Embed Size (px)
Citation preview

s36 © Royal College of Physicians, 2013. All rights reserved.
■ RESPIRATORY MEDICINE Clinical Medicine 2013, Vol 13, No 6: s36–s40
ABSTRACT – With the advent of multi-detector computed tomography, the identification of solitary pulmonary nod-ules is becoming ever more common. Although the preva-lence of malignancy in a high risk population is only 1–1.5%, accurate identification of malignant nodules is essential to allow optimal treatment. In this article we review the most common causes of solitary pulmonary nodules and discuss diagnostic algorithms as well as some of the novel diagnostic imaging techniques in development.
KEY WORDS: Solitary pulmonary nodule, lung cancer, com-puted tomography, lung cancer screening
Background
The incidental finding of a solitary pulmonary nodule (SPN) is
taking increasing prominence in the workload of both radiologists
and respiratory physicians. The introduction of helical computed
tomography (CT) during the 1990s and, more recently, multide-
tector row CT, which can generate 1–2-mm thick slices, has ena-
bled the identification of ever smaller subcentimetre nodules.
Prevalence rates of pulmonary nodules have been reported mainly
in the context of lung cancer-screening trials and vary widely from
8% to 51%,1,2 depending upon the population studied. In addition,
approximately 10% of individuals will develop a new nodule over
a 1-year period.3 Whereas up to half of all smokers over the age of
50 years will have at least one nodule,4 the prevalence of lung
cancer in a high-risk population is only approximately 1–1.5%.2
Lung cancer is the leading cause of cancer deaths worldwide.2
The overall 5-year survival rate of patients with lung cancer
across Europe is only 10% because of the large percentage of
patients presenting with locally advanced or metastatic disease.2
This contrasts sharply with the good surgical outcomes for stage
1a (tumour size <2 cm) non-small cell lung cancer with post-
operative 5-year survival approaching 80%.1,5 Therefore,
balancing the need for identifying an early-stage lung cancer with
the risk of over-investigation and/or -radiation exposure and
provoking undue anxiety in patients with benign lesions is piv-
otal in the diagnostic evaluation and management of the SPN.
Definition
A pulmonary nodule is a round or oval lesion, 3 cm or less in
diameter, of soft-tissue density that is completely surrounded by,
and obliterates, the underlying lung parenchyma.6 The 3-cm cut
off is arbitrary because lung nodules were originally described on
chest radiographs as pulmonary opacities 1–3 cm in diameter.6,7
The advent of thin-slice spiral CT has allowed more accurate
measurement of nodule size and characterisation of morphology,
in particular the identification of ground-glass opacities. These are
intrapulmonary nodules, with a solid component of <5% of the
nodule volume, that do not attenuate the architecture of the
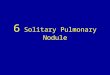
underlying lung parenchyma.8 The term ‘subsolid nodule’ is inter-
changeable with ground-glass nodule (GGN) when the latter
encompasses discrete pulmonary nodules that are either of pure
ground-glass or have part-solid attenuation (Fig 1).8
Differential diagnosis
The differential diagnosis of an incidental SPN encompasses up
to 80 different conditions.7 The probable diagnosis in any given
scenario is influenced by the individual’s age, smoking history,
history of occupational exposures and other risk factors for
malignancy, as well as country of residence.7 Some of the infec-
tious, non-infectious and neoplastic causes of an SPN are listed
in Table 1. In the absence of any other CT features, the likelihood
of a SPN being a metastasis from an extrapulmonary malignancy
Investigation and management of the solitary pulmonary nodule
Rawya Ahmed, Nagmi R Qureshi and Robert C Rintoul
Rawya Ahmed, specialty trainee in respiratory medicine, Eastern
Deanery; Nagmi R Qureshi, consultant cardiothoracic radiologist;
Robert C Rintoul, consultant respiratory physician
Papworth Hospital, Cambridge, UK Fig 1. Part-solid, part ground-glass nodule.
CMJ1306-s36-s40-Rintoul.indd 36CMJ1306-s36-s40-Rintoul.indd 36 11/21/13 9:53:49 PM11/21/13 9:53:49 PM

Investigation and management of the solitary pulmonary nodule
© Royal College of Physicians, 2013. All rights reserved. s37
mately 21–400 days.6 Faster volume-doubling times of <20 days
or slower growth rates of >400 days are more likely to reflect
infectious or benign aetiologies, respectively.9 Stability of growth
over 2 years implies a doubling time of more than 730 days;6 it
was previous conventional wisdom that this stability reflected a
benign aetiology.6,10 It is now recognised that GGNs might reflect
slow-growing adenocarcinoma and their stability over 2 years
reduces, but does not eliminate, the likelihood of malignancy.9
The best predictors for a nodule being benign are chronicity
and patterns of calcification.10 Previous imaging, if available,
rather than a bronchogenic carcinoma varies according to the
site of the original primary.9,10 It is more likely in cases of
melanoma, sarcoma or testicular carcinoma, but less likely if the
primary is a head and neck cancer, or originating from the upper
gastrointestinal tract, bladder, cervix or prostate.9
Nodule morphology and growth as a predictor of aetiology
The SPN is often an incidental finding in an asymptomatic indi-
vidual. Most malignant nodules have doubling times of approxi-
Table 1. Causes of a solitary pulmonary nodule.
Cause Features that might help support a diagnosis
Malignant neoplasm
Primary bronchogenic carcinoma Risk factors for lung cancer
Lymphoma Mediastinal or extrapulmonary lymphadenopathy; presence of B symptoms should be sought
Solitary metastasis (spread commonly from skin, head and neck, thyroid, breast, upper gastrointestinal tract, colon, ovaries, prostate, testes and skin sarcomas)
History of current and/or previous cancer of corresponding site
Carcinoid Smooth, well-defined edges, low attenuation on contrast-enhanced CT, but negative on PET
Non-infectious cause
Hamartoma Smooth well-defined edges, fat content or chondroid ‘popcorn’ pattern of calcification
Intrapulmonary lymph node Usually below the carina, subpleural or close to fissure, half-moon or polygonal in shape
Rounded atelectasis Basal, subpleural, whorl appearance
Intrapulmonary haematoma Present following recent thoracic and/or pleural procedure or intercostal chest drain insertion
Mucoid impaction Previous radiology demonstrating mucocele or bronchial atresia in corresponding region
Infected bulla History of emphysema
Infection and/or inflammation
TB and/or atypical mycobacteria Previous history of TB or presence of calcified lymph nodes; immune-compromised state
Aspergillus fumigatus Chronic lung disease; immune-compromised state
Histoplasmosis Current and/or previous residence of, or travel to, North, Central and South America
Coccidiomycosis Current and/or previous residence of, or travel to, southwestern USA
Ecchinomycosis Current and/or previous residence of, or travel to, sheep- and cattle-raising regions of the Mediterranean and Asia
Dirofilariasis Parasitic infection caused by dog heartworm, common in North America and southern Europe
Round pneumonia Pneumococcus infection
Sarcoidosis Extrapulmonary manifestations of sarcoidosis, other lung parenchymal features and mediastinal lymphadenopathy
Rheumatoid lung nodule Seropositive rheumatoid arthritis, presence of skin rheumatoid nodules
Granulomatosis with polyangiitis (Wegner’s granulomatosis)
Symptoms and extrapulmonary features suggestive of vasculitis
Benign neoplasm
Chondroma
Lipoma Low attenuation on contrast-enhanced CT, fat content
Fibroma
Neural tumour (eg neurofibroma or schwannoma) Features of neurofibromatosis
Congenital causes
Pulmonary sequestration Visible feeding vessel directly from systemic circulation
Bronchogenic cyst
CT = computerised tomography; PET = positron emission tomography; TB = tuberculosis.
CMJ1306-s36-s40-Rintoul.indd 37CMJ1306-s36-s40-Rintoul.indd 37 11/21/13 9:53:50 PM11/21/13 9:53:50 PM

Rawya Ahmed, Nagmi R Qureshi and Robert C Rintoul
s38 © Royal College of Physicians, 2013. All rights reserved.
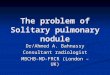
might provide valuable information about chronicity and aeti-
ology. Hamartomas can exhibit chondroid or ‘popcorn-like’
calcification (Fig 2). A wholly calcified nodule is likely to be an
old granuloma, as are nodules with central or laminated
calcification patterns.6 By contrast, eccentric or peripheral calci-
fication can imply a carcinoma that has engulfed an adjacent
calcified granuloma and this should raise suspicion of a
malignant process.1
Other morphological characteristics, such as nodule mar-
gins, cavitation and wall thickness and the presence of satellite
nodules, do not enable distinction between benign and
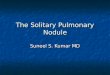
malignant nodules.6 Spicules and lobulated margins can repre-
sent irregular interstitial fibrosis or infiltrative tumour growth
(Fig 3).9,11 Although the presence of lobulated or spiculated
margins increases the likelihood of malignancy, it is not a pre-
requisite, because one in five nodules with smooth margins is
malignant.1,6 It is now recognised that some indeterminant
subpleural or intraparenchymal nodules represent intra-
pulmonary lymph nodes (IPLNs).12 Ranging in size between 3
and 10 mm, IPLNs can wax and wane in size, confusing the
unwary and leading to repeat CT for an otherwise ‘normal’
structure. Confident diagnosis by an experienced thoracic
radiologist, based on location and morphology, can often avoid
unnecessary patient anxiety.
Evaluating the growth rate of an SPN can be difficult and is
dependent upon its size. For a spherical nodule, a doubling of its
volume results in only a 26–30% increase in its diameter.8,10
Accurately and reproducibly measuring a 1-mm increase in diam-
eter of a 4-mm nodule is harder than for a 3-cm mass. A 1-mm
increase in diameter of a 4-mm nodule represents a doubling in
volume1 that, if occurring during a certain time frame, increases
the likelihood of malignancy. However, this can be easily over-
looked given intra- and inter-observer variation in nodule size
measurements, particularly in the presence of spiculated margins.
In the context of lung-screening trials, up to one in five posi-
tive-screening CT scans at baseline were the result of part-solid
or non-solid GGNs.8 Such lesions are associated with higher
rates of malignancy, with adenocarcinoma being the most
common subtype.8,11 The previously used term ‘bronchiolo-
alveolar carcinoma’ has recently been reclassified in a continuum
of pre-invasive to overtly malignant subtypes, with atypical
adenomatous hyperplasia being a premalignant subtype and
adenocarcinoma in situ and minimally invasive adenocarcinoma
describing lesions with lepidic growth patterns, with and without
invasive features, respectively.13 Invasive adenocarcinoma is fur-
ther subdivided according to growth patterns.13
Risk assessment
The diagnostic approach to the incidental SPN should include
a thorough assessment of the individual with a full history
and physical examination, with particular attention paid to
factors increasing cancer risk. In addition to routinely identi-
fied risk factors for lung cancer, such as age, active and passive
smoking history and occupational exposure to carcinogens,
including asbestos, other risk factors should not be over-
looked. Previous history of cancer of any type as well as
exposure to radiotherapy, cancer in a first-degree relative and
lung parenchymal abnormalities, such as chronic obstructive
pulmonary disease and interstitial pulmonary fibrosis, should
be recorded.
The probability of a nodule being malignant increases with
age, being <3% in under-40-year olds, but 50% in those over 60
years of age.1 Furthermore, the prevalence of malignancy
increases with nodule size and is estimated from lung cancer-
screening study data to be <1% in nodules <5 mm in diameter,
and >80% in those larger than 2 cm.1 Hence, evaluating an SPN
in the context of a patient’s age and other risk factors, along with
its size, enables a quanitative assessment of lung cancer risk and
guides the management approach.
Quantitative risk assessment of lung cancer was originally
proposed during the 1970s, using Bayesian analysis,7 and has
been advocated again recently.14 Various mathematical models
exist using a combination of the individual’s characteristics (eg
age, smoking history and previous history of cancer) and fea-
tures of the SPN (eg nodule size and location, and presence of
spiculations) to compute a likelihood ratio of cancer.14,15 Patel et
al argue that a pre-test probability calculation improves risk
stratification and facilitates further management along Fleischner
Society guidelines.14
Diagnostic algorithm
CT is the modality of choice for the initial diagnosis and followup
of pulmonary nodules. Contrast-enhanced CT enables identifica-
tion of parenchymal abnormalities as well as staging of the medi-
astinum and extrapulmonary structures. Unenhanced low-dose
thin-slice multidetector row CT is best utilised for characterising
nodule morphology and assessing growth on followup.
Fig 2. ‘Popcorn’ pattern calcification within a hamartoma in an unenhanced computer tomograph scan of chest.
CMJ1306-s36-s40-Rintoul.indd 38CMJ1306-s36-s40-Rintoul.indd 38 11/21/13 9:53:51 PM11/21/13 9:53:51 PM

Investigation and management of the solitary pulmonary nodule
© Royal College of Physicians, 2013. All rights reserved. s39
Fig 3. Spiculated pulmonary nodule that is highly suggestive of malignancy.
from malignant nodules in a retrospective case series with a
sensitivity and specificity of 91% and 90%, respectively.17
Nodule volume measurements and volume-doubling time esti-
mation using CT volumetric software is currently being utilised
in the UK Lung Screen (UKLS) and the Dutch-Belgian (NELSON)
lung cancer screening trials, comparing low-dose CT with usual
care in those at higher risk of lung cancer.18,19
The degree of contrast enhancement of a nodule depends upon
its vascularity, with correlation between nodule vascular endothe-
lial growth factor expression and microvessel density and uptake
of intravenous contrast medium.6,20 Administration of contrast
followed by serial image acquisition at 60-s intervals for 4 min
enables the measurement of nodule enhancement at fixed time
intervals and the calculation of net enhancement values. A
nodule demonstrating an increase of 15 Hounsfield units (HU)
or less after injection of contrast is likely to be benign, whereas an
increase of >30 HU suggests malignancy.21 A cut-off value of 15
HU has a high sensitivity (98%), reducing false negative rates, but
limited specificity (58%), with an overlap in enhancement pat-
terns and attenuation values between benign and malignant
lesions. The utility of dynamic contrast-enhanced CT is being
investigated in the current UK-based Solitary Pulmonary Nodule
Investigation trial (SPUtNIk).22 This study also includes health
economic modelling for the evaluation of SPNs.
Dynamic contrast-enhanced magnetic resonance imaging
(MRI) is emerging as a tool with better sensitivity and specificity
than CT or PET in distinguishing malignant from benign nod-
ules, in particular those associated with active inflammation.9,23
Investigators have studied different aspects of this technique,
with some looking at the initial first pass of contrast via the arte-
rial system, whereas others have analysed the arterial inflow and
subsequent diffusion and redistribution of contrast into the
Positron emission tomography (PET) uses a positron-emitting
radionuclide isotope of fluorine attached to a glucose analogue
(18F-fluorodeoxyglucose [FDG]) that is avidly taken up by
tissue with high metabolic activity. Combining PET with CT
enables better anatomical correlation of parenchymal abnor-
mality on CT with areas of high metabolic activity on PET, as
well as assessment of the mediastinum for the purposes of
staging. Sensitivity and specificity values of combined PET-CT
have been shown by several studies to be superior to those for
PET or CT alone, and have been reported to be as high as 96%
and 88%, respectively, with a negative predictive value of 92%.9
FDG uptake is influenced by tumour size and metabolic activity
and, thus, PET has a limited role in the diagnostic assessment of
small (<8–10 mm) or purely GGNs.9,16
The approach to the management of the incidental solid SPN
should follow Fleischner Society guidelines,4 outlined in Table 2.
These propose surveillance CT scan followup at set intervals
based on nodule size (mean of length and width) and the indi-
vidual’s risk factors for malignancy; the low-risk group being
those with no or minimal smoking history and no risk factors
for malignancy. The guidelines are not applicable to those sus-
pected of having infection, undergoing CT as part of staging for
known or suspected carcinoma of any site, or those under the
age of 35 years.
Fleischner Society recommendations have recently been pro-
duced for the management of subsolid nodules.13 All individuals
are considered equally without risk stratification and subsolid
nodules are assessed depending on their type and multiplicity.
When assessing multiple nodules, the recommendations are
based on the features of the dominant lesion. It is worth noting
that these recommendations are based on low-dose thin-slice
(1-mm) CT scans reconstructed with appropriate windows for
the solid and non-solid components, with measurements per-
formed across two dimensions and growth assessed against the
original baseline CT. Pure GGNs ≤5 mm do not require followup
if solitary, provided it is confirmed that they have no solid com-
ponent on thin-slice CT. If multiple, interval scans at 2 and 4
years are recommended, as well as investigations to rule out other
causes of multiple GGNs. If >5 mm, pure GGNs, whether solitary
or multiple, require an initial scan at 3 months to confirm persist-
ence and then annual CT scans for a minimum of 3 years. Solitary
part-solid GGNs require initial CT scans at 3 months and, if per-
sistent and with a solid component of <5 mm, can be followed
annually. Part-solid GGNs with a solid component >5 mm
should be considered for biopsy or surgical resection.
Novel diagnostic imaging techniques
Several imaging techniques to better enable differentiation
between benign and malignant lesions are being evaluated.
Nodule growth can be estimated from volumetric measurements
and prediction about likelihood of malignancy inferred from
calculation of volume-doubling time. Using a volume-doubling
time of 500 days as the upper limit for malignancy, but excluding
GGNs, Revel et al proposed a strategy to differentiate benign
CMJ1306-s36-s40-Rintoul.indd 39CMJ1306-s36-s40-Rintoul.indd 39 11/21/13 9:53:51 PM11/21/13 9:53:51 PM

Rawya Ahmed, Nagmi R Qureshi and Robert C Rintoul
s40 © Royal College of Physicians, 2013. All rights reserved.
MacMahon H, Austin JHM, Gamsu G 4 et al. Guidelines for the man-
agement of small pulmonary nodules detected on CT scans: a state-
ment from the Fleischner Society. Radiology 2005;237:395–400.
Detterbeck FC, Boffa DJ, Tanoue LT. The new lung cancer staging 5
system. Chest 2009;136:260–71.
Hartman TE. Radiologic evaluation of the solitary pulmonary nodule. 6
Semin Thorac Cardiovasc Surgery 2002;14:261–7.
Toomes H, Delphendahl A, Manke HG, Vogt-Moykopf I. The coin 7
lesion of the lung. Cancer 1983;51:534–7.
Henschke CI, Yakelevitz DF, Mirtcheva R 8 et al. CT screening for lung
cancer: frequency and significance of part-solid and nonsolid nodules.
Am J Roentgenol 2002;178:1053–7.
Patel VK, Naik SK, Naidich DP 9 et al. A practical algorithmic approach
to the diagnosis and management of solitary pulmonary nodules. Part
1: Radiological characteristics and imaging modalities. Chest
2013;143:825–39.
Ost D, Fein AM, Feinsilver SH. The solitary pulmonary nodule. 10 N Engl
J Med 2003;348:2535–42.
Kim HY, Shim YM, Lee KS 11 et al. Persistent pulmonary nodular ground
glass opacity at thin-section CT: histopathologic comparisons.
Radiology 2007;245:267–75.
Ahn MI, Gleeson TG, Chan IH 12 et al. Perifissural nodules seen at CT
screening for lung cancer. Radiology 2010;254:949–56.
Naidich DP, Bankier AA, MacMahon H 13 et al. Recommendations for
the management of subsolid pulmonary nodules detected at CT: A
statement from the Fleischner Society. Radiology 2013;266:304–17.
Patel VK, Naik SK, Naidich DP 14 et al. A practical algorithmic approach
to the diagnosis and management of solitary pulmonary nodules: Part
2: Pretest probability and algorithm. Chest 2013;143:840–6.
Chest X-ray.com. SPN Calculator, 2013. www.chestx-ray.com/index.15
php/calculators/spn-calculator [Accessed 19 November 2013].
Yap CS, Schiepers C, Fishbein MC 16 et al. FDG-PET imaging in lung
cancer: how sensitive is it for bronchioloalveolar carcinoma? Eur J
Nucl Med 2002;29:1166–73.
Revel MP, Merlin A, Peyrard S 17 et al. Software volumetric evaluation of
doubling times for differentiating benign versus malignant pulmonary
nodules. Am J Roentgenol 2006;187:135–42.
Baldwin DR, Duffy SW, Wald NJ 18 et al. UK Lung Screen (UKLS) nodule
management protocol: modeling of a single screen randomized con-
trolled trial of low-dose CT screening for lung cancer. Thorax
2011;66:308–13.
Horeweg N, van der Aalst CM, Thunnissen E 19 et al. Characteristics of
lung cancers detected by computer tomography screening in the rand-
omized NELSON trial. Am J Respir Crit Care Med 2013;187:848–54.
Yi CA, Lee KS, Kim EA 20 et al. Solitary pulmonary nodules: dynamic
enhanced multi-detector row CT study and comparison with vascular
endothelial growth factor and microvessel density. Radiology
2004;233:191–9.
Swensen SJ, Viggiano RW, Midthun DE 21 et al. Lung nodule enhance-
ment at CT: multicentre study. Radiology 2000;214:73–80.
UK Clinical Research Network Study Portfolio, 2013. http://public.22
ukcrn.org.uk/Search/Portfolio.aspx?titleAcro=sputnik&SearchType=Any
[Accessed 2 October 2013].
Zou Y, Zhang M, Wang Q 23 et al. Quantative investigation of solitary
pulmonary nodules: dynamic contrast–enhanced MRI and histopatho-
logic analysis. Am J Roentgenol 2008;191:252–9.
Address for correspondence: Dr RC Rintoul, Department of Thoracic Oncology, Papworth Hospital, NHS Foundation Trust, Papworth Everard, Cambridge CB23 3RE.Email: [email protected]
interstitial space. Distinct patterns of contrast uptake and
washout demonstrated in malignant and benign inflammatory
nodules have been attributed to differences in nodule micro-
vasculature architecture.23
Summary
The SPN poses a diagnostic challenge that requires careful
clinical–radiological correlation by an expert multidisciplinary
team to avoid over-investigation of benign lesions, while
improving lung cancer survival through detection of early-stage
disease amenable to surgical resection. At present, the Fleischner
guidelines form the backbone for nodule management, although
novel imaging techniques might enable further refinement to
this approach in the future.
References
Wahidi MM, Govert JA, Goudar RK 1 et al. Evidence for the treatment
of patients with pulmonary nodules: when is it lung cancer? Chest
2007;132:94S–107S.
Pastorino U. Current status of lung cancer screening. 2 Thorac Surg Clin
2013;23:129–40.
Pastorino U, Bellomi M, Landoni C. Early lung cancer detection with 3
spiral CT and positron emission tomography in heavy smokers: 2 year
results. Lancet 2003;362:593–97.
Table 2. Fleischner Society guidelines for CT surveillance of incidental solitary pulmonary nodules.
Nodule size* (mm)
CT interval periods from baseline scan (if no change in nodule size)
Low-risk individual†
≤4 mm None required
>4–6 mm 12 months then discharge if remains stable
>6–8 mm 6–9 months, 18–24 months, then discharge
>8 mm Consider further evaluation with contrast-enhanced CT scan, PET-CT and biopsy; otherwise surveillance at 3, 9 and 24 months
High-risk individual†
≤4 mm 12 months then discharge if no change in nodule size
>4–6 mm 6–9 months, 18–24 months, then discharge if no change
>6–8 mm 3–6 months, 9–12 months, 24 months, then discharge if no change
>8 mm Consider further evaluation with contrast-enhanced CT scan, PET-CT and biopsy; otherwise surveillance at 3, 9 and 24 months
*Size is a mean of 2 axial measurements (length and width).†Risk is categorised as low if there is no or minimal history of smoking and no other risk factors for malignancy. High-risk individuals have a history of smoking and/or other risk factors for malignancy.
CT = computerised tomography; PET = positron emission tomography.
CMJ1306-s36-s40-Rintoul.indd 40CMJ1306-s36-s40-Rintoul.indd 40 11/21/13 9:53:52 PM11/21/13 9:53:52 PM