Embed Size (px)
Citation preview

ftiapap
Interleukin-2 Profiles Shortly After Tacrolimus Conversion From aTwice-Daily to Once-Daily RegimenA. Meçule, F. Tinti, A. Bachetoni, L. Poli, M. D’Alessandro, C. Alessandri, I. Umbro, I. Nofroni,P.B. Berloco, and A.P. Mitterhofer
ABSTRACT
A number of studies have indicated that kidney recipients can be safely converted from thetwice-daily formulation (Tac-T) to the same dose of a once-daily tacrolimus (TAC)regimen (Tac-O) based upon monitoring of renal function. Conversion from Tac-T toTac-O is commonly followed by a reduction in Tac trough levels, estimated by someauthors to be about 20%. These alterations seem to not be associated with a modificationof graft function, but study of inflammatory cytokines would be useful. The aims of ourstudy were to monitor Tac, C-reactive protein (CRP), and interleukin (IL)-2 levels as wellas to evaluate renal function among stable renal transplant patients converted from aTac-T to a Tac-O regimen. We enrolled 10 consecutive stable kidney transplanted patients.Tac trough levels, serum creatinine concentrations, glomerular filtration rates using theModification of Diet in Renal Disease formula (MDRD), CRP, and clinical assessmentwere performed monthly for 6 months before and 3 months after the conversion. Afterconversion we observed a slight but not significant reduction in Tac trough level. Renalfunction evaluated by serum creatinine and MDRD as well as CRP were not significantlydifferent after conversion. IL-2 levels remained stable after conversion. We identified agroup of patients showing reduced Tac trough levels below the therapeutic range and agroup with stable Tac levels. No significant differences were observed among the twogroups before versus after the conversion. Our results did not show a modification of IL-2,CRP and renal function levels, at 3 months after conversion despite the lower Tac troughconcentrations. The clinical meaning of Tac trough alterations is not clear. They mightreflect inter- and intraindividual differences in the clearance of Tac as recently described.
They did not seem to be associated with activation of an inflammatory pathway.mci
KIDNEY TRANSPLANTATION is the treatment ofchoice for patients with end-stage renal disease. The
use of immunosuppressive drugs requires a fine balancebetween adequate immunosuppression to prevent rejectionand excessive treatment leading to toxic, infectious, andneoplastic complications. The calcineurin inhibitor tacroli-mus (Tac) remains an important immunosuppressant, sinceits use has led to acute rejection rates as low as 10% at 1year after transplantation.1 This clinical objective resultsrom individualized dosing regimens achieved by therapeu-ic drug monitoring (TDM) seeking to target calcineurmnhibitor (CNI) exposure in terms of area under the curvend trough levels. Indeed, TDM has become routine clinicalractice in renal transplantation; it has been related to lowercute rejection as well as toxicity rates. Tac inhibits the
hosphatase activity of calcineurin in a dosage-dependent© 2011 Published by Elsevier Inc.360 Park Avenue South, New York, NY 10010-1710
Transplantation Proceedings, 43, 1017–1019 (2011)
anner, leading to reduction in the production of a range ofytokines, particularly interleukin-2 (IL-2), which are involvedn transplant rejection.
From the Department of Clinical Medicine, Nephrology andDialysis Unit (A.M., F.T., I.U., A.P.M.), Sapienza University ofRome, Rome, Italy; Department of General Surgery, OrganTransplant Unit “Paride Stefanini” (A.B., L.P., M.D., P.B.B.),Sapienza University of Rome, Rome, Italy; Department of Inter-nal Medicine and Medical Specialities (C.A.), Sapienza Universityof Rome, Rome, Italy; and Department of Experimental Medicineand Pathology (I.N.), Sapienza University of Rome, Rome, Italy.
This study was supported by the Consorzio Interuniversitarioper I Trapianti.
Address reprint requests to Anna Paola Mitterhofer, Vialedell’Università 37, 00185 Rome, Italy. E-mail: annapaola.mitter@
uniromal.it0041-1345/–see front matterdoi:10.1016/j.transproceed.2011.02.047
1017

goc
cboTt
af
fifp(b
tXp(
s
letTp
s�awera
umw
ISM
1018 MEÇULE, TINTI, BACHETONI ET AL
A number of studies have indicated that kidney recipientscan be safely converted based upon renal function from thetwice-daily formulation (Tac-T) to the same dose of once-daily Tac (Tac-O).2–4 Tac is a critical dose drug with anarrow therapeutic window and large interindividual andintraindividual pharmacokinetic variabilities.5,6 Recently,enetic studies have demonstrated that the various patternsf cytochrome genotypes influence slower or faster Taclearance.7 A significant correlation has been shown be-
tween a high within-patient variability in Tac clearance andworse graft survival. These patients have greater incidenceof subclinical episodes leading to chronic rejection and tolong-term graft dysfunction.8 Subclinical rejections areharacterized by the absence of creatinine modifications,ut alterations of C-reactive protein (CRP) and expressionf cytokines, including IL-2 and IL-6.9,10 Conversion fromac-T to Tac-O is commonly followed by a reduction in Tac
rough levels,3,11 which has been estimated by some authorsat about 20%.12 These alterations seem to not be associatedwith modifications of graft function, but there is the issue oftheir effects on inflammatory cytokines. The aims of ourstudy were to monitor Tac, CRP, and IL-2 levels as well asto evaluate renal function among stable renal transplantpatients converted from a Tac-T to a Tac-O regimen.
MATERIALS AND METHODS
From February 2010, we enrolled 10 consecutive, stable kidneytransplant patients treated with Tac mycophenolate mofetil, andless than 10 mg/daily corticosteroids. Eligibility criteria were: age18 to 70 years; stable Tac-T regimen for �6 months with stablerenal function; and 3 to 5 years posttransplantation. Patients wereconverted from Tac-T to Tac-O at the same dosage (1 mg: 1 mg)The Tac-T patients were of mean age 58 � 6 years; 6 were malend 4 were female; 9 received a cadaveric transplant; mean timerom transplantation was 43.3 � 6 months.
Tac trough levels, serum creatinine concentrations, glomerularltration rates using the Modification of Diet in Renal Diseaseormula (MDRD), CRP content, and clinical assessments wereerformed monthly for 6 months before (T6–T0) and 3 monthsT1–T3) after conversion. Each patient served as his own controlased upon values before versus after conversion.Tac trough levels were maintained in the therapeutic range of 4
o 10 ng/mL, as measured by the Flex technique (DimensionPand System) according to the product insert. The accuracy andrecision were evaluated by the International Testing SchemeD.W. Holt, St Georges Hospital Medical School, London, UK).
The Immunoturbidity Latex Test was performed for CRP mea-urements (�g/L; with normal range 100–6000). Plasma samples
were collected at baseline (before conversion, T0) and at 3 monthsthereafter (T3) to assess IL-2 content. Commercially availablemultiplex bead-based immunoassay kits (Human 27-plex, Bio-Radlaboratories, Hercules, Calif, USA) were used to measure IL-2concentrations using assays performed according to the manufac-turer’s instructions. Each sample was assayed in duplicate. Datawere analyzed with Bio-Plex manager software, version 4.1.1(Bio-Rad laboratories). Values with a coefficient of variation�12% were excluded from the final data analysis. The concentra-tions (pg/mL) of various analytes in the plasma samples weredetermined with the aid of standard curves generated in the
multiplex assays.Statistical Techniques
We preliminarily performed a descriptive analysis consisting ofpercentages, averages, and standard deviations. Because the datashowed normality despite the limited sample size, we employedparametric methods for an inferential approach. The homogeneityof variances was evaluated with the Levene test. Mean variationsand total area of distributions were evaluated with Student t test forpaired data. All tests were performed using SPSS system 18.0(SPSS Inc, Chicago, Ill, USA) with P values below .05 consideredsignificant.
RESULTS
Pre- and postconversion values of Tac trough levels, renalfunction, CRP and IL-2 levels are reported in Table 1. Weobserved a slight but insignificant reduction in Tac troughlevels after conversion. Renal function evaluated by serumcreatinine and MDRD were not significantly different afterconversion as well as CRP. IL-2 levels remained stable afterconversion.
Among our patients, we identified two groups based onTac trough levels: group A (n � 5) showed a reductionbelow the therapeutic range and group B (n � 5), stable Tacevels. No alterations of renal function or significant differ-nces in markers of inflammation were observed betweenhe two groups before versus after conversion (Table 2).here were no episodes of acute rejection among ouratients.
DISCUSSION
A number of studies have indicated that kidney recipientscan be safely converted from the Tac-T to the same dose ofthe Tac-O daily formulation. Conversion from Tac-T toTac-O is commonly followed by a reduction in Tac troughlevels3,11 estimated by some authors to be about 20%.12 Inome de novo kidney transplant recipients sometimes50% higher doses of Tac-O dosage have been required to
chieve therapeutic concentrations.4 In all of these studiese did not observe a modification of graft function param-ters among converted or de novo patients. Consideringenal function monitoring, we excluded the presence ofcute rejection episodes but not subclinical ones.
Alterations of CRP and cytokine profiles, IL-2 in partic-lar, have been demonstrated to be a reliable inflammatoryarker suggestive of subclinical rejection.8,9 In our study,e assessed IL-2 levels, which are considered to be the
Table 1. Pre- and Postconversion Values
Preconversion Postconversion P
Tacrolimus (ng/mL) 5.0 � 1.3 4.3 � 1.4 .147CRP (�g/L) 3483 � 1013 5400 � 10,033 .714L-2 (pg/mL) 5 � 0 5 � 0erum creatinine (mg/dL) 1.7 � 0.5 1.8 � 0.5 .239DRD (mL/min) 43.6 � 15.5 53.7 � 21.5 .133
Results are expressed as mean � SD. Preconversion: mean of values in the6 months before conversion; postconversion: mean of values in the 3 months
after conversion. CRP, C-reactive protein; IL-2, interleukine-2; MDRD, Modifi-cation of Diet in Renal Disease formula; SD, standard deviation.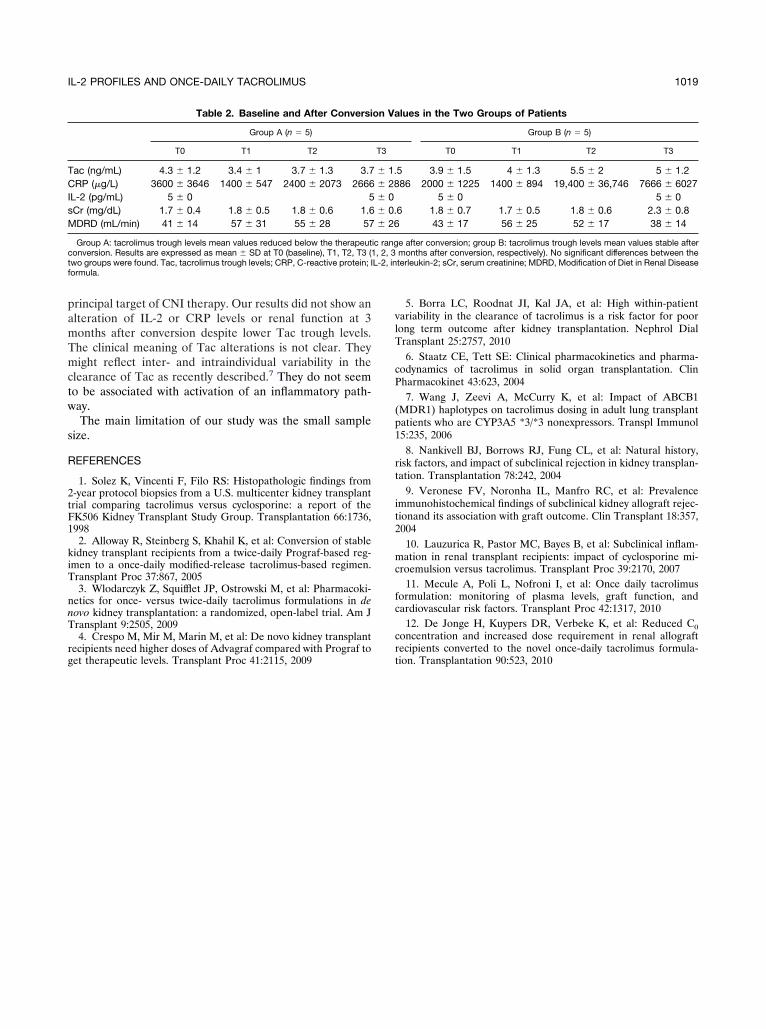
tw
s
CIsM
L-2, in
IL-2 PROFILES AND ONCE-DAILY TACROLIMUS 1019
principal target of CNI therapy. Our results did not show analteration of IL-2 or CRP levels or renal function at 3months after conversion despite lower Tac trough levels.The clinical meaning of Tac alterations is not clear. Theymight reflect inter- and intraindividual variability in theclearance of Tac as recently described.7 They do not seemo be associated with activation of an inflammatory path-ay.The main limitation of our study was the small sample
ize.
REFERENCES
1. Solez K, Vincenti F, Filo RS: Histopathologic findings from2-year protocol biopsies from a U.S. multicenter kidney transplanttrial comparing tacrolimus versus cyclosporine: a report of theFK506 Kidney Transplant Study Group. Transplantation 66:1736,1998
2. Alloway R, Steinberg S, Khahil K, et al: Conversion of stablekidney transplant recipients from a twice-daily Prograf-based reg-imen to a once-daily modified-release tacrolimus-based regimen.Transplant Proc 37:867, 2005
3. Wlodarczyk Z, Squifflet JP, Ostrowski M, et al: Pharmacoki-netics for once- versus twice-daily tacrolimus formulations in denovo kidney transplantation: a randomized, open-label trial. Am JTransplant 9:2505, 2009
4. Crespo M, Mir M, Marin M, et al: De novo kidney transplant
Table 2. Baseline and After Conversi
Group A (n � 5)
T0 T1 T2
Tac (ng/mL) 4.3 � 1.2 3.4 � 1 3.7 � 1.3 3.7RP (�g/L) 3600 � 3646 1400 � 547 2400 � 2073 2666
L-2 (pg/mL) 5 � 0 5Cr (mg/dL) 1.7 � 0.4 1.8 � 0.5 1.8 � 0.6 1.6DRD (mL/min) 41 � 14 57 � 31 55 � 28 57
Group A: tacrolimus trough levels mean values reduced below the therapeutconversion. Results are expressed as mean � SD at T0 (baseline), T1, T2, T3 (two groups were found. Tac, tacrolimus trough levels; CRP, C-reactive protein; Iformula.
recipients need higher doses of Advagraf compared with Prograf toget therapeutic levels. Transplant Proc 41:2115, 2009
5. Borra LC, Roodnat JI, Kal JA, et al: High within-patientvariability in the clearance of tacrolimus is a risk factor for poorlong term outcome after kidney transplantation. Nephrol DialTransplant 25:2757, 2010
6. Staatz CE, Tett SE: Clinical pharmacokinetics and pharma-codynamics of tacrolimus in solid organ transplantation. ClinPharmacokinet 43:623, 2004
7. Wang J, Zeevi A, McCurry K, et al: Impact of ABCB1(MDR1) haplotypes on tacrolimus dosing in adult lung transplantpatients who are CYP3A5 *3/*3 nonexpressors. Transpl Immunol15:235, 2006
8. Nankivell BJ, Borrows RJ, Fung CL, et al: Natural history,risk factors, and impact of subclinical rejection in kidney transplan-tation. Transplantation 78:242, 2004
9. Veronese FV, Noronha IL, Manfro RC, et al: Prevalenceimmunohistochemical findings of subclinical kidney allograft rejec-tionand its association with graft outcome. Clin Transplant 18:357,2004
10. Lauzurica R, Pastor MC, Bayes B, et al: Subclinical inflam-mation in renal transplant recipients: impact of cyclosporine mi-croemulsion versus tacrolimus. Transplant Proc 39:2170, 2007
11. Mecule A, Poli L, Nofroni I, et al: Once daily tacrolimusformulation: monitoring of plasma levels, graft function, andcardiovascular risk factors. Transplant Proc 42:1317, 2010
12. De Jonge H, Kuypers DR, Verbeke K, et al: Reduced C0concentration and increased dose requirement in renal allograft
lues in the Two Groups of Patients
Group B (n � 5)
T0 T1 T2 T3
5 3.9 � 1.5 4 � 1.3 5.5 � 2 5 � 1.286 2000 � 1225 1400 � 894 19,400 � 36,746 7666 � 6027
5 � 0 5 � 06 1.8 � 0.7 1.7 � 0.5 1.8 � 0.6 2.3 � 0.8
43 � 17 56 � 25 52 � 17 38 � 14
e after conversion; group B: tacrolimus trough levels mean values stable aftermonths after conversion, respectively). No significant differences between theterleukin-2; sCr, serum creatinine; MDRD, Modification of Diet in Renal Disease
on Va
T3
� 1.� 28� 0� 0.� 26
ic rang1, 2, 3
recipients converted to the novel once-daily tacrolimus formula-tion. Transplantation 90:523, 2010





























