Embed Size (px)
Citation preview

Intrapartum use of fetal scalp hematocrit in the diagnosis of profound fetal anemia caused by fetomatemal hemorrhage
Arie Herman, M.D., Yan Bukovsky, M.D., Levi Benson, M.D., Zvi Weinraub, M.D., and Eliyahu Caspi, M.D.
Zerifin, Israel
A case of massive fetomaternal hemorrhage that caused profound fetal anemia is presented. Timely intrapartum assessment of fetal hematocrit of 15% by means of scalp sampling aided in the delivery of a newborn infant with hemoglobin 0f 3 gm/dl and hematocrit of 10%. (AM J OssTET GYNECOL 1987;157: 1182-3.)
Key words: Fetomaternal hemorrhage, fetal anemia, scalp hematocrit
Profound fetal anemia is a life-threatening complication and is usually a result of hemorrhage, hemolysis, or isoimmunization. Antepartum and especially intrapartum diagnosis in suspicious cases may be crucial since the fetuses are not able to tolerate the stress of labor. In this case report, timely intrapartum diagnosis of unexpected 'profound anemia caused by massive fetomaternal hemorrhage helped deliver a healthy newborn infant.
From the Department of Obstetrics and Gynecology and Neonatology, Assaf Haroffe Medical Center.
Received for publication March 19, 1987; accepted May 19, 1987. Reprint requests: A, Herman, M.D., Department of Obstetrics and
Gynecology, Assaf Haroffe Medical Center, Zerifin, Israel 70300.
\
Case report A 24-year-old, gravida 1, blood type A, Rh-positive
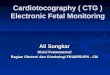
patient was referred at 39 weeks' gestation because of decreased fetal movements. Pregnancy was uneventful, and ultrasound examination performed 12 hours earlier was normal except for decreased body movements and absent breathing movements. On admission uterine size was consistent with term, and the cervix was soft, effaced 50%, admitting two fingers, and the head engaged. An oxytocin challenge test after a nonreactive nonstress test was positive (Fig. 1, A) and an induction of labor was begun. Amniotic fluid was clear and of a normal amoJ.Int. Internal monitoring demonstrated a saltatory sinusoidal pattern with decreased variability (Fig. 1, B). The results of two scalp pH examinations were 7.29 and 7.28. Because the scalp blood samples
\ : .· . .... . . : . .:-.~ .
Fig. 1. Fetal heart rate recording. (Uterine contractions are not presented.) A, Upper recording. Positive oxytocin challenge test. B, Lower recording. Intrapartum internal monitoring.
1182

Volume 157 Number 5
seemed watery, scalp blood hematocrit level was determined. The result was 15% and an emergency cesarean section was performed. A pale, 3020 gm male infant with an Apgar score of 1 at 1 minute and 5 at 5 minutes, with cord blood pH of 7.25, was delivered. Immediate resuscitation included ventilation and blood transfusion. Initial hemoglobin was 3 gm/dl, hematocrit 10%, reticulocytes 3.8%, and negative hemolytic tests. Neonatal recovery was rapid with spontaneous breathing on the same day with normal astrope. The infant was discharged after 10 days without any abnormal finding.
Developmental examinations during the following year were normal. The peripheral maternal blood test for fetal red blood cells (Kleihauer and Betke) was 2.8% (approximately 150 ml of fetal blood) and established the diagnosis of fetomaternal hemorrhage. Meticulous pathologic examination of the placenta did not show any abnormality.
Comment
Intrapartum diagnosis of severe fetal anemia was described recently by Silva et a!.' They used scalp hematocrit in a case of vaginal bleeding after amniotomy, and the low hematocrit level confirmed their suspicion of bleeding vasa previa.
Diagnosis of fetal anemia 1183
Renaer et al. 2 described eight cases and reviewed the entity of fetomaternal hemorrhage as a cause of perinatal mortality and morbidity. In only one case was fetal anemia diagnosed antenatally in an alive fetus. They used maternal blood tests for fetal red blood count and neonatal blood after delivery. Those tests are recommended in any case of trauma, placental abruption, traumatic amniocentesis, external version, or unex
plain~d fetal death. None of these was valid in our case. In this case the
nonpathologic scalp pH almost deceived us. Fortunately, the diluted appearance of the scalp sampling led us to examine fetal hematocrit. The test is feasible in most cases in which scalp sampling for pH is obtainable. We recommend its consideration in any case of suspected fetal bleeding, watery appearance of fetal blood, and significant discrepancy between fetal monitoring and scalp pH.
REFERENCES
l. Silva PO, Stoskopf CG, Keegan KA, et a!. Use of fetal scalp hematocrit in the diagnosis of severe hemorrhage from vasa previa. AMJ 0BSTET GYNECOL 1985;153:307.
2. Renaer M, Van de Putte I, Vermylen C. Massive fewmaternal hemorrhage as a cause of perinatal mortality and morbidity. Eur J Obstet Gynec Reprod Bioi 1976;6:125.