion of medications causing vasoconstriction.11 this va-sodilator improves blood flow to the area to facilitate re-moval of the toxic medication and to protect the damaged tissue. the dose is 0.1 to 0.2 mg/Kg to a maximum of 10 mg given through the catheter or subcutaneously. It is ef-fective up to 12 hours after the infiltration.7,10 It should not be given to premature infants, and all patients should be monitored for hypotension and tachycardia.10 the in-juries best treated with phentolamine are listed in table 3.
nitroglycerin also has been found to be beneficial fol-lowing infiltration of medications causing vasoconstric-tion.11 It also causes vasodilatation of local vessels, im-proving blood flow to the area and facilitating removal of the toxic medication and increasing the blood flow to the injured tissues. only small amounts should be used, and care should be taken because of the possibility of hy-potension and tachycardia.5 the injuries best treated with nitroglycerin ointment are listed in table 4.
dressings. the area of injury should be protected with a nonadherent dressing and followed closely. many of these injuries will be self-limited and resolve with no further treatment.
debridement. tissue necrosis can occur as a result of the tissue damage; in such cases, the author recommends using the enzymatic debriding agent collagenase to re-move the eschar. In vivo research12, and a review of the literature13 have shown that collagenase does not damage normal tissue, making it a good treatment choice. al-though experience using this product in this age group is limited, the author has found it to be a useful and safe alternative for these patients (see Figure 2).
In the author’s experience, aggressive sharp debride-ment in these very small and delicate patients can result in more tissue damage. However, as the eschar loosens, sharp debridement can be used to completely remove only the necrotic tissue. If a significant amount of tissue has been lost, a practitioner familiar with children and neonates should be consulted for sharp debridement.
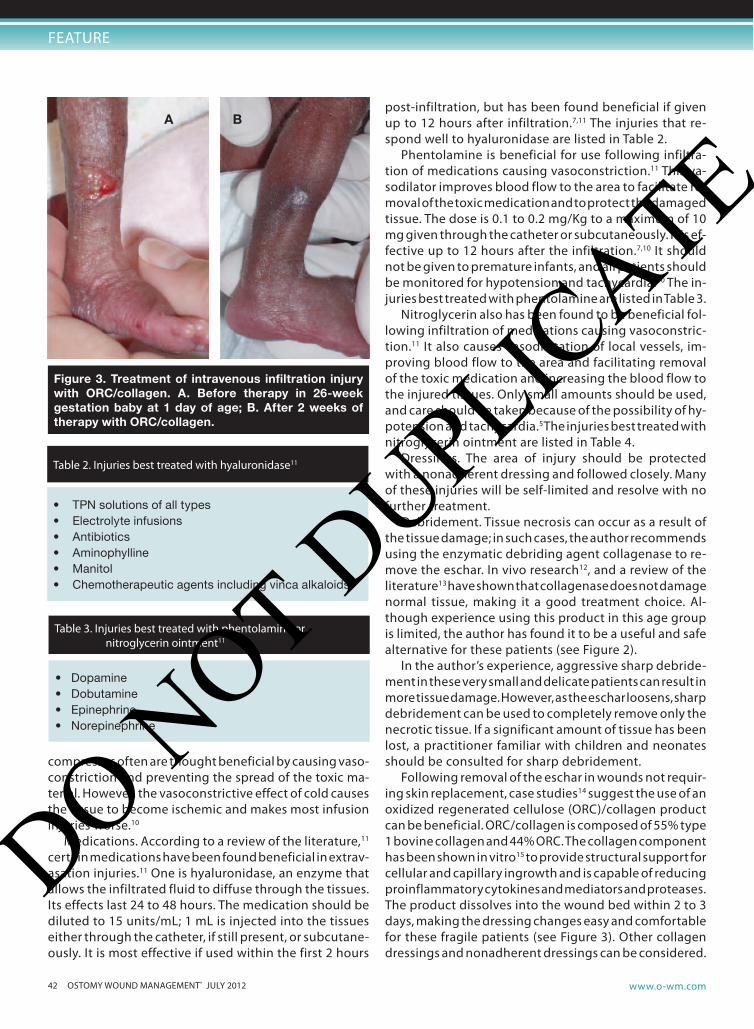
Following removal of the eschar in wounds not requir-ing skin replacement, case studies14 suggest the use of an oxidized regenerated cellulose (orC)/collagen product can be beneficial. orC/collagen is composed of 55% type 1 bovine collagen and 44% orC. the collagen component has been shown in vitro15 to provide structural support for cellular and capillary ingrowth and is capable of reducing proinflammatory cytokines and mediators and proteases. the product dissolves into the wound bed within 2 to 3 days, making the dressing changes easy and comfortable for these fragile patients (see Figure 3). other collagen dressings and nonadherent dressings can be considered.
• Dopamine• Dobutamine• Epinephrine• Norepinephrine
table 3. Injuries best treated with phentolamine or nitroglycerin ointment11
Figure 3. Treatment of intravenous infiltration injury with ORC/collagen. A. Before therapy in 26-week gestation baby at 1 day of age; B. After 2 weeks of therapy with ORC/collagen.
A B
• TPN solutions of all types• Electrolyte infusions• Antibiotics• Aminophylline• Manitol• Chemotherapeutic agents including vinca alkaloids
table 2. Injuries best treated with hyaluronidase11
DO NOT D
UPLICATE

july 2012 ostomy wound management® 43www.o-wm.com
Intravenous InFIltratIon InjurIes
silver-containing dressings should be used with great care in children and neonates; while dressings releasing very low levels of silver have been found in pediatric case stud-ies to be well-tolerated and not damage the cells in the wound bed, toxicity of silver dressings, a growing con-cern in children, has resulted in systemic serum levels 800 times normal18,19 and their use should be avoided.
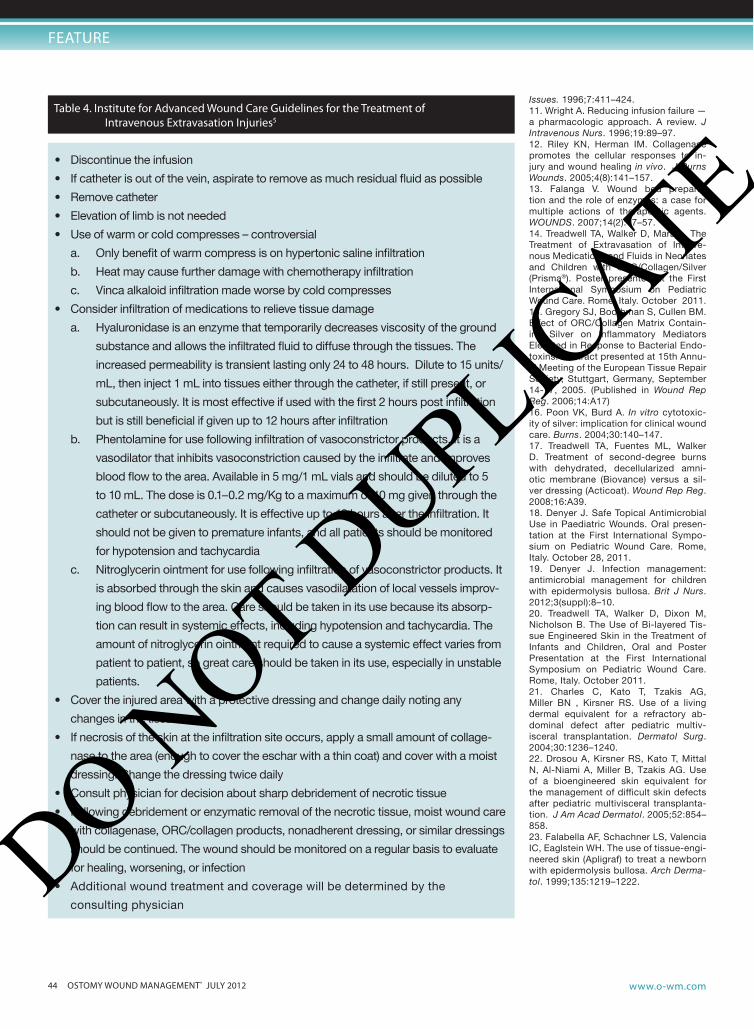
skin replacement. If the tissue defects are large, clo-sure may be difficult and require skin replacement. skin grafting in very young children is fraught with hazard and produces another wound just as difficult to close as the original lesion. the author and other clinicians have found that the use of cell-containing tissue-engineered skin products that have been approved for use in chron-ic wounds can have a great benefit in these patients.20-23
(although these products are only approved for use with diabetic foot ulcers, apligraf [organogenesis, Inc, Can-ton, ma] has approval for humanitarian use in infants and children with epidemolysis bullosa.) these products are designed to provide healthy cells to the wound bed to stimulate and accelerate healing (see Figure 4).
Conclusion extravasation injury from intravenous fluid is a poten-
tially serious complication in infants and children. when prevention efforts fail, early recognition and appropriate treatment are essential to minimize the extent of the in-jury. most injuries will heal spontaneously without com-plications. Per opinion and research,10 having a clinical practice guideline in place before injuries occur is critical to encourage early recognition and immediate and in-
formed treatment. the guideline used by the Institute for advanced wound Care at Baptist medical Center, mont-gomery, al, (see table 4) has worked well in the author’s center; use by others is pending. Fortunately, technolo-gy has provided treatment options for the patients with significant injuries that have been useful in the author’s clinical practice. additional work will be required to ac-complish earlier recognition of these injuries, if possible, and continued research with various wound dressings will be required to find the optimal treatment of wounds in this age group. n
references1. Treadwell TA. Intramuscular injection site injuries masquerading as
pressure ulcers. WOUNDS. 2003;15(9):302–312.2. Brown H. Jean Denis and the Transfusion of Blood, Paris, 1667-1668.
Isis Brown Harcourt;1947;39z;15–29.3. Tucker H. Blood Work: A Tale of Medicine and Murder in the Scientific
Revolution. New York, NY: W.W. Norton and Co;2011:233.4. Weatherhill T. Case of malignant cholera in which four hundred and
eighty ounces of fluid were injected into the veins with success. Lan-cet. 1832;18(470):688
5. Treadwell T, Fuentes ML, Walker D, Mara L. The Approach to Injuries Due to Extravasation of Intravenous Medications and Fluids. Poster presented at the Symposium on Advanced Wound Care. Dallas, TX. April 2009.
6. Thomas D, Rowe HN, Keats J, Morgan RJH. The Management of Ex-travastion Injury in Neonates. Available at: www.worldwidewounds.com/1997/october/Neonates/NeonatePaper.html. Accessed June 11, 2012.
7. Hastings-Tolsma MT, Yucha CB, Tompkins J, Robson L, Szevereny N. Effect of warm and cold applications on the resolution of IV infiltra-tions. Res Nurs Health. 1993;16:171–178.
8. Yucha CB, Hastings-Tolsma M, Szeverenyi NM. Effect of elevation on intravenous extravasations. J Intraven Nurs. 1994;17:231–234.
9. Larson DL. What is the appropriate management of tissue extravasation by antitumor agents? Plast Reconstr Surg. 1985;75:397–405.
10. Montgomery LA, Budreau GK. Implementing a clinical practice guide-line to improve pediatric intravenous infiltration outcomes. AACN Clin
Figure 4. Treatment of intravenous infiltration injury with bilayered tissue-engineered skin. A. Injury due to do-pamine infiltration: before debridement; B. Post debridement; C. Application of bilayered, tissue-engineered skin; D. Healed 3 weeks post-application of bilayered, tissue-engineered skin.
A B C D
DO NOT D
UPLICATE
44 ostomy wound management® july 2012 www.o-wm.com
Feature
Issues. 1996;7:411–424.11. Wright A. Reducing infusion failure — a pharmacologic approach. A review. J Intravenous Nurs. 1996;19:89–97.12. Riley KN, Herman IM. Collagenase promotes the cellular responses to in-jury and wound healing in vivo. J Burns Wounds. 2005;4(8):141–157.13. Falanga V. Wound bed prepara-tion and the role of enzymes: a case for multiple actions of therapeutic agents. WOUNDS. 2007;14(2):47–57.14. Treadwell TA, Walker D, Mara L. The Treatment of Extravasation of Intrave-nous Medications and Fluids in Neonates and Children with ORC/Collagen/Silver (Prisma®). Poster presented at the First International Symposium on Pediatric Wound Care. Rome, Italy. October 2011.15. Gregory SJ, Boothman S, Cullen BM. Effect of ORC/Collagen Matrix Contain-ing Silver on Inflammatory Mediators Elevated in Response to Bacterial Endo-toxins. Abstract presented at 15th Annu-al Meeting of the European Tissue Repair Society, Stuttgart, Germany, September 14-17, 2005. (Published in Wound Rep Reg. 2006;14:A17) 16. Poon VK, Burd A. In vitro cytotoxic-ity of silver: implication for clinical wound care. Burns. 2004;30:140–147.17. Treadwell TA, Fuentes ML, Walker D. Treatment of second-degree burns with dehydrated, decellularized amni-otic membrane (Biovance) versus a sil-ver dressing (Acticoat). Wound Rep Reg. 2008;16:A39.18. Denyer J. Safe Topical Antimicrobial Use in Paediatric Wounds. Oral presen-tation at the First International Sympo-sium on Pediatric Wound Care. Rome, Italy. October 28, 2011. 19. Denyer J. Infection management: antimicrobial management for children with epidermolysis bullosa. Brit J Nurs. 2012;3(suppl):8–10.20. Treadwell TA, Walker D, Dixon M, Nicholson B. The Use of Bi-layered Tis-sue Engineered Skin in the Treatment of Infants and Children, Oral and Poster Presentation at the First International Symposium on Pediatric Wound Care. Rome, Italy. October 2011.21. Charles C, Kato T, Tzakis AG, Miller BN , Kirsner RS. Use of a living dermal equivalent for a refractory ab-dominal defect after pediatric multiv-isceral transplantation. Dermatol Surg. 2004;30:1236–1240.22. Drosou A, Kirsner RS, Kato T, Mittal N, Al-Niami A, Miller B, Tzakis AG. Use of a bioengineered skin equivalent for the management of difficult skin defects after pediatric multivisceral transplanta-tion. J Am Acad Dermatol. 2005;52:854–858.23. Falabella AF, Schachner LS, Valencia IC, Eaglstein WH. The use of tissue-engi-neered skin (Apligraf) to treat a newborn with epidermolysis bullosa. Arch Derma-tol. 1999;135:1219–1222.
• Discontinue the infusion
• If catheter is out of the vein, aspirate to remove as much residual fluid as possible
• Remove catheter
• Elevation of limb is not needed
• Use of warm or cold compresses – controversial
a. Only benefit of warm compress is on hypertonic saline infiltration
b. Heat may cause further damage with chemotherapy infiltration
c. Vinca alkaloid infiltration made worse by cold compresses
• Consider infiltration of medications to relieve tissue damage
a. Hyaluronidase is an enzyme that temporarily decreases viscosity of the ground
substance and allows the infiltrated fluid to diffuse through the tissues. The
increased permeability is transient lasting only 24 to 48 hours. Dilute to 15 units/
mL, then inject 1 mL into tissues either through the catheter, if still present, or
subcutaneously. It is most effective if used with the first 2 hours post infiltration
but is still beneficial if given up to 12 hours after infiltration
b. Phentolamine for use following infiltration of vasoconstrictor products. It is a
vasodilator that inhibits vasoconstriction caused by the infiltrate and improves
blood flow to the area. Available in 5 mg/1 mL vials and should be diluted to 5
to 10 mL. The dose is 0.1–0.2 mg/Kg to a maximum of 10 mg given through the
catheter or subcutaneously. It is effective up to 12 hours after the infiltration. It
should not be given to premature infants, and all patients should be monitored
for hypotension and tachycardia
c. Nitroglycerin ointment for use following infiltration of vasoconstrictor products. It
is absorbed through the skin and causes vasodilatation of local vessels improv-
ing blood flow to the area. Care should be taken in its use because its absorp-
tion can result in systemic effects, including hypotension and tachycardia. The
amount of nitroglycerin ointment required to cause a systemic effect varies from
patient to patient, so great care should be taken in its use, especially in unstable
patients.
• Cover the injured area with a protective dressing and change daily noting any
changes in the tissue
• If necrosis of the skin at the infiltration site occurs, apply a small amount of collage-
nase to the area (enough to cover the eschar with a thin coat) and cover with a moist
dressing. Change the dressing twice daily
• Consult physician for decision about sharp debridement of necrotic tissue
• Following debridement or enzymatic removal of the necrotic tissue, moist wound care
with collagenase, ORC/collagen products, nonadherent dressing, or similar dressings
should be continued. The wound should be monitored on a regular basis to evaluate
for healing, worsening, or infection
• Additional wound treatment and coverage will be determined by the
consulting physician
table 4. Institute for advanced wound Care guidelines for the treatment of Intravenous extravasation Injuries5
DO NOT D
UPLICATE





























