Embed Size (px)
Citation preview

This article was downloaded by: [86.29.223.245]On: 30 June 2014, At: 01:46Publisher: Taylor & FrancisInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Journal of Health Communication:International PerspectivesPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/uhcm20
Interventions for Individuals with LowHealth Literacy: A Systematic ReviewStacey L. Sheridan a , David J. Halpern b , Anthony J. Viera c , NancyD. Berkman d , Katrina E. Donahue c & Karen Crotty ea Department of Medicine , University of North Carolina at ChapelHill , Chapel Hill, North Carolina, USAb Department of Medicine , Duke University , Durham, NorthCarolina, USAc Department of Family Medicine , University of North Carolina atChapel Hill , Chapel Hill, North Carolina, USAd Program on Healthcare Quality and Outcomes, RTI International,Research Triangle Park , North Carolina, USAe Contractor , RTI International , Research Triangle Park, NorthCarolina, USAPublished online: 27 Sep 2011.
To cite this article: Stacey L. Sheridan , David J. Halpern , Anthony J. Viera , Nancy D. Berkman ,Katrina E. Donahue & Karen Crotty (2011) Interventions for Individuals with Low Health Literacy: ASystematic Review, Journal of Health Communication: International Perspectives, 16:sup3, 30-54, DOI:10.1080/10810730.2011.604391
To link to this article: http://dx.doi.org/10.1080/10810730.2011.604391
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the“Content”) contained in the publications on our platform. Taylor & Francis, our agents,and our licensors make no representations or warranties whatsoever as to the accuracy,completeness, or suitability for any purpose of the Content. Versions of published Taylor& Francis and Routledge Open articles and Taylor & Francis and Routledge Open Selectarticles posted to institutional or subject repositories or any other third-party website arewithout warranty from Taylor & Francis of any kind, either expressed or implied, including,but not limited to, warranties of merchantability, fitness for a particular purpose, or non-infringement. Any opinions and views expressed in this article are the opinions and viewsof the authors, and are not the views of or endorsed by Taylor & Francis. The accuracy ofthe Content should not be relied upon and should be independently verified with primarysources of information. Taylor & Francis shall not be liable for any losses, actions, claims,

proceedings, demands, costs, expenses, damages, and other liabilities whatsoever orhowsoever caused arising directly or indirectly in connection with, in relation to or arisingout of the use of the Content. This article may be used for research, teaching, and private study purposes. Terms &Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions It is essential that you check the license status of any given Open and OpenSelect article to confirm conditions of access and use.
Dow
nloa
ded
by [
86.2
9.22
3.24
5] a
t 01:
46 3
0 Ju
ne 2
014

Articles
Interventions for Individuals with Low HealthLiteracy: A Systematic Review
STACEY L. SHERIDAN
Department of Medicine, University of North Carolina at Chapel Hill,Chapel Hill, North Carolina, USA
DAVID J. HALPERN
Department of Medicine, Duke University, Durham,North Carolina, USA
ANTHONY J. VIERA
Department of Family Medicine, University of North Carolina at ChapelHill, Chapel Hill, North Carolina, USA
NANCY D. BERKMAN
Program on Healthcare Quality and Outcomes, RTI International,Research Triangle Park, North Carolina, USA
KATRINA E. DONAHUE
Department of Family Medicine, University of North Carolina at ChapelHill, Chapel Hill, North Carolina, USA
KAREN CROTTY
Contractor, RTI International, Research Triangle Park,North Carolina, USA
The U.S. Department of Health and Human Services recently called for action onhealth literacy. An important first step is defining the current state of the literatureabout interventions designed to mitigate the effects of low health literacy. We per-formed an updated systematic review examining the effects of interventions thatauthors reported were specifically designed to mitigate the effects of low health
The authors of this report are responsible for its content. Statements in the report shouldnot be construed as endorsement by the Agency for Healthcare Research and Quality or theU.S. Department of Health and Human Services.
Address correspondence to Stacey L. Sheridan, Department of Medicine, University ofNorth Carolina at Chapel Hill, 5039 Old Clinic Bldg, CB 7110, Chapel Hill, NC 27599,USA. E-mail: [email protected]
Journal of Health Communication, 16:30–54, 2011Copyright # Taylor & Francis Group, LLCISSN: 1081-0730 print=1087-0415 onlineDOI: 10.1080/10810730.2011.604391
30
Dow
nloa
ded
by [
86.2
9.22
3.24
5] a
t 01:
46 3
0 Ju
ne 2
014

literacy. We searched MEDLINE1, The Cumulative Index to Nursing and AlliedHealth Literature (CINAHL), PsycINFO, Educational Resources InformationCenter (ERIC), and the Cochrane Library databases (2003 forward for health lit-eracy; 1966 forward for numeracy). Two reviewers independently reviewed titles,abstracts, and full-text articles for inclusion and included studies that examined out-comes by health literacy level and met other pre-specified criteria. One reviewerabstracted article information into evidence tables; a second checked accuracy.Two reviewers independently rated study quality using predefined criteria. Among38 included studies, we found multiple discrete design features that improved com-prehension in one or a few studies (e.g., presenting essential information by itselfor first, presenting information so that the higher number is better, adding iconarrays to numerical information, adding video to verbal narratives). In a few studies,we also found consistent, direct, fair or good-quality evidence that intensiveself-management interventions reduced emergency department visits and hospitaliza-tions; and intensive self- and disease-management interventions reduced diseaseseverity. Evidence for the effects of interventions on other outcomes was eitherlimited or mixed. Multiple interventions show promise for mitigating the effects oflow health literacy and could be considered for use in clinical practice.
Health literacy is ‘‘the degree to which individuals can obtain, process, and under-stand the basic health information and services they need to make appropriate healthdecisions’’ (Institute of Medicine, 2004; Ratzan & Parker, 2000; U.S. Department ofHealth and Human Services, 2000) and function effectively in the health careenvironment. It represents a constellation of skills including the ability to interpretdocuments and read and write prose (print literacy), use quantitative information(numeracy), and speak and listen effectively (oral literacy) (Institute of Medicine,2004).
Low health literacy is a significant problem in the United States, affecting 36%of adults (Kutner, Greenberg, Jin, & Paulsen, 2006). Furthermore, low health liter-acy has been linked to poorer health outcomes (DeWalt, Berkman, Sheridan, Lohr,& Pignone, 2004).
Given the enormous burden of low health literacy and the potential to reducepoor outcomes with intervention, the U.S. Department of Health and HumanServices recently released a national action plan on health literacy (National ActionPlan to Improve Health Literacy, 2010). This action plan calls for increased research,development, implementation, and evaluation of interventions to improve health lit-eracy. An important step in this process is defining the current state of the literature.
In this paper, we report the results of a systematic evidence review that evaluatesthe effectiveness of interventions designed to mitigate the effects of low health liter-acy through either single or multiple literacy-directed strategies. This reviewwas commissioned by the Agency for Healthcare Research and Quality (AHRQ)as part of a larger report to determine the effects of health literacy and healthliteracy-directed interventions on health-relevant outcomes. It updates a review thatwe conducted in 2004 (Berkman et al., 2004).
Methods
We developed and followed a standard protocol for this systematic review, seekingguidance from a technical expert panel with expertise in health literacy. A technicalreport providing a detailed description of our methods and full results is available at:http://www.ahrq.gov/clinic/tp/lituptp.htm
Interventions for Low Health Literacy 31
Dow
nloa
ded
by [
86.2
9.22
3.24
5] a
t 01:
46 3
0 Ju
ne 2
014

Key Questions
The key questions we answer in this paper are: for those with low health literacy,what are effective interventions to
. improve use of health care services,
. improve health outcomes,
. affect the costs of care, and
. reduce disparities in health care service use and=or health outcomes amongdifferent racial, ethnic, cultural, or age groups?
Data Sources and Selection
We searched MEDLINE1, the Cumulative Index to Nursing and Allied HealthLiterature (CINAHL), the Cochrane Library, PsycINFO, and the EducationalResources Information Center (ERIC) to identify articles on interventions thatauthors reported were specifically designed to mitigate the effects of low healthliteracy and=or numeracy. For health literacy, we searched from 2003 to May 25,2010 (thereby updating our prior review). For numeracy, we searched from 1966to May 25, 2010 (because numeracy was not originally addressed). For this paper,we updated our searches from May 2010 through February 22, 2011 in order tobe current with the most recent literature. Because no medical subject headings(MeSH) specifically identify health literacy-related articles, we conducted key wordsearches (using the terms health literacy, numeracy, literacy, and terms or phrasesrelated to instruments known to measure these). We also manually searchedreference lists of review articles for additional studies.
We used standard Evidence-based Practice Center methods of dual review todetermine article inclusion (Berkman et al., 2011). Inclusion criteria are shown inTable 1.
Data Extraction and Quality Assessment
After determining article inclusion, one reviewer entered data about studies intoevidence tables and a second checked information for accuracy.
Two reviewers independently rated the quality of studies (good, fair, or poor)using standard predefined criteria (Berkman et al., 2011) that assessed selection bias,measurement bias, confounding, and inadequate power. Reviewers resolved alldisagreements by consensus and excluded poor-quality studies from analysis.
Data Synthesis and Analysis
We synthesized data qualitatively, dividing studies into those that used one specificliteracy-directed strategy and those that used multiple strategies. We did not have asufficient number of studies with similar outcomes or interventions to considermeta-analysis. To aid interpretation of findings, we emailed study authors to obtainadditional details about studied interventions.
Role of the Funding Source
AHRQ commissioned this review, but did not participate in the systematic review orpreparation of the manuscript.
32 S. L. Sheridan et al.
Dow
nloa
ded
by [
86.2
9.22
3.24
5] a
t 01:
46 3
0 Ju
ne 2
014

Results
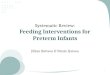
Our search results are shown in Figure 1. After excluding studies that did not meetour inclusion criteria, including those that were relevant but of poor quality(Bickmore, Pfeifer, & Paasche-Orlow, 2009; Carbone, Lennon, Torres, & Rosal,
Table 1. Inclusion criteria for review
Inclusion category Inclusion criteria
Study population All races, ethnicities, and cultural groups.All ages.Primary language is the same as that of the interventionmaterial.
Health literacy, numeracy, or oral health literacy levels ofindividuals are quantitatively measured and reported.
Health Outcomes Includes a health-related outcome of interesta:. Use of health care services
� Preventive services use� Receipt of recommended treatment� Office visits� Emergency department visits� Hospitalizations
. Health outcomes� Knowledge=comprehension� Accuracy of risk perception� Self-efficacy� Health-related skills (i.e., seeking info, taking meds,
self-monitoring, accessing care)� Intent for behavior� Behavior� Adherence to meds=behavior� Disease severity (i.e., biomarkers, symptoms)� Quality of life� Death
. Costs
. Disparities by age, race, ethnicity, or cultureIntervention Interventions that authors report are designed specifically to
mitigate the effects of low health literacy.Uses single or multiple literacy-directed strategies.
Study Design Experimental study design.Analyses Stratify results by health literacy levels of participants.b
Publication Status English only. Articles in print in peer reviewed journal.
aWe defined outcomes of interest using a logic model based on several models of health lit-eracy and an integrated model of behavioral theory (Fishbein, 2000; Paasche-Orlow & Wolf,2007).
bIn contrast to our full AHRQ report, the analysis for this paper also excludes articles thatdo not stratify results by health literacy (because these studies provide only indirect evidence ofthe intervention effect for those with low literacy).
Interventions for Low Health Literacy 33
Dow
nloa
ded
by [
86.2
9.22
3.24
5] a
t 01:
46 3
0 Ju
ne 2
014

2006; Cordasco et al., 2009; DeWalt, Pignone, et al., 2004; Garcia-Retamano &Galesic, 2010; Gazmararian et al., 2010; Kalichman, Cherry, & Cain, 2005; Kandulaet al., 2009; Ntiri & Stewart, 2009; van Servellen et al., 2003, 2005), we included 42
Figure 1. Study flow diagram. Abbreviations: cRCT, cluster randomized controlled trial;RCT, randomized controlled trial.
34 S. L. Sheridan et al.
Dow
nloa
ded
by [
86.2
9.22
3.24
5] a
t 01:
46 3
0 Ju
ne 2
014

studies in our AHRQ review. In this article, we focus on the 26 studies from ourAHRQ review that report results stratified by literacy level and thereby providethe most direct evidence for our key questions (Bryant et al., 2009; Campbell,Goldman, Boccia, & Skinner, 2004; DeWalt et al., 2006; Ferreira et al., 2005;Galesic, Garcia-Retamero, & Gigerenzer, 2009; Galesic, Gigerenzer, & Straubinger,2009; Garcia-Retamero & Galesic, 2009; Gerber et al., 2005; Greene & Peters, 2009;Greene, Peters, Mertz, & Hibbard, 2008; Jay et al., 2009; Kim, Love, Quistberg, &Shea, 2004; Kripalani, Bengtzen, Henderson, & Jacobson, 2008; Paasche-Orlowet al., 2005; Peters, Dieckmann, Dixon, Hibbard, & Mertz, 2007; Robinson, Calmes,& Bazargan, 2008; R. Rothman et al., 2004; R. L. Rothman et al., 2004; Rothmanet al., 2006; Sobel et al., 2009; Sudore et al., 2006; Volandes et al., 2009; Wallaceet al., 2009; Wright, Whitwell, Takeichi, Hankins, & Marteau, 2009; Yates & Pena,2006). We additionally synthesized these results with the results of 7 studies from our2004 AHRQ review (Davis et al., 1996; Davis et al., 1998; Davis, Holcombe, Berkel,Pramanik, & Divers, 1998; Meade, McKinney, & Barnas, 1994; Michielutte,Bahnson, Dignan, & Schroeder, 1992; Murphy, Chesson, Walker, Arnold, &Chesson, 2000; Wydra, 2001) and 5 studies from our February 2011 update thatare stratified by literacy level (Leroy & Miller, 2010; Ross, Ashford, Bleechington,Dark, & Erwin, 2010; Tait, Voepel-Lewis, Zigmund-Fisher, & Fagerlin, 2010;Wilson et al., 2010; Wolf et al., 2011).
Study Characteristics
Of 38 included studies, 22 were randomized controlled trials (RCTs), 1 acluster-randomized trial (cRCT), 5 non-randomized controlled trials (NRCTs) and10 quasi-experimental studies. All were of fair or good quality. Fourteen reportedon the effects of one specific strategy to mitigate the effects of low health literacy(see Table 2); 24 used a mixture of strategies combined into one intervention (seeTable 3). Thirty studies stratified results by health literacy and eight by numeracy.
Effects of Single-Strategy Interventions on Health Care Service Use
No included studies examined the effects of single-strategy interventions on healthcare service use.
Effects of Single-Strategy Interventions on Health Outcomes
Fourteen studies focused on testing discrete design features that might improveoutcomes for individuals with low health literacy. These studies focused exclusivelyon the outcomes of comprehension, health-related skills, and behavioral intent.
Knowledge=ComprehensionTwo RCTs addressed the effects of alternative document design on comprehension(Greene et al., 2008; Peters, Dieckmann, Dixon, Hibbard, & Mertz, 2007). Oneexamined the effects of highlighting the common features of comparative infor-mation (Greene et al., 2008). In this study, presenting 13 features of health plans sideby side with common features first (rather than in random order) provided no bene-fit in comprehension in low- or high-literacy subgroups in unadjusted analyses.However, highlighting the two or four advantages and disadvantages of plans
Interventions for Low Health Literacy 35
Dow
nloa
ded
by [
86.2
9.22
3.24
5] a
t 01:
46 3
0 Ju
ne 2
014

Table
2.Summary
ofstudiesusingsingle
strategyto
mitigate
theeffectsoflow
healthliteracy
Source
Design
(Sample
size)
Population
Healthliteracy
levels
Control
Intervention
Outcomes
Bryantet
al.,
2009
RCT
(232)
Patients
inurology
specialty
clinic
inUS
28%<highschool
onREALM
Standard
American
Urological
Association
BPH
Symptom
Score
(AUA-SS)
Multim
edia
AUA-SS
Comprehensiona
Galesic,
Gigerenzer,
etal.,2009
RCT
(162)
University
students
and
older
adultsin
Germany
Meanscore
9.7
on
12-ptnumeracy
scale
derived
from
Lipkus&
Schwartz
Conditional
probabilities
(%)
dem
onstrating
PPV
ofgenetic
testing
Naturalfrequencies
(x=10,000)
dem
onstratingPPV
ofgenetic
testing
Accuracy
ofrisk
perception
Galesic,
Garcia-
Retamero,
etal.,2009
Factorial
RCT
(171)
University
students
and
older
adultsin
Germany
Meanscore
9.5
on
12-ptnumeracy
scale
derived
from
Lipkus&
Schwartz
NumericalRisk
(presented
alternately
as
ARR
orRRR)
Iconarrays
Accuracy
ofrisk
perception
Garcia-R
etamero
andGalesic,
2009
RCT
(1047)
Population
sample
ofUS
andGerman
adults
49%
Low
numeracy
(>medianscore
on9-item
scale
adaptedfrom
Lipkusand
Schwartz)
b
Numerical
inform
ation
aboutRRR
(including
inform
ation
withvarying
size
denominators)
Numericalinform
ation
(RRR)plusicon
array(including
inform
ation
presentedwith
varying
sizesof
denominators)
Accuracy
ofrisk
perceptiona
36
Dow
nloa
ded
by [
86.2
9.22
3.24
5] a
t 01:
46 3
0 Ju
ne 2
014

Greeneet
al.,
2008
RCT
(303)
Community
dwellingadults
inUS
50%
Low
(score
less
than10on
DR
Numeracy
Test)
(1)Side-by-side
(random)
comparisonof
characteristics
(2)No
framew
ork
(1)Common=unique
presentationof
characteristics
(2a)Short
framew
ork
(2b)Longframew
ork
Comprehen
sion
Meadeet
al.,
1994
RCT
(192)
Patients
ina
primary
care
clinic
inUS
Medianscore:7th
gradeon
WRAT
Nointervention
(1)Brochure
oncolon
cancerscreening
(5–6th
gradereading
level)
(2)Videotapeoncolon
cancerscreening
(5–6th
gradereading
level)
Knowledge
Murphyet
al.,
2000
NRCT
(192)
Patients
ata
sleepclinic
inUS
40%<9th
grade
onREALM
Brochure
onsleep
apnea.(12th
gradereading
level)
Video
onsleepapnea.
(12th
gradereading
level)
Comprehen
sion
Peterset
al.,
2007
(Study1)
RCT
(303)
Community
dwellingadults
inUS
50%
Low
(score
less
than10on
DR
Numeracy
Test)
Nonordered
,nonquality
info.
(1)Ordered
cost,
quality,non-quality
info.
(2)Cost
andquality
info.only
Comprehen
sion,
Skill
Peterset
al.,
2007
(Study2)
RCT
(303)
Community
dwellingadults
inUS
50%
Low
(score
less
than10on
DR
Numeracy
Test)
Numbersonly
(1)Essentialinfo
accompaniedby
black=whitesymbols
(2)Essentialinfo
accompaniedby
traffic
symbols
Comprehen
sion,
Skill (C
ontinued
)
37
Dow
nloa
ded
by [
86.2
9.22
3.24
5] a
t 01:
46 3
0 Ju
ne 2
014

Table
2.Continued
Source
Design
(Sample
size)
Population
Healthliteracy
levels
Control
Intervention
Outcomes
(3)Essentialand
non-essen
tialinfo
accompaniedby
black=whitesymbols
(4)Essentialand
non-essen
tialinfo
accompaniedby
traffic
symbols
Peterset
al.,2007
(Study3)
RCT
(303)
Community
dwellingadults
inUS
50%
Low
(score
less
than10on
DR
Numeracy
Test)
Lower
number
isbetterquality,
nosymbols
(1)Higher
number
isbetterquality,no
symbols
(2)Lower
number
isbetterquality,
symbols
(3)Higher
number
isbetterquality,
symbols
Comprehension,
Skill
Taitet
al.,2010
RCT
(408)
Patients
ina
surgical
waitingareain
US
HL
notreported,
although51%
low
numeracy
onsubjective
numeracy
scale
Textpresentation
comparing
benefitsand
risksoftw
ohypothetical
drugs
1)Tabularand2)
pictograph
presentations
comparingbenefits
andrisksoftw
ohypotheticaldrugs
Comprehension
38
Dow
nloa
ded
by [
86.2
9.22
3.24
5] a
t 01:
46 3
0 Ju
ne 2
014

Volandes
etal.,
2009
RCT
(200)
Patients
in4
primary
care
clinicsin
US
18%�6th
grade
and12%
7th-8th
grade
onREALM
Verbalnarrative
aboutadvanced
dem
entia
Verbal
narrativeþvideo
showingfeaturesof
advanceddem
entia
Knowledgea,
Intent
Wilsonet
al.,
2010
RCT
(435)
Primary
care
clinicsin
2US
cities
15%�6th
grade
and28%
7th-8th
grade
onREALM
Novideo
orprint
material
Printwithprint
take-home
Video
alone
Video
withprint
take-home
Knowledge
Wrightet
al.,
2009
RCT
(140)
Internet
users
inUK
41%
Low
(incorrect
answ
erto
first
questionon
Lipkus
numeracy
scale)
Disperseddot
iconarray(3
differentrisk
magnitudes:
3%,6%,50%)
Grouped
doticon
array(3
differentrisk
magnitudes:3%,6%,
50%)
Comprehension
Abbreviations:
12-pt,12-point;ARR,absolute
risk
reduction;AUA-SS,AmericanUrologicalAssociation-Symptom
Score;BPH,benignprostatichyper-
plasia;info,inform
ation;NRCT,nonrandomized
controlled
trial;PPV,positivepredictivevalue;RCT,randomized
controlled
trial;REALM,Rapid
Estim
ate
ofAdultLiteracy
inMedicine;
RRR,relativerisk
reduction;UK,United
Kingdom;US,United
States;WRAT,WideRangeAchievem
entTest.
aAdjusted
forrelevantconfounders.
bWeightedpercents.
39
Dow
nloa
ded
by [
86.2
9.22
3.24
5] a
t 01:
46 3
0 Ju
ne 2
014

Table
3.Summary
ofincluded
interventionstudiesusingmixed
interventionsforlow
healthliteracy
Source
Design
(Sample
size)
Population
Health
literacy
levels
Control
Intervention
Outcomes
Campbell
etal.,2004
RCT
(233)
Patients
in1University
MedicalComplexin
US
50%�8th
gradeon
Woodcock
Johnson
Standard
consentform
(1)Sim
plified
consentform
(2)Video
consent
(3)Computerizedcon-
sent
Comprehensiona
Davisand
Bocchini,
1996
NRCT
(522)
Parents
ofpediatric
patients
inUS
47%<9th
gradeon
REALM
CDC
pamphlet
onpolio
vaccination
Sim
plified
LSU
pamphletonpolio
vaccination
Comprehension
Davis,
Frederickson,
etal.,1998
NRCT
(610)
Parents
ofpediatric
patients
at3clinics
inUS
31%<9th
gradeon
REALM
Improved
CDC
pamphleton
polio
vaccination
Sim
plified
LSU
pamphletonpolio
vaccination
Comprehension
Davis,
Holcombe,
etal.,1998
NRCT
(183)
Patients
inoncology
clinicsandadultsin
low-incomehousing
complexes
inUS
25%<6th
gradeon
REALM
Standard
consent
form
Speciallydeveloped
consentform
Comprehension
DeW
altet
al.,
2006
RCT
(127)
Patients
ingeneral
medicineand
cardiologyclinics
inUS
41%
inadeq.
on
S-TOFHLA
Usualcareþlow
literacy
pamphleton
CHF
CHF
self-m
anagem
ent
program
Knowledgea
Self-efficacy
Behavior
Quality
oflife
Use
ofhealth
care
services
40
Dow
nloa
ded
by [
86.2
9.22
3.24
5] a
t 01:
46 3
0 Ju
ne 2
014

Ferreiraet
al.,
2005
cRCT
(113
MDs,
1,978pts)
Patients
at2general
medicineclinicsin
US
31%<9th
gradeon
TOFHLA
b
UsualCare
Literacy
trainingfor
physiciansand
educationon
colorectalcancer
screeningfor
patients
Use
ofHealth
care
Services
Gerber
etal.,
2005
RCT
(144)
Patients
in5outpatient
clinicsin
US
56%<22
(inadeq.or
marginal)on
S-TOFHLA
Usualcareþ
computerized
quizzeson
diabetes-related
concepts
Diabetes
self-m
anagem
ent
intervention
Knowledgea
Self-efficacy
HgbA1c,
Use
ofhealthcare
Services
Greeneand
Peters,2009
RCT
(122)
Medicaid
recipients
in1UScounty
57%
with
TOFHLA
Cloze
score
�18(outof
20)
Standard
Medicaid
healthplan
comparison
chart
Sim
plified
Medicaid
healthplan
comparisonchart
Comprehension
Jayet
al.,2009
RCT
(56)
Adultsatacommunity
outreach
screeningin
US
17%�22
(inadeq.or
marginal)on
S-TOFHLA
Standard
FDA
materials
explaining
nutritionlabel
Nutritionlabel
inform
ationcard
andvideo
tutorial
Comprehensiona
Kim
etal.,2004
Quasi-,
pre-post
(92)
Participants
inadia-
betes
educationclass
at
auniversity
hospitalin
US
23%<22
(inadeq.or
marginal)on
S-TOFHLA
None
Diabetes
self-m
anagem
ent
intervention
Knowledgea
Behavior
HgbA1c
(Continued
)
41
Dow
nloa
ded
by [
86.2
9.22
3.24
5] a
t 01:
46 3
0 Ju
ne 2
014

Table
3.Continued
Source
Design
(Sample
size)
Population
Health
literacy
levels
Control
Intervention
Outcomes
Kripalaniet
al.,
2008
Quasi-,post
only
(408)
Patients
inprimary
care
clinic
inUS
21%<3rd
grade,
25%
4th–6th
grade,
and
31%
7th–8th
gradeon
REALM
None
(1)ModifiedPrint
inform
edConsent
withOralOverview
Knowledgea
Leroyand
Miller,
2010
Quasi-,
pre-post
(48)
Communitydwelling
adultsin
US
35%
with
REALM-
<9th
grade
None
Healthtopic
overview:
atable
ofcontents
linkingnounphrases
tomedicalwordsin
thetextvia
arrows
andhighlighting
Knowledge
Michielutte
etal.,1992
RCT
(217)
Patients
in1of4clinics
inUS(familypractice,
ob-gyn,family
planning,STI)
Below
median
score
of
46on
WRAT-R
None
(1)Illustrated
brochure
oncervical
cancerscreening
withnarrativetext
(2)Non-illustrated
brochure
withsim-
ple
bulleted
text
Comprehension
Paasche-Orlow
etal.,2005
Quasi-,
pre-post
(73)
Inpatients
at2academ
ichospitalsin
US
22%
inadeq.
on
S-TOFHLA
None
Asthma
Self-Managem
ent
Intervention
Knowledgea
Adherence
Disease
Symptoms
42
Dow
nloa
ded
by [
86.2
9.22
3.24
5] a
t 01:
46 3
0 Ju
ne 2
014

Robinson
etal.,2008
Quasi-,
pre-post
(110)
Patients
atpediatric
allergyclinic
inUS
Meanscore
3.2
onGilmore
Oral
Reading
Test
None
Asthma
Self-Managem
ent
Intervention
Self-efficacy
a
Use
ofHealth
care
services
Ross
etal.,2010
Quasi-,
pre-post
(49)
Adultsattending
churches
or
communitycenters
in2UScounties
22%
inadeq.
and16%
marginal
literacy
on
TOFHLA
None
Inform
edDecision
MakingVideo
on
PSA
Screening
Knowledge
Rothman,
Malone,
etal.,
2004
Quasi-,
pre-post
(159)
Patients
at1general
medicineclinic
inUS
55%�6th
gradeon
REALM
None
Diabetes
Self-Managem
ent
Intervention
HgbA1c(and
other
biomarkers)
Rothman,
Dew
alt,et
al.,
2004
Rothman,So,
etal.,2006
RCT
(217)
Patients
at1general
medicineclinic
inUS
38%�6th
gradeon
REALM
1-houreducation
session
Diabetes
Self
Managem
ent
Intervention
HgbA1c
(andother
biomarkers)a
Cost
Sobelet
al.,2009
Quasi,
pre-post
(130)
Patients
in1general
medicineclinic
and
adultsattendinga
faithbased
organizationoradult
basiceducationcenter
inUS
26%�6th
gradeand
33%
7th–8th
gradeon
REALM
None
Linearvideo
tutorial
aboutasthmaandits
managem
ent
Knowledgea
Sudore
etal.,
2006
Quasi-,
post-only
(204)
Patients
at1general
medicineclinic
inUS
22%
inadeq.
and18%
marginalon
TOFHLA
None
Sim
plified
consent
form
Comprehensiona
(Continued
)
43
Dow
nloa
ded
by [
86.2
9.22
3.24
5] a
t 01:
46 3
0 Ju
ne 2
014

Table
3.Continued
Source
Design
(Sample
size)
Population
Health
literacy
levels
Control
Intervention
Outcomes
Wallace
etal.,
2009
Quasi-,
pre-post
(250)
Patients
at3general
medicineclinicsin
US
29%
inadeq.
and14%
marginalon
TOFHLA
None
Diabetes
Self-Managem
ent
Intervention
Knowledge
Self-efficacy
Wolfet
al.,
2011
NRCT
(500)
Patientatprimary
care
clinicsin
2UScities
20%�6th
gradeon
REALM
32%
7th–8th
gradeon
REALM
Usual
prescription
medicinelabel
Patient-centeredlabel
(PCL)thatspecified
exact
timeformed
dosesþ=�
graphic
Comprehension
Wydra,2001
RCT
Patients
at4
comprehensivecancer
centers
inUS
63%�109on
WRAT
Usualcare
Interactivevideodisc
ondealingwith
cancertreatm
ent
fatigue(N
OS)
Behavior
Yatesand
Pena,2006
RCT
(200)
Patients
in1em
ergency
departmentin
New
Zealand
16%
REALM
<9th
gradec
Standard
head
traumaadvice
form
Sim
plified
head
traumaadviceform
Comprehensiona
Abbreviations:
CDC,Centers
forDisease
ControlandPrevention;CHF,congestiveheart
failure;cR
CT,cluster
randomized
controlled
trial;FDA,The
FederalDrugAdministration;HgbA1c,
glycosylatedhem
oglobin;inadeq.,inadequate;LSU,LouisianaState
University;MDs,
medicaldoctors;NOS,not
otherwisespecified;NRCT,non-randomized
controlled
trial;PCL,patient-centeredlabel;PSA,prostate-specific
antigen;ob-gyn,obstetrics-gynecology;pts,
patients;Quasi-,quasi-experim
entalstudy;RCT,randomized
controlled
trial;REALM,Rapid
Estim
ate
ofAdultLiteracy
inMedicine;
STI,
sexuallytrans-
mittedinfection;S-TOFHLA,short
form
TestofFunctionalHealthliteracy
inAdults;TOFHLA,TestofFunctionalHealthLiteracy
inAdults;US,United
States;WideRangeAchievem
entTest;WRAT-R
,WideRangeAchievem
entTest-Revised.
aAdjusted
forrelevantconfounders.
bLiteracy
level
measuredin
only
19%
ofpatients.
c Readfrom
table.
44
Dow
nloa
ded
by [
86.2
9.22
3.24
5] a
t 01:
46 3
0 Ju
ne 2
014

provided small improvements for those with high numeracy (unadjusted difference0.3–0.7 points on a 6-point scale). Unfortunately, it had no effect or actually wor-sened comprehension for those with low numeracy (unadjusted difference for presen-tations of four advantages and disadvantages:�0.5 points on a 6-point scale,p< .05). A second study examined the effects of presenting only essential infor-mation and=or putting essential information first (Peters et al., 2007). In this study,both low- and high-numeracy participants who received only essential informationabout hospital quality (e.g., death rates) had better comprehension of information(unadjusted difference, high numeracy: þ0.3 on a 3-point scale, p< .01; low numer-acy: þ0.7, p< .01) than individuals who received both essential and nonessentialquality information (e.g., death ratesþ hospital satisfaction rates). Additionally,when all quality information was presented, putting the essential information firstimproved comprehension for low- (but not high-) numeracy individuals (unadjusteddifference: þ0.6 on a 3-point scale, p< .01), although there was a notable ceilingeffect in the high-numeracy group.
Three RCTs examined the effects of alternative numerical presentations on com-prehension (Galesic, Gigerenzer et al., 2009; Garcia-Retamero & Galesic, 2009;Peters et al., 2007). One found that presenting information on hospital quality sothat the higher number (rather than the lower number) indicated better quality(i.e., ‘‘nurses per patient’’ rather than ‘‘patients per nurses’’) improved the meannumber of correct responses to comprehension questions in low- but nothigh-numeracy subgroups (unadjusted difference, low numeracy: þ0.7 on a 4-pointscale, p< .01; high numeracy þ0.2, p> .05; Peters et al., 2007). A second study foundthat presenting disease risk and treatment benefit information using the same (versusdifferent) denominators resulted in appreciable improvements in comprehension(adjusted p¼ .001), with a greater effect among those with low (þ25 percentagepoints) versus high numeracy (þ16 percentage points, unadjusted p for numeracyeffect¼ .001) (Garcia-Retamero & Galesic, 2009). A third study found that usingnatural frequencies (rather than percentages) to present information about baselinedisease rates and genetic test characteristics improved the accuracy of participants’estimates of their probability of disease following genetic testing (unadjustedp¼ .001) with similar effects for both high- (þ24 percentage points) and low- (þ27percentage points) numeracy individuals (Galesic, Gigerenzer et al., 2009).
One study (Tait, Voepel-Lewis, Zikmund-Fisher, & Fagerlin, 2010) examinedthe effect of substituting pictorial information for prose. This RCT found that pre-senting comparative information on the harms and benefits of two drugs in tablesrather than text improved understanding, particularly for those with low literacy(þ2.36 on a 5-point scale, p< .05 for understanding essential meaning; þ2.78 on7-point scale, p< .05 for understanding exact meaning). Compared with text, iconarrays (i.e., pictographs representing the proportion of individuals affected by dis-ease) also improved understanding of the essential (but not exact) meaning for thosewith low literacy (þ1.23 on 5-point scale, p< .025).
Five studies (Galesic, Garcia-Retamero et al., 2009; Garcia-Retamero & Galesic,2009; Peters et al., 2007; Wright et al., 2009), including two in the same article, exam-ined the effects of additive or alternative pictorial information on comprehension.Two RCTs examined the effect of adding symbols to numerical information. One(Peters et al., 2007) found that adding plus and minus signs to depict the conceptsof ‘‘more=fewer patients per nurse’’ or ‘‘more=fewer nurses per patient’’ had noeffect on comprehension overall or in the low numeracy subgroups. It slightly
Interventions for Low Health Literacy 45
Dow
nloa
ded
by [
86.2
9.22
3.24
5] a
t 01:
46 3
0 Ju
ne 2
014

worsened comprehension, however, in the high-numeracy subgroup (unadjusted dif-ference: �0.3 on a 4-point scale, p< .05). A second study (Peters et al., 2007) foundthat adding black and white circles (i.e., all black, half-black half-white, all white) orcolored traffic light symbols (i.e., green, yellow, red circles) to hospital quality infor-mation to indicate relative quality had no effect on comprehension in either low- orhigh-numeracy individuals.
Two RCTs (Galesic, Garcia-Retamero et al., 2009; Garcia-Retamero & Galesic,2009) showed that adding icon arrays to numerical information improved under-standing for low-literacy individuals. However, one showed that the benefit (unad-justed difference þ23 percentage points, adjusted p¼ .002) was not as great asswitching from relative risk reduction (RRR) to absolute risk reduction (ARR)presentations (absolute difference: þ49 percentage points, p¼ .001). Additionally,the second showed that the added value of icon arrays varied by whether the diseaserisk and treatment benefit information to be interpreted used the same or differentdenominators (unadjusted absolute difference, same denominator: þ11%; differentdenominator: þ32%, p-values not reported). Interestingly, icon arrays worsenedcomprehension for high-literacy individuals if denominators were the same andalready easily interpretable (unadjusted absolute difference: �16 percentage points,p not reported).
One RCT (Wright et al., 2009) examined the effect of providing alternatepictorial information. It found that icon arrays with grouped (rather than dispersed)dots tended to lead to higher comprehension (adjusted OR 2.26; 95% CI 0.799 to6.57), although results weren’t statistically significant.
Four RCTs (Bryant et al., 2009; Campbell et al., 2004; Meade et al., 1994;Wilson et al., 2010) and one NRCT (Murphy et al., 2000) examined the effects ofsubstituting various media for print and found conflicting results.
Health-Related SkillThree RCTs (Peters et al., 2007) reported in the same paper showed that presentingonly essential quality information, presenting higher numbers as better quality, andadding minus symbols to ‘‘lower number is better’’ numerical presentations aided thechoice of higher quality hospitals in individuals with low numeracy (unadjustedabsolute difference ranging from 12–23 percentage points). However, adding coloredtraffic symbols to indicate relative quality tended to worsen choice of higher qualityhospitals (unadjusted absolute difference: �11 percentage points, p> .05) eventhough they improved choices for higher numeracy individuals (þ16 percentagepoints, p< .05).
Behavioral IntentOne RCT found that adding video to a verbal narrative on preference for comfortcare increased preferences for comfort care as an end-of-life strategy (adjusted oddsratio [OR] 3.9, 95% confidence interval [CI], 1.8–8.6) (Volandes et al., 2009).
Effect of Single-Strategy Interventions on Costs and Disparities
No included studies examined the effect of single-strategy interventions on costs ordisparities.
46 S. L. Sheridan et al.
Dow
nloa
ded
by [
86.2
9.22
3.24
5] a
t 01:
46 3
0 Ju
ne 2
014

Effects of Mixed-Strategy Interventions on Health Care Service Use
Use of ServicesOne cRCT showed that an intensive intervention providing clinicians with infor-mation on health literacy and patients with information on colorectal cancer screen-ing (Ferreira et al., 2005) increased completion of any colorectal cancer screening testover 18 months (absolute difference 8.9 percentage points, p¼ .003). The impactdiffered by health literacy level, with an absolute difference of 26 percentage pointsin the low-health-literacy subgroup (p¼ .002) and 3 percentage points in thehigh-health-literacy subgroup (p¼ .65) when adjusting only for the clustering ofpatients within providers. One additional RCT of a minimally intensive diabetesself-management intervention showed no effect on recommended medical servicesin literacy subgroups; however, authors did not describe this outcome in sufficientdetail to allow interpretation.
Emergency Department VisitsOne quasi-experimental study promoting asthma self-management by childrenreported an overall reduction in emergency department visits (unadjusted mean dif-ference �30 percentage points, p< .01), with a striking effect in children who showedimprovements in reading compared to those who didn’t (adjusted OR 0.34, 95% CI,0.22–0.52) (Robinson et al., 2008).
HospitalizationsOneRCT reported no overall reduction in hospitalizations with a congestive heart failure(CHF) self-management intervention, but a significant reduction in a subgroup of indi-viduals with low health literacy (adjusted incidence rate ratio 0.39, 95% CI, 0.16–0.91)(DeWalt et al., 2006). A quasi-experimental study of an asthma self-management inter-vention also reported fewer hospitalizations (adjusted mean difference: �15 percentagepoints, p< .001) (Robinson et al., 2008), although the effect did not differ by literacy level.
Effects of Mixed-Strategy Interventions on Health Outcomes
KnowledgeFour RCTs, 4 NRCTs, and 8 quasi-experimental studies provided conflicting evi-dence on whether mixed-strategy interventions that reduced readability, altereddocument design, or provided education or self-management changed knowledgeor comprehension. (Gerber et al., 2005; Kim et al., 2004; Leroy & Miller, 2010; Rosset al., 2010; Sobel et al., 2009; Wallace et al., 2009).
Self-EfficacyOne RCT and one quasi-experimental study provided mixed evidence regarding theeffects of minimally intensive diabetes self-management interventions on self-efficacy(Gerber et al., 2005; Wallace et al., 2009). The RCT found no effect in either low- orhigh-health-literacy subgroups.
Health-Related SkillOne RCT (Jay et al., 2009) found that label-reading skill was increased after anutrition label card and 8-minute video tutorial on label reading, compared with astandard nutrition label alone (adjusted absolute difference in proportion of
Interventions for Low Health Literacy 47
Dow
nloa
ded
by [
86.2
9.22
3.24
5] a
t 01:
46 3
0 Ju
ne 2
014

knowledge questions correct: þ12 percentage points, p< 0.05). The effect was great-er among those with adequate (þ23 percentage points) versus inadequate health lit-eracy (þ1 percentage point) in adjusted analysis, however, analysis of the inadequateliteracy subgroup was underpowered. One NRCT (Wolf et al., 2011) found that amedicine label that specified the exact dosing times (rather than how many timesper day the medicine should be taken) improved patients’ ability to correctly describemedicine use (adjusted relative risk [RR] for low-literacy participants: 1.39, 95% CI1.14 to 1.68). Adding a graphic actually worsened understanding in the overallsample.
Health BehaviorTwo studies examined the effect of interventions on self-care behavior. Onequasi-experimental study (Kim et al., 2004) found a significant overall effect of adiabetes self-management intervention on the number of self-care days in the lastweek (effect size and exact p-value not reported [NR]). However, the effect variedwithin health literacy subgroups. In adjusted analysis, individuals with inadequatehealth literacy had greater improvements in dietary behavior, foot care, and glucosemonitoring, while individuals with adequate health literacy had greater improve-ments in exercise. There was no difference among groups in medication adherence.A second RCT (Wydra, 2001) examined the effect of a videodisc on dealing withcancer fatigue and found an improvement in self-care behaviors (effect size NR,p< .0001) with similar effects, regardless of health literacy level.
AdherenceTwo quasi-experimental studies examined the effects of self-management interven-tions on adherence (Kim et al., 2004; Paasche-Orlow et al., 2005). Both reportedno difference in the effect of their interventions by health literacy level, but providedinsufficient information to determine overall or subgroup effect sizes.
Disease SeverityFour studies examined the effect of self- or disease-management interventions onbiomarkers of disease. One RCT of a minimally intensive (�54 minutes) computer-ized diabetes self-management program found no effect on hemoglobin (Hgb) A1c,blood pressure, or body mass index (BMI) in participants overall or in low-health-literacy subgroups in an adjusted analysis (Gerber et al., 2005). However, other,more intensive, interventions demonstrated significant effects. One quasi-experimental study of a diabetes self-management intervention with 10 hours ofinstruction found a statistically significant decrease in HgbA1c (unadjusted absolutedifference, post-pre: �1.3 percent, exact p-value NR) with no difference in effectamong health literacy subgroups in an adjusted analysis (Kim et al., 2004). Addition-ally, one RCT (R. L. Rothman et al., 2004) testing an intensive disease managementintervention (8 hours of instruction plus pharmacist adjustment of medication)showed a significant decrease in HgbA1c with intervention in the low-health-literacygroup (adjusted absolute difference �1.4 percent, 95% CI, �2.3 to �0.6) and a non-significant decrease in the high-health-literacy group (adjusted absolute difference �0.5 percent, 95% CI, �1.4 to 0.3) (R. L. Rothman et al., 2004). Systolic blood press-ure was also significantly lowered among all participants (adjusted absolute differ-ence �7.6 mmHg, 95% CI, �13 to �2.2 mmHg). A quasi-experimental study ofthe same intervention supported these results (R. Rothman et al., 2004).
48 S. L. Sheridan et al.
Dow
nloa
ded
by [
86.2
9.22
3.24
5] a
t 01:
46 3
0 Ju
ne 2
014

A final quasi-experimental study examined the effects of a minimally intensive(�30 minutes) asthma self-management intervention on asthma symptom control;however, results were underpowered for this analysis, limiting conclusions(Paasche-Orlow et al., 2005).
Quality of LifeOne RCT examined the effects of an intensive CHF self-management intervention(10–16 visits of unspecified length) on heart failure-related quality of life. This studyreported no effects of its intervention on participant scores on the Minnesota Livingwith Heart Failure scale (MLHF; range 0–105) overall (adjusted absolute difference:�2, 95% CI – 5 to 9) or by health literacy subgroup (adjusted absolute difference,inadequate: �1.6, 95% CI – 15 to 12; adequate: �4.2, 95% CI – 14 to 6) (DeWaltet al., 2006).
Effects of Mixed-Strategy Interventions on Costs
One RCT examined the labor and total costs of its successful diabetes diseasemanagement intervention (R. L. Rothman et al., 2004; Rothman et al., 2006). Thisstudy reported total costs of $36.97 per patient per month (range in sensitivity analy-sis $16.22 to $88.56 per patient per month) for an intervention that included an aver-age of 13 hours of education, skill building, and medication adjustment per patient.
Effects of Mixed-Strategy Interventions on Disparities
No included studies addressed the effects of mixed health literacy interventions onhealth disparities.
Discussion
In this systematic review of interventions designed to mitigate the effects of lowhealth literacy, we found several discrete design features that improved participantcomprehension in one or a few studies (e.g., presenting essential information by itselfor first, presenting information so that the higher number is better, presentingnumerical information in tables rather than text, adding icon arrays to numericalinformation, adding video to verbal narrative). Furthermore, we found a few studiesthat provided consistent, direct evidence that intensive mixed-strategy interventionsfocusing on self-management reduced emergency department visits and hospitaliza-tions, and that intensive mixed-strategy interventions focusing on self- and diseasemanagement reduced disease severity. Whenever possible, these latter interventionsshould be considered for use in clinical practice. Evidence for the effects of otherinterventions on other outcomes was either limited or mixed, precluding conclusions.
In this review, we also found significant advances in the field of health literacyresearch. Our 2004 review included few interventions of any type, few outcomesbeyond comprehension, and few studies that stratified their analyses by health liter-acy level (Pignone, DeWalt, Sheridan, Berkman, & Lohr, 2005). In this review, inter-ventions were more varied, the outcomes more diverse, and the subgroup analysesmore frequent. These advances afford greater insights into effective interventionsand support crosscutting observations that begin to illuminate the design featuresthat facilitate intervention success. For instance, common features of interventions
Interventions for Low Health Literacy 49
Dow
nloa
ded
by [
86.2
9.22
3.24
5] a
t 01:
46 3
0 Ju
ne 2
014

that changed distal outcomes (e.g., disease biomarkers and hospitalizations) includedtheir high intensity, theory basis, pilot testing, emphasis on skill building, and deliv-ery by a health professional, for example, a pharmacist or a diabetes educator,(DeWalt et al., 2006; Robinson et al., 2008; R. L. Rothman et al., 2004); several alsoemployed simplified text and teach-back methodologies that have been shown to beeffective in the psycholinguistic and educational literatures (Snow, 2002). A smallnumber of studies afford further advances: They have shown that not all interven-tions with intuitive appeal are necessarily successful; some appear to provide nobenefit to populations with low health literacy (Greene et al., 2008) and some appearto incite potential harm (Peters et al., 2007). They also underscore that interventionsmay have different effects on those with low and high health literacy (Greene et al.,2008; Peters et al., 2007), raising questions about whether universal health literacyprecautions will ultimately be the best approach toward improving the health ofthe population.
Despite research advances, there remains much to be done. First, researchshould continue to address the methodological issues that will ensure high-qualityinferences about what works in order to mitigate the effects of low health literacy.Most important, researchers need to give more attention to issues of confounding.Although all studies in this review stratified results by health literacy, few stratifiedrandomization within health literacy subgroups or adjusted for potential confound-ing within subgroups. Additionally, only one study presented baseline characteristicsstratified by literacy level in order to facilitate assessment of potential confounding(DeWalt et al., 2006). Researchers also need to give more attention to issues of sam-ple size. Some studies in this review included too few low-literacy participants to beable to determine intervention effects for this subgroup. Others had too few parti-cipants to be able to determine intervention effects for all studied outcomes. Givenchallenges with recruitment and funding, researchers need creative solutions in orderto ensure adequate samples for high-quality inference. One solution may be theformation of a literacy trial group that would define a set of relevant outcomesfor future study and would plan ahead for meta-analyses that aggregate results fromsmaller studies.
To continue to advance the field of health literacy research, work should alsoproceed on several fronts. First, research should focus on confirming the effective-ness of discrete design features or mixed-strategy interventions that, to date, haveshown success only in limited populations. Second, research should explore yetuntested interventions. Such interventions might include interventions to increasemotivation to process information (e.g., fotonovellas); interventions that workaround the problem of low health literacy (e.g., patient navigators); and interven-tions that change physician behavior, practice structure, or existing health policy.Third, research should continue to explore the features that make health literacyinterventions successful. Although a combination of intervention features has beenshown to ensure the success of interventions, paring away ineffective features couldsave delivery time and be more cost-effective. Finally, research should explore thebest ways to disseminate and implement effective health literacy interventions. Suchan effort might be aided by creating a central, accessible library of literacy-directedinterventions.
In considering such recommendations, readers should consider the limitations ofour review. First, although we performed rigorous reviews of the literature, it is poss-ible we missed relevant literature. Medline has no MeSH term for health literacy,
50 S. L. Sheridan et al.
Dow
nloa
ded
by [
86.2
9.22
3.24
5] a
t 01:
46 3
0 Ju
ne 2
014

necessitating alternate search strategies to identify relevant studies. Second, theremight be publication bias. Third, we included only those studies in which investiga-tors quantitatively measured the health literacy or numeracy of their populations.We may have missed some important interventions examined in studies that mea-sured health literacy only by self-report. Finally, we examined only a predefinedset of outcomes and might have missed outcomes or interventions important to someresearchers, clinicians, and policymakers. These outcomes can be examined in futurereviews.
Conclusions
Despite limitations, we feel our review offers insights to aid a national action plan tomitigate the effects of low health literacy. Specifically, our review outlines (a) effec-tive interventions that could be implemented by practitioners today, (b) future areasin need of research, and (c) conceptual and methodological issues that should beaddressed in future research. Giving attention to these observations will afford usincreasing potential to reduce the negative effects of low health literacy on healthoutcomes.
References
Berkman, N. D., DeWalt, D. A., Pignone, M. P., Sheridan, S. L., Lohr, K. N., Lux, L. et al.(2004). Summary, Evidence Report=Technology Assessment No. 87. Retrieved July 19,2008, from http://www.ahrq.gov/clinic/epcsums/litsum.pdf
Berkman, N. D., Sheridan, S. L., Donahue, K. E., Halpern, D. J., Viera, A., Crotty, K. et al.(2011).Health literacy interventions and outcomes: An update of the literacy and health out-comes systematic review of the literature (Evidence Report=Technology Assessment,Number 199. Prepared by RTI International-University of North CarolinaEvidence-based Practice Center under Contract No. 290–2007-10056-I. AHRQ Publi-cation Number 11-E006). Rockville, MD: Agency for Healthcare Research and Quality.
Bickmore, T. W., Pfeifer, L. M., & Paasche-Orlow, M. K. (2009). Using computer agents toexplain medical documents to patients with low health literacy. Patient Education andCounseling, 75(3), 315–320.
Bryant, M. D., Schoenberg, E. D., Johnson, T. V., Goodman, M., Owen-Smith, A., & Master,V. A. (2009). Multimedia version of a standard medical questionnaire improves patientunderstanding across all literacy levels. Journal of Urology, 182(3), 1120–1125.
Campbell, F. A., Goldman, B. D., Boccia, M. L., & Skinner, M. (2004). The effect of formatmodifications and reading comprehension on recall of informed consent information bylow-income parents: A comparison of print, video, and computer-based presentations.Patient Education and Counseling, 53(2), 205–216.
Carbone, E. T., Lennon, K. M., Torres, M. I., & Rosal, M. C. (2006). Testing the feasibility ofan interactive learning styles measure for U.S. Latino adults with type 2 diabetes and lowliteracy. International Quarterly of Community Health Education, 25(4), 315–335.
Cordasco, K. M., Asch, S. M., Bell, D. S., Guterman, J. J., Gross-Schulman, S., Ramer, L.et al. (2009). A low-literacy medication education tool for safety-net hospital patients.American Journal of Preventive Medicine, 37(6 Suppl 1), S209–216.
Davis, T. C., Bocchini Jr., J. A., Fredrickson, D., Arnold, C., Mayeaux, E. J., Murphy, P. W.,et al. (1996). Parent comprehension of polio vaccine information pamphlets. Pediatrics,97(6 Pt 1), 804–810.
Davis, T. C., Fredrickson, D. D., Arnold, C., Murphy, P. W., Herbst, M., & Bocchini, J. A.(1998). A polio immunization pamphlet with increased appeal and simplified language
Interventions for Low Health Literacy 51
Dow
nloa
ded
by [
86.2
9.22
3.24
5] a
t 01:
46 3
0 Ju
ne 2
014

does not improve comprehension to an acceptable level. Patient Education and Counsel-ing, 33(1), 25–37.
Davis, T. C., Holcombe, R. F., Berkel, H. J., Pramanik, S., & Divers, S. G. (1998). Informedconsent for clinical trials: A comparative study of standard versus simplified forms.Journal of the National Cancer Institute, 90(9), 668–674.
DeWalt, D. A., Berkman, N. D., Sheridan, S., Lohr, K. N., & Pignone, M. P. (2004). Literacyand health outcomes: A systematic review of the literature. Journal of General InternalMedicine, 19(12), 1228–1239.
DeWalt, D. A., Malone, R. M., Bryant, M. E., Kosnar, M. C., Corr, K. E., Rothman, R. L.,et al. (2006). A heart failure self-management program for patients of all literacy levels: Arandomized, controlled trial [ISRCTN11535170]. BioMed Central Health ServicesResearch, 6, 30.
DeWalt, D. A., Pignone, M., Malone, R., Rawls, C., Kosnar, M. C., George, G. et al. (2004).Development and pilot testing of a disease management program for low literacy patientswith heart failure. Patient Education and Counseling, 55(1), 78–86.
Ferreira, M. R., Dolan, N. C., Fitzgibbon, M. L., Davis, T. C., Gorby, N., Ladewski, L. et al.(2005). Health care provider-directed intervention to increase colorectal cancer screeningamong veterans: Results of a randomized controlled trial. Journal of Clinical Oncology,23(7), 1548–1554.
Fishbein, M. (2000). The role of theory in HIV prevention. AIDS Care, 12(3), 273–278.Galesic, M., Garcia-Retamero, R., & Gigerenzer, G. (2009). Using icon arrays to communi-
cate medical risks: Overcoming low numeracy. Health Psychology, 28(2), 210–216.Galesic, M., Gigerenzer, G., & Straubinger, N. (2009). Natural frequencies help older adults
and people with low numeracy to evaluate medical screening tests. Medical DecisionMaking, 29(3), 368–371.
Garcia-Retamero, R., & Galesic, M. (2009). Communicating treatment risk reduction topeople with low numeracy skills: A cross-cultural comparison. American Journal of PublicHealth, 99(12), 2196–2202.
Garcia-Retamero, R., & Galesic, M. (2010). Who profits from visual aids: Overcomingchallenges in peoples understanding of risks [corrected]. Social Science and Medicine,70(7), 1019–1025.
Gazmararian, J., Jacobson, K. L., Pan, Y., Schmotzer, B., & Kripalani, S. (2010). Effect of apharmacy-based health literacy intervention and patient characteristics on medicationrefill adherence in an urban health system. Annals of Pharmacotherapy, 44(1), 80–87.
Gerber, B. S., Brodsky, I. G., Lawless, K. A., Smolin, L. I., Arozullah, A. M., Smith, E. V.et al. (2005). Implementation and evaluation of a low-literacy diabetes education com-puter multimedia application. Diabetes Care, 28(7), 1574–1580.
Greene, J., & Peters, E. (2009). Medicaid consumers and informed decision making. HealthCare Financing Review, 30(3), 25–40.
Greene, J., Peters, E., Mertz, C. K., & Hibbard, J. H. (2008). Comprehension and choice of aconsumer-directed health plan: An experimental study. American Journal of ManagedCare, 14(6), 369–376.
Institute of Medicine. (2004). Health literacy: A prescription to end confusion–executive sum-mary. Retrieved November 26, 2008, from http://www.nap.edu/catalog/10883.html
Jay, M., Adams, J., Herring, S. J., Gillespie, C., Ark, T., Feldman, H. et al. (2009). A rando-mized trial of a brief multimedia intervention to improve comprehension of food labels.Preventive Medicine, 48(1), 25–31.
Kalichman, S. C., Cherry, J., & Cain, D. (2005). Nurse-delivered antiretroviral treatmentadherence intervention for people with low literacy skills and living with HIV=AIDS.Journal of the Association of Nurses in AIDS Care, 16(5), 3–15.
Kandula, N. R., Nsiah-Kumi, P. A., Makoul, G., Sager, J., Zei, C. P., Glass, S., et al. (2009).The relationship between health literacy and knowledge improvement after a multimediatype 2 diabetes education program. Patient Education and Counseling, 75(3), 321–327.
52 S. L. Sheridan et al.
Dow
nloa
ded
by [
86.2
9.22
3.24
5] a
t 01:
46 3
0 Ju
ne 2
014

Kim, S., Love, F., Quistberg, D. A., & Shea, J. A. (2004). Association of health literacywith self-management behavior in patients with diabetes. Diabetes Care, 27(12), 2980–2982.
Kripalani, S., Bengtzen, R., Henderson, L. E., & Jacobson, T. A. (2008). Clinical research inlow-literacy populations: Using teach-back to assess comprehension of informed consentand privacy information. IRB: Ethics and Human Research, 30(2), 13–19.
Kutner, M., Greenberg, E., Jin, Y., & Paulsen, C. (2006). The health literacy of America’sadults: results from the 2003 National Assessment of Adult Literacy (NCES 2006-483).Retrieved November 17, 2008, from http://eric.ed.gov/PDFS/ED493284.pdf
Leroy, G., & Miller, T. (2010). Perils of providing visual health information overviews forconsumers with low health literacy or high stress. Journal of the American MedicalInformatics Association, 17(2), 220–223.
Meade, C. D., McKinney, W. P., & Barnas, G. P. (1994). Educating patients with limitedliteracy skills: The effectiveness of printed and videotaped materials about colon cancer.American Journal of Public Health, 84(1), 119–121.
Michielutte, R., Bahnson, J., Dignan, M. B., & Schroeder, E. M. (1992). The use of illustra-tions and narrative text style to improve readability of a health education brochure.Journal of Cancer Education, 7(3), 251–260.
Murphy, P. W., Chesson, A. L., Walker, L., Arnold, C. L., & Chesson, L. M. (2000). Compar-ing the effectiveness of video and written material for improving knowledge amongsleep disorders clinic patients with limited literacy skills. Southern Medical Journal,93(3), 297–304.
National action plan to improve health literacy. (2010). From http://www.health.gov/communication/HLActionPlan/
Ntiri, D. W., & Stewart, M. (2009). Transformative learning intervention: Effect on functionalhealth literacy and diabetes knowledge in older African Americans. Gerontology &Geriatrics Education, 30(2), 100–113.
Paasche-Orlow, M. K., Riekert, K. A., Bilderback, A., Chanmugam, A., Hill, P., Rand, C. S.et al. (2005). Tailored education may reduce health literacy disparities in asthmaself-management. American Journal of Respiratory and Critical Care Medicine, 172(8),980–986.
Paasche-Orlow, M. K., & Wolf, M. S. (2007). The causal pathways linking health literacy tohealth outcomes. American Journal of Health Behavior, 31(Suppl 1), S19–26.
Peters, E., Dieckmann, N., Dixon, A., Hibbard, J. H., & Mertz, C. K. (2007). Less is more inpresenting quality information to consumers. Medical Care Research and Review, 64(2),169–190.
Pignone, M., DeWalt, D. A., Sheridan, S., Berkman, N., & Lohr, K. N. (2005). Interventionsto improve health outcomes for patients with low literacy. A systematic review. Journal ofGeneral Internal Medicine, 20(2), 185–192.
Ratzan, S. C., & Parker, R. M. (2000). National library of medicine current bibliographies inmedicine: Health literacy. In C. R. Selden, M. Zorn, S. C. Ratzan & R. M. Parker (Eds.),Bethesda, MD: National Institutes of Health, U.S. Department of Health and HumanServices.
Robinson, Jr. L. D., Calmes, D. P., & Bazargan, M. (2008). The impact of literacy enhance-ment on asthma-related outcomes among underserved children. Journal of the NationalMedical Association, 100(8), 892–896.
Ross, L., Ashford, A. D., Bleechington, S. J., Dark, T., & Erwin, D. O. (2010). Applicabilityof a video intervention to increase informed decision making for prostate-specific antigentesting. Journal of the National Medical Association, 102(3), 228–236.
Rothman, R., Malone, R., Bryant, B., Horlen, C., DeWalt, D., & Pignone, M. (2004). Therelationship between literacy and glycemic control in a diabetes disease-managementprogram. Diabetes Educator, 30(2), 263–273.
Rothman, R. L., DeWalt, D. A., Malone, R., Bryant, B., Shintani, A., Crigler, B., et al.(2004). Influence of patient literacy on the effectiveness of a primary care-based diabetes
Interventions for Low Health Literacy 53
Dow
nloa
ded
by [
86.2
9.22
3.24
5] a
t 01:
46 3
0 Ju
ne 2
014

disease management program. Journal of the American Medical Association, 292(14),1711–1716.
Rothman, R. L., So, S. A., Shin, J., Malone, R. M., Bryant, B., DeWalt, D. A., et al. (2006).Labor characteristics and program costs of a successful diabetes management program.American Journal of Managed Care, 12(5), 277–283.
Snow, C. E. (2002). Reading for understanding: Toward a research and development program inreading comprehension (prepared for the Office of Education Research and Improvement,U.S. Department of Education). RAND.
Sobel, R. M., Paasche-Orlow, M. K., Waite, K. R., Rittner, S. S., Wilson, E. A., & Wolf, M.S. (2009). Asthma 1-2-3: A low literacy multimedia tool to educate African Americanadults about asthma. Journal of Community Health, 34(4), 321–327.
Sudore, R. L., Landefeld, C. S., Williams, B. A., Barnes, D. E., Lindquist, K., & Schillinger,D. (2006). Use of a modified informed consent process among vulnerable patients: Adescriptive study. Journal of General Internal Medicine, 21(8), 867–873.
Tait, A. R., Voepel-Lewis, T., Zigmund-Fisher, B. J., & Fagerlin, A. (2010). Presentingresearch risks and benefits to parents: Does format matter? Anesthesia & Analgesia,111(3), 718–723.
U.S. Department of Health, & Human Services. (2000). 11: Health Communication, InHealthy People 2010: Objectives for Improving Health (2nd ed.). Retrieved July 19,2008, from http://www.healthypeople.gov/Document/pdf/uih/2010uih.pdf
van Servellen, G., Carpio, F., Lopez, M., Garcia-Teague, L., Herrera, G., Monterrosa, F.,et al. (2003). Program to enhance health literacy and treatment adherence in low-incomeHIV-infected Latino men and women. AIDS Patient Care and STDS, 17(11), 581–594.
van Servellen, G., Nyamathi, A., Carpio, F., Pearce, D., Garcia-Teague, L., Herrera, G., et al.(2005). Effects of a treatment adherence enhancement program on health literacy,patient-provider relationships, and adherence to HAART among low-incomeHIV-positive Spanish-speaking Latinos. AIDS Patient Care and STDS, 19(11), 745–759.
Volandes, A. E., Paasche-Orlow, M. K., Barry, M. J., Gillick, M. R., Minaker, K. L., Chang,Y., et al. (2009). Video decision support tool for advance care planning in dementia:Randomised controlled trial. British Medical Journal, 338, b2159.
Wallace, A. S., Seligman, H. K., Davis, T. C., Schillinger, D., Arnold, C. L., Bryant-Shilliday,B., et al. (2009). Literacy-appropriate educational materials and brief counseling improvediabetes self-management. Patient Education and Counseling, 75(3), 328–333.
Wilson, E. A. H., Park, D. C., Curtis, L. M., Cameron, K. A., Clayman, M. L., Makoul, G.,et al. (2010). Media and memory: The efficacy of video and print materials for promotingpatient education about asthma. Patient Education and Counseling, 80(3), 393–398.
Wolf, M. S., Davis, T. C., Curtis, L. M., Webb, J. A., Bailey, S. C., Shrank, W. H., et al. (2011).Effect of standardized, patient-centered label instructions to improve comprehension ofprescription drug use. Medical Care, 49(1), 96–100.
Wright, A. J., Whitwell, S. C., Takeichi, C., Hankins, M., & Marteau, T. M. (2009). Theimpact of numeracy on reactions to different graphic risk presentation formats: Anexperimental analogue study. British Journal of Health Psychology, 14(Pt 1), 107–125.
Wydra, E. W. (2001). The effectiveness of a self-care management interactive multimediamodule. Oncology Nursing Forum, 28(9), 1399–1407.
Yates, K., & Pena, A. (2006). Comprehension of discharge information for minor head injury:A randomised controlled trial in New Zealand. New Zealand Medical Journal, 119(1239),U2101.
54 S. L. Sheridan et al.
Dow
nloa
ded
by [
86.2
9.22
3.24
5] a
t 01:
46 3
0 Ju
ne 2
014