Embed Size (px)
Citation preview
INTEGRATED CHRONIC DISEASE MANAGEMENT
2
INTEGRATED CHRONIC DISEASE MANAGEMENT
Integrated Chronic Disease Management (ICDM) is a model of managed care that provides for integrated prevention, treatment and care of chronic patients at primary healthcare level (PHC) to ensure a seamless transition to “assisted” self-
management within the community.
The aim of ICDM is to achieve optimal clinical outcomes for patients with chronic communicable and non-communicable diseases (NCDs) using the health system building blocks approach.
Purpose of the ICDM is to respond to the growing burden of chronic diseases in South Africa in an efficient and cost effective manner.
These pillars are supported through a sustained, strengthened and integrated health system.
PILLARS OF THE MODEL: f Primary prevention identification of high-risk individuals at community and facility level
f Secondary prevention through planned, optimal evidence- based clinical care using an interdisciplinary approach
f Cultivate a sense of individual responsibility through assisted self-management at community level
f Strengthening of the implementation of health policies addressing the social determinants of health at a population level
ICDM WILL BE ACHIEVED THROUGH: f Strong stewardship and ownership at all levels of the health system
f Health service re-organisation at facility level
f Clinical management support at facility level
f “Assisted” self-management at community level
f Strengthening of support systems and structures within the health system.
3
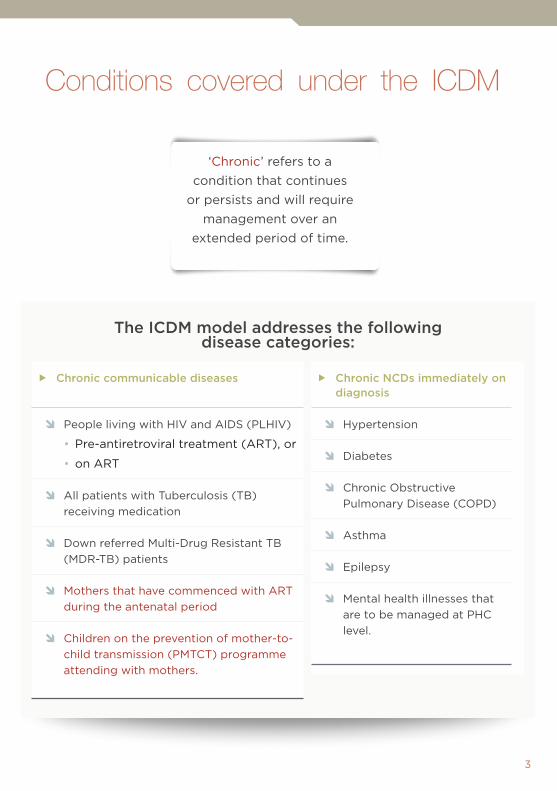
Conditions covered under the ICDM
‘Chronic’ refers to a condition that continues
or persists and will require management over an
extended period of time.
The ICDM model addresses the following disease categories:
f Chronic communicable diseases
Ô People living with HIV and AIDS (PLHIV)
•Pre-antiretroviral treatment (ART), or
•on ART
Ô All patients with Tuberculosis (TB) receiving medication
Ô Down referred Multi-Drug Resistant TB (MDR-TB) patients
Ô Mothers that have commenced with ART during the antenatal period
Ô Children on the prevention of mother-to-child transmission (PMTCT) programme attending with mothers.
f Chronic NCDs immediately on diagnosis
Ô Hypertension
Ô Diabetes
Ô Chronic Obstructive Pulmonary Disease (COPD)
Ô Asthma
Ô Epilepsy
Ô Mental health illnesses that are to be managed at PHC level.
4
INTEGRATED CHRONIC DISEASE MANAGEMENT
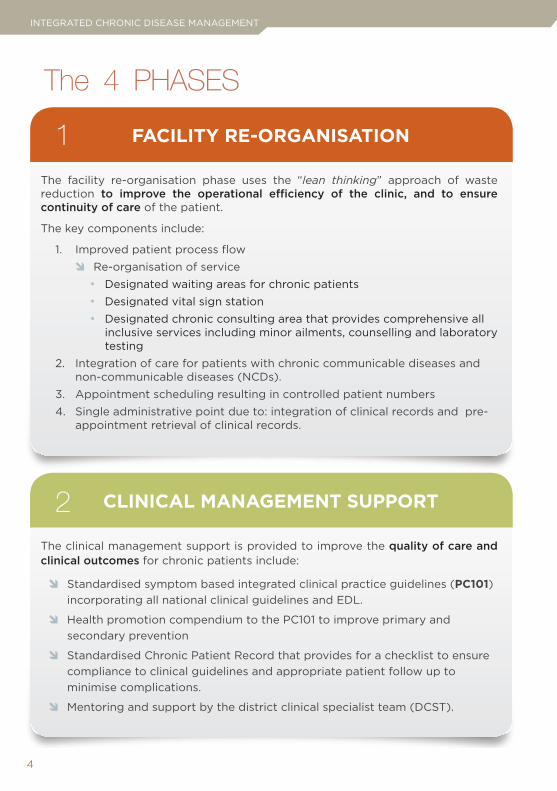
FACILITY RE-ORGANISATION
The facility re-organisation phase uses the “lean thinking” approach of waste reduction to improve the operational efficiency of the clinic, and to ensure continuity of care of the patient.
The key components include:
1. Improved patient process flow Ô Re-organisation of service• Designated waiting areas for chronic patients• Designated vital sign station • Designated chronic consulting area that provides comprehensive all
inclusive services including minor ailments, counselling and laboratory testing
2. Integration of care for patients with chronic communicable diseases and non-communicable diseases (NCDs).
3. Appointment scheduling resulting in controlled patient numbers4. Single administrative point due to: integration of clinical records and pre-
appointment retrieval of clinical records.
CLINICAL MANAGEMENT SUPPORT
The clinical management support is provided to improve the quality of care and clinical outcomes for chronic patients include:
Ô Standardised symptom based integrated clinical practice guidelines (PC101) incorporating all national clinical guidelines and EDL.
Ô Health promotion compendium to the PC101 to improve primary and secondary prevention
Ô Standardised Chronic Patient Record that provides for a checklist to ensure compliance to clinical guidelines and appropriate patient follow up to minimise complications.
Ô Mentoring and support by the district clinical specialist team (DCST).
The 4 PHASES
1
2
5
“ASSISTED” SELF-MANAGEMENT
Patients that are classified as stable (all parameters are within normal range over a period of three months on presentation at the facility and have no signs of disease progression or end organ damage) according to the clinical guidelines should be down referred to the PHC ward-based outreach team.
The community care givers (CCGs) or community health workers (CHWs) within the PHC ward-based outreach team, will visit patients at their homes on a monthly basis to:
Ô provide health promotion and education,
Ô check medicine adherence,
Ô do point of care testing and delivery of medication and,
Ô referral to health facility, if indicated.
You are the key to delivering quality services to the population. Change is not easy - discipline and persistence equals success
3
6
INTEGRATED CHRONIC DISEASE MANAGEMENT
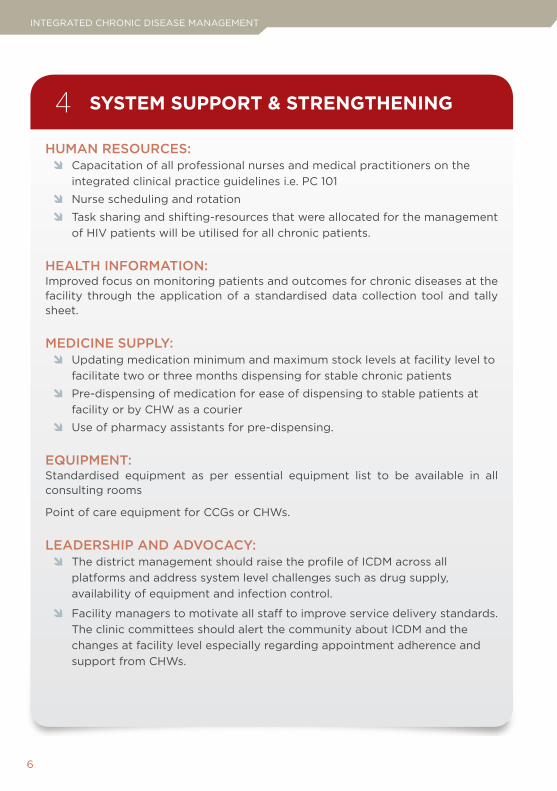
SYSTEM SUPPORT & STRENGTHENING
HUMAN RESOURCES: Ô Capacitation of all professional nurses and medical practitioners on the
integrated clinical practice guidelines i.e. PC 101
Ô Nurse scheduling and rotation
Ô Task sharing and shifting-resources that were allocated for the management of HIV patients will be utilised for all chronic patients.
HEALTH INFORMATION:Improved focus on monitoring patients and outcomes for chronic diseases at the facility through the application of a standardised data collection tool and tally sheet.
MEDICINE SUPPLY: Ô Updating medication minimum and maximum stock levels at facility level to
facilitate two or three months dispensing for stable chronic patients
Ô Pre-dispensing of medication for ease of dispensing to stable patients at facility or by CHW as a courier
Ô Use of pharmacy assistants for pre-dispensing.
EQUIPMENT:Standardised equipment as per essential equipment list to be available in all consulting rooms
Point of care equipment for CCGs or CHWs.
LEADERSHIP AND ADVOCACY: Ô The district management should raise the profile of ICDM across all
platforms and address system level challenges such as drug supply, availability of equipment and infection control.
Ô Facility managers to motivate all staff to improve service delivery standards. The clinic committees should alert the community about ICDM and the changes at facility level especially regarding appointment adherence and support from CHWs.
4
7
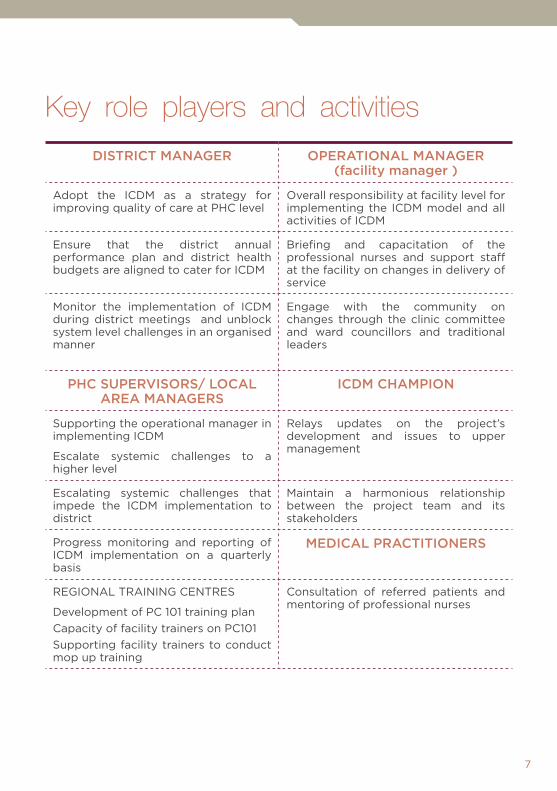
Key role players and activities
DISTRICT MANAGER OPERATIONAL MANAGER (facility manager )
Adopt the ICDM as a strategy for improving quality of care at PHC level
Overall responsibility at facility level for implementing the ICDM model and all activities of ICDM
Ensure that the district annual performance plan and district health budgets are aligned to cater for ICDM
Briefing and capacitation of the professional nurses and support staff at the facility on changes in delivery of service
Monitor the implementation of ICDM during district meetings and unblock system level challenges in an organised manner
Engage with the community on changes through the clinic committee and ward councillors and traditional leaders
PHC SUPERVISORS/ LOCAL AREA MANAGERS
ICDM CHAMPION
Supporting the operational manager in implementing ICDM
Escalate systemic challenges to a higher level
Relays updates on the project’s development and issues to upper management
Escalating systemic challenges that impede the ICDM implementation to district
Maintain a harmonious relationship between the project team and its stakeholders
Progress monitoring and reporting of ICDM implementation on a quarterly basis
MEDICAL PRACTITIONERS
REGIONAL TRAINING CENTRES
Development of PC 101 training planCapacity of facility trainers on PC101Supporting facility trainers to conduct mop up training
Consultation of referred patients and mentoring of professional nurses
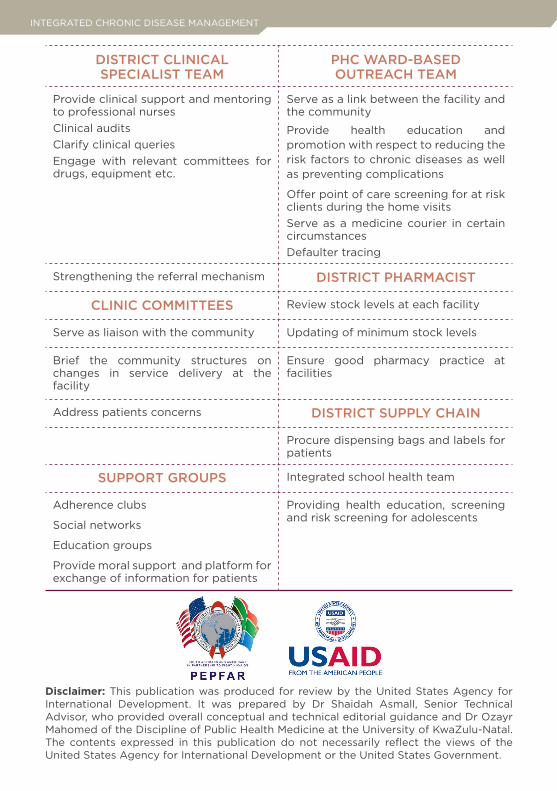
INTEGRATED CHRONIC DISEASE MANAGEMENT
DISTRICT CLINICAL SPECIALIST TEAM
PHC WARD-BASED OUTREACH TEAM
Provide clinical support and mentoring to professional nursesClinical auditsClarify clinical queriesEngage with relevant committees for drugs, equipment etc.
Serve as a link between the facility and the community
Provide health education and promotion with respect to reducing the risk factors to chronic diseases as well as preventing complications
Offer point of care screening for at risk clients during the home visits Serve as a medicine courier in certain circumstancesDefaulter tracing
Strengthening the referral mechanism DISTRICT PHARMACIST
CLINIC COMMITTEES Review stock levels at each facility
Serve as liaison with the community Updating of minimum stock levels
Brief the community structures on changes in service delivery at the facility
Ensure good pharmacy practice at facilities
Address patients concerns DISTRICT SUPPLY CHAIN
Procure dispensing bags and labels for patients
SUPPORT GROUPS Integrated school health team
Adherence clubs
Social networks
Education groups
Provide moral support and platform for exchange of information for patients
Providing health education, screening and risk screening for adolescents
Disclaimer: This publication was produced for review by the United States Agency for International Development. It was prepared by Dr Shaidah Asmall, Senior Technical Advisor, who provided overall conceptual and technical editorial guidance and Dr Ozayr Mahomed of the Discipline of Public Health Medicine at the University of KwaZulu-Natal. The contents expressed in this publication do not necessarily reflect the views of the United States Agency for International Development or the United States Government.