Embed Size (px)
DESCRIPTION
INTEGRATED RECOVERY Lessons Learned: Implementing IDDT. Organizational / System Aspect 2 County Examples Debbie Innes-Gomberg, Ph.D. -Los Angeles Adrian Carroll, MFT - Stanislaus January 19, 2007. Organization-Wide and IDDT Team Specific. - PowerPoint PPT Presentation
Citation preview

INTEGRATED RECOVERY
Lessons Learned: Implementing IDDT
Organizational / System Aspect2 County Examples
Debbie Innes-Gomberg, Ph.D. -Los AngelesAdrian Carroll, MFT - Stanislaus
January 19, 2007

Organization-Wide and IDDT Team Specific
• IDDT provides principles and tools that can be used organization-wide to improve Co-occurring capability throughout

Organization-Wide and IDDT Team Specific
• IDDT provides principles and tools that can be used organization-wide to improve Co-occurring capability throughout
• As well as build specific enhanced IDDT teams

Organization-Wide Elements:
• Commitment • Philosophy • Training• Access policy• Time unlimited• Outcome monitoring• Self-help • Housing and employment• Residential services• Levels of care• Steering committee

System Elements that Support IDDT Specific Programs:
• Client to staff ratio• Supervising to the model• Team approach• Enhanced trainings• Quality management• Fidelity monitoring• Specific Outcomes• Quality Improvement (forms, processes)• Access to housing (wet, damp, dry)

Use of IDDT in Larger System Change Efforts in L.A.
• Los Angeles County’s Adult Systems of Care Transformation
• Creating a continuum of recovery-oriented services
• Using stages of change to guide service delivery and treatment planning
• Creating strategies for client flow through the continuum of services

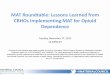
Welcoming/Triage Strategic Services and Supports Wellness Centers Full Service Partnerships Key Focus: short term, intensive welcoming and assessment resulting in quality referrals and enhanced use of community resources
Key Focus: Strategic mental health and supportive services resulting in client movement to wellness services and enhanced recovery.
Key Focus: Self-directed services with peer and professional support geared toward physical/emotional recovery and increased community assimilation
Key Focus: Intensive, whatever it takes service approach for clients who are homeless, incarcerated, in institutions or for whom care is provided solely through the family
IDDT Elements: Integrated assessment and Tx planning, stage-wise interventions, use of motivational interviewing, self-help services, multi-disciplinary treatment team
IDDT Elements: Integrated assessment and Tx planning, stage-wise interventions, use of motivational interviewing, self-help services, family education and support, secondary interventions for non-responders, multi-disciplinary treatment team
IDDT Elements: stage-wise interventions, self-help, family education and support, focus on health and well-being
IDDT Elements: Integrated assessment and Tx planning, stage-wise interventions, use of motivational interviewing, self-help services, family education and support, secondary interventions for non-responders, access to comprehensive services, multi-disciplinary treatment team
MORS levels: 2-7 MORS levels: 3-6 MORS levels: 6-8 MORS levels: At enrollment: 1-2 At graduation: 7
Engagement of clients for < 60 days to determine level of need, using extended assessment and recovery scale referral and linkage to specific service
Evidence based/best practices designed to enhance recovery, engagement, self-coordination and coping skills – short term, intensive and longer term. Including CBT, DBT, illness management, referral to housing and employment specialists within Center
Peer-directed support groups and individualized problem solving, including Wellness Recovery Action Planning
Multidisciplinary team, including housing and employment specialists and a peer advocate. Client to staff ratio <15:1. Interventions geared toward stage of change.
Peer- led Welcoming/ Greeting/Information Dissemination, including use of storytelling to enhance client engagement in services
Group and individual treatment modalities
Healthy living activities, including psychoeducation and health management groups
Emphasis on obtaining housing and employment, with intensive ongoing support and opportunities for community assimilation
Introduction to Peer-Run Services (welcoming and orientation groups for clients who are unengaged and for those who are engaged but poorly self-coordinating)
Integrated dual diagnosis interventions geared toward clients in the contemplation, preparation and action phases.
Medication furnished by Nurse Practitioners
Use of Service Area Navigator to develop community supportive services and enhanced linkage capacity
Medication services Linkage to primary care services, where possible
Crisis Intervention More professional problem-solving assistance than in Wellness Centers
Self-directed crisis management
Medication services Referrals to housing, employment and opportunities for community assimilation
Community integration
Benefits establishment Frequent team review of clients to ensure optimal forward movement
Referrals to housing, employment and opportunities for community assimilation
Referrals to housing, employment and opportunities for community assimilation
COUNTY OF LOS ANGELES – DEPARTMENT OF MENATL HEALTH
ADULT SYSTEMS OF CARE TRANSFORMATION-RECOVERY-BASED LEVELS OF OUTPATIENT CARE

Use of IDDT Model Elements to Enhance Service Delivery in L.A.
• Focus on person-centered treatment planning
• Team-based services
• Stage-based assessment and interventions based on readiness for change

COUNTY OF LOS ANGELES – DEPARTMENT OF MENTAL HEALTH
ADULT SYSTEMS OF CARE
Big 7 Organizational Transformation
I. Domains of Change: Staff Transformation (enhancing staff belief in recovery, instilling hope in
staff). Staff-consumer interactions (developing welcoming environments,
developing successful strategies to work with challenging individuals). Organizational structures and processes (collecting and using quality of
life and recovery-based outcome measures, developing structures to promote consumer flow through the system, building strong team structures).
Available services and capacity (developing quality of life support services, strengthening collaboration with other social service agencies, developing community belonging and connections).
II. Values of recovery-oriented change:
Hope Healing Authority Community Engagement
III. Use of Integrated Dual Diagnosis Treatment principles to create a recovery-
oriented service continuum: Integrated assessment and treatment planning. Use of stage-specific interventions that match client readiness for change,
including motivational interviewing. Incorporating self-help services into all levels of care. Team decision-making. Use of SAMHSA-supported practices such as Illness Management, Family
Education and Support, psychoeducation, Supported Housing and Employment
Focus on health and wellness.

SAMHSA 4 Quadrants
• Target population for IDDT are those COD individuals with Serious Mental Illness


Stanislaus experience
• Recovery focus
• Integrated system vs. Integrated treatment
• Wellness Recovery Center
• Exit strategies as a recovery concept
• Identify internal experts and early adopters
• Recovery Milestones


Stanislaus experience
• Stages of change model:
-SATS (AOD)
-MH stages based on Milestones (MH)
-Stage-based treatment
-Staff change model


STAGE
1
2
3
4
5
STAGES OF
CHANGE
Pre-Contemplation
Contemplation
Preparation
Action
Maintenance
STAGES OF
IMPLEMENTATION
Unaware or uninterested
Consensus building
Motivating
Implementing
Sustaining
Steps: 1 Ask important questions
Conduct a needs assessment
Define your rationale
Conduct a baseline fidelity review
Maintain oversight
2 Begin the change process
Develop awareness of available options
Identify stake-holders
Develop a baseline fidelity action plan
Monitor fidelity
3 Identify current practices and rationales
Build consensus Develop stage-wise interventions
Monitor outcomes
4 Examine your mission, values, goals, and vision
Find your “champions”
Acquire and integrate training
Network with others
5 Check it out Identify financial resources
Engage in clinical consultation
Provide ongoing training
6 Engage technical assistance
Assemble a steering committee
Provide stage-wise interventions
Engage in ongoing consultation
7 Assess the pros and cons
Conduct a readiness assessment
Develop and monitor outcomes
Expand services
8 Develop informed consent and consensus
Decide to implement or not
Continue to educate and train stakeholders
Transform the organizational culture
9 Explore concerns Recruit a team leader
Address barriers
10 Plan to start small Address unintended consequences
11 Assemble the multi-disciplinary service team
12
Begin an implementation plan

Stanislaus experience
• System Transformation
-MHSA FSP, 2034, ACT
-Wellness Recovery level of care
-LOCUS LOC system, caseload ratio
-Normalizing use of Primary Care Physician
• Levels of Care


Stanislaus County Behavioral Health and Recovery Services – Draft 7/2005
KEY COMPONENTS (that support Recovery) Stage of Recovery. Clinical Risk. Level of Functioning.
Case Management / Care Coordination
Housing, Employment, Education, and Wraparound Supports
Meds, MD, RN, Physical Health Services
Counseling and Therapy
Psycho-Education
Peer Supports
Family
ACT or ACT-lite Locus: 4
Pre-contemplation to early active treatment. High risk. High degree of impairment.
< 10-15:1 24/7 >50% in field Outreach and engagement. Multidisciplinary teams. Stage-based. Follow while in hospital.
Extensive use of wrap-around supports, housing and employment services. Housing 1st Work 1st.
Readily available. <150:1
MH, IDDT and AOD readily available, as needed. Culturally appropriate and strength based. Group treatment.
Yes
Peers used in engagement and outreach and as role models of hope and recovery. Self-help encouraged.
Family actively engaged as resource, engagement approach and as natural supports.
Intensive Community Supports and Services Locus: 3
Pre-contemplation to Relapse prevention. Moderate to high risk. Moderate to high degree of impairment.
<35-40:1 Multidisciplinary teams. Stage-based.
Housing 1st Work 1st. Independent living and competitive employment are goals.
Readily available.
MH, COD and AOD readily available, as needed. Culturally appropriate and strength based. Group treatment.
Yes
Peers used in engagement and outreach, as well as in building supports, role model hope and recovery. Self-help encouraged.
Family actively engaged as resource, engagement approach and as natural supports. Self-help encouraged.
Mental Health
Adult
Community Supports & Integrated Services (ACSIS)
LEVELS
OF CARE
Wellness Recovery Locus: 2,1
Contemplation to maintenance. Low to moderate risk. Low to moderate impairment.
>40:1, 200:1 Brief episodes of case management.
Peer supports for independent living and competitive employment.
Readily available. Possible med. Rx groups.
As adjunct to peer support, not instead of. Possible use of interns or referral out. Self-help for AOD.
Yes
Extensive use of peer supports as primary component of this level.
Family self-help actively supported.
Non-Specialty Mental Health Primary Care Locus:? 1
Beginning recovery to maintenance. Low to moderate risk. Low to moderate impairment.
Primary Care Physician may provide these services. Medication support, medical services limited counseling, education and community referrals.

Stanislaus experience
• Client flow through System-Early expectations-Ease of re-admission-SSI concerns-PCP relationships-Peer support throughout-Recovery conversation-Transparency of treatment process-Measurement and accountability

Team Structure

SUPPORT WHEEL
Be Selective In Choosing Support Phone Numbers
Phone Numbers
Use In A Circular Manner So Not To Burn Out Any One Source
My Recovery

Cornerstones of Empowerment Developed by Consumers and Family Members
7/08/06
I have the right to know my diagnosis, criteria, and what medications are used to treat said diagnosis AND I have the responsibility to fully participate in my treatment plan. (Welfare & Institutions Code 5325.1)
I have the right to know what my treatment options are AND I have the responsibility to inform and educate staff about what treatments have worked or not worked for me currently and in the past. (Welfare & Institutions Code 5325.1)
I have the right to feel comfortable to ask questions, and have the time to understand and be understood. (Customer services & client empowerment)
I have the right to a name and phone number, map or directions, when referrals are made, and a right to call back if a connection wasn't made AND I have the responsibility to follow through on referrals and to call back if a connection wasn't made. (BHRS Coordination of Services for Consumers and Families 70.1.110)
I have the right to file a complaint and be supported on that AND I have the responsibility to let staff know what complaints or problems I am experiencing with the staff (program) so they can be resolved. If they cannot be resolved then I have the responsibility to file a complaint. (Patients rights)
I have the right to define who I want involved as my family and support system with my treatment AND I have the responsibility to let staff know what family members, friends, support system I want involved with my treatment. (Cultural Competency Clinical Standards, Client & Family Involvement in Services Policy 90.1.111)
I have the right to a choice and explanation of the providers on my treatment team AND that I be an active participant in my treatment. (N.T.T.P Curriculum, Client & Family Involvement in Services Policy 90.1.111)
I have the right to ask for a change of provider when I feel my provider and I are not a good partnership AND I have the responsibility to inform staff about what type of provider I need when I feel my provider and I are not a good partnership. (Patients Rights)
I have the right to be respected for my beliefs, sexual orientation, ethnicity, culture, religion, spirituality, etc AND I have the responsibility to be respectful of others beliefs, sexual orientation, ethnicity, culture, religions, spirituality, etc. (BHRS NON DISCRIMINATION Policy 40.2.108 policy)
I have the right to express, in a considerate way, my feelings and emotions on issues without providers minimizing my concerns AND I have the responsibility not to blame others for my feelings and emotions. (Customer service) I have the right to pursue a safe independent living arrangement that works for me AND I have the responsibility to choose a place to live and to be responsible in maintaining my home. (Recovery Story B. Farr, Wellness Recovery Action Plan) I have the right to know all resources such as support people, self help, warm line, crisis services, officer of the day to call on when my case manager, clinician, counselor is not available AND I have the responsibility to use my support system, develop my unique coping skills and to share them with my provider, family members and others who support me. (Relapse Prevention Plan, Advanced Directives)
I have the right to be fully informed of volunteer opportunities to strengthen my recovery AND I have the responsibility to share my recovery and to participate in opportunities that strengthen my recovery. (Milestones in Recovery)
I have a right to review my medical record according to the H.I.P.A.A. regulations. (BHRS H.I.P.A.A. policy)

Stanislaus experience
• IDDT as model for implementing any EBP-Levels of implementation
• Fidelity Scales as a guide and measure• Promotes team approach
-Multidisciplinary-AOD, Psychiatrist, RN, CM, Clinician, E&H
• Stages-provides conceptual framework to bridge MH/AOD, Harm reduction & recovery-Consumer centered

Summary of Lessons Learned
• QUESTIONS