Embed Size (px)
Citation preview
Iron Deficiency Iron Deficiency AnemiaAnemia
DefinitionDefinition
Iron deficiencyIron deficiency is defined as a decreased is defined as a decreased total iron body contenttotal iron body content..Iron deficiency anemiaIron deficiency anemia occurs when iron occurs when iron deficiency is sufficiently severe to diminish deficiency is sufficiently severe to diminish erythropoiesis and cause the development erythropoiesis and cause the development of anemiaof anemia . .
Iron deficiency is the most prevalent single Iron deficiency is the most prevalent single deficiency state on a worldwide basis. It is deficiency state on a worldwide basis. It is important economically because it important economically because it diminishes the capability of individuals diminishes the capability of individuals who are affected to perform physical labor, who are affected to perform physical labor, and it diminishes both growth and learning and it diminishes both growth and learning in childrenin children..
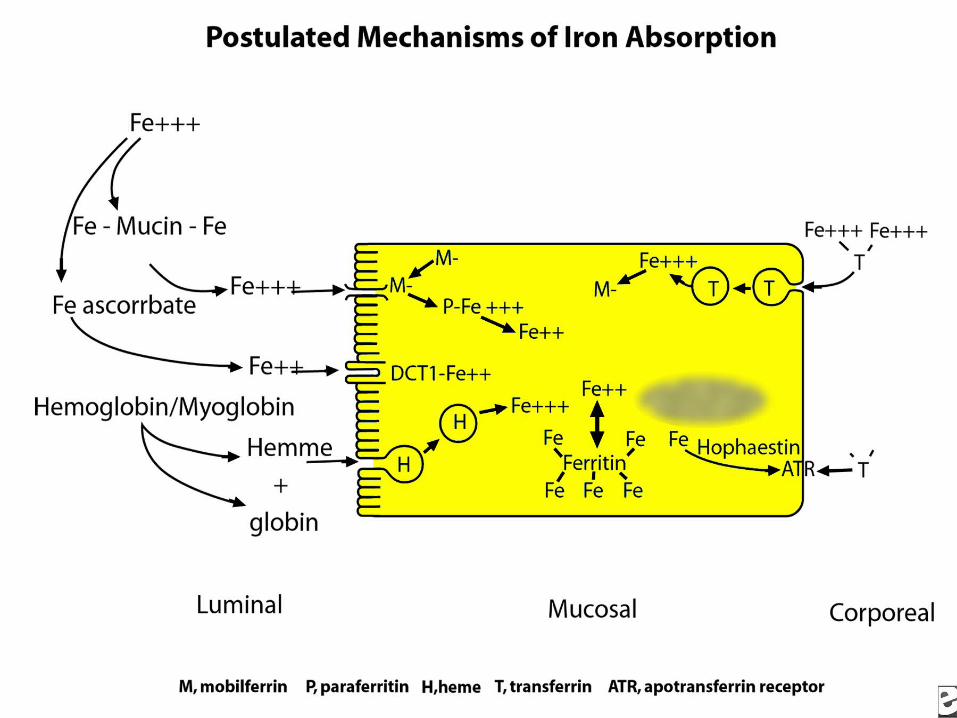
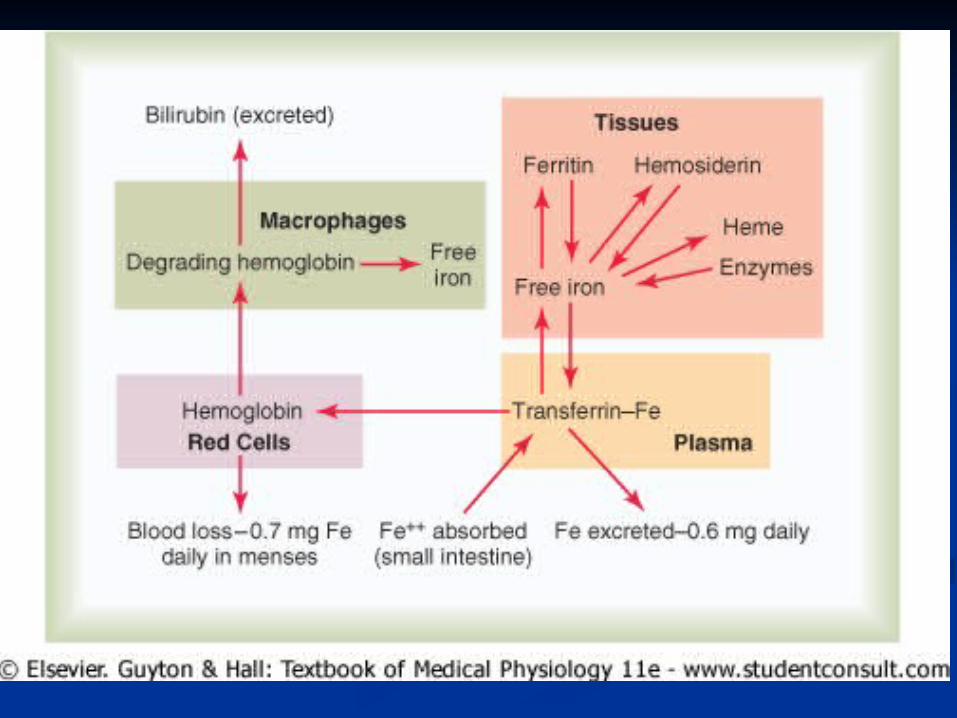
Some iron is lost from the blood due Some iron is lost from the blood due to hemorrhage, menstruation, etc. to hemorrhage, menstruation, etc. and must be replaced from the dietand must be replaced from the diet . .On average men need to replace On average men need to replace about 1 mg of iron per day, women about 1 mg of iron per day, women need 2 mgneed 2 mg per day per day. Apotransferrin . Apotransferrin (transferrin without the iron) is (transferrin without the iron) is present in GI lining cells and is present in GI lining cells and is also released in the bile. It picks up also released in the bile. It picks up iron from the GI tract and iron from the GI tract and stimulates receptors on the lining stimulates receptors on the lining cells which absorb it by pinocytosiscells which absorb it by pinocytosis . .
Once through the mucosal cell iron is Once through the mucosal cell iron is carried in blood as transferrin to the carried in blood as transferrin to the liver and marrow. Iron leaves the liver and marrow. Iron leaves the transferrin molecule to bind to transferrin molecule to bind to ferritin ferritin in these tissues. Most excess in these tissues. Most excess iron will not be absorbed due to iron will not be absorbed due to saturation of ferritin, reduction of saturation of ferritin, reduction of apotransferrin, and an inhibitory apotransferrin, and an inhibitory process in the lining tissue (process in the lining tissue (Mucosal Mucosal CurtainCurtain))..
IRONIRON
Essential for the synthesis of Essential for the synthesis of HemoglobinHemoglobin..
Deficiency causes Deficiency causes Microcytic, Microcytic, Hypochromic AnemiaHypochromic Anemia..
The The MCV (MEAN MCV (MEAN CORPUSCULAR VOLUME-CORPUSCULAR VOLUME-NORMAL 90), Color Index & NORMAL 90), Color Index & MCHMCH (MEAN CORPUSCULAR (MEAN CORPUSCULAR HEMOGLOBIN) are lowHEMOGLOBIN) are low..
ERYTHROID PROGENITOR CELLSERYTHROID PROGENITOR CELLS
BFU-EBFU-E: Burst Forming Unit – : Burst Forming Unit – ErythrocyteErythrocyte::
Give rise each to thousands of Give rise each to thousands of nucleated erythroid precursor nucleated erythroid precursor
cells, in vitrocells, in vitro..Undergo some changes to Undergo some changes to
become the Colony Forming become the Colony Forming Units-Erythrocyte (Units-Erythrocyte (CFU-ECFU-E))
Regulator: Burst Promoting Regulator: Burst Promoting Activity (Activity (BPABPA))
ERYTHROID PROGENITOR CELLSERYTHROID PROGENITOR CELLS
CFU-ECFU-E: Colony Forming Unit- : Colony Forming Unit- ErythrocyteErythrocyte::
Well differentiated erythroid Well differentiated erythroid progenitor cellprogenitor cell..
Present only in the Red Bone Present only in the Red Bone MarrowMarrow..
Can form upto 64 nucleated Can form upto 64 nucleated erythroid precursor cellserythroid precursor cells..
Regulator: Regulator: ErythropoietinErythropoietin..Both these Progenitor cells Both these Progenitor cells
cannot be distinguished except cannot be distinguished except by in vitro culture methodsby in vitro culture methods..
Normoblastic PrecursorsNormoblastic Precursors
PROERYTHROBLAST PROERYTHROBLAST (PRONORMOBLAST)(PRONORMOBLAST)::
Large cell: 15 – 20 Microns in Large cell: 15 – 20 Microns in diameterdiameter..
Cytoplasm is deep violet-blue Cytoplasm is deep violet-blue stainingstaining
Has Has no Hemoglobinno Hemoglobin..Large nucleus 12 Microns occupies Large nucleus 12 Microns occupies
3/43/4thth of the cell volume of the cell volume..Nucleus has fine stippled reticulum Nucleus has fine stippled reticulum
& many nucleoli& many nucleoli..
Normoblastic PrecursorsNormoblastic Precursors
EARLY EARLY NORMOBLAST(BASOPHILIC NORMOBLAST(BASOPHILIC
ERYTHROBLAST)ERYTHROBLAST)::Smaller in sizeSmaller in size..Shows active MitosisShows active Mitosis..No nucleoli in the nucleusNo nucleoli in the nucleus..Fine chromatin network with Fine chromatin network with
few condensation nodes foundfew condensation nodes found..Hemoglobin begins to formHemoglobin begins to form..Cytoplasm still BasophilicCytoplasm still Basophilic..
Normoblastic PrecursorsNormoblastic Precursors
INTERMEDIATE INTERMEDIATE NORMOBLAST(ERYTHROBLASNORMOBLAST(ERYTHROBLAST)T)::
Has a diameter of 10 – 14 Has a diameter of 10 – 14 MicronsMicrons..
Shows active MitosisShows active Mitosis..
Increased Hemoglobin content in Increased Hemoglobin content in the cytoplasmthe cytoplasm
Cytoplasm is Cytoplasm is PolychromatophilicPolychromatophilic..
Normoblastic PrecursorsNormoblastic Precursors
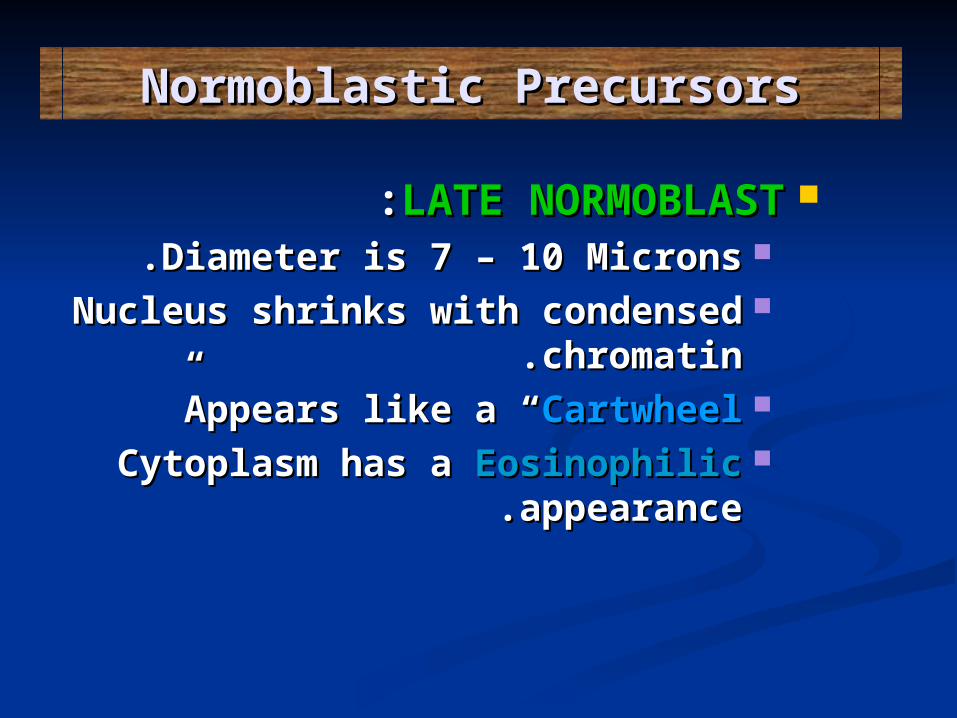
LATE NORMOBLASTLATE NORMOBLAST::Diameter is 7 – 10 MicronsDiameter is 7 – 10 Microns..Nucleus shrinks with condensed Nucleus shrinks with condensed
chromatinchromatin..Appears like a “Appears like a “CartwheelCartwheel””Cytoplasm has a Cytoplasm has a EosinophilicEosinophilic
appearanceappearance..
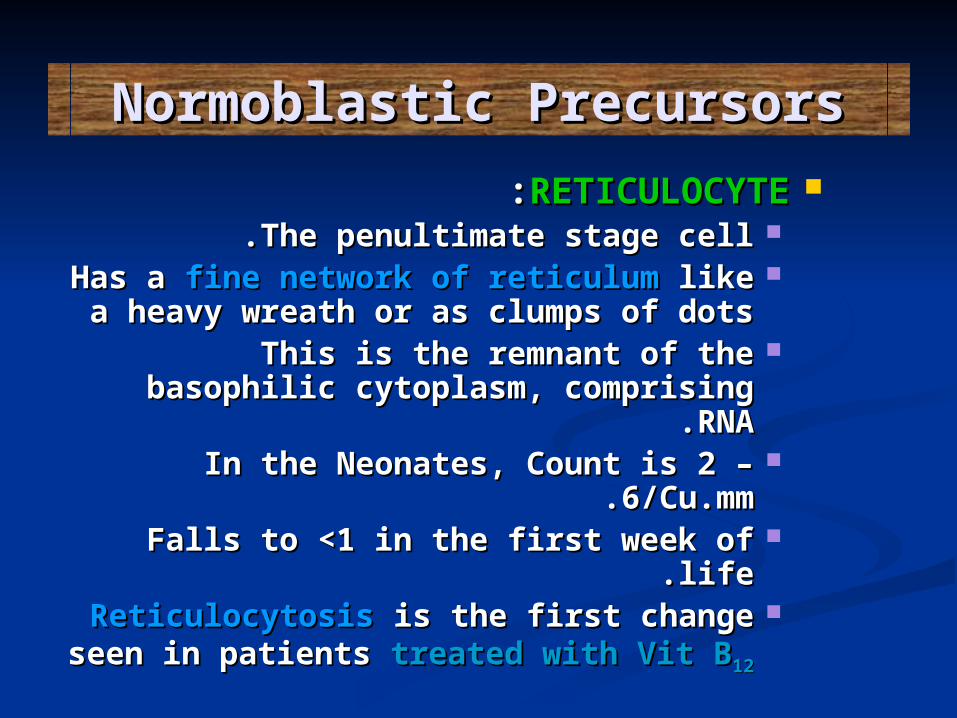
Normoblastic PrecursorsNormoblastic PrecursorsRETICULOCYTERETICULOCYTE::
The penultimate stage cellThe penultimate stage cell..Has a Has a fine network of reticulum fine network of reticulum like a like a
heavy wreath or as clumps of dotsheavy wreath or as clumps of dotsThis is the remnant of the basophilic This is the remnant of the basophilic
cytoplasm, comprising RNAcytoplasm, comprising RNA..In the Neonates, Count is 2 – In the Neonates, Count is 2 –
6/Cu.mm6/Cu.mm..Falls to <1 in the first week of lifeFalls to <1 in the first week of life..ReticulocytosisReticulocytosis is the first change is the first change
seen in patients seen in patients treated with Vit Btreated with Vit B1212
Normoblastic PrecursorsNormoblastic Precursors
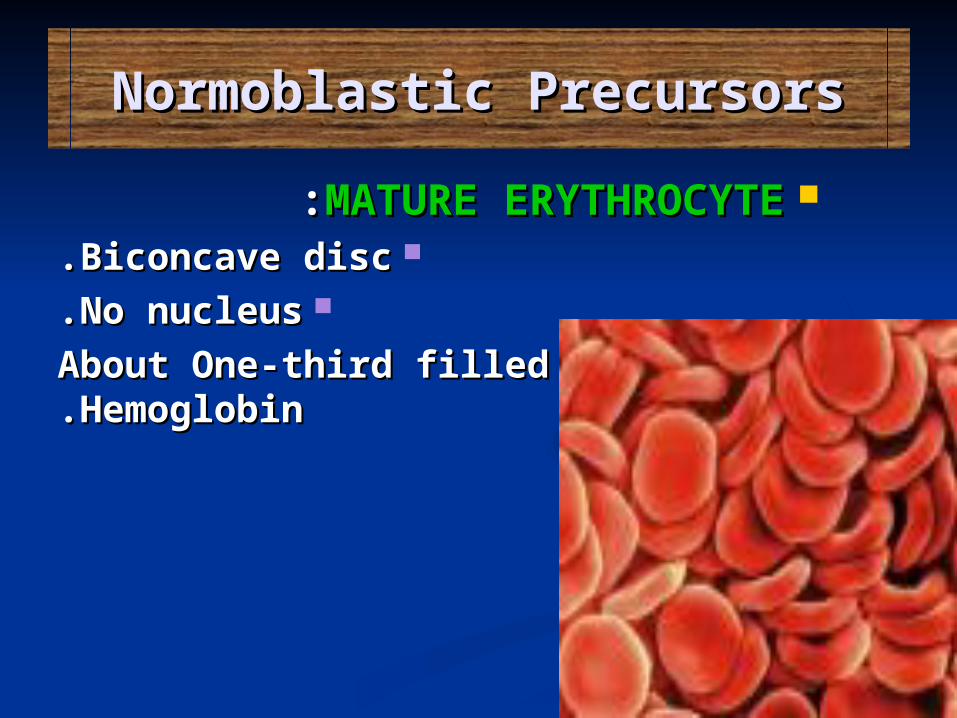
MATURE ERYTHROCYTEMATURE ERYTHROCYTE::Biconcave discBiconcave disc..
No nucleusNo nucleus..About One-third filled with About One-third filled with
HemoglobinHemoglobin..
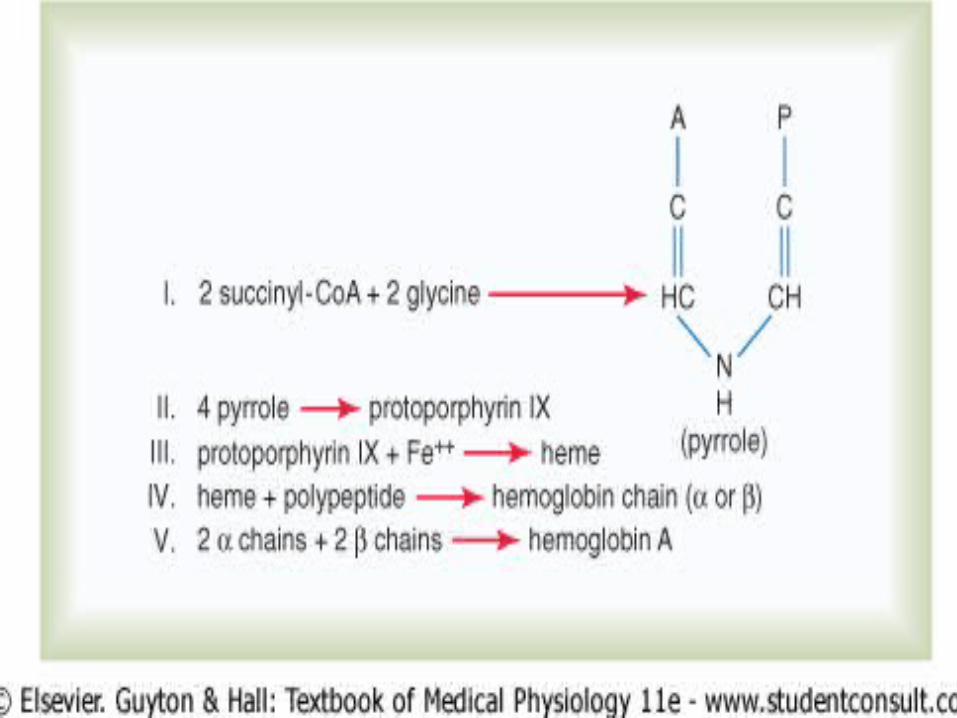
Iron MetabolismIron Metabolism Uses of Iron in bodyUses of Iron in body::
11..For the formation of For the formation of hemoglobinhemoglobin
22 . .For formation of other elements like e.g., For formation of other elements like e.g., myoglobinmyoglobin, , cytochromescytochromes, , cytochrome oxidasecytochrome oxidase, , peroxidaseperoxidase, , catalasecatalaseThe total quantity of iron in the body averages The total quantity of iron in the body averages 4 to 5 grams4 to 5 grams,,
11 . .6565 % % in the form of hemoglobinin the form of hemoglobin . .22 . .44 per cent is in the form of myoglobinper cent is in the form of myoglobin , ,
33 . .11 per cent is in the form of the various heme per cent is in the form of the various heme compounds that promote intracellular compounds that promote intracellular oxidationoxidation , ,
44 . .0.10.1 per cent is combined with the protein per cent is combined with the protein transferrin in the blood plasmatransferrin in the blood plasma , ,
55 . .1515 to 30 per cent is stored for later use, to 30 per cent is stored for later use, mainly in the reticuloendothelial system and mainly in the reticuloendothelial system and liver parenchymal cells, principally in the liver parenchymal cells, principally in the form of ferritinform of ferritin..
Daily Loss of IronDaily Loss of Iron.. 11 . .Excretion in faeces: 0.6 milligram per dayExcretion in faeces: 0.6 milligram per day , ,
22 . .Loss due to bleeding in woman due to menstrual Loss due to bleeding in woman due to menstrual loss :1.3 mg/dayloss :1.3 mg/day..
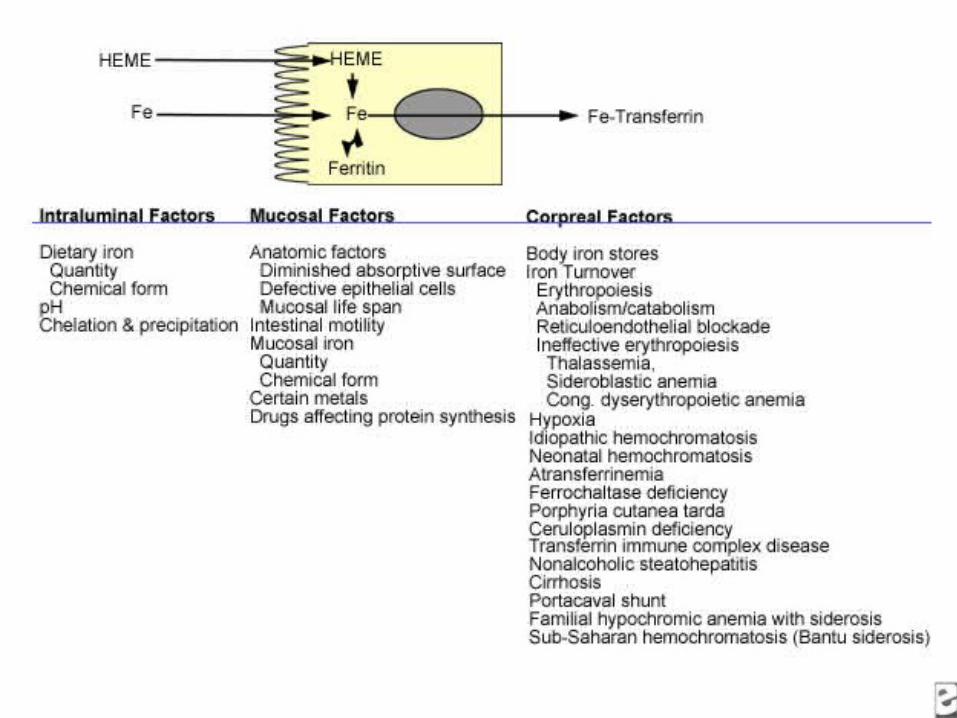
Absorption of Iron from the Intestinal TractAbsorption of Iron from the Intestinal Tract Iron is absorbed from all parts of the small intestine, Iron is absorbed from all parts of the small intestine, mostly by the following mechanismmostly by the following mechanism . .
The liver secretes moderate amounts of The liver secretes moderate amounts of apotransferrinapotransferrin into the bile, which flows through the bile duct into into the bile, which flows through the bile duct into the duodenumthe duodenum . .
In duodenum the apotransferrin binds with iron and In duodenum the apotransferrin binds with iron and with hemoglobin and myoglobin from meat. This with hemoglobin and myoglobin from meat. This combination is called combination is called transferrintransferrin..
Transferrin binds with receptors in the membranes of Transferrin binds with receptors in the membranes of the intestinal epithelial cellsthe intestinal epithelial cells . .
Then, by pinocytosis, the transferrin molecule, carrying Then, by pinocytosis, the transferrin molecule, carrying its iron store, is absorbed into the epithelial cells its iron store, is absorbed into the epithelial cells and released into the blood capillaries beneath these and released into the blood capillaries beneath these cells in the form of cells in the form of plasma transferrinplasma transferrin . .
Iron absorption from the intestines is very slow, only a Iron absorption from the intestines is very slow, only a few milligrams per day. Therefore even when large few milligrams per day. Therefore even when large quantities of iron are present in the food, only small quantities of iron are present in the food, only small proportions can be absorbedproportions can be absorbed..
Regulation of Total Body Iron by Regulation of Total Body Iron by Controlling Rate of AbsorptionControlling Rate of Absorption..
When the body has become saturated with When the body has become saturated with iron so that essentially all apoferritin in iron so that essentially all apoferritin in the iron storage areas is already combined the iron storage areas is already combined with iron, the rate of additional iron with iron, the rate of additional iron absorption from the intestinal tract absorption from the intestinal tract becomes greatly decreasedbecomes greatly decreased . .
On the contrary, when the iron stores have On the contrary, when the iron stores have become depleted, the rate of absorption become depleted, the rate of absorption can increase five times normal. Thus, total can increase five times normal. Thus, total body iron is regulated by altering the rate body iron is regulated by altering the rate of absorptionof absorption..
EpidemiologyEpidemiologyIn North America and Europe, iron In North America and Europe, iron deficiency is most common in women of deficiency is most common in women of childbearing age and usually as a childbearing age and usually as a manifestation of hemorrhagemanifestation of hemorrhage . .
Iron deficiency caused solely by diet is Iron deficiency caused solely by diet is uncommonuncommon in adults in countries where in adults in countries where meat is an important part of the dietmeat is an important part of the diet . .
Depending upon the criteria used for the Depending upon the criteria used for the diagnosis of iron deficiency, approximately diagnosis of iron deficiency, approximately 4-8% of premenopausal women are iron 4-8% of premenopausal women are iron deficientdeficient . .
In men and postmenopausal women, iron In men and postmenopausal women, iron deficiency is uncommon in the absence of deficiency is uncommon in the absence of bleedingbleeding..
RaceRaceRace probably has Race probably has no significant effect no significant effect upon the upon the occurrence of iron deficiency anemia; however, occurrence of iron deficiency anemia; however, because diet and socioeconomic factors play a role because diet and socioeconomic factors play a role in the prevalence of iron deficiency, it more in the prevalence of iron deficiency, it more frequently is observed in people of various racial frequently is observed in people of various racial backgrounds living in poorer areas of the worldbackgrounds living in poorer areas of the world..
SexSexAn adult male absorbs and loses about 1 mg of iron An adult male absorbs and loses about 1 mg of iron from a diet containing 10-20 mg daily. During from a diet containing 10-20 mg daily. During childbearing years, an adult female loses an childbearing years, an adult female loses an average of 2 mg of iron daily and must absorb a average of 2 mg of iron daily and must absorb a similar quantity of iron in order to maintain similar quantity of iron in order to maintain equilibrium. Because the average woman eats less equilibrium. Because the average woman eats less than the average man does, she must be more than than the average man does, she must be more than twice as efficient in absorbing dietary iron in order twice as efficient in absorbing dietary iron in order to maintain equilibrium and avoid developing iron to maintain equilibrium and avoid developing iron deficiency anemiadeficiency anemia..
EtiologyEtiologyDietDiet MeatMeat provides a source of heme iron, which is less affected by provides a source of heme iron, which is less affected by the dietary constituents that markedly diminish the dietary constituents that markedly diminish bioavailability than nonheme iron is. The prevalence of iron bioavailability than nonheme iron is. The prevalence of iron deficiency anemia is low in geographic areas where meat is deficiency anemia is low in geographic areas where meat is an important constituent of the diet. In areas where meat is an important constituent of the diet. In areas where meat is sparse, iron deficiency is commonplacesparse, iron deficiency is commonplace . .
Substances that diminish the absorption of ferrous and ferric Substances that diminish the absorption of ferrous and ferric iron areiron are phytates phytates, , oxalatesoxalates, , phosphatesphosphates, , carbonatescarbonates, and , and tannatestannates. These substances have little effect upon the . These substances have little effect upon the absorption of heme iron. Similarly, ascorbic acid increases absorption of heme iron. Similarly, ascorbic acid increases the absorption of ferric and ferrous iron and has little effect the absorption of ferric and ferrous iron and has little effect upon the absorption of heme ironupon the absorption of heme iron . .Purified heme is absorbed poorly because heme polymerizes into macromolecules. Globin degradation products diminish heme polymerization, making it more available for absorption. They also increase the absorption of nonheme iron because the peptides from degraded globin bind the iron to prevent both precipitation and polymerization; thus, absorption of iron in spinach is increased when eaten with meat. Heme and nonheme iron uptake by intestinal
absorptive cells is noncompetitive.
HemorrhageHemorrhage
Bleeding for any reason produces iron depletion. If Bleeding for any reason produces iron depletion. If sufficient blood loss occurs, iron deficiency sufficient blood loss occurs, iron deficiency anemia ensuesanemia ensues . .
A single sudden loss of blood produces a post-A single sudden loss of blood produces a post-hemorrhagic anemia that is normocytic. The hemorrhagic anemia that is normocytic. The bone marrow is stimulated to increase bone marrow is stimulated to increase production of hemoglobin, thereby depleting iron production of hemoglobin, thereby depleting iron in body stores. Once they are depleted, in body stores. Once they are depleted, hemoglobin synthesis is impaired and microcytic hemoglobin synthesis is impaired and microcytic hypochromic erythrocytes are producedhypochromic erythrocytes are produced..
Maximal changes in the red blood cell cellular Maximal changes in the red blood cell cellular indices occur in approximately 120 days, at a indices occur in approximately 120 days, at a time when all normal erythrocytes produced time when all normal erythrocytes produced prior to the hemorrhage are replaced by prior to the hemorrhage are replaced by microcytesmicrocytes . .
Prior to this time, the peripheral smear shows a Prior to this time, the peripheral smear shows a dimorphic population of erythrocytes, normocytic dimorphic population of erythrocytes, normocytic cells produced prior to the bleed, and microcytic cells produced prior to the bleed, and microcytic cells produced after bleeding. This is reflected in cells produced after bleeding. This is reflected in the red blood cell distribution width (RDW); the red blood cell distribution width (RDW); thus, the earliest evidence of the development of thus, the earliest evidence of the development of an iron-deficient erythropoiesis is seen in the an iron-deficient erythropoiesis is seen in the peripheral smear and by an increased RDWperipheral smear and by an increased RDW..
Hemosiderinuria, hemoglobinuria, and pulmonary Hemosiderinuria, hemoglobinuria, and pulmonary hemosiderosishemosiderosis Iron deficiency anemia can occur from loss of body iron in Iron deficiency anemia can occur from loss of body iron in the urine. If a freshly obtained urine specimen appears the urine. If a freshly obtained urine specimen appears bloody but contains no red blood cells, suspect bloody but contains no red blood cells, suspect hemoglobinuria. Obtain confirmation in the laboratory hemoglobinuria. Obtain confirmation in the laboratory that the pigment is hemoglobin and not myoglobin. This that the pigment is hemoglobin and not myoglobin. This can be accomplished easily because 60% ammonium can be accomplished easily because 60% ammonium sulfate precipitates hemoglobin but not myoglobinsulfate precipitates hemoglobin but not myoglobin . .
Hemoglobinuria classically is ascribed to paroxysmal Hemoglobinuria classically is ascribed to paroxysmal nocturnal hemoglobinuria, but it can occur with any nocturnal hemoglobinuria, but it can occur with any brisk intravascular hemolytic anemia. In the early days of brisk intravascular hemolytic anemia. In the early days of heart surgery with implantation of artificial valves, this heart surgery with implantation of artificial valves, this mechanism of producing iron deficiency anemia was mechanism of producing iron deficiency anemia was commonplace in large university hospitals. Today, with commonplace in large university hospitals. Today, with better prostheses, it has become a less frequent clinical better prostheses, it has become a less frequent clinical problem. With less severe hemolytic disorders, there may problem. With less severe hemolytic disorders, there may be no significant hemoglobinuria. Investigate renal loss be no significant hemoglobinuria. Investigate renal loss of iron by staining the urine sediment for iron. of iron by staining the urine sediment for iron. Hemosiderin is detected intracellularly. Most of these Hemosiderin is detected intracellularly. Most of these patients have a low or absent plasma haptoglobin. patients have a low or absent plasma haptoglobin. Similarly, pulmonary hemosiderosis can result in Similarly, pulmonary hemosiderosis can result in sufficient loss of iron as hemosiderin from the lungssufficient loss of iron as hemosiderin from the lungs..
Malabsorption of ironMalabsorption of iron Prolonged achlorhydria may produce iron deficiency because Prolonged achlorhydria may produce iron deficiency because acidic conditions are required to release ferric iron from acidic conditions are required to release ferric iron from food. Then, it can be chelated with mucin and other food. Then, it can be chelated with mucin and other substances (amino acids, sugars, amides) to keep it soluble substances (amino acids, sugars, amides) to keep it soluble and available for absorption in the more alkaline duodenumand available for absorption in the more alkaline duodenum . .Starch Starch and and clayclay eating produce malabsorption of iron and iron eating produce malabsorption of iron and iron deficiency anemia. Specific inquiry is required to elicit a deficiency anemia. Specific inquiry is required to elicit a history of either starch or clay eating because patients do history of either starch or clay eating because patients do not volunteer the informationnot volunteer the information . .
Extensive surgical removal of the proximal small bowel or Extensive surgical removal of the proximal small bowel or chronic diseases, such as untreated sprue or celiac disease, chronic diseases, such as untreated sprue or celiac disease, can diminish iron absorptioncan diminish iron absorption . .
Rarely, patients with no history of malabsorption have iron Rarely, patients with no history of malabsorption have iron deficiency anemia and fail to respond to oral iron therapy. deficiency anemia and fail to respond to oral iron therapy. Most merely are noncompliant with therapy. Before placing Most merely are noncompliant with therapy. Before placing these patients on parenteral therapy, document iron these patients on parenteral therapy, document iron malabsorption by either malabsorption by either measuring absorption of measuring absorption of radio-iron radio-iron or by obtaining a baseline fasting serum-iron or by obtaining a baseline fasting serum-iron concentration and repeating the test one-half hour and 1 concentration and repeating the test one-half hour and 1 hour after administration of a freshly prepared oral solution hour after administration of a freshly prepared oral solution of ferrous sulfate (50-60 mg of iron) under observation. The of ferrous sulfate (50-60 mg of iron) under observation. The serum iron should increase by 50% over the fasting serum iron should increase by 50% over the fasting specimenspecimen . .
Clinical ManifestationsClinical ManifestationsFatigue and diminished capability to perform Fatigue and diminished capability to perform hard labor are attributed to the lack of hard labor are attributed to the lack of circulating hemoglobin; however, they occur circulating hemoglobin; however, they occur out of proportion to the degree of anemia out of proportion to the degree of anemia and probably are due to a depletion of and probably are due to a depletion of proteins that require iron as a part of their proteins that require iron as a part of their structurestructure . .
Increasing evidence suggests that deficiency or Increasing evidence suggests that deficiency or dysfunction of nonhemoglobin proteins has dysfunction of nonhemoglobin proteins has deleterious effects. These include muscle deleterious effects. These include muscle dysfunction, dysfunction, pica, pica, pagophagia, dysphagia pagophagia, dysphagia with esophageal webbing (Plummer-Vinson with esophageal webbing (Plummer-Vinson Syndrome or Paterson-Kelley Syndrome), Syndrome or Paterson-Kelley Syndrome), poor scholastic performance, altered poor scholastic performance, altered resistance to infection, and altered behaviorresistance to infection, and altered behavior..
A dietary history is importantA dietary history is important . .Vegetarians Vegetarians are more likely to develop iron deficiency, unless are more likely to develop iron deficiency, unless their diet is supplemented with iron. National programs of their diet is supplemented with iron. National programs of dietary iron supplementation are initiated in many portions dietary iron supplementation are initiated in many portions of the world where meat is sparse in the diet and iron of the world where meat is sparse in the diet and iron deficiency anemia is prevalent. Unfortunately, affluent deficiency anemia is prevalent. Unfortunately, affluent nations also supplement iron in foodstuffs and vitamins nations also supplement iron in foodstuffs and vitamins without recognizing the potential contribution of iron to without recognizing the potential contribution of iron to free radical formation and the prevalence of genetic iron free radical formation and the prevalence of genetic iron overloading disordersoverloading disorders . .
Elderly patients, because of poor economic circumstances, Elderly patients, because of poor economic circumstances, may try to survive on a may try to survive on a "tea and toast""tea and toast" diet because they do diet because they do not wish to seek aid.not wish to seek aid. They may also be hesitant to shareThey may also be hesitant to share this this dietary informationdietary information . .
PicaPica can be the etiology of iron deficiency among people who can be the etiology of iron deficiency among people who habitually eat either clay or laundry starch. Hippocrates habitually eat either clay or laundry starch. Hippocrates recognized clay eating; however, physicians do not recognized clay eating; however, physicians do not recognize it unless the patient and family are specifically recognize it unless the patient and family are specifically queried. Both substances decrease the absorption of dietary queried. Both substances decrease the absorption of dietary iron. Clay eating (iron. Clay eating (GeophagiaGeophagia) occurs worldwide in all races, ) occurs worldwide in all races, though it is more common in Asia Minor. Starch eating though it is more common in Asia Minor. Starch eating ((AmylophagiaAmylophagia) is a habit in females of African heritage, and ) is a habit in females of African heritage, and it often is started in pregnancy as a treatment for morning it often is started in pregnancy as a treatment for morning sicknesssickness..
HemorrhageHemorrhage Two thirds of body iron is present in circulating red Two thirds of body iron is present in circulating red blood cells as hemoglobin. Each gram of hemoglobin blood cells as hemoglobin. Each gram of hemoglobin contains 3.47 mg of iron; thus, each mL of blood lost contains 3.47 mg of iron; thus, each mL of blood lost from the body (hemoglobin 15 g/dL) results in a loss from the body (hemoglobin 15 g/dL) results in a loss of 0.5 mg of iron. Bleeding is the most common of 0.5 mg of iron. Bleeding is the most common cause of iron deficiency in North America and cause of iron deficiency in North America and Europe. Patients report a history of bleeding from Europe. Patients report a history of bleeding from most orifices (most orifices (hematuriahematuria, , hematemesishematemesis, , hemoptysishemoptysis) ) before they develop chronic iron deficiency anemia; before they develop chronic iron deficiency anemia; however, gastrointestinal bleeding may go however, gastrointestinal bleeding may go unrecognized, and excessive menstrual losses may unrecognized, and excessive menstrual losses may be overlookedbe overlooked . .
Patients often do not understand the significance of a Patients often do not understand the significance of a melanotic stool. Unless menstrual flow changes, melanotic stool. Unless menstrual flow changes, patients do not seek medical attention. If they do, patients do not seek medical attention. If they do, they report that their menses are normal in response they report that their menses are normal in response to inquiry for self-evaluation. Because of the marked to inquiry for self-evaluation. Because of the marked differences among women with regard to menstrual differences among women with regard to menstrual blood loss (10-250 mL per menses), query the blood loss (10-250 mL per menses), query the patient about a specific history of clots, cramps, and patient about a specific history of clots, cramps, and the use of multiple tampons and padsthe use of multiple tampons and pads..
DurationDuration
Iron deficiency in the absence of anemia is Iron deficiency in the absence of anemia is asymptomaticasymptomatic. One half of patients with . One half of patients with moderate iron deficiency anemia develop moderate iron deficiency anemia develop pagophagiapagophagia. Usually, they crave ice to . Usually, they crave ice to suck or chew. Occasionally, patients are suck or chew. Occasionally, patients are seen who prefer cold celery or other cold seen who prefer cold celery or other cold vegetables in lieu of ice. vegetables in lieu of ice. Leg crampsLeg cramps, , which occur on climbing stairs, also are which occur on climbing stairs, also are common in patients deficient in ironcommon in patients deficient in iron . .
Often, patients can provide a distinct Often, patients can provide a distinct point in time when these symptoms first point in time when these symptoms first occurred, providing an estimate of the occurred, providing an estimate of the duration of the iron deficiencyduration of the iron deficiency..
SignsSignsAnemia produces nonspecific Anemia produces nonspecific pallor pallor of the of the mucous membranesmucous membranes . .
A number of abnormalities of epithelial tissues A number of abnormalities of epithelial tissues are described in association with iron deficiency are described in association with iron deficiency anemiaanemia . .
These include These include esophageal webbingesophageal webbing, , koilonychiakoilonychia, , glossitisglossitis, , angular stomatitisangular stomatitis, and , and gastric atrophygastric atrophy . .
The exact relationship of these findings to iron The exact relationship of these findings to iron deficiency is unclear and may involve other factors. deficiency is unclear and may involve other factors. For example, in publications from the United For example, in publications from the United Kingdom, esophageal webbing and Kingdom, esophageal webbing and atrophic changes atrophic changes of the tongueof the tongue and and the corner of the mouththe corner of the mouth are are reported in as many as 15% of patients with iron reported in as many as 15% of patients with iron deficiency; however, they are much less common in deficiency; however, they are much less common in the United States and other portions of the worldthe United States and other portions of the world..
SplenomegalySplenomegaly may occur with severe, persistent, may occur with severe, persistent, untreated iron deficiency anemia. This is untreated iron deficiency anemia. This is uncommon in the United States and Europeuncommon in the United States and Europe..
Differential DiagnosesDifferential Diagnoses Spherocytosis, HereditarySpherocytosis, HereditaryThalassemia, AlphaThalassemia, AlphaThalassemia, BetaThalassemia, Beta
Anemia of chronic disordersHemoglobin CC diseaseLead poisoningMicrocytic anemiasSideroblastic anemias
DXDXLabLab:.:.CBC countCBC count This documents the severity of the anemia. In chronic This documents the severity of the anemia. In chronic iron deficiency anemia, the cellular indices show a iron deficiency anemia, the cellular indices show a microcyticmicrocytic and and hypochromichypochromic erythropoiesis, i.e., both erythropoiesis, i.e., both the mean corpuscular volume (MCV) and mean the mean corpuscular volume (MCV) and mean corpuscular hemoglobin concentration (MCHC) have corpuscular hemoglobin concentration (MCHC) have values below the normal range for the laboratory values below the normal range for the laboratory performing the test. (Reference range values for the performing the test. (Reference range values for the MCV and MCHC are 83-97 fL and 32-36 g/dL, MCV and MCHC are 83-97 fL and 32-36 g/dL, respectively)respectively) . .
Often, the platelet count is elevated (>450,000/Often, the platelet count is elevated (>450,000/µµL). This L). This normalizes following iron therapynormalizes following iron therapy . .
The WBC count is usually within reference ranges The WBC count is usually within reference ranges (4500-11,000/(4500-11,000/µµL)L) . .
If the CBC count is obtained after blood loss, the If the CBC count is obtained after blood loss, the cellular indices do not enter the abnormal range until cellular indices do not enter the abnormal range until most of the erythrocytes produced before the bleed most of the erythrocytes produced before the bleed are destroyed at the end of their normal lifespan (120 are destroyed at the end of their normal lifespan (120 d)d)..
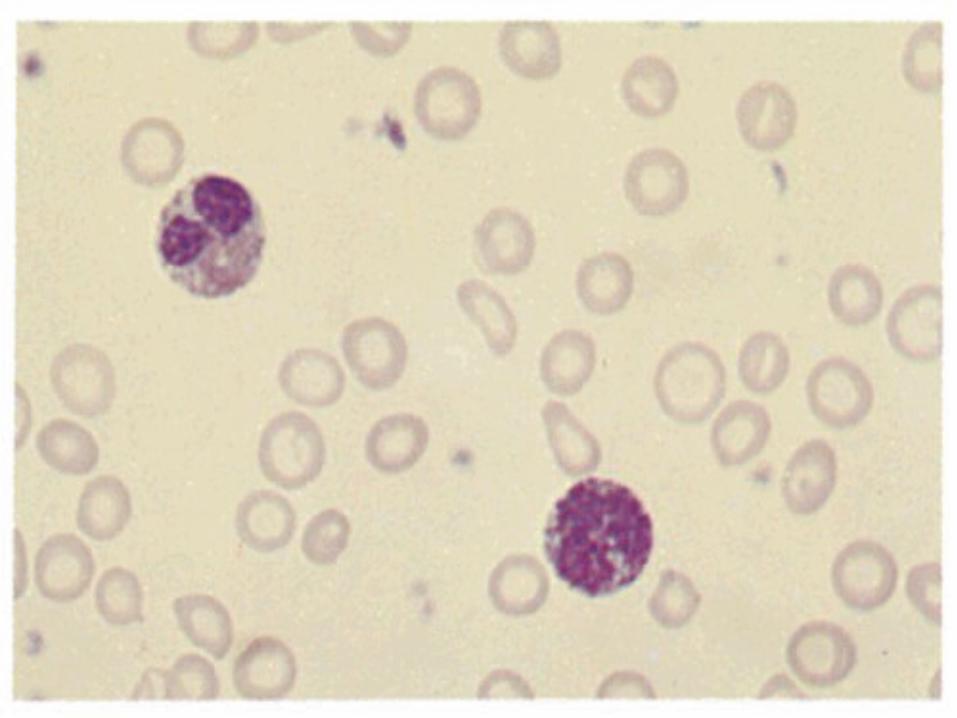
Peripheral smearPeripheral smear Examination of the peripheral smear is an important part of Examination of the peripheral smear is an important part of the workup of patients with anemia. Examination of the the workup of patients with anemia. Examination of the erythrocytes shows erythrocytes shows microcyticmicrocytic and and hypochromichypochromic red red blood cells in chronic iron deficiency anemia. The blood cells in chronic iron deficiency anemia. The microcytosis is apparent in the smear long before the MCV microcytosis is apparent in the smear long before the MCV is decreased after an event producing iron deficiency. is decreased after an event producing iron deficiency. Platelets usually are increased in this disorderPlatelets usually are increased in this disorder . .
Unlike thalassemia, target cells usually are not present, and Unlike thalassemia, target cells usually are not present, and anisocytosis and poikilocytosis are not marked. It lacks the anisocytosis and poikilocytosis are not marked. It lacks the intraerythrocytic crystals seen in hemoglobin C disordersintraerythrocytic crystals seen in hemoglobin C disorders . .
Combined folate deficiency and iron deficiency are Combined folate deficiency and iron deficiency are commonplace in areas of the world with little fresh produce commonplace in areas of the world with little fresh produce and meat. The peripheral smear reveals a population of and meat. The peripheral smear reveals a population of macrocytes mixed among the microcytic hypochromic cells. macrocytes mixed among the microcytic hypochromic cells. This combination can normalize the MCVThis combination can normalize the MCV
Serum iron, total iron-binding capacity (TIBC), and serum Serum iron, total iron-binding capacity (TIBC), and serum ferritinferritin: A low serum iron and ferritin with an elevated TIBC : A low serum iron and ferritin with an elevated TIBC are are diagnosticdiagnostic of iron deficiency. While a low serum ferritin of iron deficiency. While a low serum ferritin is virtually diagnostic of iron deficiency, a normal serum is virtually diagnostic of iron deficiency, a normal serum ferritin can be seen in patients who are deficient in iron and ferritin can be seen in patients who are deficient in iron and have coexistent diseases (hepatitis, anemia of chronic have coexistent diseases (hepatitis, anemia of chronic disorders). These test findings are useful in distinguishing disorders). These test findings are useful in distinguishing iron deficiency anemia from other microcytic anemiasiron deficiency anemia from other microcytic anemias..
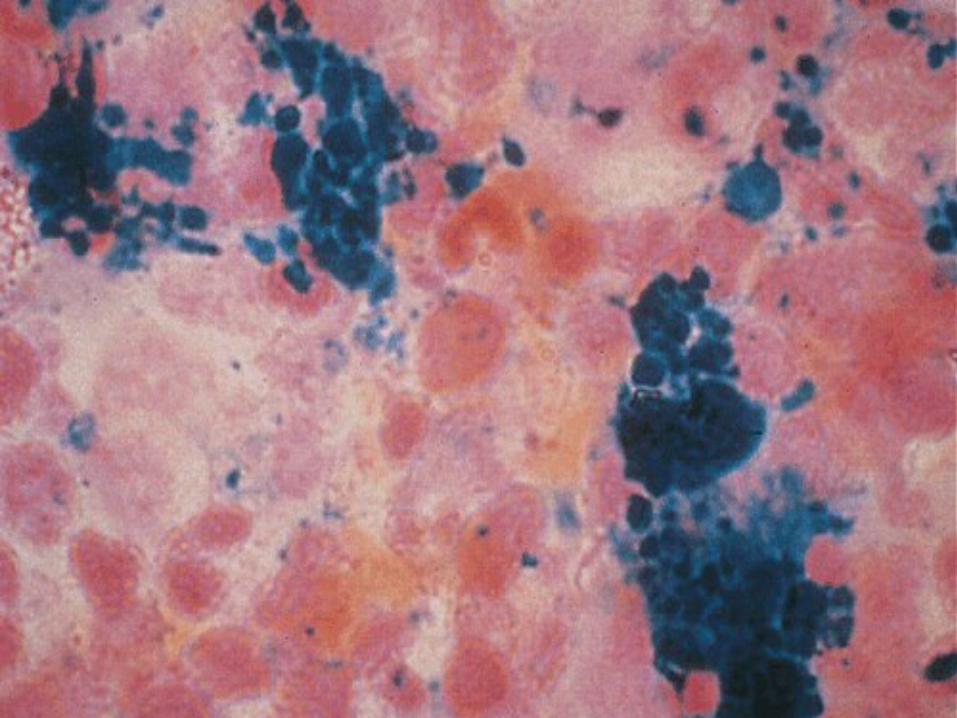
A A bone marrow aspiratebone marrow aspirate can be diagnostic of iron deficiency. can be diagnostic of iron deficiency. The absence of stainable iron in a bone marrow aspirate The absence of stainable iron in a bone marrow aspirate that contains spicules and a simultaneous control specimen that contains spicules and a simultaneous control specimen containing stainable iron permit establishment of a containing stainable iron permit establishment of a diagnosis of iron deficiency without other laboratory testsdiagnosis of iron deficiency without other laboratory tests . .
Other laboratory tests are useful to establish the etiology of Other laboratory tests are useful to establish the etiology of iron deficiency anemia and to exclude or establish a iron deficiency anemia and to exclude or establish a diagnosis of 1 of the other microcytic anemiasdiagnosis of 1 of the other microcytic anemias . .
Testing stool for the presence of hemoglobinTesting stool for the presence of hemoglobin is useful in is useful in establishing gastrointestinal bleeding as the etiology of establishing gastrointestinal bleeding as the etiology of iron deficiency anemia. Usually, chemical testing that iron deficiency anemia. Usually, chemical testing that detects more than 20 mL of blood loss daily from the upper detects more than 20 mL of blood loss daily from the upper gastrointestinal tract is employed. More sensitive tests are gastrointestinal tract is employed. More sensitive tests are available; however, they produce a high incidence of false-available; however, they produce a high incidence of false-positive results in people who eat meat. Severe iron positive results in people who eat meat. Severe iron deficiency anemia can occur in patients with a persistent deficiency anemia can occur in patients with a persistent loss of less than 20 mL/dloss of less than 20 mL/d . .
To detect blood loss, the patient can be placed on a strict To detect blood loss, the patient can be placed on a strict vegetarian diet for 3-5 days and the stool can be tested for vegetarian diet for 3-5 days and the stool can be tested for hemoglobin using a benzidine method, or red blood cells hemoglobin using a benzidine method, or red blood cells can be radiolabeled with radiochromium and retransfused. can be radiolabeled with radiochromium and retransfused. Stools are collected, and the radioactivity is quantified in a Stools are collected, and the radioactivity is quantified in a gamma-detector and compared to the radioactivity in a gamma-detector and compared to the radioactivity in a measured quantity of the patient's blood. An immunological measured quantity of the patient's blood. An immunological method of detecting human species-specific hemoglobin in method of detecting human species-specific hemoglobin in stool is under development and could increase specificity stool is under development and could increase specificity and sensitivityand sensitivity..
HemoglobinuriaHemoglobinuria and and hemosiderinuriahemosiderinuria can can be detected by laboratory testing as be detected by laboratory testing as described under Causes. This documents described under Causes. This documents iron deficiency to be due to renal loss of iron deficiency to be due to renal loss of iron and incriminates intravascular iron and incriminates intravascular hemolysis as the etiologyhemolysis as the etiology . .
Hemoglobin electrophoresisHemoglobin electrophoresis and and measurement of hemoglobin A2 and fetal measurement of hemoglobin A2 and fetal hemoglobin are useful in establishing hemoglobin are useful in establishing either beta-thalassemia or hemoglobin C either beta-thalassemia or hemoglobin C or D as the etiology of the microcytic or D as the etiology of the microcytic anemiaanemia . .
Unfortunately, simple tests do not exist for Unfortunately, simple tests do not exist for alpha-thalassemia in most laboratories, alpha-thalassemia in most laboratories, and it is a diagnosis of exclusionand it is a diagnosis of exclusion . .
Other TestsOther Tests
Incubated Incubated osmotic fragilityosmotic fragility is useful. is useful. Microspherocytosis may produce a low-normal Microspherocytosis may produce a low-normal or slightly abnormal MCV; however, the MCHC or slightly abnormal MCV; however, the MCHC usually is elevated rather than decreased, and usually is elevated rather than decreased, and the peripheral smear shows a lack of central the peripheral smear shows a lack of central pallor rather than hypochromiapallor rather than hypochromia . .
Measure Measure tissue lead concentrationstissue lead concentrations. Chronic . Chronic lead poisoning may produce a mild lead poisoning may produce a mild microcytosis. The anemia probably is related to microcytosis. The anemia probably is related to the anemia of chronic disorders. The incidence the anemia of chronic disorders. The incidence of lead poisoning is greater in individuals who of lead poisoning is greater in individuals who are iron deficient than in healthy subjects are iron deficient than in healthy subjects because increased absorption of lead occurs in because increased absorption of lead occurs in individuals who are iron deficient. Paint in old individuals who are iron deficient. Paint in old houses has been a source of lead poisoning in houses has been a source of lead poisoning in children and painterschildren and painters..
A A bone marrow aspiratebone marrow aspirate stained for iron ( stained for iron (PerlsPerls or or Prussian blue stainPrussian blue stain) can be diagnostic of iron ) can be diagnostic of iron deficiency provided spicules are present in the smear deficiency provided spicules are present in the smear and a control specimen containing iron is performed at and a control specimen containing iron is performed at the same time. While this largely has been displaced in the same time. While this largely has been displaced in the diagnosis of iron deficiency by performance of the diagnosis of iron deficiency by performance of serum iron, TIBC, and serum ferritin, the absence of serum iron, TIBC, and serum ferritin, the absence of stainable iron in a bone marrow aspirate is the stainable iron in a bone marrow aspirate is the criterion standard for the diagnosis of iron deficiency. criterion standard for the diagnosis of iron deficiency. It is diagnostic in identifying the sideroblastic anemias It is diagnostic in identifying the sideroblastic anemias by showing ringed sideroblasts in the aspirate stained by showing ringed sideroblasts in the aspirate stained with Perls stain. Occasionally, it is useful in separating with Perls stain. Occasionally, it is useful in separating patients with the anemia of chronic disorders or alpha-patients with the anemia of chronic disorders or alpha-thalassemia from patients with iron deficiency, and it is thalassemia from patients with iron deficiency, and it is useful in identifying patients with both iron deficiency useful in identifying patients with both iron deficiency and the anemia of chronic disordersand the anemia of chronic disorders..Histologic FindingsHistologic FindingsThe The absence of stainable ironabsence of stainable iron in body tissues, including in body tissues, including the bone marrow and liver, is the most useful the bone marrow and liver, is the most useful histological finding in individuals who are iron histological finding in individuals who are iron deficient. Nonspecific abnormalities of epithelial deficient. Nonspecific abnormalities of epithelial tissues are reported in iron deficiency. These include tissues are reported in iron deficiency. These include gastric atrophygastric atrophy and and clubbing of the small intestinal clubbing of the small intestinal villivilli. While they suggest that iron deficiency is a . While they suggest that iron deficiency is a pantropic disorder, they have little clinical diagnostic pantropic disorder, they have little clinical diagnostic valuevalue..
TreatmentTreatmentThe most economical and effective medication in the The most economical and effective medication in the treatment of iron deficiency anemia is the treatment of iron deficiency anemia is the oral oral administration of ferrous ironadministration of ferrous iron salts. Among the various salts. Among the various iron salts, iron salts, ferrous sulfateferrous sulfate most commonly is used. most commonly is used. Claims are made that other iron salts are absorbed Claims are made that other iron salts are absorbed better and have less morbidity. Generally, the toxicity is better and have less morbidity. Generally, the toxicity is proportional to the amount of iron available for proportional to the amount of iron available for absorption. If the quantity of iron in the test dose is absorption. If the quantity of iron in the test dose is decreased, the percentage of the test dose absorbed is decreased, the percentage of the test dose absorbed is increased, but the quantity of iron absorbed is increased, but the quantity of iron absorbed is diminished. There are advocates for the use of carbonyl diminished. There are advocates for the use of carbonyl iron because of the greater safety with children who iron because of the greater safety with children who ingest their mothers' medication. Decreased gastric ingest their mothers' medication. Decreased gastric toxicity is claimed but not clearly demonstrated in toxicity is claimed but not clearly demonstrated in human trials. Bioavailability is approximately 70% of a human trials. Bioavailability is approximately 70% of a similar dose of ferrous sulfatesimilar dose of ferrous sulfate . .
Reserve Reserve parenteral ironparenteral iron for patients who are either unable for patients who are either unable to absorb oral iron or who have increasing anemia to absorb oral iron or who have increasing anemia despite adequate doses of oral iron. It is expensive and despite adequate doses of oral iron. It is expensive and has greater morbidity than oral preparations of ironhas greater morbidity than oral preparations of iron..Reserve Reserve transfusion of packed RBCtransfusion of packed RBC for patients with for patients with either significant acute bleeding or patients in danger either significant acute bleeding or patients in danger of hypoxia and/or coronary insufficiencyof hypoxia and/or coronary insufficiency..
Ferrous sulfateFerrous sulfate
325325 mg (60 mg iron) PO with each meal tidmg (60 mg iron) PO with each meal tid
Calcium supplementation decreases Calcium supplementation decreases bioavailability of iron when metals are bioavailability of iron when metals are ingested simultaneously; absorption is ingested simultaneously; absorption is enhanced by ascorbic acid; interferes enhanced by ascorbic acid; interferes with tetracycline absorption; food and with tetracycline absorption; food and antacids impair absorptionantacids impair absorption
Dextran-ironDextran-iron Replenishes depleted iron stores in the Replenishes depleted iron stores in the bone marrow where it is incorporated into bone marrow where it is incorporated into hemoglobin. Parenteral use of iron-hemoglobin. Parenteral use of iron-carbohydrate complexes has caused carbohydrate complexes has caused anaphylactic reactions, and its use should anaphylactic reactions, and its use should be restricted to patients with an be restricted to patients with an established diagnosis of iron deficiency established diagnosis of iron deficiency anemiaanemia whose whose anemia is not corrected anemia is not corrected with oral therapywith oral therapy. Required dose can be . Required dose can be calculated (3.5 mg iron/g of hemoglobin) calculated (3.5 mg iron/g of hemoglobin) or obtained from tables in the textsor obtained from tables in the texts . .
For IV use, may be diluted in 0.9% sterile For IV use, may be diluted in 0.9% sterile saline. Do not add to solutions containing saline. Do not add to solutions containing medications or parenteral nutrition medications or parenteral nutrition solutionssolutions..