Embed Size (px)
Citation preview
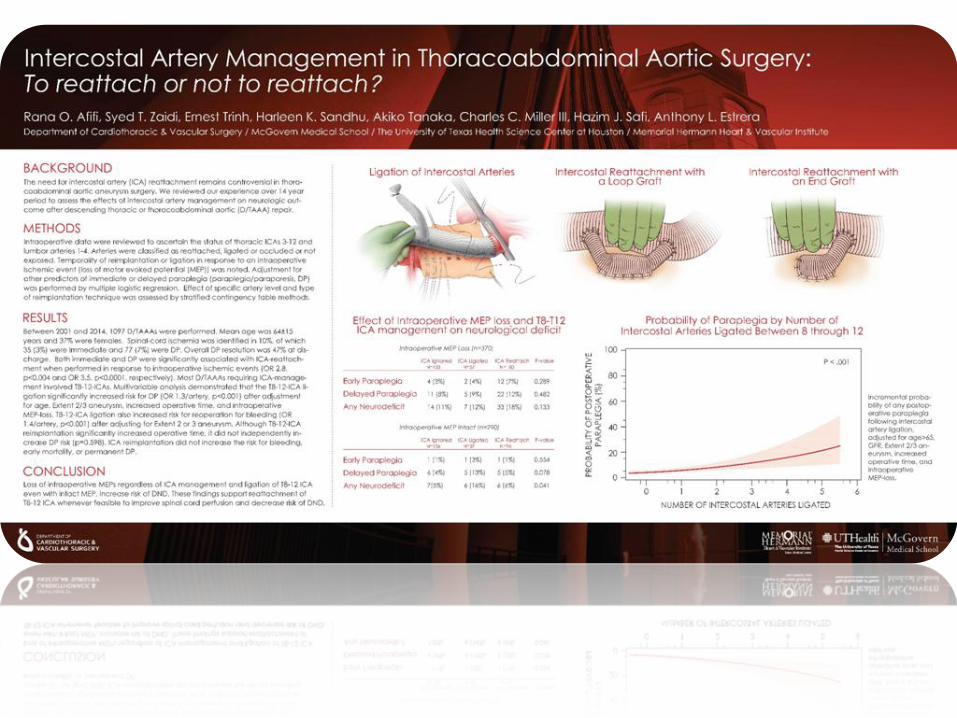
Intercostal Artery Management in
Thoracoabdominal Aortic Surgery: To
reattach or not to reattach? Rana O. Afifi, MD
Department of Cardiothoracic and Vascular Surgery
McGovern Medical School
The University of Texas Science Center at Houston
Memorial Hermann Heart & Vascular Institute
Assistant Professor
No Disclosures

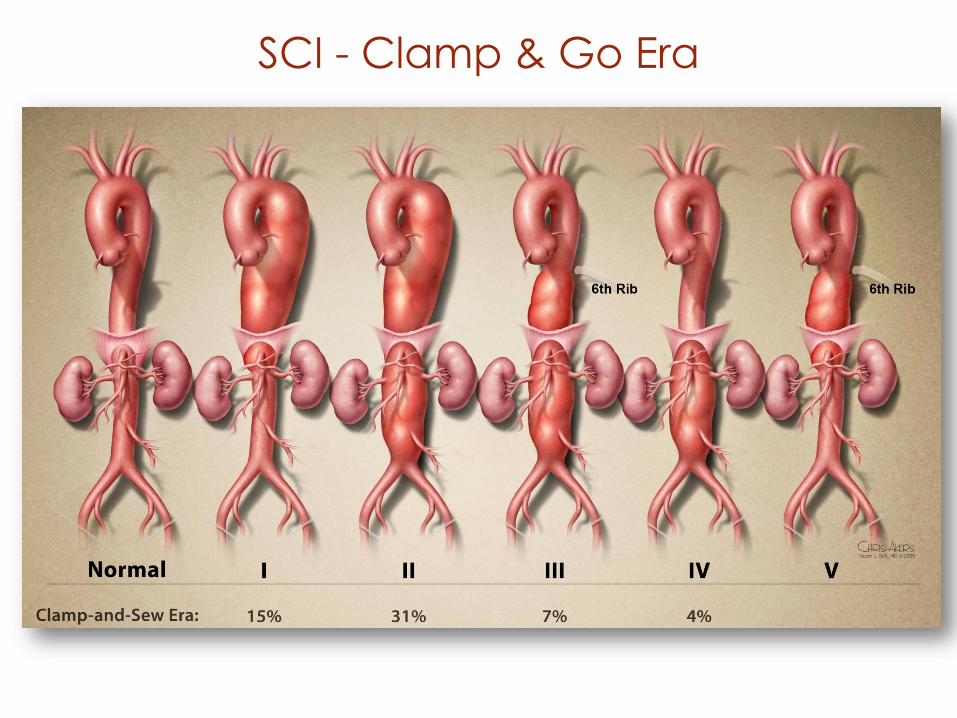
SCI - Clamp & Go Era
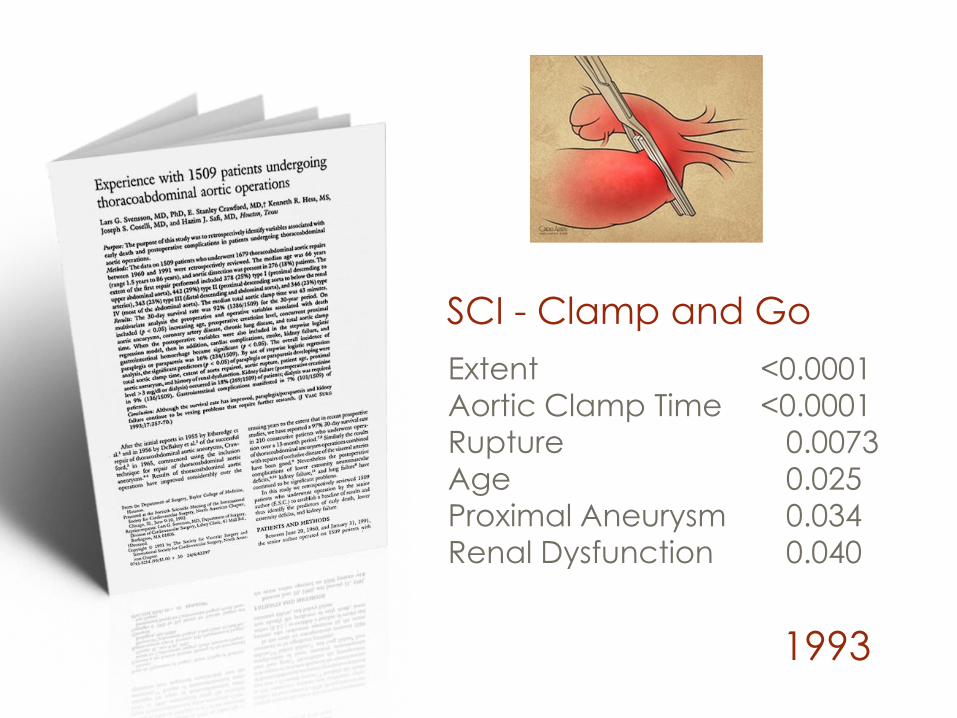
1993
Extent <0.0001
Aortic Clamp Time <0.0001
Rupture 0.0073
Age 0.025 Proximal Aneurysm 0.034
Renal Dysfunction 0.040
SCI - Clamp and Go
Spinal Cord Protection
Rationale for
Spinal Cord Protection
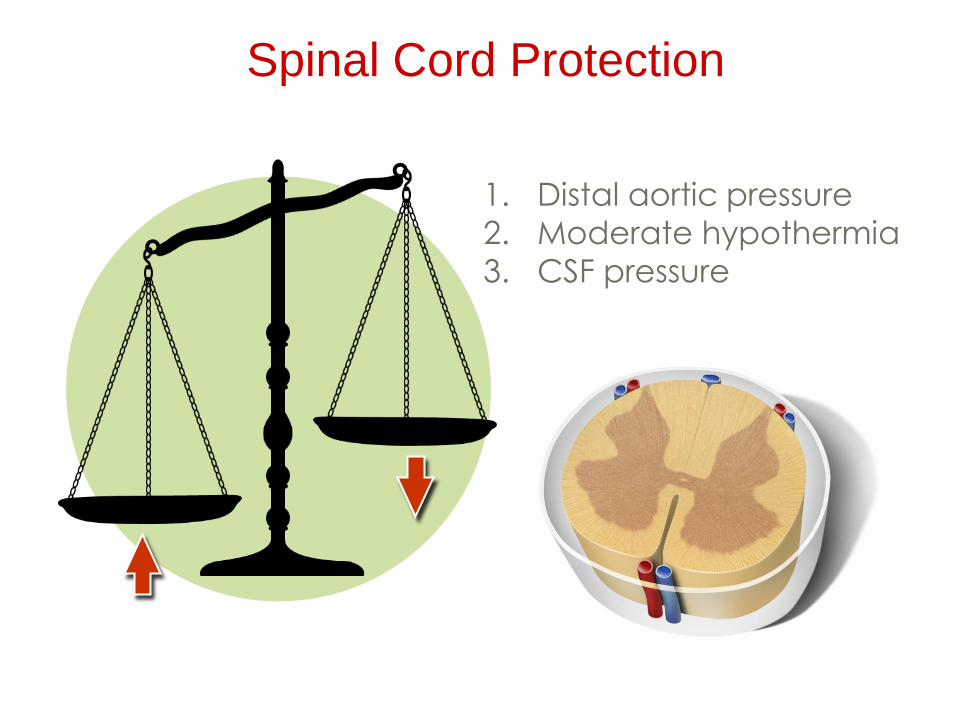
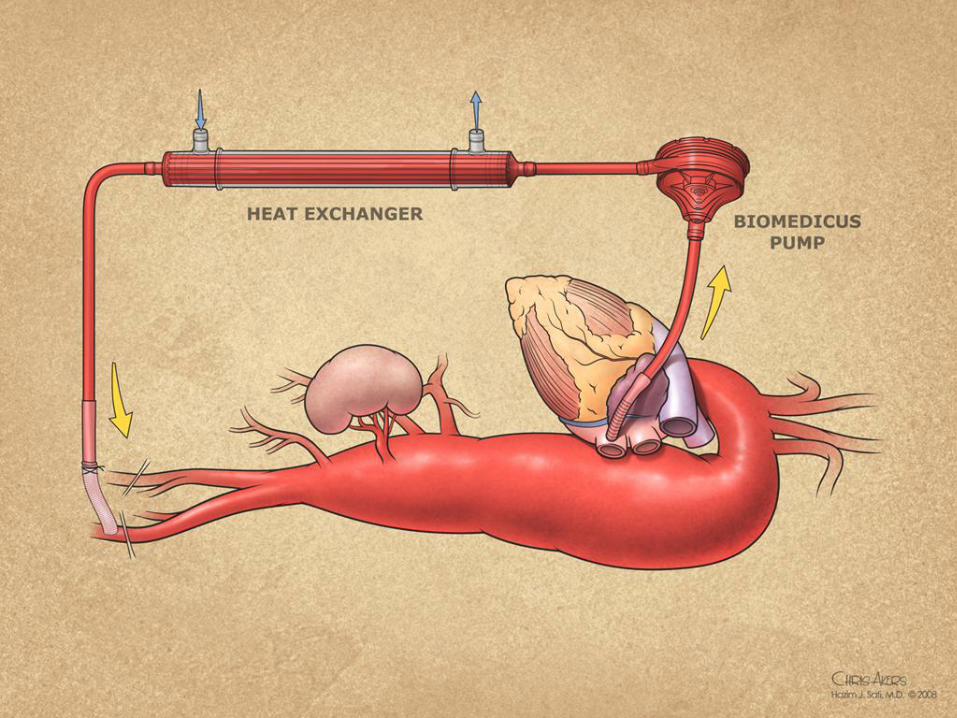
1. Distal aortic pressure
2. Moderate hypothermia
3. CSF pressure
Spinal Cord Protection

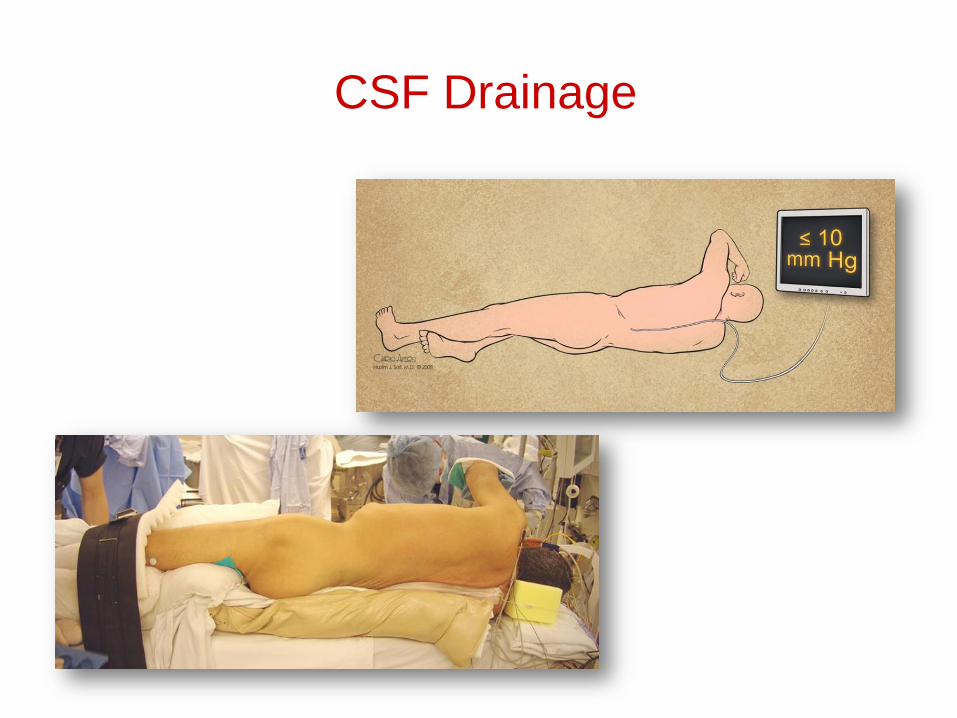
CSF Drainage
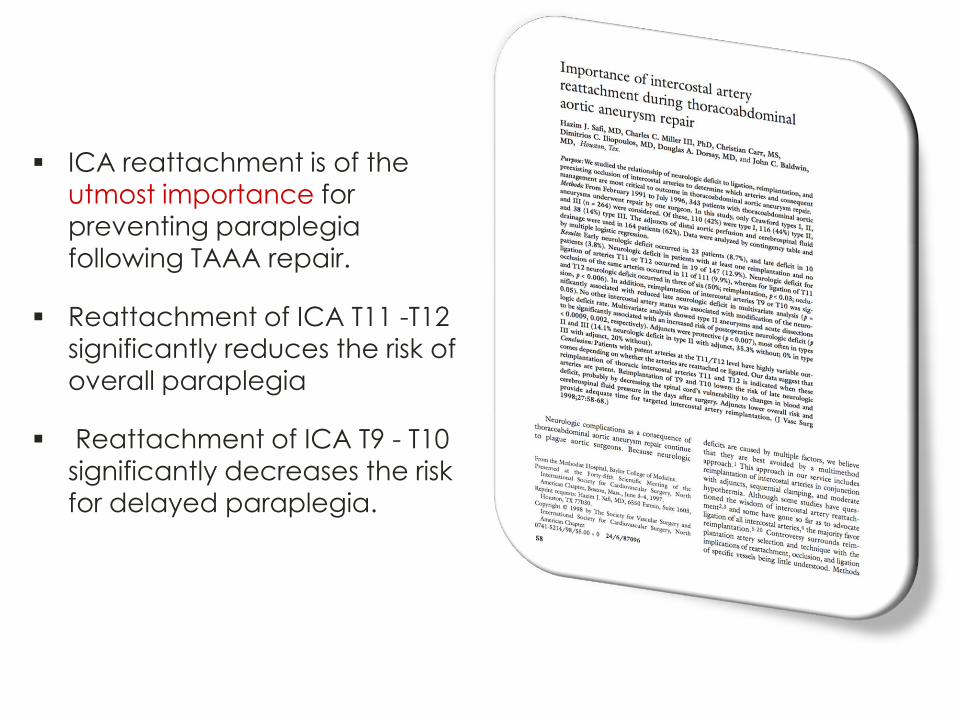
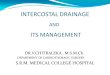
ICA reattachment is of the
utmost importance for
preventing paraplegia
following TAAA repair.
Reattachment of ICA T11 -T12
significantly reduces the risk of
overall paraplegia
Reattachment of ICA T9 - T10
significantly decreases the risk
for delayed paraplegia.
Neuromonitoring

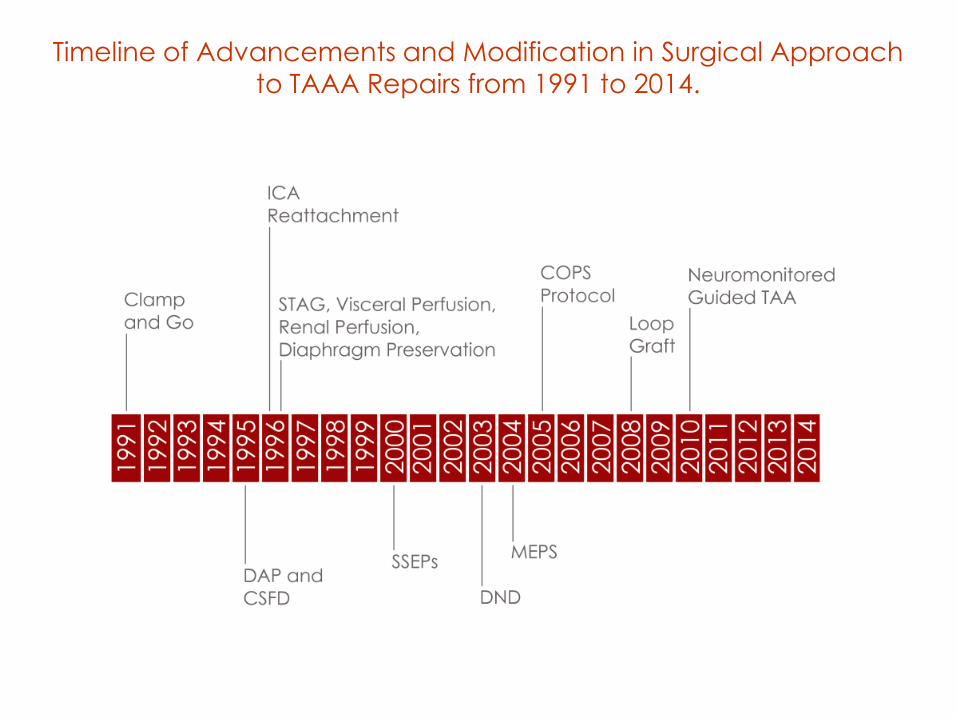
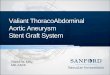
Timeline of Advancements and Modification in Surgical Approach
to TAAA Repairs from 1991 to 2014.
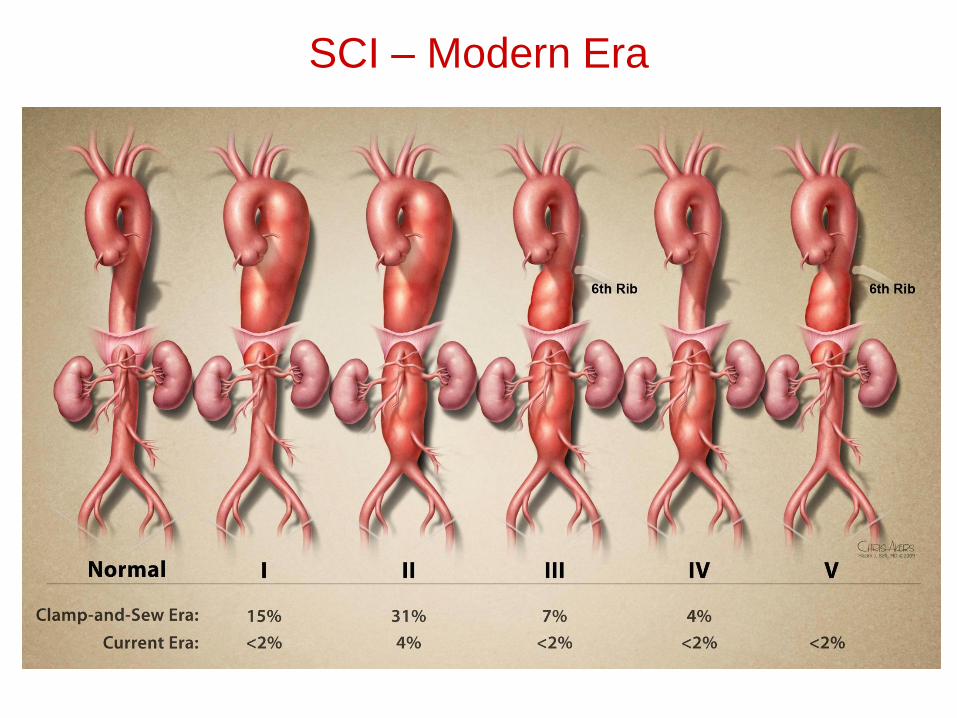
SCI – Modern Era
Collateral Network Concept
Endovascular Era
Methods
We reviewed all cases of open D/TAAA repair between 2001-2014.
We retrospectively reviewed
Patient characteristics
Intraoperative variables and complications
Intraoperative data to ascertain the status of thoracic
ICAs 3-12 and lumbar arteries 1-4.
Postoperative paraplegia was evaluated for this
cohort.
Methods
ICA Status Determination:
Not manipulated
Natively occluded
Not exposed in the surgical field
Ligated
Reattached into the aortic circulation
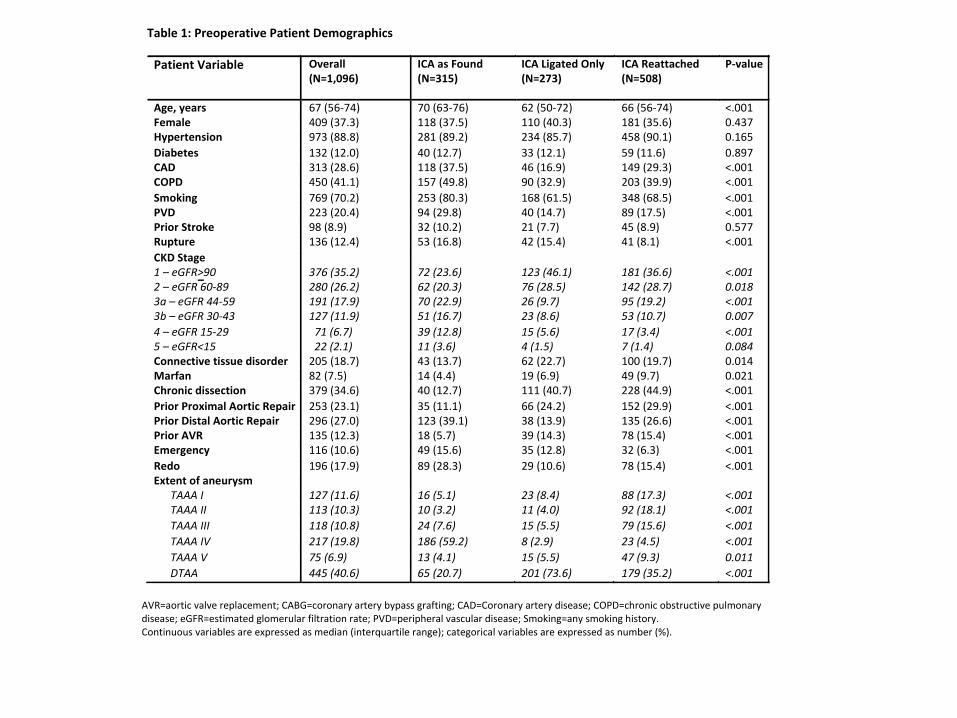
Table1:PreoperativePatientDemographics
PatientVariable Overall(N=1,096)
ICAasFound(N=315)
ICALigatedOnly(N=273)
ICAReattached(N=508)
P-value
Age,years 67(56-74) 70(63-76) 62(50-72) 66(56-74) <.001Female 409(37.3) 118(37.5) 110(40.3) 181(35.6) 0.437Hypertension 973(88.8) 281(89.2) 234(85.7) 458(90.1) 0.165
Diabetes 132(12.0) 40(12.7) 33(12.1) 59(11.6) 0.897CAD 313(28.6) 118(37.5) 46(16.9) 149(29.3) <.001COPD 450(41.1) 157(49.8) 90(32.9) 203(39.9) <.001
Smoking 769(70.2) 253(80.3) 168(61.5) 348(68.5) <.001PVD 223(20.4) 94(29.8) 40(14.7) 89(17.5) <.001PriorStroke 98(8.9) 32(10.2) 21(7.7) 45(8.9) 0.577Rupture 136(12.4) 53(16.8) 42(15.4) 41(8.1) <.001
CKDStage1–eGFR>902–eGFR60-893a–eGFR44-593b–eGFR30-43
4–eGFR15-295–eGFR<15
376(35.2)280(26.2)191(17.9)127(11.9)
71(6.7)22(2.1)
72(23.6)62(20.3)70(22.9)51(16.7)
39(12.8)11(3.6)
123(46.1)76(28.5)26(9.7)23(8.6)
15(5.6)4(1.5)
181(36.6)142(28.7)95(19.2)53(10.7)
17(3.4)7(1.4)
<.0010.018<.0010.007
<.0010.084
Connectivetissuedisorder 205(18.7) 43(13.7) 62(22.7) 100(19.7) 0.014Marfan 82(7.5) 14(4.4) 19(6.9) 49(9.7) 0.021Chronicdissection 379(34.6) 40(12.7) 111(40.7) 228(44.9) <.001
PriorProximalAorticRepair 253(23.1) 35(11.1) 66(24.2) 152(29.9) <.001PriorDistalAorticRepair 296(27.0) 123(39.1) 38(13.9) 135(26.6) <.001PriorAVR 135(12.3) 18(5.7) 39(14.3) 78(15.4) <.001Emergency 116(10.6) 49(15.6) 35(12.8) 32(6.3) <.001
Redo 196(17.9) 89(28.3) 29(10.6) 78(15.4) <.001Extentofaneurysm TAAAI 127(11.6) 16(5.1) 23(8.4) 88(17.3) <.001TAAAII 113(10.3) 10(3.2) 11(4.0) 92(18.1) <.001
TAAAIII 118(10.8) 24(7.6) 15(5.5) 79(15.6) <.001
TAAAIV 217(19.8) 186(59.2) 8(2.9) 23(4.5) <.001
TAAAV 75(6.9) 13(4.1) 15(5.5) 47(9.3) 0.011
DTAA 445(40.6) 65(20.7) 201(73.6) 179(35.2) <.001
AVR=aorticvalvereplacement;CABG=coronaryarterybypassgrafting;CAD=Coronaryarterydisease;COPD=chronicobstructivepulmonarydisease;eGFR=estimatedglomerularfiltrationrate;PVD=peripheralvasculardisease;Smoking=anysmokinghistory.Continuousvariablesareexpressedasmedian(interquartilerange);categoricalvariablesareexpressedasnumber(%).
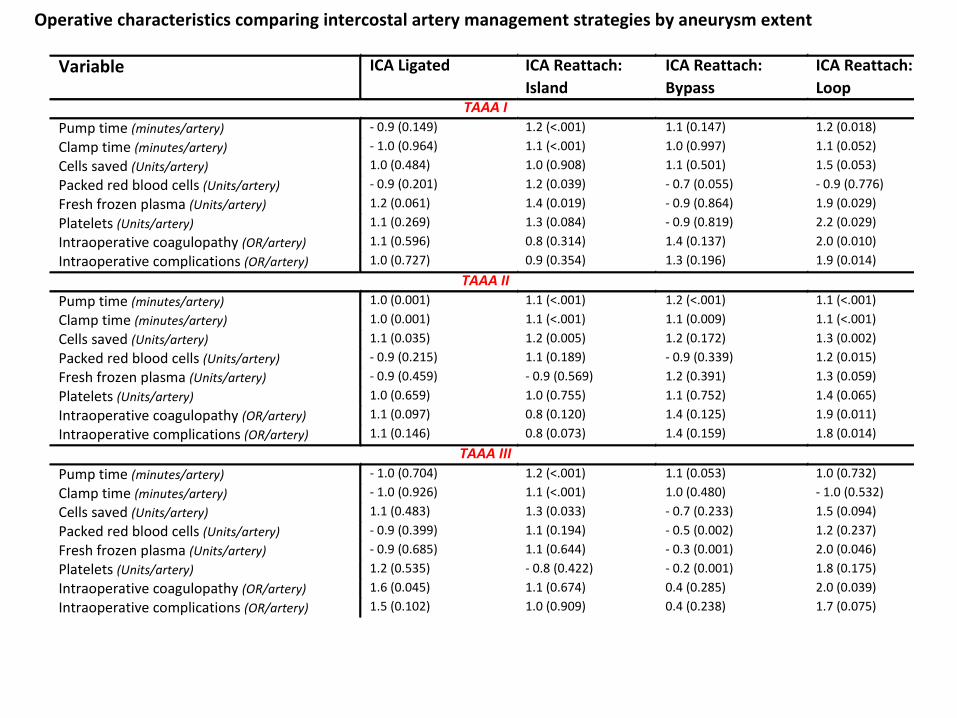
Operativecharacteristicscomparingintercostalarterymanagementstrategiesbyaneurysmextent
Variable ICALigated ICAReattach:
Island
ICAReattach:
Bypass
ICAReattach:
LoopTAAAI
Pumptime(minutes/artery) -0.9(0.149) 1.2(<.001) 1.1(0.147) 1.2(0.018)
Clamptime(minutes/artery) -1.0(0.964) 1.1(<.001) 1.0(0.997) 1.1(0.052)
Cellssaved(Units/artery) 1.0(0.484) 1.0(0.908) 1.1(0.501) 1.5(0.053)
Packedredbloodcells(Units/artery) -0.9(0.201) 1.2(0.039) -0.7(0.055) -0.9(0.776)
Freshfrozenplasma(Units/artery) 1.2(0.061) 1.4(0.019) -0.9(0.864) 1.9(0.029)
Platelets(Units/artery) 1.1(0.269) 1.3(0.084) -0.9(0.819) 2.2(0.029)
Intraoperativecoagulopathy(OR/artery) 1.1(0.596) 0.8(0.314) 1.4(0.137) 2.0(0.010)
Intraoperativecomplications(OR/artery) 1.0(0.727) 0.9(0.354) 1.3(0.196) 1.9(0.014)
TAAAII
Pumptime(minutes/artery) 1.0(0.001) 1.1(<.001) 1.2(<.001) 1.1(<.001)
Clamptime(minutes/artery) 1.0(0.001) 1.1(<.001) 1.1(0.009) 1.1(<.001)
Cellssaved(Units/artery) 1.1(0.035) 1.2(0.005) 1.2(0.172) 1.3(0.002)
Packedredbloodcells(Units/artery) -0.9(0.215) 1.1(0.189) -0.9(0.339) 1.2(0.015)
Freshfrozenplasma(Units/artery) -0.9(0.459) -0.9(0.569) 1.2(0.391) 1.3(0.059)
Platelets(Units/artery) 1.0(0.659) 1.0(0.755) 1.1(0.752) 1.4(0.065)
Intraoperativecoagulopathy(OR/artery) 1.1(0.097) 0.8(0.120) 1.4(0.125) 1.9(0.011)
Intraoperativecomplications(OR/artery) 1.1(0.146) 0.8(0.073) 1.4(0.159) 1.8(0.014)
TAAAIII
Pumptime(minutes/artery) -1.0(0.704) 1.2(<.001) 1.1(0.053) 1.0(0.732)
Clamptime(minutes/artery) -1.0(0.926) 1.1(<.001) 1.0(0.480) -1.0(0.532)
Cellssaved(Units/artery) 1.1(0.483) 1.3(0.033) -0.7(0.233) 1.5(0.094)
Packedredbloodcells(Units/artery) -0.9(0.399) 1.1(0.194) -0.5(0.002) 1.2(0.237)
Freshfrozenplasma(Units/artery) -0.9(0.685) 1.1(0.644) -0.3(0.001) 2.0(0.046)
Platelets(Units/artery) 1.2(0.535) -0.8(0.422) -0.2(0.001) 1.8(0.175)
Intraoperativecoagulopathy(OR/artery) 1.6(0.045) 1.1(0.674) 0.4(0.285) 2.0(0.039)
Intraoperativecomplications(OR/artery) 1.5(0.102) 1.0(0.909) 0.4(0.238) 1.7(0.075)
Results
Early paraplegia : 35/1,096 (3.2%) patients.
Delayed paraplegia : 77/1,061 (7.3%) patients.
Results
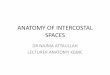
MEPs were available for only 660/1,096 (60%) of the cohort.
MEPs were lost in 370/660 (56%) of cases during surgery
332 of these (90%) recovered in the operating room.
13 (3.5%) did so after anesthesia maneuvers
74 (20%) following distal aortic perfusion
112 (31%) after restoration of distal pulsatile flow
133 (36%) after segmental artery reattachment
(p<0.0001; Cochran-Armitage test for trend)
Study Limitations
A retrospective study.
MEP monitoring began only after 2004. Therefore, data on
MEPs were available for only (60%) of the cohort.
The analysis focused mainly on ICAs T8-12
The lack anatomical information regarding collateral
circulation status .

Conclusions
Increased risk of delayed paraplegia :
Loss of intraoperative MEPs.
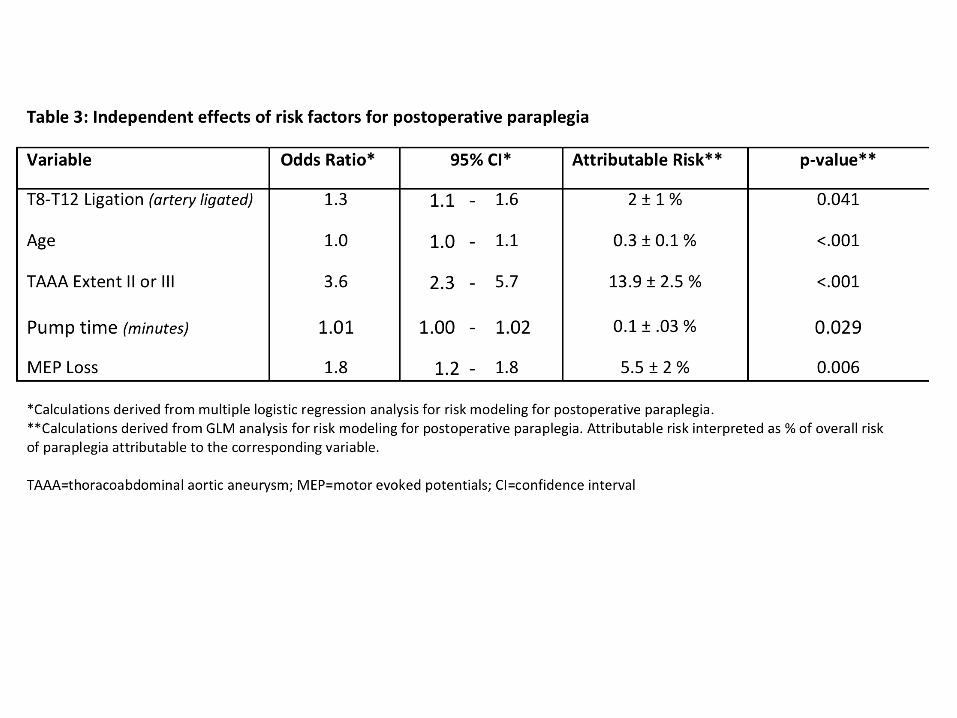
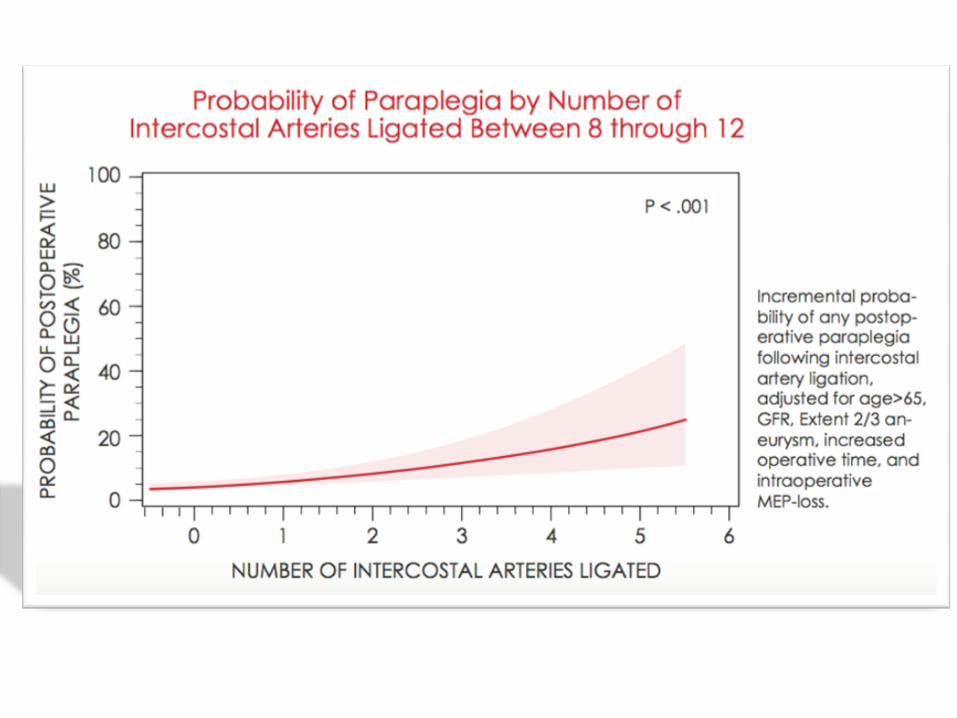
Ligation of T8-12 ICA (even with intact MEPs).
These findings support reattachment of T8-12 ICA,
whenever feasible, to improve spinal cord perfusion and
prevent delayed paraplegia.
1998 2017

Thank You