Embed Size (px)
Citation preview
pharmacoepidemiology and drug safety 2008; 17: 577–586ww.interscience.wiley.com) DOI: 10.1002/pds.1608
Published online 1 May 2008 in Wiley InterScience (wORIGINAL REPORT
Influence of antidepressants on glycaemic control in patientswith diabetes mellitusy
M. J. Knol MSc1,2*, H. J. Derijks PharmD2,3, M. I. Geerlings PhD1, E. R. Heerdink PhD2,P. C. Souverein PhD2, K. J. Gorter MD, PhD1, D. E. Grobbee MD, PhD1z
and A. C. G. Egberts PharmD, PhD2,4z
1Julius Center for Health Sciences and Primary Care, University Medical Center Utrecht, Utrecht, The Netherlands2Department of Pharmacoepidemiology and Pharmacotherapy, Utrecht Institute of Pharmaceutical Sciences, UtrechtUniversity, Utrecht, The Netherlands3Department of Clinical Pharmacy, Orbis Medical Center, Sittard, The Netherlands4Department of Clinical Pharmacy, University Medical Center Utrecht, Utrecht, The Netherlands
SUMMARY
Purpose Anecdotal evidence suggests that antidepressants (ADs) may complicate glycaemic control. The objective of thislongitudinal study was to investigate the influence of ADs on glycaemic control within diabetes patients.Methods From the pharmacy registry database PHARMO, we selected insulin users who did not use oral antidiabetics.The study population comprised: 133 patients with at least 12 months insulin use before and 6 months during an ADepisode, including 56 patients with an additional 6 months of insulin use after the AD episode; 180 patients with 24 monthsinsulin use without an AD episode. Glycaemic control was measured as the amount of insulin used, which was calculatedintra-individually in 3-month periods. We stratified for selective serotonin reuptake inhibitors (SSRIs) and tricyclicantidepressants (TCAs).Results Mean age (s.d.) of the subjects was 53.9 (19) years; 46.9% were men. Overall, the amount of insulin used did notchange during or after AD use. No-AD users showed an increase of 16% in amount of insulin used over a period of 2 years(p< 0.001). SSRI users showed a decrease of 13% in amount of insulin used during the AD episode (p¼ 0.029), while nochange was seen in TCA users. Notable was the large intra- and interindividual variation in amount of insulin used across allgroups.Conclusions Overall, AD use did not influence glycaemic control in diabetes patients. The tendency for a differencebetween SSRIs and TCAs is suggestive for a pharmacologic effect of ADs rather than a general effect of depression onglycaemic control. Copyright # 2008 John Wiley & Sons, Ltd.
key words—antidepressant; depression; insulin; diabetes
Received 12 September 2007; Revised 19 March 2008; Accepted 20 March 2008
*Correspondence to: M. J. Knol, Julius Center for Health Sciencesand Primary Care, University Medical Center Utrecht, Str. 6.131,P.O. Box 85500, 3508 GA Utrecht, The Netherlands.E-mail: [email protected] conflict of interest was declared.zProfessor.
Copyright # 2008 John Wiley & Sons, Ltd.
INTRODUCTION
Depression is a common co-morbidity in patientswith diabetes mellitus. The risk of depression isdoubled in patients with diabetes compared to thosewithout diabetes.1 In addition, among diabetespatients depression is associated with poor glycaemiccontrol.2 In turn, poor glycaemic control is a risk

578 m. j. knol ET AL.
factor for macrovascular complications, such ascardiovascular disease, and microvascular compli-cations, such as retinopathy and nephropathy.HbA1c, which is an aggregate measure of glycaemiccontrol over the 120-day period before testing, is animportant indicator for diabetes regulation. Efficacystudies have demonstrated that achieving andmaintaining HbA1c levels below 7% substantiallydecreased diabetes-related complications in individ-uals.3,4
Both depression and AD use can influenceglycaemic control in diabetes patients in severalways.5,6 Depression can worsen glycaemic controlby life style changes such as altered food intake,decreased physical activity, smoking and decreasedmedication adherence. Although, one study showedthat self-care behaviour could not fully explain theassociation between depression and glycaemiccontrol.7 From a physiological perspective, depres-sion can lead to increased cortisol secretion of thehypothalamic pituitary adrenal (HPA) axis, whichcan cause hyperglycaemia and thereby worsenglycaemic control. Evidence on the effect ofantidepressants (ADs) on glucose and insulin levelsmainly comes from animal studies, case reports andshort-term trials with selected and small groups ofpatients. AD use can disturb glycaemic control by itshyperglycaemic effect, which is thought to be morepronounced in some tricyclic antidepressants (TCAs)such as nortriptyline.8–10 In contrast, some selectiveserotonin reuptake inhibitors (SSRIs), such asfluoxetine and paroxetine, may decrease bloodglucose levels and HbA1c and reduce insulinrequirements.11–13 AD use could also improveglycaemic control because of successful treatmentof depression.In diabetes patients, changes in the degree of
glycaemic control can be deduced from changes inthe amount of insulin that these patients need.Patients using insulin monitor their own bloodglucose levels and they will use more insulinwhen their blood glucose is high and less when itis low.The main objective of the present study was to
investigate the influence of AD treatment onglycaemic control, measured as the amount of insulinused, within diabetes patients with an episode of ADuse. To study this we described the variability inamount of insulin used in diabetes patients before,during and after an episode of AD use. To study thenatural course of the amount of insulin used overtime we also included diabetes patients without anepisode of AD use.
Copyright # 2008 John Wiley & Sons, Ltd. P
METHODS
Data source
Our cohort was selected from the PHARMOdatabase. This database is described in detailelsewhere.14 In short, the PHARMO databasecomprises all pharmacy dispensing records of allresidents of about 50 Dutch municipalities, countingfor approximately two million patient histories.Since virtually all patients in the Netherlands areregistered with a single community pharmacy,pharmacy records are almost complete with regardto prescription drugs independent of the prescriber.In the Netherlands, ADs and insulin are onlyavailable as prescription drugs. Therefore, pharmacydata will cover all use of these drugs. Availablevariables in this database include gender, date ofbirth, dispensed drugs (coded according to theAnatomical Therapeutic Chemical (ATC) classifi-cation), drug dispensing date, amount of drugdispensed, prescribed dosage regimen and prescriber.
Study population
For this study, pharmacy data from 1991 to 2003were used. From the PHARMO database, all subjectswith a prescription of any AD (ATC code¼N06A�),a prescription of insulin (ATC code¼A10A�) and noprescription of any oral antidiabetic drug (ATCcode¼A10B�) were identified (n¼ 840). From thissample, patients were included in the study popu-lation if they met the following criteria: (1) 18 yearsor older at the start of AD use; (2) used insulin for atleast 12 months before the start of the AD and (3) theepisode of AD use (defined in detail later) lasted forat least 6 months. This resulted in a study sample of133 patients, of whom 56 also had at least 6 monthsof insulin use after they stopped with the AD. Theduration of the periods before, during and after anAD episode were arbitrarily chosen so that we wouldhave both a considerable amount of follow-up timeand a considerable amount of patients to study.
To study the natural course of the amount of insulinused over a certain time period, a random sample ofinsulin users without a prescription of any AD andwithout a prescription of any oral antidiabetic drugwas selected from the PHARMO database. Thesepatients were assigned a random index date in such away that the distribution of the index date relative tothe total period of insulin use was similar to thedistribution of the start of the AD episode relative tothe total period of insulin use in AD users.Subsequently, patients were included in the study
harmacoepidemiology and Drug Safety, 2008; 17: 577–586DOI: 10.1002/pds
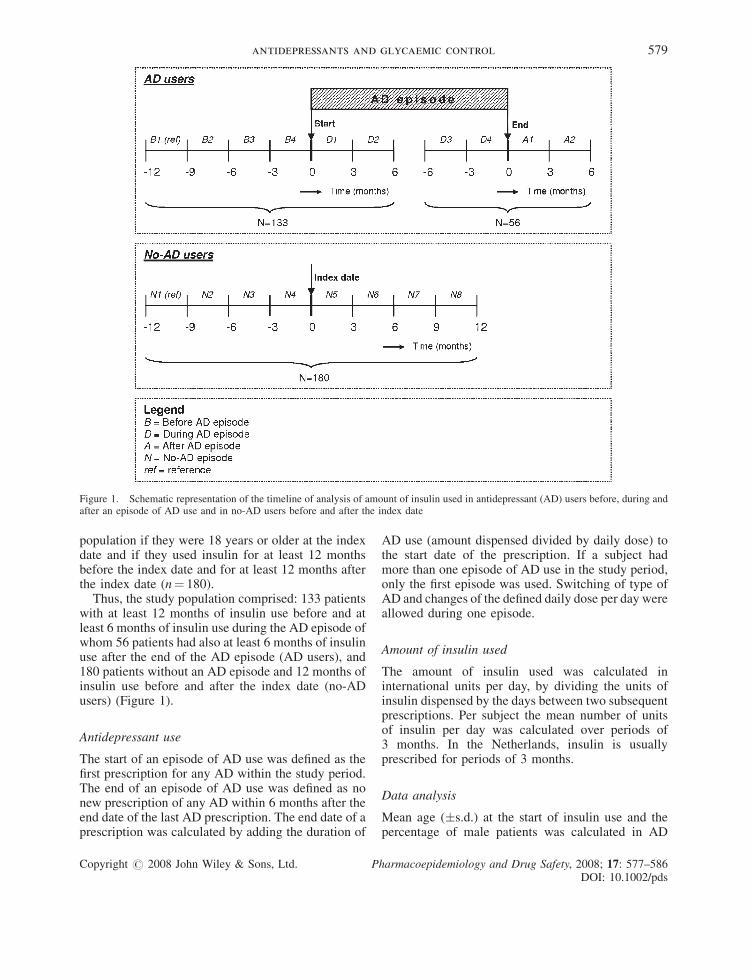
Figure 1. Schematic representation of the timeline of analysis of amount of insulin used in antidepressant (AD) users before, during andafter an episode of AD use and in no-AD users before and after the index date
antidepressants and glycaemic control 579
population if they were 18 years or older at the indexdate and if they used insulin for at least 12 monthsbefore the index date and for at least 12 months afterthe index date (n¼ 180).
Thus, the study population comprised: 133 patientswith at least 12 months of insulin use before and atleast 6 months of insulin use during the AD episode ofwhom 56 patients had also at least 6 months of insulinuse after the end of the AD episode (AD users), and180 patients without an AD episode and 12 months ofinsulin use before and after the index date (no-ADusers) (Figure 1).
Antidepressant use
The start of an episode of AD use was defined as thefirst prescription for any AD within the study period.The end of an episode of AD use was defined as nonew prescription of any AD within 6 months after theend date of the last AD prescription. The end date of aprescription was calculated by adding the duration of
Copyright # 2008 John Wiley & Sons, Ltd. P
AD use (amount dispensed divided by daily dose) tothe start date of the prescription. If a subject hadmore than one episode of AD use in the study period,only the first episode was used. Switching of type ofAD and changes of the defined daily dose per day wereallowed during one episode.
Amount of insulin used
The amount of insulin used was calculated ininternational units per day, by dividing the units ofinsulin dispensed by the days between two subsequentprescriptions. Per subject the mean number of unitsof insulin per day was calculated over periods of3 months. In the Netherlands, insulin is usuallyprescribed for periods of 3 months.
Data analysis
Mean age (�s.d.) at the start of insulin use and thepercentage of male patients was calculated in AD
harmacoepidemiology and Drug Safety, 2008; 17: 577–586DOI: 10.1002/pds

580 m. j. knol ET AL.
users and no-AD users. In AD users the number of ADepisodes and the duration of the first AD episode werecalculated. Also, the percentage of patients that usedSSRIs (selective serotonin reuptake inhibitors), TCAsand other ADs and the percentage of patients that hada change of defined daily dose of AD or a switch of ADduring the first episode were calculated.The distribution of the amount of insulin used at
the different time points in AD and no-AD userswas skewed to the left. The tests for normality(Kolmogorov–Smirnov) were all significant, indicat-ing non-normality. Log transformation solved thisnon-normality for some time points but not for all.For this reason we chose to perform non-parametrictests.Differences in the amount of insulin used over time
were tested with the non-parametric Friedman test forrepeated measurements. Differences between twotime points were tested with the non-parametricWilcoxon test for paired observations. To show theintra-individual differences over time we calculatedthe relative amount of insulin used in each period re-lative to the reference period. The reference period inthe AD users and no-AD users was the 3-month periodbetween 12 and 9 months before the start of the ADepisode (Figure 1; period B1) and the 3-month periodbetween 12 and 9 months before the index date(Figure 1; period N1), respectively. For each subjectthe relative amount of insulin used was calculated bydividing the units of insulin used in each 3-monthperiod by the units of insulin used in the referenceperiod. For example a subject used 50 units ofinsulin per day in reference period B1 and used55 units per day in period B2, meaning that the relativeamount of insulin used in this subject was 1.10 (55/50)in period B2. Subsequently, for each 3-month periodthe median relative amount and interquartile rangeover all patients was calculated and presented ingraphs.Besides calculating the relative amount of insulin
used between the 3-month periods, we calculated ineach period the percentage of patients that increased(relative amount of insulin used >1.10), decreased(relative amount of insulin used <0.90) and keptconstant on their insulin used (relative amount ofinsulin used between 0.90 and 1.10). This was done inAD users as well as in no-AD users. Differencesin percentages between two time points were testedwith the McNemar test for paired proportions.We stratified all analyses for the two main types of
ADs, namely SSRIs and TCAs, because previousstudies suggested that SSRIs and TCAs have contra-dictory effects on glycaemic control. Patients who
Copyright # 2008 John Wiley & Sons, Ltd. P
switched from one type of AD to another within theperiods that we studied, were excluded from theseanalyses. Differences in the amount of insulin usedover time between SSRI users and TCA users weretested with a mixed between-within subjects analysisof variance (a non-parametric alternative is notavailable). To show the intra-individual differencesover time we calculated the relative amount of insulinused in each period relative to the reference period, asdescribed above, and presented this in graphs.Differences between SSRI and TCA users inpercentage of increasers and decreasers in amountof insulin used in one time point were tested with thex2 test.
We calculated the change in amount of insulin usedwe could detect with 80% power and an a of 0.05 withthe observed data. The change we could detectbetween the various time points within the patientswith an AD episode ranged from 6.4 to 10.6 units ofinsulin used (about 10–16% change), with one outlierfor the difference between D3 and D4 where we coulddetect a change of 14.6 units of insulin. For thepatients without an AD episode the change we coulddetect ranged from 5.7 to 7.9 units of insulin used(about 10–13% change).
RESULTS
Table 1 presents the baseline characteristics in ADusers and no-AD users. The mean age of the AD users(54.8� 19) was comparable with the age of the no-ADusers (53.0� 19). The no-AD users were more oftenmale (48.3%) than the AD users (45.1%). Themajority of the AD users (91%) had only one episodeof AD use during the study period. The duration ofthe first episode was 6–12 months in most patients(43.6%) and more than 24 months in 25.6% of theAD users. SSRIs were most frequently used and18 patients (13.5%) used different types of ADs duringthe first AD episode. In almost 50% of the patients thedefined daily dose of AD was changed during the ADepisode.
Figure 2 shows the median relative amount ofinsulin used in AD users before, during and after anAD episode (upper graph) and the median relativeamount of insulin used in no-AD users (lower graph).The upper graph showed a significant increase in theamount of insulin used in AD users before the ADepisode (p¼ 0.035). There were no significantchanges over time in the amount of insulin usedwhen analysing period B1 through D2 (p¼ 0.094) orperiod B1 through A2 (p¼ 0.916). There were nosignificant differences between time points before or
harmacoepidemiology and Drug Safety, 2008; 17: 577–586DOI: 10.1002/pds
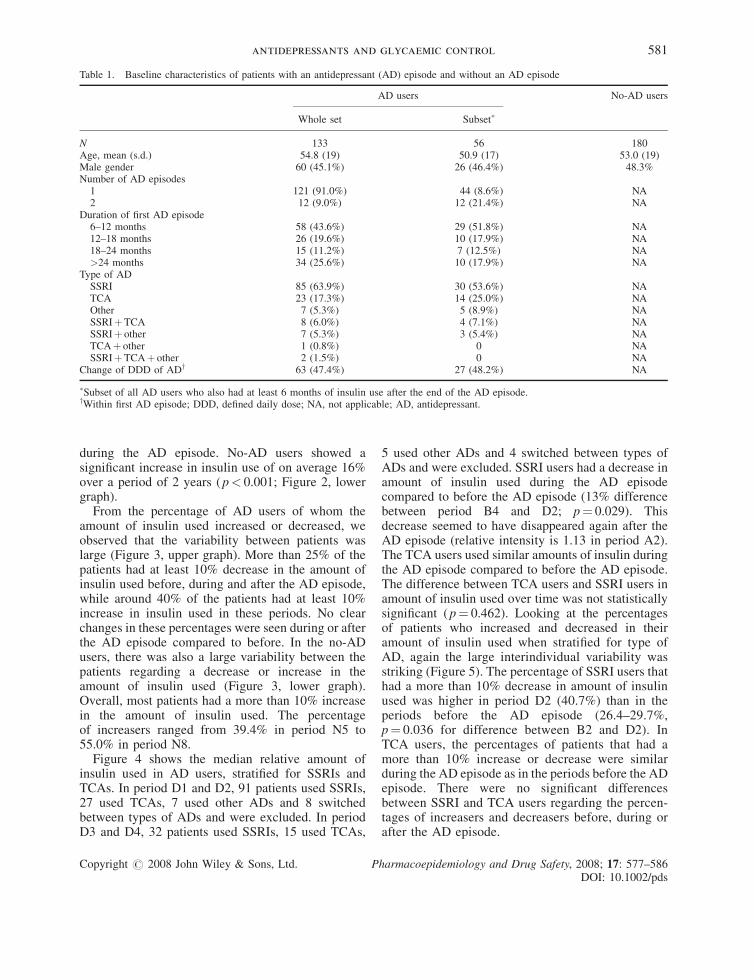
Table 1. Baseline characteristics of patients with an antidepressant (AD) episode and without an AD episode
AD users No-AD users
Whole set Subset�
N 133 56 180Age, mean (s.d.) 54.8 (19) 50.9 (17) 53.0 (19)Male gender 60 (45.1%) 26 (46.4%) 48.3%Number of AD episodes1 121 (91.0%) 44 (8.6%) NA2 12 (9.0%) 12 (21.4%) NA
Duration of first AD episode6–12 months 58 (43.6%) 29 (51.8%) NA12–18 months 26 (19.6%) 10 (17.9%) NA18–24 months 15 (11.2%) 7 (12.5%) NA>24 months 34 (25.6%) 10 (17.9%) NA
Type of ADSSRI 85 (63.9%) 30 (53.6%) NATCA 23 (17.3%) 14 (25.0%) NAOther 7 (5.3%) 5 (8.9%) NASSRIþTCA 8 (6.0%) 4 (7.1%) NASSRIþ other 7 (5.3%) 3 (5.4%) NATCAþ other 1 (0.8%) 0 NASSRIþTCAþ other 2 (1.5%) 0 NA
Change of DDD of ADy 63 (47.4%) 27 (48.2%) NA
�Subset of all AD users who also had at least 6 months of insulin use after the end of the AD episode.yWithin first AD episode; DDD, defined daily dose; NA, not applicable; AD, antidepressant.
antidepressants and glycaemic control 581
during the AD episode. No-AD users showed asignificant increase in insulin use of on average 16%over a period of 2 years (p< 0.001; Figure 2, lowergraph).
From the percentage of AD users of whom theamount of insulin used increased or decreased, weobserved that the variability between patients waslarge (Figure 3, upper graph). More than 25% of thepatients had at least 10% decrease in the amount ofinsulin used before, during and after the AD episode,while around 40% of the patients had at least 10%increase in insulin used in these periods. No clearchanges in these percentages were seen during or afterthe AD episode compared to before. In the no-ADusers, there was also a large variability between thepatients regarding a decrease or increase in theamount of insulin used (Figure 3, lower graph).Overall, most patients had a more than 10% increasein the amount of insulin used. The percentageof increasers ranged from 39.4% in period N5 to55.0% in period N8.
Figure 4 shows the median relative amount ofinsulin used in AD users, stratified for SSRIs andTCAs. In period D1 and D2, 91 patients used SSRIs,27 used TCAs, 7 used other ADs and 8 switchedbetween types of ADs and were excluded. In periodD3 and D4, 32 patients used SSRIs, 15 used TCAs,
Copyright # 2008 John Wiley & Sons, Ltd. P
5 used other ADs and 4 switched between types ofADs and were excluded. SSRI users had a decrease inamount of insulin used during the AD episodecompared to before the AD episode (13% differencebetween period B4 and D2; p¼ 0.029). Thisdecrease seemed to have disappeared again after theAD episode (relative intensity is 1.13 in period A2).The TCA users used similar amounts of insulin duringthe AD episode compared to before the AD episode.The difference between TCA users and SSRI users inamount of insulin used over time was not statisticallysignificant (p¼ 0.462). Looking at the percentagesof patients who increased and decreased in theiramount of insulin used when stratified for type ofAD, again the large interindividual variability wasstriking (Figure 5). The percentage of SSRI users thathad a more than 10% decrease in amount of insulinused was higher in period D2 (40.7%) than in theperiods before the AD episode (26.4–29.7%,p¼ 0.036 for difference between B2 and D2). InTCA users, the percentages of patients that had amore than 10% increase or decrease were similarduring the AD episode as in the periods before the ADepisode. There were no significant differencesbetween SSRI and TCA users regarding the percen-tages of increasers and decreasers before, during orafter the AD episode.
harmacoepidemiology and Drug Safety, 2008; 17: 577–586DOI: 10.1002/pds
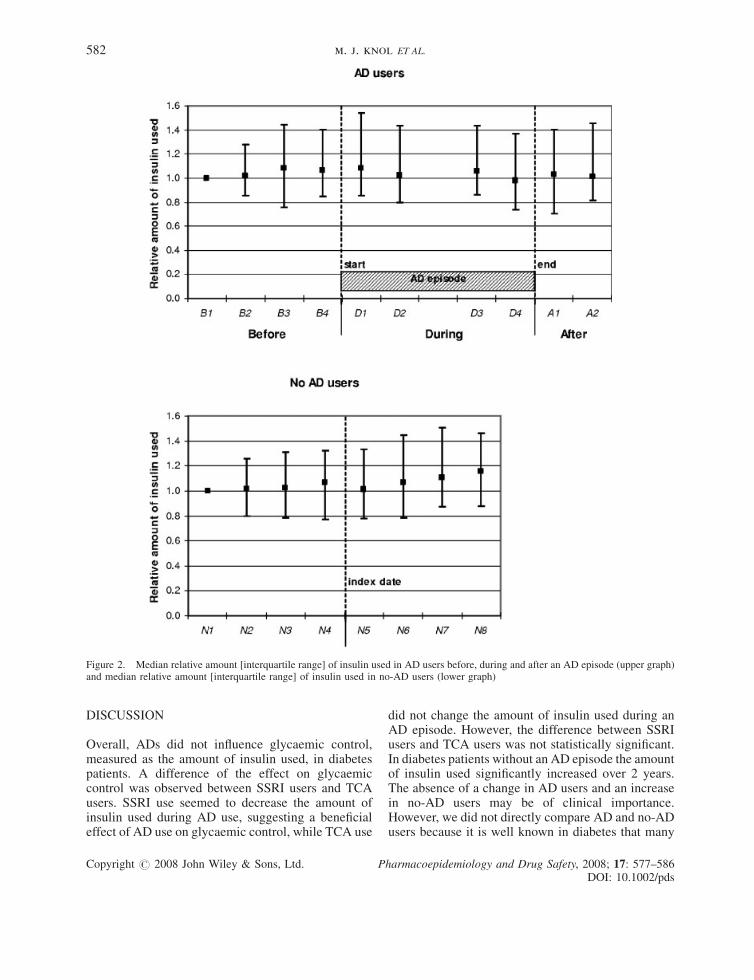
Figure 2. Median relative amount [interquartile range] of insulin used in AD users before, during and after an AD episode (upper graph)and median relative amount [interquartile range] of insulin used in no-AD users (lower graph)
582 m. j. knol ET AL.
DISCUSSION
Overall, ADs did not influence glycaemic control,measured as the amount of insulin used, in diabetespatients. A difference of the effect on glycaemiccontrol was observed between SSRI users and TCAusers. SSRI use seemed to decrease the amount ofinsulin used during AD use, suggesting a beneficialeffect of AD use on glycaemic control, while TCA use
Copyright # 2008 John Wiley & Sons, Ltd. P
did not change the amount of insulin used during anAD episode. However, the difference between SSRIusers and TCA users was not statistically significant.In diabetes patients without an AD episode the amountof insulin used significantly increased over 2 years.The absence of a change in AD users and an increasein no-AD users may be of clinical importance.However, we did not directly compare AD and no-ADusers because it is well known in diabetes that many
harmacoepidemiology and Drug Safety, 2008; 17: 577–586DOI: 10.1002/pds
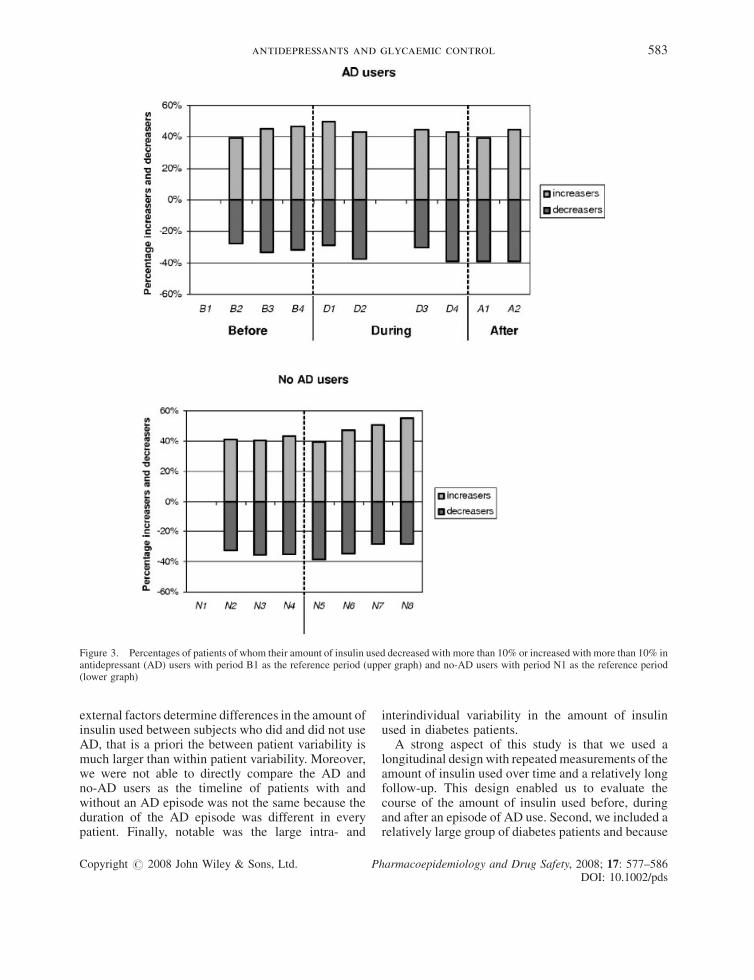
Figure 3. Percentages of patients of whom their amount of insulin used decreased with more than 10% or increased with more than 10% inantidepressant (AD) users with period B1 as the reference period (upper graph) and no-AD users with period N1 as the reference period(lower graph)
antidepressants and glycaemic control 583
external factors determine differences in the amount ofinsulin used between subjects who did and did not useAD, that is a priori the between patient variability ismuch larger than within patient variability. Moreover,we were not able to directly compare the AD andno-AD users as the timeline of patients with andwithout an AD episode was not the same because theduration of the AD episode was different in everypatient. Finally, notable was the large intra- and
Copyright # 2008 John Wiley & Sons, Ltd. P
interindividual variability in the amount of insulinused in diabetes patients.A strong aspect of this study is that we used a
longitudinal design with repeated measurements of theamount of insulin used over time and a relatively longfollow-up. This design enabled us to evaluate thecourse of the amount of insulin used before, duringand after an episode of AD use. Second, we included arelatively large group of diabetes patients and because
harmacoepidemiology and Drug Safety, 2008; 17: 577–586DOI: 10.1002/pds
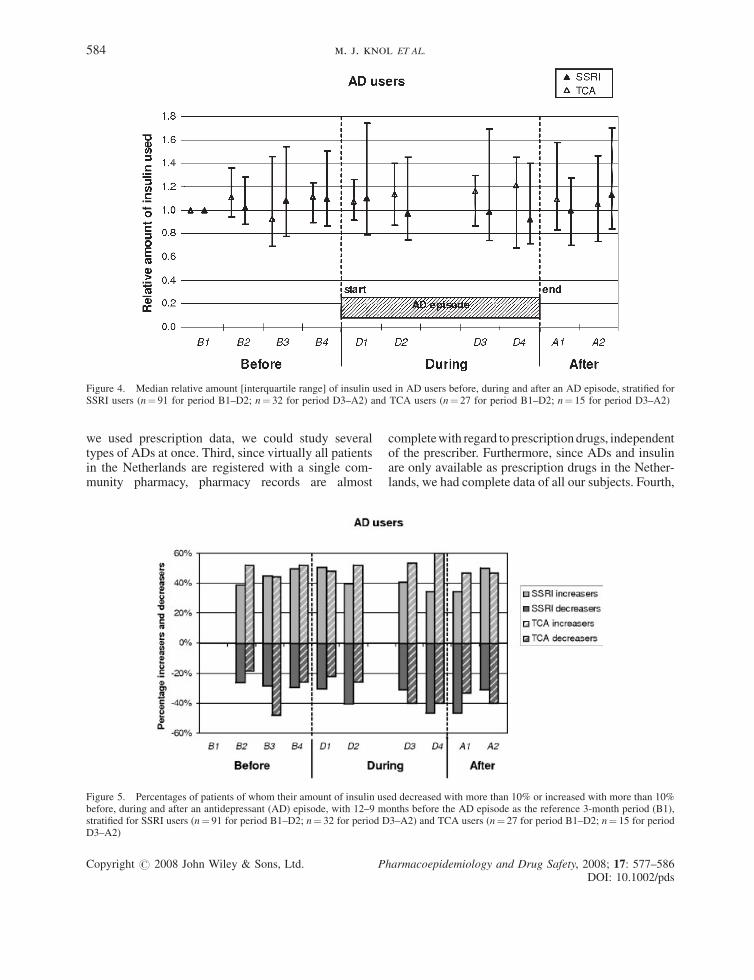
Figure 4. Median relative amount [interquartile range] of insulin used in AD users before, during and after an AD episode, stratified forSSRI users (n¼ 91 for period B1–D2; n¼ 32 for period D3–A2) and TCA users (n¼ 27 for period B1–D2; n¼ 15 for period D3–A2)
584 m. j. knol ET AL.
we used prescription data, we could study severaltypes of ADs at once. Third, since virtually all patientsin the Netherlands are registered with a single com-munity pharmacy, pharmacy records are almost
Figure 5. Percentages of patients of whom their amount of insulin usbefore, during and after an antidepressant (AD) episode, with 12–9 mstratified for SSRI users (n¼ 91 for period B1–D2; n¼ 32 for period DD3–A2)
Copyright # 2008 John Wiley & Sons, Ltd. P
completewith regard to prescriptiondrugs, independentof the prescriber. Furthermore, since ADs and insulinare only available as prescription drugs in the Nether-lands, we had complete data of all our subjects. Fourth,
ed decreased with more than 10% or increased with more than 10%onths before the AD episode as the reference 3-month period (B1),3–A2) and TCA users (n¼ 27 for period B1–D2; n¼ 15 for period
harmacoepidemiology and Drug Safety, 2008; 17: 577–586DOI: 10.1002/pds

KEYPOINTS
� In this longitudinal study antidepressant use didnot influence the overall glycaemic control indiabetes patients.
� The tendency for a difference that we observedbetween SSRIs and TCAs is suggestive for aphysiologic effect of antidepressants rather thana general effect of depression on glycaemiccontrol.
� The differences between SSRIs and TCAs inglycaemic control were rather small and prob-ably not of importance for choosing a specifictype of antidepressant in patients with diabetesmellitus.
antidepressants and glycaemic control 585
we calculated the amount of insulin used withinpatients, which gives more reliable results than be-tween subject analyses, because the relation under studyis less likely to be confounded by external factors.
A limitation of this study is that our method ofmeasuring glycaemic control, that is the amount ofinsulin used of diabetes patients using pharmacy data,may not be sensitive enough to detect small changes inthe amount of insulin used. Second, we assessedinsulin use in periods of 3 months. This period waschosen to get a valid estimate of insulin use becauseinsulin is mostly prescribed for periods of 3 months inthe Netherlands. However, it might be that this3-month period was too long to detect changes ininsulin use, that is that changes were levelled out overthe 3-month period. Third, as we only had prescriptiondata we could not differentiate between type 1 andtype 2 diabetes patients. We selected users of insulinwithout use of oral antidiabetic drugs, meaning thatthe study population probably included mostlypatients with type 1 diabetes. Fourth, the amount ofinsulin used was used as a proxy for glycaemiccontrol. However, we think that our outcome measure,in a population of insulin users who will predomi-nantly adjust insulin dose on measured blood glucoselevels, is a good measure for changes in glycaemiccontrol. Other outcome measures like changes inHbA1c values and changes in average blood glucosemay be less accurate, because many patients willadjust insulin dose by strict glucose monitoring.
To our knowledge, this is the first study thatinvestigated the influence of ADs on glycaemic controlin an observational study with repeated measurements.Previous studies investigated the influence of differentADs on HbA1c levels, glucose levels and plasmainsulin levels. Most of these studies had smallsample sizes (<50 patients),11,15,16 studied non-diabetic patients,11,15,17 or had a short study duration(<6 months of AD treatment).11,16 The results of thesestudies were inconsistent. One study found a signifi-cant decrease of blood glucose after treatment with theSSRI fluoxetine, and a significant increase in bloodglucose after use of the TCA imipramine.11 Otherstudies did not find significant effects on blood glucoselevels of paroxetine,16 bupropion17 and severalTCAs.15 The study of treatment with the SSRIparoxetine found a significant decrease of HbA1c16
and the study where several TCAs were evaluatedfound an increased insulin sensitivity after treatment.15
The latter finding is inconsistent with other studies thatreported unfavourable effects of TCAs on glucose andinsulin homeostasis. A review of the effects of ADs onglucose homeostasis and insulin sensitivity concluded
Copyright # 2008 John Wiley & Sons, Ltd. P
that, in general, serotonergic ADs had a favourableeffect on blood glucose levels and insulin sensitivity.6
Both venlafaxine and duloxetine, which are serotoninand noradrenaline reuptake inhibitors, had neutralmetabolic effects and TCAs disrupted glucose homeo-stasis. Our results corroborate with the conclusions ofthe review but the variation in the amount of insulinused between the subjects in our study was too large toreally confirm these findings. A recent case reportfound a close association between imipramine treat-ment and insulin use,18 but we were unable to replicatethis finding. Most studies on the association betweendepression (as opposed to ADs) and HbA1c arecross-sectional studies and these also showed conflict-ing results. Some found a significant association,19,20
while others did not.21,22 Recently, a randomizedclinical trial showed that depression recovery withsertraline as well as sustained remission with andwithout treatment are associated with improvements inglycaemic control.23
In conclusion, in this longitudinal study AD useoverall did not influence glycaemic control in diabetespatients. The tendency for a difference that weobserved between SSRIs and TCAs is suggestive fora pharmacologic effect of ADs rather than a generaleffect of depression on glycaemic control. Thedifferences between SSRIs and TCAs in glycaemiccontrol were rather small and probably not ofimportance for choosing a specific type of AD inpatients with diabetes mellitus.
ACKNOWLEDGEMENTS
This study was supported by an unrestricted grantfrom Novo Nordisk and the Scientific Institute ofDutch Pharmacists (WINAp).
harmacoepidemiology and Drug Safety, 2008; 17: 577–586DOI: 10.1002/pds

586 m. j. knol ET AL.
REFERENCES
1. Anderson RJ, Freedland KE, Clouse RE, Lustman PJ. Theprevalence of comorbid depression in adults with diabetes: ameta-analysis. Diabetes Care 2001; 24: 1069–1078.
2. Lustman PJ, Anderson RJ, Freedland KE, de Groot M, CarneyRM, Clouse RE. Depression and poor glycemic control: ameta-analytic review of the literature. Diabetes Care 2000;23: 934–942.
3. The Diabetes Control and Complications Trial Research Group.The effect of intensive treatment of diabetes on the developmentand progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med 1993; 329: 977–986.
4. UK Prospective Diabetes Study (PDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared withconventional treatment and risk of complications in patientswith type 2 diabetes (UKPDS 33). Lancet 1998; 352: 837–853.
5. Goodnick PJ, Henry JH, Buki VM. Treatment of depression inpatients with diabetes mellitus. J Clin Psychiatry 1995; 56:128–136.
6. McIntyre RS, Soczynska JK, Konarski JZ, Kennedy SH. Theeffect of antidepressants on glucose homeostasis and insulinsensitivity: synthesis and mechanisms. Expert Opin Drug Saf2006; 5: 157–168.
7. Lustman PJ, Clouse RE, Ciechanowski PS, Hirsch IB, Freed-land KE. Depression-related hyperglycemia in type 1 diabetes:a mediational approach. Psychosom Med 2005; 67: 195–199.
8. Erenmemisoglu A, Ozdogan UK, Saraymen R, Tutus A. Effectof some antidepressants on glycaemia and insulin levels ofnormoglycaemic and alloxan-induced hyperglycaemic mice.J Pharm Pharmacol 1999; 51: 741–743.
9. Goodnick PJ. Use of antidepressants in treatment of comorbiddiabetes mellitus and depression as well as in diabetic neuro-pathy. Ann Clin Psychiatry 2001; 13: 31–41.
10. Lustman PJ, Griffith LS, Clouse RE, et al. Effects of nortripty-line on depression and glycemic control in diabetes: results of adouble-blind, placebo-controlled trial. Psychosom Med 1997;59: 241–250.
11. Ghaeli P, Shahsavand E, Mesbahi M, Kamkar MZ, Sadeghi M,Dashti-Khavidaki S. Comparing the effects of 8-week treatmentwith fluoxetine and imipramine on fasting blood glucose ofpatients with major depressive disorder. J Clin Psychopharma-col 2004; 24: 386–388.
Copyright # 2008 John Wiley & Sons, Ltd. P
12. Maheux P, Ducros F, Bourque J, Garon J, Chiasson JL. Fluox-etine improves insulin sensitivity in obese patients with non-insulin-dependent diabetes mellitus independently of weightloss. Int J Obes Relat Metab Disord 1997; 21: 97–102.
13. Park S, Choi SB. Does fluoxetine administration influenceinsulin resistance in 90% pancreatectomized rats? Metabolism2002; 51: 38–43.
14. Herings RM, Bakker A, Stricker BH, Nap G. Pharmaco-morbidity linkage: a feasibility study comparing morbidity intwo pharmacy based exposure cohorts. J Epidemiol CommunityHealth 1992; 46: 136–140.
15. Okamura F, Tashiro A, Utumi A, et al. Insulin resistance inpatients with depression and its changes during the clinicalcourse of depression: minimal model analysis. Metabolism2000; 49: 1255–1260.
16. Paile-Hyvarinen M, Wahlbeck K, Eriksson JG. Quality of lifeand metabolic status in mildly depressed women with type2 diabetes treated with paroxetine: a single-blind randomisedplacebo controlled trial. BMC Family Practice 2003; 4: 7.
17. Jain AK, Kaplan RA, Gadde KM, et al. Bupropion SR vs.placebo for weight loss in obese patients with depressivesymptoms. Obes Res 2002; 10: 1049–1056.
18. Derijks HJ, De Koning FH, Meyboom RH, Heerdink ER,Spooren PF, Egberts AC. Impaired glucose homeostasis afterimipramine intake in a diabetic patient. J Clin Psychopharma-col 2005; 25: 621–623.
19. Gross R, Olfson M, Gameroff MJ, et al. Depression andglycemic control in Hispanic primary care patients with dia-betes. J Gen Intern Med 2005; 20: 460–466.
20. Katon W, Von Korff M, Ciechanowski P, et al. Behavioral andclinical factors associated with depression among individualswith diabetes. Diabetes Care 2004; 27: 914–920.
21. Ciechanowski PS, KatonWJ, Russo JE, Hirsch IB. The relation-ship of depressive symptoms to symptom reporting, self-careand glucose control in diabetes. Gen Hosp Psychiatry 2003; 25:246–252.
22. Paschalides C, Wearden AJ, Dunkerley R, Bundy C, Davies R,Dickens CM. The associations of anxiety, depression andpersonal illness representations with glycaemic control andhealth-related quality of life in patients with type 2 diabetesmellitus. J Psychosom Res 2004; 57: 557–564.
23. Lustman PJ, Clouse RE, Nix BD, et al. Sertraline for preventionof depression recurrence in diabetes mellitus: a randomized,double-blind, placebo-controlled trial. Arch Gen Psychiatry2006; 63: 521–529.
harmacoepidemiology and Drug Safety, 2008; 17: 577–586DOI: 10.1002/pds