Embed Size (px)
Citation preview

INTRACELLULAR FLUID LOSS IN DIAR,RHEAL DISEASE
ALLAN M. BUTLEI~, M.D. , CtIARLES F . McKIIA~N, M.D., AND JAMES L. GAMBLE, M . D .
W I T H ASSISTANCE OF PAULINE ~V~ARSII
BOSTON, ~/[ASS.
INTRODUCTION
T HE process of the dehydration of infants in the course of diarrheal disease may be briefly described. u and diarrhea produce
a loss of gastrointestinal secretions and thereby cause a withdrawal from the blood plasma of the water and materials used in the construc- tion of these secretions. The blood plasma is, however, sustained over a considerable interval, both as regards volume and composition, at the expense of interstitial fluid and the extensive loss of interstitial fluid which is so conspicuously eVident in dehydrated patients is thus produced. Eventually the interstitial reservoir is depleted an4 then, with dangerous rapidity, the volume of the plasma falls and distor- tions of the electrolyte structure of the plasma develop. 1 It is thus apparent that an essential step in the repair of dehydration should consist in refilling the interstitial body fluid compartments. This is usually accomplished by the subcutaneous administration of physio- logic salt solution which provides the two quantitatively important electrolytes, sodium and chloride ion. With more finesse, a solution which c~pies in detail the composition of interstitial fluid may be used. 2
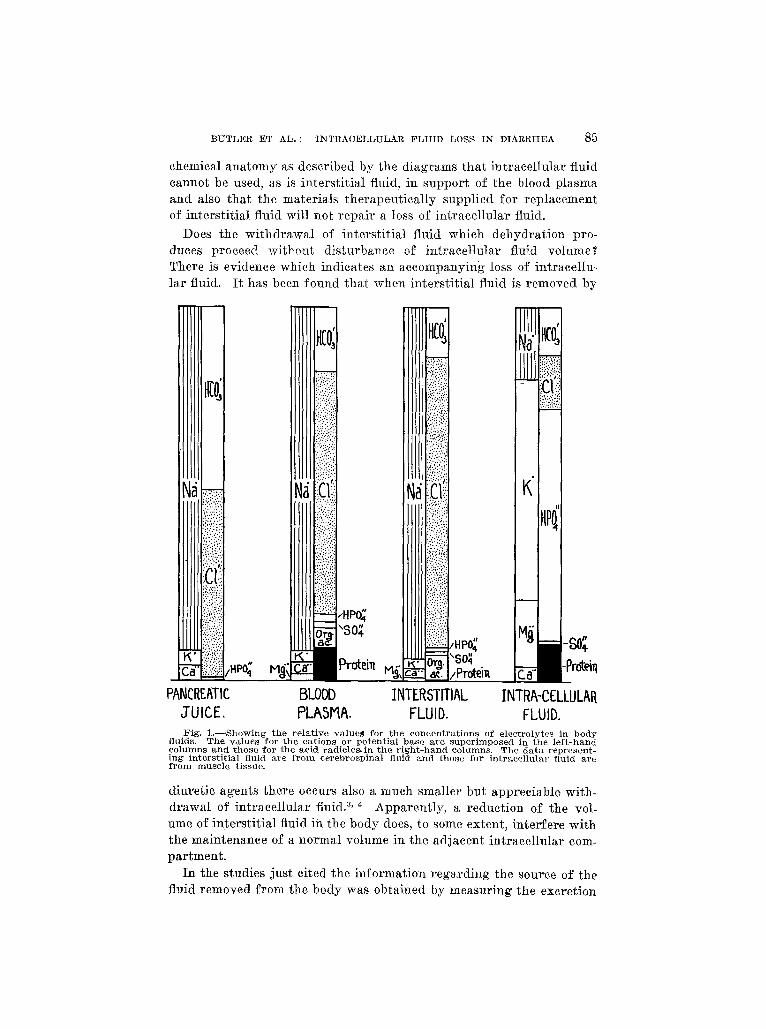
There remains for consideration the possibility that dehydration produces also a withdrawal of appreciable quantities of intracellular fluid. The implications of Such an event must be considered in terms of the electrolyte content of intraeclluiar fluid as compared with that of the extracellular fluids. As may be seen in the diagrams in Fig. 1, there are only slight differences in the relative values of the inorganic factors in the composition of b]ood plasma and of interstitial fluid. These differences are referable, in terms of the Donnan law, to the presence of the nonpermeating protein ions in the plasma. Intra- cellular fluid, however, presents an electrolyte pat tern which differs widely from that of the extracellular fluids. Here, instead of sodium, potassium is the chief factor in the total fixed base value and phos- phate almost replaces chloride. The mechanism which permits these large differences in the values for the. individual electrolytes in the two adjacent fluids has not been discovered. I t is evident from their
From the Department of Pediatrics, Harvard 3/iedieal School, and from the In- fants ' and Children's Hospitals.
84
B U T L E R ET AL. : INTRACELLULA_R F L U I D LOSS I N DIARRHEA 8 5
chemical ana t om y as described by the d iagrams tha t in t race l lu lar fluid cannot be used, as is in ters t i t ia l fluid, in s u p p o r t of the blood p lasma and also tha t the mater ia ls the rapeu t i ca l ly suppl ied fo r rep lacement of in ters t i t ia l fluid will not r epa i r a loss of in t race] lu lar fluid.
Does the wi thd rawa l of in ters t i t ia l fluid which dehydra t ion pro- duces proceed wi thout d is turbance of in t race l lu ta r fluid volume? There is evidence which indicates an aecompanyincg loss of intracel lu- la r fluid. I t has been found tha t when inters t i t ia l fluid is r emoved by
~ rol:eiTI
PANCREATIC BLOOD INTERSTITIAL INTRA-CELLULAR JUICE. PLASMA. FLUID. FLUID. Fig'. L - - S h o w i n g t he r e l a t i v e v a l u e r for t h e c o n c e n t r a t i o n s of e l ec t ro ly tes in body
fluids. T h e v a l u e s fo r t he ca t ions or po t en t i a l b a s e a r e s u p e r i m p o s e d in the l e f t - h a n d co lumns a n d those fo r the ac id radic les , in t h e r i g h t - h a n d columns. T h e d a t a r e p r e s e n t - ing" i n t e r s t i t i a l fluid a r e f r o m e e r e b r o s p i n a l fluid a n d those for i n t r a c e l l u l a r fluid a r e f r o m m u s c l e t issue.
diuret ic agents there occurs also a much smal ler but apprec iable with- d rawa l of in t race l lu la r fluid2, ~ Apparen t ly , a reduct ion of the vol- ume of in ters t i t ia l fluid in the body does, to some extent , in ter fere with the main tenance of a normal volume in the ad jacent in t raeelh i lar com- par tment .
In the studies just cited the in format ion r ega rd ing the source of the fluid removed f rom the body was obta ined by measur ing the excret ion

86 THE JOURNAL OF PEDIATRICS
of sodium and of po tass ium in the urine. I f the f a i r ly sa t i s fac tor i ly established proposi t ion tha t a loss of e lectrolyte f rom the body is ae- companied by a corresponding amount of' w a t e r be aceepted, measure- ments of a loss of sodium and of po tass ium can, as the da ta in Fig. 1 indicate, be used to calculate respect ive ly a w i thd rawa l of extraeel lu- lar and o,f intra.eellular water. This premise is used in an investigation of body fluid losses by infants in the a.dvaaeed and severe stage of diar- rheal disease, the res,ults of which are presented in this paper. The chief i tem of a t tempt was to learn whether or' not there is a considerable loss of. intraeel lular fluid in addition to. the large loss. of interst i t ial fluid.
PLAN OF STUDY
Two infants were studied over a period of twenty-four hours im-
mediately following their entrance to the hospital. Both were suffer-
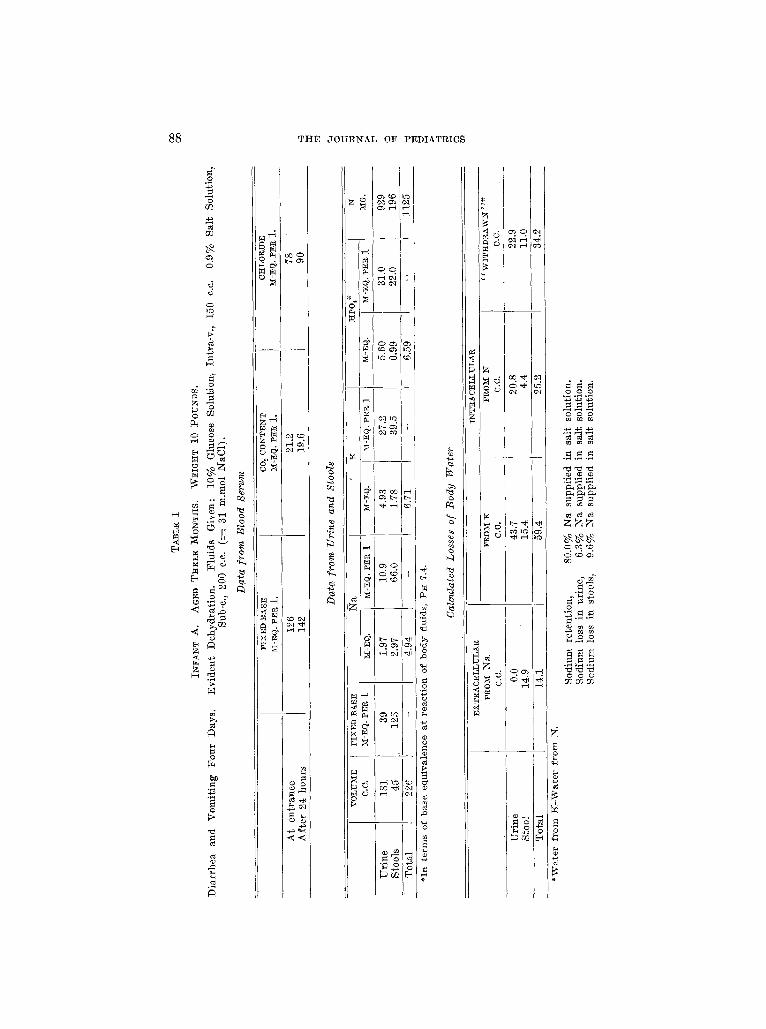
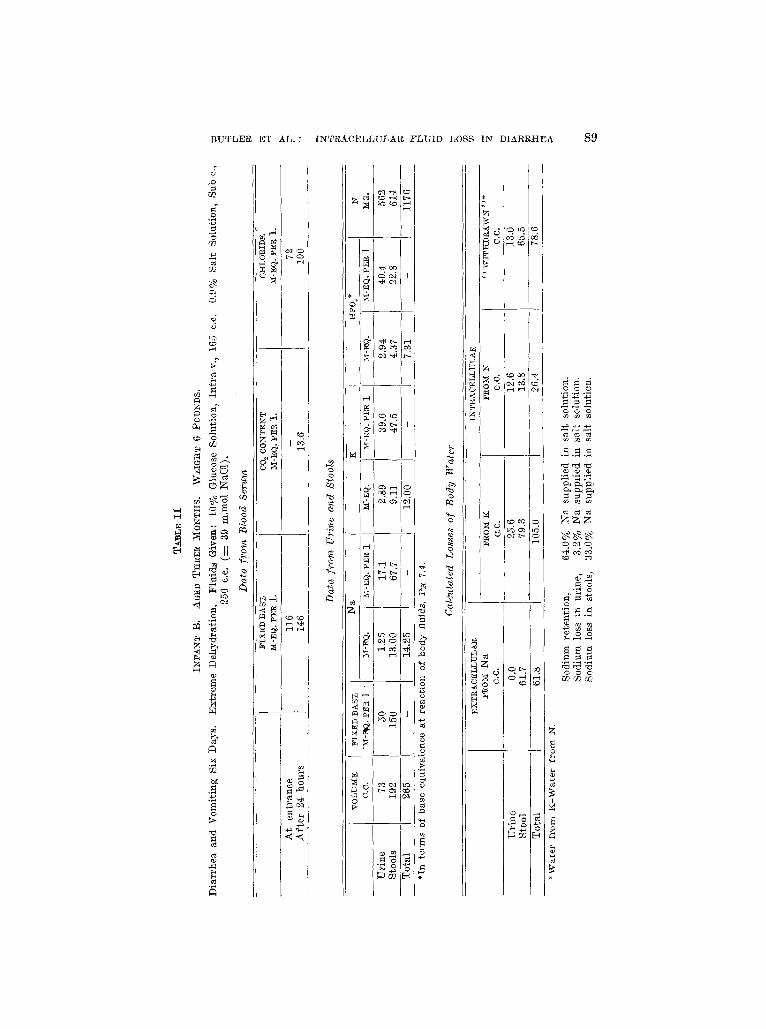
ing severely f rom diar rhea l disease wi th vomiting' and were exten- sively dehydra ted . So f a r as eould be determined, no food had been re ta ined fo r several days. They were given no food dur ing the twen ty- four hour per iod but did receive salt solution subcutaneous ly and glu- cose solution i n t r a v e n o u s l y . The substanees measm'ed in the urine and stools m a y the re fo re be t aken as deseribing losses f rom the body. Sodium and chloride f rom the adminis te red salt solution can p robab ly correct ly be included in this s ta tement since the quant i t ies supplied were doubtless less t han the deficits which dehydra t ion had produced. Wi th the hope of obtaining' a urine specimen before beginning' t reat - ment, the fluids were not adminis te red unt i l a f t e r the first eight hours. Catheter iza t ion then, however , fa i led to produce a specimen. The in- f an t s were thus evident ly anurie, and the urine, seer'eted dur ing the subsequent s ixteen hem's m a y be r ega rded as a response to the fluids given. The infants were comfor t ab ly immobil ized on the metabol i sm bed and a collection of ur ine and of stools over the twen ty - fou r hour per iod was obtained. I n order to insure a complete ur ine specimen, the infants were ca theter ized at the end of the period. One. of the infants (A) vomited a few e.e. of fluid. Wi th this except ion vomit ing, which had been f requent before enter ing the hospital , was absent dur- ing the per iod of study. Blood samples were t aken at the beginning and at the end of the twen ty - four -hour interval .
Measurements of to ta l fixed base, sodium, potassium, phosphorus and n i t rogen were obtained f rom both urine, and stools. The concen- t ra t ions of to ta l fixed base, chloride, and carbon dioxide content were de te rmined in the serum of the blood samples, collected and separa ted under o i l .
The following methods of analysis were used: total base by the method of FfskeS; sodium by nranyl zinc acetate precipitation as described by Butler and TuthilD; potassium by Fiske 's modified cobaltinitrite method in which potassium is reprecipitated as potassium acid tartrateT; phosphorus by the method of Fiske and

]~UTLER ~T AL. : ]NTRACELLULA-I~ FLUID LOSS IN DIARttt=IEA :~7
Subba rows ; ch lor ide by ~ i s k e and_ L i n ' s method of wet ash ing wi th n i t r i c acid
and po tas s ium p e r m a n g a n a t e and Vo lha rd t i t r a t i onP ; carbon d ioxide content of the
serum accord ing to Van Slyke and Sendroy~o; and n i t r o g e n by maero-I~je ldahl .
RESULTS AND DISCUSSION
If the loss of body fluid in diarrheal disease caused by failure of reabsorption of gastrointestinal secretions is limited to extraeellular fluids and if the quantity of intracellular fluid presenting for ex- cretion is determined only by the extent to which body protoplasm is destroyed as a result of the factor of fasting which the situation con- tains, the composition of the fixed base excretion in urine and stools can be postulated readily by reference to the diagrams in Fig'. I. In other words, nearly all of the fixed base in the stools should be sodium and, owing to the sodium deficit thus produced within the body, no sodium, should be permitted to enter the urine. The fixed base in the urine should consist chiefly of potassium, the amom~t of which should correspond to the extent of the destruction of body protoplasm as in- dicated by the nitrogen excretion.
The measurements actually obtained from the two iniants (Tables I and II) extensively disobey these expectations. In both instances the quantity of potassium in the stools is, in relation to sodium, very much larger than would be expected on the basis of the relatively small value for potassium in gastrointestinal secretions and in the extraeellular fluids (Fig. 1). The urines both contain appreciable quantities of sodium which, ho.wever, are small fractio~s of the amounts of sodium supplied by the administered salt solution. The expected considerable excretion of potassium is found. When, however, the loss of intraeellular fluid calculated from the urine potassium is com- pared with the loss of fluid as estimated from urine nitrogen, it is found to be much larger. These calculated values are given in the third section of the tables, e It thus seems that potassium and a cor- responding quantity of intracellular water are excreted in tile urine to a much greater extent than can be accounted for by the destmtetion of body protoplasm as measured by the nitrogen exeretion.~ The
*The formulas used in ca lcu la t ing the ex t ra - and in t race l lu la r fluid losses were those of Peters and Van Slyke~:
l~Ia - 0.425 I( - - l i t e r s of ex t race l lu la r wa te r lost.
148
K - 0.017 Na _ liters of intracellular water lost. 112
Jn which ]?qa and I~ represent milligram equivalents of base found. As regards the 0.0 value for extraeellular water in urine which was founcl for both infants, it rnay be noted that the factor 0.425 I4 in the first equation produced values for ]:qa from intracellular water os 2.10 m-eq. for infant A_ and 1.23 m-eq. for infant ~, which very closely cancel the found values for Na given in the table, 1.97 m-eq. and 1.25 m-eq. respectively.
The intraeellular fluid loss corresponding to destruction of protoplasm was calcu- lated f rom the fo rmula :
Nitrogen (gm.) x 29.5 x .76 = c,c. water. tAny nitrogen lost through' the skin could not account for the excess of excretion
of Dotassiurn over nitrogen in the urine and stools as available dat~ indicate that the ratio of nltrogen to, potassium in sweat is less than that obtaining in protoplasm.
88 T I ~ E J O U R N A L O F P E D I A T R I C ~
o ~
r
r-~
g ~
v~
z
o
h~
/1/ t r
,q~4
g ~ g
(x)
o o o
B U T L E R E T A L . : I N T ~ A C E L L U L A l l F L U I D L O S S I N D I A R R H E A 8 9
~'~d
r~
Z ~
N N
N C/2
f, il I x ' g ~
",~ t'~ r--t
o~o
o o
o o c~ Of 2 m
90 T~E JOURNAL OF PEDIATRICS
simplest explana t ion of this finding is that , in addi t ion to the release of wa t e r f r o m des t royed protoplasm, there occurs a w i thd rawa l of w a t e r f r o m tissue cells. The ex ten t of this w i thd rawa l of in t race l lu la r wa t e r is measured by sub t rac t ing the value for released water , calcu- la ted f rom the n i t rogen measm'ement , f rom the to ta l excre t ion of in t raeel lu]ar wa t e r calculated f rom the potass ium excretion. In the stools the value fo r " w i t h d r a w n " wa te r thus obtained const i tutes much the g rea te r pa r t of the excret ion of in t raee l lu la r water , and is a pp rox i m a t e l y as la rge a quant i ty as the ext racel lu]ar wa t e r loss cal- culated f r o m the sodium content of the stools. The to ta l value for " w i t h d r a w n " in t raee l lu la r w a t e r in the ur ine and stools t aken to- ge ther is, in both exper iments , ac tual ly l a rge r than the to ta l excre- t ion of ex t race l ]n lar water .
The measurements obta ined f rom the initial blood serum samples show extensve changes f rom thei r no rmal values fo r the three quan- t i t a t ive ly impor t an t s t ruc tu ra l fac tors and demons t ra te tha t the proc- ess of dehydra t ion has passed the point beyond which the p lasma cannot be accura te ly susta ined by w a t e r and mater ia ls f rom the inter- s t i t ial reservoir .
The: major ' f inding f rom this s tudy of two infants in an advanced s tage of dehydra t ion is the evidence just p resen ted demons t ra t ing that , in addi t ion to the loss of in ters t i t ia l fluid, which we are accus- tomed to r ega rd as the essential event, there is opera t ive also a proc- ess of w i thd rawa l of in t race l lu la r fluid p roduc ing a wa te r loss which is quan t i t a t ive ly even la rger than the loss of in ters t i t ia l water .
The da ta obta ined f rom these infants do not explain the process of w i thd rawa l of in t race l lu la r fluid. An especial ly puzzling f ea tu re is its r emova l to a large extent in the stools, which unde r the conditions of this s tudy, are assumed to be composed of gas t ro in tes t ina l secretions in which the concentra t ion of potass ium has a p p r o x i m a t e l y the same small value found in the blood plasma, 5.0 m-eq. per liter. I n the stools f rom these infants, the concentra t ion of po tass ium was fo r A, 39.5 m-eq. per l i ter and fo r B, 47.5 m-eq. pe r liter. The disabi l i ty of renal function, which is a consequence of severe dehydrat ion, p robab ly somewhat raises the level of po tass ium in the plasma. Direct infor- mat ion on this point is un f o r tuna t e ly lacking. I t has been found, however, t ha t in advanced renal disease the concentra t ion of potas- sium is r a r e l y more than double, the normal value. The subjects of this s tudy received glucose solution which p re sumab ly enabled the kidneys to opera te fa i r ly accura te ly as indicated by the secret ion of a sizable volume of r a t h e r dilute urine. I t is, therefore , a l toge the r im- probable tha t po tass ium accumula ted in the ex t raee l lu la r fluids to an extent sufficient to explain di rect ly the high values found ia the stools.
There is some t emp ta t i on to suggest a subst i tu t ion of po tass ium for sodium b y the secre tory mechanisms in suppor t ing the requi red osmo- lar value of the intes t inal fluids. Tha t the to ta l concent ra t ion of
B U T L E R ET AI~. : I N T R A C E L L U L A I ~ I~LUID LOSS I N D I A R R H E A 91
electrolytes was sustained at a p p r o x i m a t e l y the body fluid level is shown by the rough agreement of the to ta l fixed base concentra t ion in the. stools wi th the values for' fixed base found in tile p lasma. I t is, however, physiological ly unl ikely tha t unusual substances could be employed in the construct ion of secretions and, since these infants received sodium chloride solution, there is li t t le basis for' supposing a pt t rposeful or' compulsory subst i tu t ion of po tass ium and phospha te for the r'egular~y used mater ia ls , sodium and chloride.
Ano the r conjecture contains, to our minds, some degree, of prob- abili ty. This consists in premis ing a much. more rapid absorpt ion of sodium than of po tass ium f r o m the bowel wi th the resul t t ha t the potass ium content of the stools represents an accumula t ion der ived f rom the small quant i t ies present in no rma l ly cons t ruc ted secretions. In suppor t of this surmise an observat ion made b y one. of us may be cited. 12 I n the ease of a nor'real subjec t when the food contains sev- eral t imes as much sodium as potass ium and, moreover , encounters dur ing digest ion secretions which contain twenty-f ive t imes a,s much sodium as potassium, more potass ium t h a n sodium is found in the stools. Assuming no reabsorp t ion of potassium, the concentra t ions of potass ium found in the stools of these two infants wi th d iar rheal dis- ease describe an a p p r o x i m a t e l y tenfold concentra t ion of gastrointes- t inal fluids containing, when secreted, the normal value for' potassium, 5.0 m-eq. per liter. In teres t ingly it may also be. seen in the tables: tha t th.e concentra t ion of phospha te in the stools is closely ten t imes the value, found in normal blood plasma, 2.5 m-eq. per' liter'. Since un- der nor'real c i rcumstances there is ve ry li t t le reabsorp t ion of phos- pha te a l though potass ium is extens ively r e tu rned to the body fluids, this paral le l re la t ionship of the concentra t ions of potass ium and phos- pha t e in the stools of these infants to the normal blood p lasma values suggests tha t d iar rhea l disease in terferes more or less complete ly wi th the reabsorp t ion of potassium. In the case of the in fan t B, whose stool volume was ve ry large, 192 c.e., a to ta l secretion of near ly 2000 c.e. of intes t inal fluids would be requi red to aeeotmt fo r the ten- fold concentra t ion of potass ium found. This is a l a rge figure for' the secretions, but is not of an intpossible order of magni tude . The twen ty - four -hour volume of gas t ro in tes t ina l secretions fo r a normal adul t is 8-10 l i ters and the s~lrmise is permiss ible tha t the volume of the secretions m a y be much increased in d iar rheal disease. Also, a s l ight increase in the potass ium concent ra t ion in the p lasma above the normal value, which is a not improbab le e~ent in severe dehydra- tion, would g rea t ly reduee the ca lcula ted volume of secretions. F o r instance, if the p lasma potass ium in the in fan t B be. t aken as 7.5 m-eq. per l i ter ins tead of the no rma l va lue 5.0 m-eq. per' liter, the. voiume of secretions requi red to produce the concentra t ion of po tass ium found in the stools wo~tld be 1200 c.c. ins tead of 2000' e.e. This explanat ion of the la rge exeret ion of po tass ium in the stools, if it could be estab-

92 TI-tE J O U R N A L OF PEDIATRICS
lished, would describe a process of withdrawal of intracel lular fluid operative whenever abnormal circumstances produce a par t ia l inter- ference with the reabsorpt ion of gastrointest inal secretions.
The presence of an intracel lular fluid loss complicates our concep- t ion of the process of dehydrat ion and disturbs our confidence in the therapeut ic adequacy of parentera l t reatment. Since repair solutions must be placed in the vascular or in the interstit ial compartment , they cannot contain with safety the intracellular materials, such as potas- sium and phosphate, at concentrat ions above the small values pre- scribed for them in e xtracel lular fluids. The solution devised by Har tmann contains potassium appropr ia te ly to this extent. I t is evi- dent, however, tha t such solutions cannot provide an adequate re- plenishment of intracel[ular materials. Parentera l the rapy has a large, often dramatic, effectiveness: I t must be admitted, however , tha t it is not always successful and it may be hoped that recognit ion of an addi- tional pathologic process in the situation will eventual ly produce supplementary measures which will provide a more complete control of the severe stage of diarrheal disease.
SUM ~[ARY
Estimations of the extent and source of losses of body fluid by infants in an advanced stage of diarrheal disease were obtained from measurements of the excretion of sodium, potassium and ni t rogen in the urine and stools.
I t was found that intracel lular fluid is excreted in both urine and stools to an extent much greater than can be accounted for by re- lease of water due to destruction of protoplasm. The addit ional water is regarded as wi thdrawn from tissue cells. The total quant i ty of wi thdrawn intracel lular water was found to be larger than the loss of intersti t ial water.
According to the findings in this s tudy a loss of intraeellular fluid, in addition to a loss of extracel lular fluid, must be recognized in the process of dehydrat ion produced by diarrheal disease.
REFERENCES
1. Gamble, 3. L.: New Eng. J. lVi. 201: 909, 1929. 2. Itartmann, A. F., and Elman, R.: J. Exp. ~[ed. 50: 387, 1929. 3. Gamble, J. L., Blaekfan, X. D., and Hamilton, B.: J. Clin. Invest. 1: 359,
!925. 4. Blumgart, H. L., Gilllgan, D. R., Levy, R. C., Brown, M., and Volk, ~. C.:
In press. 5. l~iske, C. I~I.: J. Biol. Chem. 51: 55, 1922. 6. Butler, A. M., and Tuthill, E.: J. Biol. Chem. 93: 171, 1931. 7. Fiske, C.H.: Unpublished method. 8. Fiske, C. It., and Subbarow, u J. Biol. Chem. 66: 375~ 1925. 9. Fiske, C. It., and Lin, K. tI.: Unpublished method.
10. Van Slyke, D. D., and Sendroy, J., Jr.: J. Biol. Chem. 73: 127, 1927. 11. Peters, J. P., and Van Slyke, D.D.: Quantitative Clinical Chemistry--Interpre-
tations, Baltimore, 1931, Williams and Wilkins, p. 782. 12. MacKay, E. M., Butler, A. l~I., and Van Slyke, D. D. : Unpublished data.