Embed Size (px)
Citation preview
Journal of Substance Abuse Tre
Regular article
Interpersonal maladjustment as predictor of mothersT response to a
relational parenting intervention
Nancy E. Suchman, (Ph.D.)a,*, Thomas J. McMahon, (Ph.D.)a, Suniya S. Luthar, (Ph.D.)b
aYale University School of Medicine, Psychosocial Substance Abuse Research Center, VA-CT Healthcare System,
950 Campbell Ave. (151D), West Haven, CT 06516, USAbDepartment of Human Development, Teachers College, Columbia University, New York, NY 10027-6696, USA
Received 6 September 2003; received in revised form 2 May 2004; accepted 15 June 2004
Abstract
In previous work, Luthar and Suchman (2000, Development & Psychopathology, 12, 235) reported results of a randomized clinical
trial testing the efficacy of the Relational Psychotherapy MothersT Group (RPMG) for methadone-maintained mothers. In this extension,
we examined maternal interpersonal maladjustment as a predictor of differential response to RPMG versus standard drug counseling (DC).
We predicted that RPMG mothers with high levels of interpersonal maladjustment would improve on parent-child relationship indices,
whereas DC mothers with high levels of interpersonal maladjustment would show no improvement. Fifty-two mothers enrolled in the
study completed baseline, post-treatment and 6-month followup assessments and a subset of 24 btargetQ children between the ages of
7 and 16 completed measures on mothersT parenting. As predicted, results of hierarchical regression analyses indicated moderate
interpersonal maladjustment � treatment interaction effects for all parenting outcomes at post-treatment and for a subset of outcomes at
followup. Plotted interactions confirmed predictions that, as maternal interpersonal maladjustment increased, parenting problems improved
for RPMG mothers and remained the same or worsened for DC mothers. Results indicate the potential value of interpersonally oriented
interventions for substance-abusing mothers and their children. D 2004 Elsevier Inc. All rights reserved.
Keywords: Parent-child relations; Parent training; Parenting skills; Family relations; Child abuse
1. Introduction
In previous work, Luthar and Suchman (2000) tested the
efficacy of the Relational Psychotherapy MothersT Group
(RPMG), an adjunct parenting intervention for mothers in
methadone maintenance, in comparison with standard drug
counseling (DC) provided at methadone clinics. Concep-
tually derived from Interpersonal Psychotherapy (Klerman,
Weissman, Rounsaville, & Chevron 1984) and relational
theories of womenTs drug addiction (Finkelstein, 1996),
RPMG was designed to concurrently foster opiate addicted
mothersT interpersonal development in multiple relational
contexts (i.e. peers, family, and children) and provide direct
0740-5472/04/$ – see front matter D 2004 Elsevier Inc. All rights reserved.
doi:10.1016/j.jsat.2004.06.003
* Corresponding author. Tel.: +1 203 937 3486, ext. 7430; fax: +1 203
937 3472.
E-mail address: [email protected] (N.E. Suchman).
guidance for resolving common parenting dilemmas encoun-
tered by addicted mothers. Results from the randomized
clinical trial indicated that RPMG was more effective
than DC for reducing mothersT maltreatment of children
and improving mother-child affective relationships; post-
treatment results were largely sustained at the 6-month
followup. (See Luthar & Suchman, 1999, 2000 for support-
ing rationale and detailed report of the clinical trial).
In the present analysis of data from that study, we sought
to evaluate whether maternal interpersonal maladjustment
would be a predictor of differential parenting outcomes (e.g.
child maltreatment, positive parenting behaviors) in RPMG
vs. DC. Interpersonal maladjustment, (the degree to which
destructive interpersonal behaviors such as arguments,
excessive control, and passivity interfere with oneTs capacityto seek support and assistance), is highly prevalent among
substance abusing women (Amaro & Hardy-Fanta, 1995;
atment 27 (2004) 135–143

N.E. Suchman et al. / Journal of Substance Abuse Treatment 27 (2004) 135–143136
Byington, 1997; Finkelstein, 1996; Harden, 1998; Hender-
son, Boyd, & Mieczkowski, 1994; Mayes, 1995) and often
viewed as a major impediment to their treatment success.
Within the framework of relational theories of womenTsaddiction (Byington, 1997; Finkelstein, 1996), interpersonal
dysfunction is a precipitant of psychological distress that
bspills overQ into parenting practices. In light of these vul-
nerabilities, we were interested in determining if mothers
reporting higher levels of interpersonal maladjustment
would be more responsive to RPMG—with its central focus
on peer and parent-child relationships—than to standard
drug counseling.
Although no studies to our knowledge have examined
predictors of response to relational parenting interven-
tions, previous work has identified predictors of behav-
ioral parent training outcomes as well as interpersonal
therapies for depression. In addition to socioeconomic
disadvantage, parental psychopathology, parental stress
and inadequate parenting skills (Kazdin, 1997; Webster-
Stratton, 1998; Webster-Stratton & Hammond, 1999), a
number of relational factors have also predicted poor
response to parent training, including marital discord
(Dadds, Schwartz, & Sanders, 1987), single marital status
among parents in low socioeconomic strata (Webster-
Stratton, 1985), and lack of involvement in social, school,
and community networks (Dumas & Wahler, 1983;
Webster-Stratton, 1998). There is also evidence (Dadds
et al., 1987) that, for parents experiencing marital discord,
supplementing child management training with a rela-
tional couplesT intervention can improve parentsT responseto behavioral parent training.
Studies examining predictors of differential response to
interpersonally oriented therapies have also identified a
number of matching effects. In the NIMH Treatment of
Depression Collaborative Research Program, Interpersonal
Psychotherapy (IPT) was found to be less effective than
cognitive-behavior therapy in treating patients with avoi-
dant personality traits (Barber & Muenz, 1996), equally
effective for patients with high levels of perfectionism or
need for approval (Blatt, Quinlan, Pilkonis, & Shea, 1995),
and more effective among patients with obsessive person-
ality traits (Barber & Muenz, 1996) or lower levels of
social dysfunction (Sotsky et al., 1991). Although the last
finding linking lower levels of social dysfunction to better
response to IPT suggests that low levels of interpersonal
maladjustment might similarly be associated with a better
response to the conceptually similar RPMG, two factors
preclude this prediction. First, the findings reported by
Sotsky and colleagues (1991) were found in primarily male
subjects and therefore may not generalize to an all-female
population. Second, unlike IPT, RPMG is an intensive
interpersonal group treatment targeting improvement in the
parent-child relationship. Based on RPMGTs intensive
interpersonal focus, we expected to see an interaction
between mothersT level of interpersonal maladjustment and
response to the two therapies. Specifically, in this analysis
we expected that mothers with high levels of interpersonal
maladjustment receiving RPMG would show improvement
on parent-child relationship indices (e.g., risk for child
maltreatment, positive parenting) whereas mothers receiv-
ing DC alone would show either no improvement or a
decline on these indices.
2. Materials and methods
2.1. Overview of procedures
Heroin-addicted mothers interested in participating in
parenting groups were recruited at three methadone clinics
in New Haven, CT. Recruitment occurred via several
means, including referrals from counselors, visits made by
research assistants to ongoing drug-counseling groups and
medication lines, and referrals from mothers who had
already participated in the study. To be eligible for
inclusion, mothers had to (a) be in methadone treatment
for a heroin problem, (b) have children less than 16 years
of age, and (c) report subjective experiences of problems
with parenting. Exclusion criteria included conditions that
would impede benefit from group therapy such as
cognitive deficits, psychotic thought processes, and suici-
dality (for a more detailed description of methods, see
Luthar & Suchman, 2000).
All eligible mothers who expressed interest in the
study met with a research assistant who explained the
nature of the study and completed consent procedures.
Mothers were enrolled in the study as openings occurred.
Initial assessments were scheduled with those who agreed
to participate and mothers were randomized to either
RPMG or the comparison condition (DC) for a duration
of 48 weeks (24 weeks treatment, 24 weeks followup).
The RPMG condition entailed weekly RPMG groups in
addition to standard treatment at the clinic, whereas in
the comparison condition mothers received standard
treatment alone.
Each participant was asked to identify one of her children
about whom she was most concerned, and these identified
children of age 7 years and older were brought in to
complete assessments whenever possible. Mothers and
target children were assessed at baseline, post-treatment,
and 6-month followup. Although all of the measures
completed by mothers were written at a fourth grade reading
level and mothers were typically able to read and respond to
items independently, a research assistant was available to
assist those participants who were unfamiliar with certain
words or phrases when necessary. During interviews with
younger children (e.g., ages 7–11) the research assistant was
seated facing the child, read each item aloud, and the child
marked his or her response on an answer form that was
beyond the research assistantTs viewing range. Older
children (e.g., ages 12–16) were typically able to complete
questionnaires independently.

N.E. Suchman et al. / Journal of Substance Abuse Treatment 27 (2004) 135–143 137
To compensate families for time spent in assessments,
a staggered reimbursement schedule was used, such that
mothers and children were paid, $15 and $5 respec-
tively, for baseline assessments, $30 and $10 on
treatment completion, and $50 and $15 at the 6-month
followup assessment.
As in all clinical research involving parents and minor
children, the research protocol required that all instances of
possible child abuse and neglect be reported to the proper
authorities (e.g., the state Department of Children and
Families). The research protocol also required that mothers
and children identified as being at risk for serious or
heightened psychological disturbance be assisted in obtain-
ing appropriate followup evaluation and treatment. At-risk
mothers and children were identified and brought to the
attention of the Project Director, N. S., either by the research
therapists conducting RPMG or by research assistants
conducting assessment interviews. Specific guidelines for
identifying mothers and children at risk (e.g., verbal
acknowledgement of abuse or neglect during assessment
interviews or group sessions, scores beyond clinical cut-off
scores on research questionnaires) were established and the
clinical status of all active research participants was
reviewed in weekly clinical supervision meetings with the
RPMG clinical supervisor and weekly research staff meet-
ings with the Project Director.
During the study, minor children of four mothers were
identified by the research and/or research clinicians as
being at risk for abuse and neglect. Three instances
involved mothers with open cases at the state child
welfare services, so the mothersT methadone clinicians
contacted the respective case workers to report the
incidents. One instance involved potential abuse by a
stepfather. In this case the mother chose to make a report
to child welfare before leaving the methadone clinic.
Because this study was conducted in conjunction with
standard treatment at methadone clinics, referrals of
mothers for further evaluation and treatment was done
by their methadone clinicians. During the study, five
children were identified as being at risk for psychosocial
maladjustment. The Project Director met with mothers to
discuss concerns and arrange referrals to child guidance
clinics for further evaluation.
2.2. Sample
Sixty-one mothers enrolled in methadone maintenance
were randomized to treatment. Of the 37 mothers assigned to
RPMG, 32 completed treatment and post-treatment assess-
ments and 28 of the treatment completers also completed
followup assessments. Of the 24 mothers assigned to DC, 20
completed treatment and post-treatment assessments and 19
of the treatment completers also completed followup assess-
ments. Of the 52 mothers who completed post-treatment
assessments, 18 had children younger than 7 years of age, and
10 were unable to bring their children to the clinic at both
post-treatment and followup. Thus, post-treatment and fol-
lowup assessments were obtained for a total of 24 children
(12 RPMG, 12 DC).
Demographic data for the sample are reported elsewhere
(see Luthar & Suchman, 2000). On average, mothers in the
sample were single, Caucasian, high-school educated women
between 27 and 41 years of age. The majority of mothers
met criteria for low SES on HollingsheadTs two-factor
scale (Hollingshead & Redlich, 1958). Participants had an
average of 2.3minor children less than 16 years of age in their
care. The mean age for target children in the sample was 9.5
(SD = 4.5). Mothers and children in the two conditions
(RPMG and DC) did not differ significantly on any
demographic variable.
2.3. Treatment
2.3.1. RPMG intervention
The RPMG groups were led by female therapists in
order to optimize womenTs comfort in discussing sensitive
issues such as those relating to their own victimization.
Sessions were led by a clinical psychologist who was
assisted by a drug counselor from the methadone clinic,
thus bringing therapeutic expertise across diverse domains
including child development, womenTs psychology, and
addiction-related issues. No patients from the drug
counselorTs individual case load were enrolled in the
study, to insure that the drug counselorsT training in the
RPMG approach did not influence standard treatment of
subjects enrolled in the study. All sessions were semi-
structured, and a therapistTs manual (Luthar, Suchman, &
Boltas, 1997) providing a detailed outline for addressing
each session topic was used. Prior to beginning their
groups, all therapists delivering the RPMG intervention
received training that involved discussions on underlying
theory and specific therapeutic skills, review of session
videotapes, and an overview of the therapist manual
contents. Each group session was videotaped and RPMG
therapists received clinical supervision on a weekly basis.
2.3.2. Standard drug counseling
Treatment in the methadone clinics entailed participation
in weekly, 1-hr counseling groups in addition to pharmaco-
logical intervention (methadone) and periodic meetings with
case managers to secure basic needs (e.g., employment,
housing, welfare benefits, legal aid, and psychiatric referrals).
The weekly groups provided the standard drug counseling
that is used in methadone clinics (see Mercer, Carpenter,
Daley, Patterson, & Volpicelli, 1994; Zackon, McAuliffe, &
ChTien, 1994). Typically led by certified drug counselors andnurses, these groups are generally focused on providing
information on the unfolding of addictions, specific triggers
and pitfalls of addictive behaviors, changing addictive life-
styles, and developing coping strategies to avoid relapses.
The counselorTs stance involves frequent use of didactic
approaches and confrontation of behaviors viewed as

N.E. Suchman et al. / Journal of Substance Abuse Treatment 27 (2004) 135–143138
counterproductive to the goal of abstinence (Mercer et al.,
1994; Zackon et al., 1994).
2.4. Measures
2.4.1. Child maltreatment
The Parental Acceptance/Rejection Questionnaire
(PARQ; Rohner, 1991), a 60-item measure rated on a
4-point scale, was used to assess child maltreatment. The
PARQ yields a composite Maltreatment score comprised of
four subscales: Aggression/Hostility (e.g., bI tell my child
that s/he gets on my nervesQ), Neglect/Indifference (e.g., bIignore my child as long as s/he does not do anything to
disturb meQ), Undifferentiated Rejection (e.g., bI tell my
child I am ashamed of him/her when s/he misbehavesQ),and low expressed Warmth/Affection (e.g., reversed item:
bI try to help my child when s/he is scared or upsetQ).Parallel versions of the PARQ respectively assess mothersTand childrenTs perceptions of maternal behaviors. Compo-
site scores between 90 and 110 on both the mother and
child versions are considered to be within normal limits;
scores above 110 indicate risk for child maltreatment
(Rohner, 1991). Adequate psychometric properties have
been documented for the PARQ (Rohner, 1991). For
this sample, CronbachTs alpha coefficients for the four
subscales ranged between .72 and .89 (median .85) for
the mothers and between .72 and .94 (median .88) for
the children.
2.4.2. Positive parenting
The Parent-Child Relationship Inventory (PCRI;
Gerard, 1994), a 78-item measure rated on a 4-point scale,
served as the measure for positive parenting behaviors. The
PCRI consists of six content subscales, including Commu-
nication, Involvement, Limit Setting, Autonomy, Satisfac-
tion and Support. Three of these subscales were used to
measure mothersT positive parenting behaviors: Communi-
Table 1
Results of two-way ANOVAs examining differences in attendance, additional serv
maladjustment, and treatment � MIM interaction
Treatment (RPMG vs. DC) F
Matern
(MIM
Post-tx Followup Post-tx
Attendance 1.10 n/a .42
Additional services
Medical .00 2.41 .01
Employment 2.84 .70 .05
Drug .21 1.14 .38
Legal .27 .92 .47
Family .26 .46 .35
Psychosocial .29 2.28 .28
Other .85 .38 .01
Social Desirability .01 .07 .55
* p b .05.
cation (e.g., bMy child tells me all about his or her friendsQ),Involvement (e.g., bSometimes I wonder how I would
survive if anything were to happen to my childQ), and Limit
Setting (e.g., reversed item: bI have a hard time getting
through to my childQ). T-scores of 40 and below on any
of the subscales indicate clinically significant problems
(Gerard, 1994). The PCRI also contains a 5-item Social
Desirability scale (e.g., bI have never had any problems with
my childQ) to identify parents who are responding with a
defensive response set. Scores of 9 and below on the Social
Desirability Scale suggest that a subject is trying to appear
to be an excellent parent. Adequate psychometric properties
have been reported for the PCRI (Gerard, 1994; Heinze &
Grisso, 1996), and for this sample, CronbachTs alpha
coefficients for the subscales ranged between .61 and .80,
with a median of .77.
2.4.3. Maternal interpersonal maladjustment
The Social Adjustment Scale (SAS-SR; Weissman &
Bothwell, 1976), a 48-item measure rated on a 5-point
scale that has been used extensively with methadone
patients (Kosten, Rounsaville, & Kleber, 1987; Rounsa-
ville, Kosten, Weissman, & Kleber, 1986), served as the
measure of interpersonal maladjustment. The SAS consists
of five qualitative subscales: Instrumental Role Perform-
ance, Friction, Interpersonal Relations, Feelings and
Satisfactions, and Global Judgments. Two of these
subscales focus explicitly on maladaptive interpersonal
behavior. The Interpersonal Relations Subscale (e.g.,
bHave you been able to talk about your feelings and
problems with at least one of your friends/relatives/partner
during the last 2 weeks?Q) was designed to identify
reticence, hypersensitivity, withdrawal, and dependency in
relationships in social, family, and marital contexts. The
Friction Subscale (e.g., bHave you had any arguments with
people at work in the last two weeks?Q) assesses
the prevalence of open arguments and opposition in
ices, and social desirability scores by treatment group, level of interpersona
al Interpersonal Maladjustment
) (High vs. Low) F
Treatment � MIM
interaction F
Followup Post-tx Followup
n/a .09 n/a
4.33* .21 4.13*
.42 .50 .22
.01 .41 .37
.92 1.48 2.82
.04 .00 .33
.07 .00 1.61
.14 .37 .00
1.36 .14 .18
l
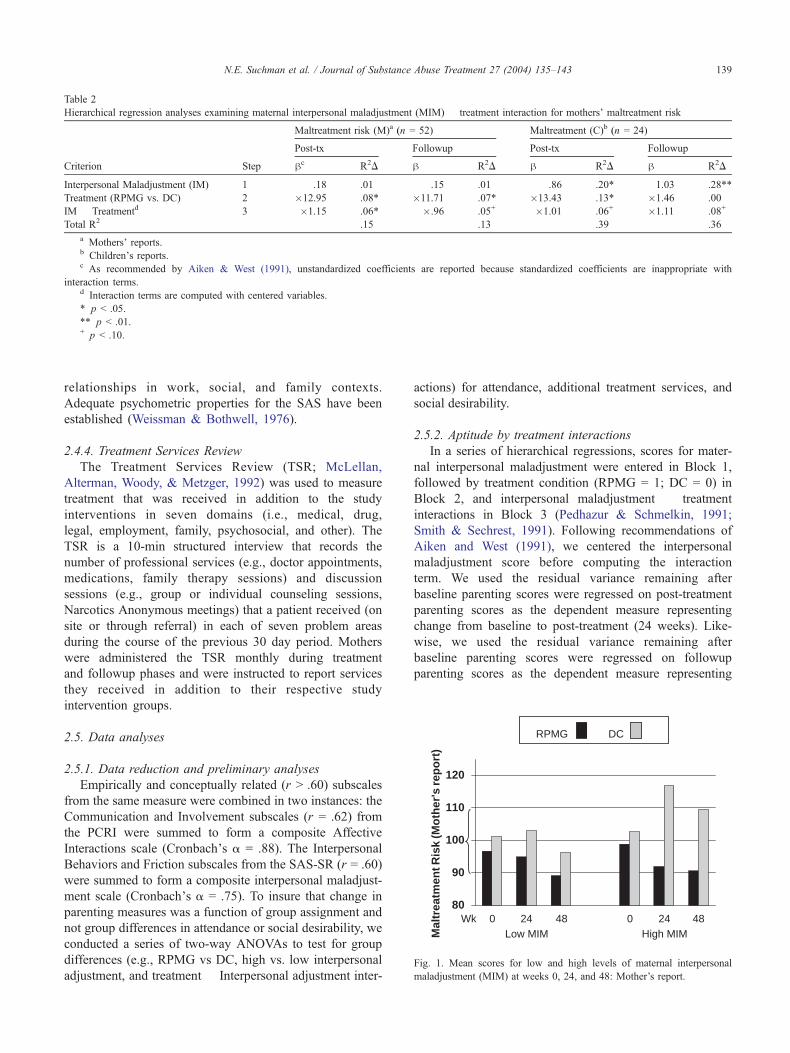
Table 2
Hierarchical regression analyses examining maternal interpersonal maladjustment (MIM) � treatment interaction for mothersT maltreatment risk
Criterion Step
Maltreatment risk (M)a (n = 52) Maltreatment (C)b (n = 24)
Post-tx Followup Post-tx Followup
hc R2D h R2D h R2D h R2D
Interpersonal Maladjustment (IM) 1 .18 .01 .15 .01 .86 .20* 1.03 .28**
Treatment (RPMG vs. DC) 2 �12.95 .08* �11.71 .07* �13.43 .13* �1.46 .00
IM � Treatmentd 3 �1.15 .06* �.96 .05+ �1.01 .06+ �1.11 .08+
Total R2 .15 .13 .39 .36
a MothersT reports.b ChildrenTs reports.c As recommended by Aiken & West (1991), unstandardized coefficients are reported because standardized coefficients are inappropriate with
interaction terms.d Interaction terms are computed with centered variables.
* p b .05.
** p b .01.+ p b .10.
Wk80
90
100
110
120
Mal
trea
tmen
t Ris
k (M
oth
er's
rep
ort
)
0 024 2448 48Low MIM High MIM
RPMG DC
Fig. 1. Mean scores for low and high levels of maternal interpersonal
maladjustment (MIM) at weeks 0, 24, and 48: Mother’s report.
N.E. Suchman et al. / Journal of Substance Abuse Treatment 27 (2004) 135–143 139
relationships in work, social, and family contexts.
Adequate psychometric properties for the SAS have been
established (Weissman & Bothwell, 1976).
2.4.4. Treatment Services Review
The Treatment Services Review (TSR; McLellan,
Alterman, Woody, & Metzger, 1992) was used to measure
treatment that was received in addition to the study
interventions in seven domains (i.e., medical, drug,
legal, employment, family, psychosocial, and other). The
TSR is a 10-min structured interview that records the
number of professional services (e.g., doctor appointments,
medications, family therapy sessions) and discussion
sessions (e.g., group or individual counseling sessions,
Narcotics Anonymous meetings) that a patient received (on
site or through referral) in each of seven problem areas
during the course of the previous 30 day period. Mothers
were administered the TSR monthly during treatment
and followup phases and were instructed to report services
they received in addition to their respective study
intervention groups.
2.5. Data analyses
2.5.1. Data reduction and preliminary analyses
Empirically and conceptually related (r N .60) subscales
from the same measure were combined in two instances: the
Communication and Involvement subscales (r = .62) from
the PCRI were summed to form a composite Affective
Interactions scale (CronbachTs a = .88). The Interpersonal
Behaviors and Friction subscales from the SAS-SR (r = .60)
were summed to form a composite interpersonal maladjust-
ment scale (CronbachTs a = .75). To insure that change in
parenting measures was a function of group assignment and
not group differences in attendance or social desirability, we
conducted a series of two-way ANOVAs to test for group
differences (e.g., RPMG vs DC, high vs. low interpersonal
adjustment, and treatment � Interpersonal adjustment inter-
actions) for attendance, additional treatment services, and
social desirability.
2.5.2. Aptitude by treatment interactions
In a series of hierarchical regressions, scores for mater-
nal interpersonal maladjustment were entered in Block 1,
followed by treatment condition (RPMG = 1; DC = 0) in
Block 2, and interpersonal maladjustment � treatment
interactions in Block 3 (Pedhazur & Schmelkin, 1991;
Smith & Sechrest, 1991). Following recommendations of
Aiken and West (1991), we centered the interpersonal
maladjustment score before computing the interaction
term. We used the residual variance remaining after
baseline parenting scores were regressed on post-treatment
parenting scores as the dependent measure representing
change from baseline to post-treatment (24 weeks). Like-
wise, we used the residual variance remaining after
baseline parenting scores were regressed on followup
parenting scores as the dependent measure representing
Mal
trea
tmen
t R
isk
(Ch
ild's
rep
ort
)
Wk80
90
100
110
120
0 024 2448 48Low MIM High MIM
RPMG DC
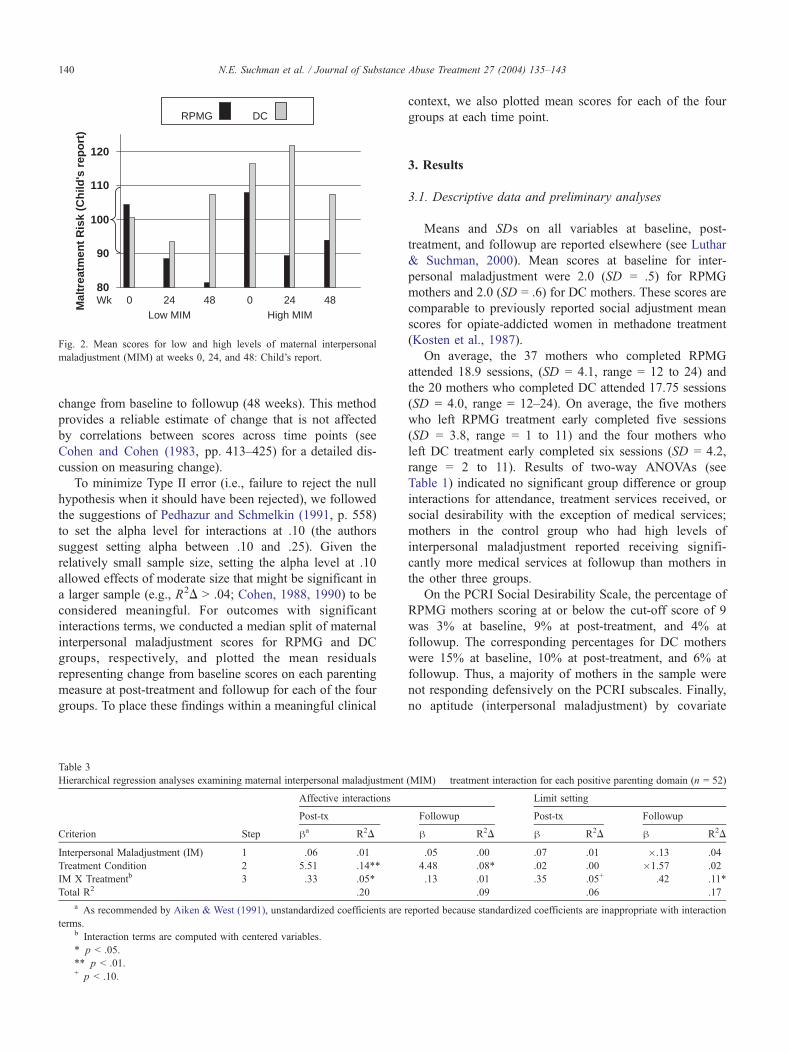
Fig. 2. Mean scores for low and high levels of maternal interpersonal
maladjustment (MIM) at weeks 0, 24, and 48: Child’s report.
N.E. Suchman et al. / Journal of Substance Abuse Treatment 27 (2004) 135–143140
change from baseline to followup (48 weeks). This method
provides a reliable estimate of change that is not affected
by correlations between scores across time points (see
Cohen and Cohen (1983, pp. 413–425) for a detailed dis-
cussion on measuring change).
To minimize Type II error (i.e., failure to reject the null
hypothesis when it should have been rejected), we followed
the suggestions of Pedhazur and Schmelkin (1991, p. 558)
to set the alpha level for interactions at .10 (the authors
suggest setting alpha between .10 and .25). Given the
relatively small sample size, setting the alpha level at .10
allowed effects of moderate size that might be significant in
a larger sample (e.g., R2D N .04; Cohen, 1988, 1990) to be
considered meaningful. For outcomes with significant
interactions terms, we conducted a median split of maternal
interpersonal maladjustment scores for RPMG and DC
groups, respectively, and plotted the mean residuals
representing change from baseline scores on each parenting
measure at post-treatment and followup for each of the four
groups. To place these findings within a meaningful clinical
Table 3
Hierarchical regression analyses examining maternal interpersonal maladjustment
Criterion Step
Affective interactions
Post-tx
ha R2D
Interpersonal Maladjustment (IM) 1 .06 .01
Treatment Condition 2 5.51 .14**
IM X Treatmentb 3 .33 .05*
Total R2 .20
a As recommended by Aiken & West (1991), unstandardized coefficients are
terms.b Interaction terms are computed with centered variables.
* p b .05.
** p b .01.+ p b .10.
context, we also plotted mean scores for each of the four
groups at each time point.
3. Results
3.1. Descriptive data and preliminary analyses
Means and SDs on all variables at baseline, post-
treatment, and followup are reported elsewhere (see Luthar
& Suchman, 2000). Mean scores at baseline for inter-
personal maladjustment were 2.0 (SD = .5) for RPMG
mothers and 2.0 (SD = .6) for DC mothers. These scores are
comparable to previously reported social adjustment mean
scores for opiate-addicted women in methadone treatment
(Kosten et al., 1987).
On average, the 37 mothers who completed RPMG
attended 18.9 sessions, (SD = 4.1, range = 12 to 24) and
the 20 mothers who completed DC attended 17.75 sessions
(SD = 4.0, range = 12–24). On average, the five mothers
who left RPMG treatment early completed five sessions
(SD = 3.8, range = 1 to 11) and the four mothers who
left DC treatment early completed six sessions (SD = 4.2,
range = 2 to 11). Results of two-way ANOVAs (see
Table 1) indicated no significant group difference or group
interactions for attendance, treatment services received, or
social desirability with the exception of medical services;
mothers in the control group who had high levels of
interpersonal maladjustment reported receiving signifi-
cantly more medical services at followup than mothers in
the other three groups.
On the PCRI Social Desirability Scale, the percentage of
RPMG mothers scoring at or below the cut-off score of 9
was 3% at baseline, 9% at post-treatment, and 4% at
followup. The corresponding percentages for DC mothers
were 15% at baseline, 10% at post-treatment, and 6% at
followup. Thus, a majority of mothers in the sample were
not responding defensively on the PCRI subscales. Finally,
no aptitude (interpersonal maladjustment) by covariate
(MIM) � treatment interaction for each positive parenting domain (n = 52)
Limit setting
Followup PostQtx Followup
h R2D h R2D h R2D
.05 .00 .07 .01 �.13 .04
4.48 .08* .02 .00 �1.57 .02
.13 .01 .35 .05+ .42 .11*
.09 .06 .17
reported because standardized coefficients are inappropriate with interaction
60
65
70
75
80
Aff
ecti
ve In
tera
ctio
ns
Wk 0 024 24Low MIM High MIM
RPMG DC
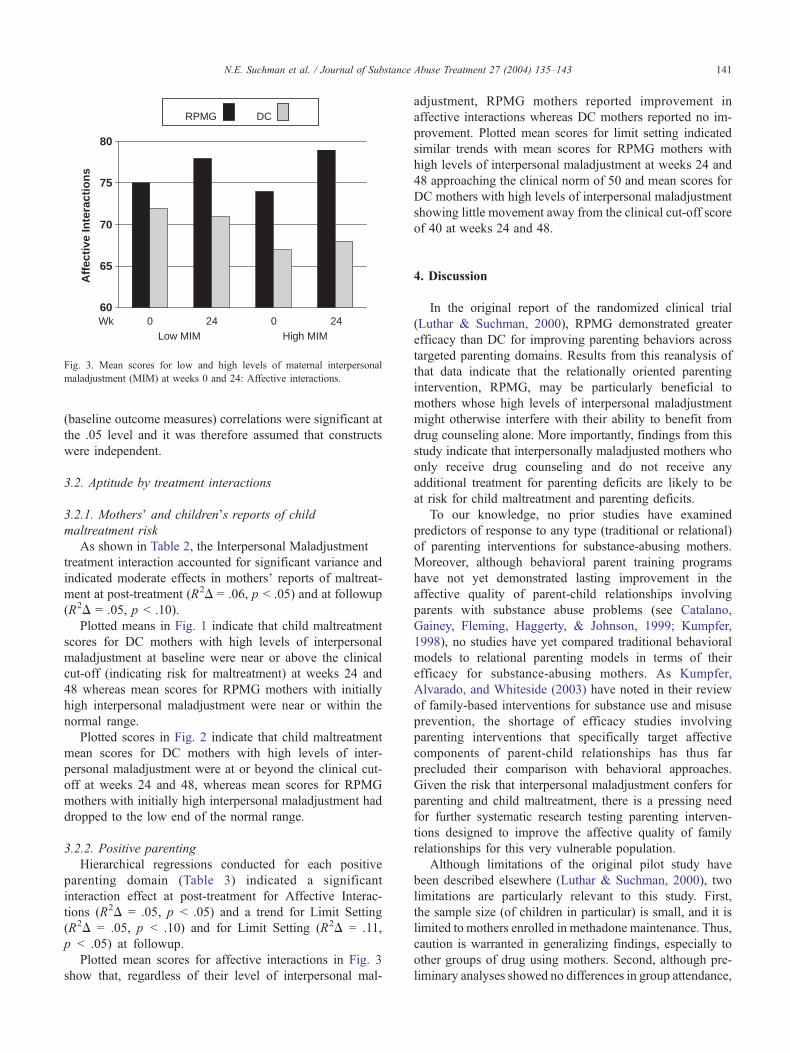
Fig. 3. Mean scores for low and high levels of maternal interpersonal
maladjustment (MIM) at weeks 0 and 24: Affective interactions.
N.E. Suchman et al. / Journal of Substance Abuse Treatment 27 (2004) 135–143 141
(baseline outcome measures) correlations were significant at
the .05 level and it was therefore assumed that constructs
were independent.
3.2. Aptitude by treatment interactions
3.2.1. MothersT and childrenTs reports of childmaltreatment risk
As shown in Table 2, the Interpersonal Maladjustment �treatment interaction accounted for significant variance and
indicated moderate effects in mothersT reports of maltreat-
ment at post-treatment (R2D = .06, p b .05) and at followup
(R2D = .05, p b .10).
Plotted means in Fig. 1 indicate that child maltreatment
scores for DC mothers with high levels of interpersonal
maladjustment at baseline were near or above the clinical
cut-off (indicating risk for maltreatment) at weeks 24 and
48 whereas mean scores for RPMG mothers with initially
high interpersonal maladjustment were near or within the
normal range.
Plotted scores in Fig. 2 indicate that child maltreatment
mean scores for DC mothers with high levels of inter-
personal maladjustment were at or beyond the clinical cut-
off at weeks 24 and 48, whereas mean scores for RPMG
mothers with initially high interpersonal maladjustment had
dropped to the low end of the normal range.
3.2.2. Positive parenting
Hierarchical regressions conducted for each positive
parenting domain (Table 3) indicated a significant
interaction effect at post-treatment for Affective Interac-
tions (R2D = .05, p b .05) and a trend for Limit Setting
(R2D = .05, p b .10) and for Limit Setting (R2D = .11,
p b .05) at followup.
Plotted mean scores for affective interactions in Fig. 3
show that, regardless of their level of interpersonal mal-
adjustment, RPMG mothers reported improvement in
affective interactions whereas DC mothers reported no im-
provement. Plotted mean scores for limit setting indicated
similar trends with mean scores for RPMG mothers with
high levels of interpersonal maladjustment at weeks 24 and
48 approaching the clinical norm of 50 and mean scores for
DC mothers with high levels of interpersonal maladjustment
showing little movement away from the clinical cut-off score
of 40 at weeks 24 and 48.
4. Discussion
In the original report of the randomized clinical trial
(Luthar & Suchman, 2000), RPMG demonstrated greater
efficacy than DC for improving parenting behaviors across
targeted parenting domains. Results from this reanalysis of
that data indicate that the relationally oriented parenting
intervention, RPMG, may be particularly beneficial to
mothers whose high levels of interpersonal maladjustment
might otherwise interfere with their ability to benefit from
drug counseling alone. More importantly, findings from this
study indicate that interpersonally maladjusted mothers who
only receive drug counseling and do not receive any
additional treatment for parenting deficits are likely to be
at risk for child maltreatment and parenting deficits.
To our knowledge, no prior studies have examined
predictors of response to any type (traditional or relational)
of parenting interventions for substance-abusing mothers.
Moreover, although behavioral parent training programs
have not yet demonstrated lasting improvement in the
affective quality of parent-child relationships involving
parents with substance abuse problems (see Catalano,
Gainey, Fleming, Haggerty, & Johnson, 1999; Kumpfer,
1998), no studies have yet compared traditional behavioral
models to relational parenting models in terms of their
efficacy for substance-abusing mothers. As Kumpfer,
Alvarado, and Whiteside (2003) have noted in their review
of family-based interventions for substance use and misuse
prevention, the shortage of efficacy studies involving
parenting interventions that specifically target affective
components of parent-child relationships has thus far
precluded their comparison with behavioral approaches.
Given the risk that interpersonal maladjustment confers for
parenting and child maltreatment, there is a pressing need
for further systematic research testing parenting interven-
tions designed to improve the affective quality of family
relationships for this very vulnerable population.
Although limitations of the original pilot study have
been described elsewhere (Luthar & Suchman, 2000), two
limitations are particularly relevant to this study. First,
the sample size (of children in particular) is small, and it is
limited to mothers enrolled in methadone maintenance. Thus,
caution is warranted in generalizing findings, especially to
other groups of drug using mothers. Second, although pre-
liminary analyses showed no differences in group attendance,

N.E. Suchman et al. / Journal of Substance Abuse Treatment 27 (2004) 135–143142
additional services received, or socially desirable responding
in the RPMG and DC conditions, we could not rule out the
possibility that attending an extra group each week (e.g., the
RPMG group) accounted for group differences in change. In
an ongoing Phase 2 randomized clinical trial comparing
response to an adjunct RPMG group with a response to an
extra relapse prevention group we will be able to address
this limitation.
With these cautions in mind, we feel these findings
nonetheless indicate the need for continued investigation of
predictors of successful parenting treatment outcomes
among substance-abusing parents. This may be an espe-
cially needy group since they have been viewed as
notoriously bdifficultQ to treat because of their interpersonal
difficulties. In particular, our findings indicate the need for
further research examining the efficacy of supportive,
relationally-oriented parenting interventions for parents
whose interpersonal deficits might otherwise interfere with
their capacities to benefit from more behaviorally-oriented
parent training.
Acknowledgments
Preparation of this manuscript was supported by
Research Scientist Development Awards K23-14606 (Such-
man) and K21-DA00202 (Luthar) and by NIDA Grants
P50-DA09241, R01-DA10726, and R01-DA11498. We
gratefully acknowledge Bruce Rounsaville for his insightful
comments on this manuscript. We also would like to thank
members of the Child and Family Research Group at the
Yale University School of Medicine and staff members at
the APT Foundation methadone clinics for their invaluable
assistance and support. A limited portion of this manuscript
was presented as an abstract at the College on Problems of
Drug Dependence Annual Meeting.
References
Aiken, L. S., & West, S. G. (1991). Multiple regression: testing and
interpreting interactions. Thousand Oaks, CA7 Sage.
Amaro, H., & Hardy-Fanta, C. (1995). Gender relations in addiction and
recovery. Journal of Psychoactive Drugs, 27, 325–337.
Barber, J. P., & Muenz, L. R. (1996). The role of avoidance and
obsessiveness in matching patients to cognitive and interpersonal
psychotherapy: Empirical findings from the Treatment for Depression
Collaborative Research Program. Journal of Consulting & Clinical
Psychology, 64, 951–958.
Blatt, S. J., Quinlan, D. M., Pilkonis, P. A., & Shea, M. T. (1995). Impact of
perfectionism and need for approval on the brief treatment of
depression: the National Institute of Mental Health Treatment of
Depression Collaborative Research Program Revisited. Journal of
Consulting & Clinical Psychology, 63, 125–132.
Byington, D. B. (1997). Applying relational theory to addiction treatment. In
S. L. A. Straussner & E. Zelvin (Eds.), Gender and addictions: Men
and women in treatment (pp. 31–46). Northvale, NJ7 Jason Aronson.
Catalano, R. F., Gainey, R. R., Fleming, C. B., Haggerty, K. P., & Johnson,
N. O. (1999). An experimental intervention with families of substance
abusers: One-year follow-up of the focus on families project.
Addiction, 94, 241–254.
Cohen, J. (1990). Things I have learned (so far). American Psychologist,
45, 1304–1312.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences.
Hillsdale, NJ7 Lawrence Erlbaum.
Cohen, J., & Cohen, P. (1983). Applied multiple regression/correlation
analysis for the behavioral sciences. Hillsdale, NJ7 Lawrence Erlbaum.
Dadds, M. R., Schwartz, S., & Sanders, M. R. (1987). Marital dis-
cord and treatment outcome in behavioral treatment of child
conduct disorders. Journal of Consulting and Clinical Psychology, 55,
396–403.
Dumas, J. E., & Wahler, R. G. (1983). Predictors of treatment outcome in
parent training: mother insularity and socioeconomic disadvantage.
Behavioral Assessment, 5, 301–313.
Finkelstein, N. (1996). Using the relational model as a context for trea-
ting pregnant and parenting chemically dependent women. In B. L.
Underhill & D. G. Finnegan (Eds.), Chemical dependency: Women at
risk (pp. 23–44). New York7 Haworth Press.
Gerard, A. B. (1994). Parent-Child Relationship Inventory (PCRI) Manual.
Los Angeles, CA7 Western Psychological Services.
Harden, B. J. (1998). Building bridges for children: addressing the
consequences of exposure to drugs and to the child welfare system.
In R. L. Hampton, V. Senatore, & T. P. Gullotta (Eds.), Substance
abuse, family violence, and child welfare: Bridging perspectives. Vol.
10. Issues in childrenTs and familiesT lives (pp. 18–61). Thousand
Oaks, CA7 Sage.
Heinze, M. C., & Grisso, T. (1996). Review of instruments assessing
parenting competencies used in child custody evaluations. Behavioral
Sciences & the Law, 14, 293–313.
Henderson, D. J., Boyd, C., & Mieczkowski, T. (1994). Gender, relation-
ships, and crack cocaine: a content analysis. Research in Nursing &
Health, 17, 265–272.
Hollingshead, A. B., & Redlich, F. C. (1958). Social class and mental
illness. New York7 Wiley.
Kazdin, A. E. (1997). Parent management training: evidence, outcomes,
and issues. Journal of the American Academy of Child & Adolescent
Psychiatry, 36, 1349–1356.
Klerman, G. L., Weissman, M. M., Rounsaville, B. J., & Chevron, E. S.
(1984). Interpersonal psychotherapy of depression (pp. 271–309). New
York7 Basic Books.
Kosten, T. R., Rounsaville, B. J., & Kleber, H. D. (1987). Predictors of
2.5-year outcome in opioid addicts: pretreatment source of income.
American Journal of Drug and Alcohol Abuse, 13, 19–32.
Kumpfer, K. L. (1998). Selective prevention interventions: The Strength-
ening Families Program. NIDA Research Monograph Series, 177,
160–207.
Kumpfer, K. L., Alvarado, R., & Whiteside, H. O. (2003). Family-based
interventions for substance use and misuse prevention. Substance Use
and Misuse, 38, 1759–1787.
Luthar, S. S., & Suchman, N. E. (1999). Developmentally informed
parenting interventions: the Relational Psychotherapy MothersT Group.In D. Cicchetti & S. L. Toth (Eds.), Rochester Symposium on De-
velopmental Psychopathology. Vol. 9. Developmental approaches to
prevention and intervention (pp. 271–309). Rochester, NY7 University
of Rochester Press.
Luthar, S. S., & Suchman, N. E. (2000). Relational Psychotherapy MothersTGroup: A developmentally informed intervention for at-risk mothers.
Development & Psychopathology, 12, 235–253.
Luthar, S. S., Suchman, N. E., Boltas, D. (1997). Relational Psychotherapy
MothersT Group: A therapistTs manual . Unpublished manuscript,
Columbia University.
Mayes, L. (1995). Substance abuse and parenting. In M. Bornstein
(Ed.), Handbook of parenting. Vol. 4. Applied and practical parenting
(pp. 101–125). Mahway, NJ7 Lawrence Erlbaum.
McLellan, A. T., Alterman, A. I., Woody, G. E., & Metzger, D.

N.E. Suchman et al. / Journal of Substance Abuse Treatment 27 (2004) 135–143 143
(1992). A quantitative measure of substance abuse treatment: The
Treatment Services Review. Journal of Nervous and Mental Disease,
180, 100–109.
Mercer, D., Carpenter, G., Daley, D., Patterson, C., & Volpicelli, J. (1994).
Group drug counseling manual. Unpublished manuscript, University of
Pittsburgh Medical Center.
Pedhazur, E. J., & Schmelkin, L. P. (1991). Measurement, design, and
analysis: An integrated approach. Hillsdale, NJ7 Lawrence Erlbaum.
Rohner, R. P. (1991). Handbook for the study of parental acceptance and
rejection. Unpublished manuscript, University of Connecticut.
Rounsaville, B. J., Kosten, T. R., Weissman, M. M., & Kleber, H. D.
(1986). Prognostic significance of psychopathology in treated opiate
addicts. Archives of General Psychiatry, 43, 739–745.
Smith, B., & Sechrest, L. (1991). Treatment of aptitude � treatment inter-
actions. Journal of Consulting & Clinical Psychology, 59, 233–244.
Sotsky, S. M., Glass, D. R., Shea, M. T., Pilkonis, P. A., Collins, J. F.,
Elkin, I., Watkins, J. T., Imber, S. D., Leber, W. R., Moyer, J., &
Oliveri, M. E. (1991). Patient predictors of response to psychotherapy
and pharmacotherapy: Findings in the NIMH Treatment of Depression
Collaborative Research Program. American Journal of Psychiatry, 148,
997–1008.
Webster-Stratton, C. (1985). Predictors of treatment outcome in parent train-
ing for conduct disordered children. Behavior Therapy, 16, 223–243.
Webster-Stratton, C. (1998). Parent training with low-income families:
Promoting parental engagement through a collaborative approach. In
J. R. Lutzker (Ed.), Handbook of child abuse research and treatment.
Issues in clinical child psychology (pp. 183–210). New York7 Plenum
Press.
Webster-Stratton, C., & Hammond, M. (1999). Marital conflict manage-
ment skills, parenting style, and early-onset conduct problems:
Processes and pathways. Journal of Child Psychology & Psychiatry
& Allied Disciplines, 40, 917–927.
Weissman, M. M., & Bothwell, S. (1976). The assessment of social
adjustment by patient self-report. Archives of General Psychiatry, 33,
1111–1115.
Zackon, F., McAuliffe, W., & ChTien, M. N. (1994). Recovery training and
self-help: Relapse prevention and aftercare for drug addicts. Wash-
ington, DC7 National Institute on Drug Abuse.