Embed Size (px)
Citation preview

PATHOPHYSIOLOGY AND NATURAL HISTORYCONGENITAL HEART DISEASE
Is the aorta truly dextroposed in tetralogy of Fallot?A two-dimensional echocardiographic answer
KARLISAAZ, M.D., JEAN L. CLOEZ, M.D., FRANCOIS MARWON, M.D., ANNE M. WORMS, M.D.,AND CLAUDE PERNOT, M.D.
ABSTRACT The embryogenesis of tetralogy of Fallot is still much debated. In particular, thedextroposition of the aorta is not considered by all pathologists as a genuine abnormality in thiscongenital heart disease but rather as a false impression due to an exaggeration of the normal overridingcaused by dilatation of the aorta secondary to abnormal hemodynamics. We used two-dimensionalechocardiography to examine the spatial position of the aortic root in 22 patients with tetralogy of Fallot(aged 5 days to 24 years, mean 6.4 years) and in 23 normal subjects (aged 1 month to 27 years, mean7.6 years). Using the parasternal short-axis view, we determined the percent rightward displacement ofthe aortic root in relation to the plane of the atrial septum, and the relationship between the aortic cuspsand the atrial septum. We measured the value of the angle 0, which was defined as the angle betweenthe plane of the atrial septum and the plane of the left coronary-noncoronary commissure and leafletappositional plane. In the control group, the aortic root was displaced to the right by only 23.6 + 7.6%;the atrial septum crossed the posterior aspect of the aortic root at the middle (n = 19) or at the right halfof the posterior cusp (n = 4), and the angle 0 had a value of 43.3 + 8.8 degrees. In the 22 patients withtetralogy, the percent rightward shift of the aortic root was augmented to 55.5 + 9% (p < .001) and theatrial septum was related to the posterior commissure in 14 patients, to the left coronary cusp in twopatients, and to the left fourth of the posterior cusp in six patients; the angle 0 had a value of 9.2 11.2degrees (p < .001). In the two groups, the position of the commissure between the right coronary andleft coronary aortic cusps was similar in relation to a line passed forward from the atrial septum. Weconclude that the aorta is truly dextroposed in tetralogy of Fallot, with a rightward shift due to aclockwise rotation of the aortic root (looking downstream), and that the axis of this rotation is theanterior aortic commissure. Our echocardiographic findings, which confirm conclusions of previousinvestigators based on pathologic anatomy, support the embryologic hypothesis of the lack of conalrotation in tetralogy of Fallot and permit a quantitation of the effects of this morphogenetic mechanism.Circulation 73, No. 5, 892-899, 1986.
IN THE PAST, the terms "dextroposition" and "over-riding" have been used interchangeably. However,overriding of the aorta should not be confused withdextroposition. Overriding of the aorta over the rightventricle occurs in the normal heart because of thesigmoid interventricular septum' as well as in heartswith isolated infundibular perimembranous ventricularseptal defect2' 3 and can be considered a normal ana-tomic feature.4 The term dextroposition indicates apathologic condition with a rightward displacement ofthe aortic root.4' There has been considerable debateconcerning whether a true dextroposition of the aortaexists in tetralogy of Fallot. Some investigators6' have
From the Department of Pediatric Cardiology, University of Nancy,Vandoeuvre-les-Nancy, France.
Address for correspondence: Karl Isaaz, M.D., Service de Cardiolo-gie Pediatrique, H6pital d'enfants, CHU Brabois, 54500 Van-dceuvre-les-Nancy, France.
Received Aug. 13, 1985; revision accepted Jan. 23, 1986.
892
suggested that in tetralogy there is only an exaggera-tion of the normal overriding aorta caused by dilatationof this vessel secondary to increased aortic flow andsimulating a dextroposition. Other authors4 5 8-11 havesuggested that the condition is typified by a true dex-troposition of the aorta with a rightward displacementand a clockwise rotation of the aortic root, particularlyin cases with severe infundibular obstruction.8
Two-dimensional echocardiography has been usedto show the ov'erriding aorta over the right ventricle inpatients with tetralogy of Fallot,'2-1 but no criteriahave been proposed to differentiate a simple exag-geration of the normal overriding from a true dextropo-sition.
In view of this uncertainty regarding one importantanatomic feature of tetralogy of Fallot, we used two-dimensional echocardiography to examine 22 patientswith tetralogy of Fallot, recording geometric measure-
CIRCULATION
by guest on May 30, 2018
http://circ.ahajournals.org/D
ownloaded from
PATHOPHYSIOLOGY AND NATURAL HISTORY-CONGENITAL HEART DISEASE
ments, and compared our results with similar measure-ments recorded in a control group of 23 normal sub-jects. The purpose of this study was to answer thequestions: is the aorta truly dextroposed in tetralogy ofFallot? If this is the case, what is the mechanism of thedextroposition? Our objective was to provide echocar-diographic arguments for or against one of the pro-posed embryologic hypothesis, the lack of conal rota-tion.
Materials and methodsClinical population. We studied 49 patients prospectively
by two-dimensional echocardiography, using the parasternalshort-axis plane at aortic valve level. Complete examination ofthe aortic root with the three aortic cusps and atrial septum waspossible in 45 (92%). Four patients were excluded because ofincomplete results. Twenty-two patients had tetralogy of Fallotand ranged in age from 5 days to 24 years (mean 6.4 years);there were 13 male and nine female patients. Sixteen (72%)patients had undergone previous surgery, 11 corrective and fivepalliative operations.The results were compared with those recorded in 23 patients
without heart disease, aged from 1 month to 27 years (mean 7.6years), including 13 male and 10 female patients. Examinationswere performed with Advanced Technology Laboratoriesequipment and 3.0 and 5.0 MHz frequency transducers.
Imaging technique. Patients were examined while in a su-pine position with the transducer placed at the left sternal borderor at the subclavicular region. The transducer was manuallyrotated to obtain a parasternal short-axis view of the aortic valvelevel'617 and slight adjustments in transducer angulation wererequired to provide simultaneously a good visualization of theaortic root with the three aortic cusps, the atrial septum, and thepulmonary valve. Still frames were converted to hard copy.
Geometric measurements and calculations. Figures I and2 show schematically the measurements and calculations werecorded in each patient. A circle circumscribing the inner sideof the aortic root was constructed, as shown in figure 1, and thepercent of its rightward displacement (d/a) in relation to the lineCD passed forward from the atrial septum was recorded (figure2). Because of the variable curvature of the middle part of theatrial septum, we took only the anterior and posterior insertionsof this septal structure into consideration to construct the lineCD. We completed the analysis of the relationships of the aorticroot with the adjacent structures (atrial septum and pulmonaryvalve) by determining: (I) the point of intersection (r) betweenthe line CD and the rim of the aortic root, and the aortic cusprelated to this point, (2) the point of intersection (o) between thepulmonary valve and the anterior aspect of the aortic root, andthe aortic cusp related to this point. To assess the mechanism ofthe hypothetical dextroposition, we constructed the followinglines (figure 2): (1) through the commissure between the leftcoronary and the noncoronary cusps (XY), (2) between theanterior aortic commissure on the inner border of the aortic rootand the posterior insertion of the atrial septum (ZD), (3) be-tween the anterior aortic commissure on the inner border of theaonic root, and the center of the circle circumscribing the inneredge of the aortic root (ZW).
These various lines defined the following angles: (l) angle 0,subtended by the lines CD and XY; this angle was conventional-ly considered as positive when the line XY was at the left of theline CD and negative when it was at the right; (2) angle ¢,subtended by CD and ZD; (3) angle p defined by CD and ZW.Funhermore, we assessed the degree of left inclination of the
atrial septum by measurement of the angle c, which was definedby the line CD and the line AB, which was drawn through theposterior wall of the atria along the first 10 mm on each side ofthe atrial septum (figure 1). The measurement of the angle s wasnecessary to interpret the results concerning the other angles (0,4, and p), which had the line CD as a common side.
Data analysis. All measurements and calculations were doneby one examiner and repeated by another observer who wasblinded to the findings of the first observer and whose determi-nations never differed from the first observer's by more than5%.
Statistical analysis. The data used for each of the compari-sons between the two groups were subsequently submitted tostatistical analysis with Student's t test and a confidence level of0.5%.
Results
The recorded measurements and calculations are in~dicated in table 1 for the patients with tetralogy ofFallot and in table 2 for the subjects in the con-
pv
A
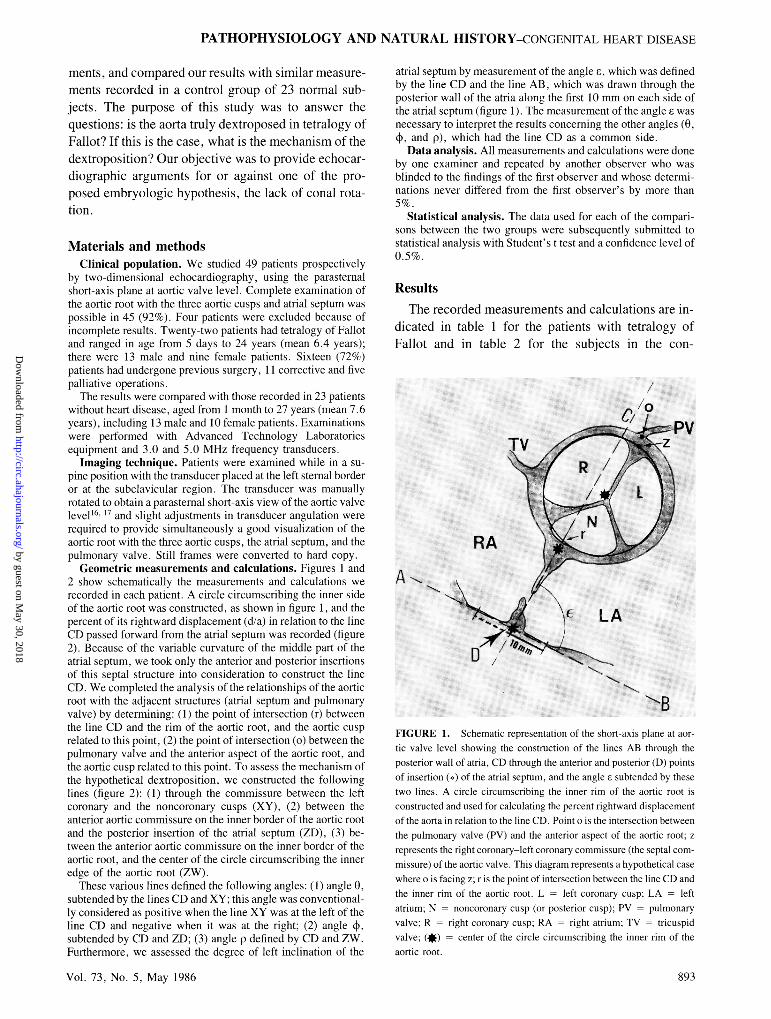
FIGURE 1. Schematic representation of the short-axis plane at aor-
tic valve level showing the construction of the lines AB through theposterior wall of atria, CD through the anterior and posterior (D) pointsof insertion (e) of the atrial septum, and the angle a subtended by thesetwo lines. A circle circumscribing the inner rim of the aortic root isconstructed and used for calculating the percent rightward displacementof the aorta in relation to the line CD. Point o is the intersection betweenthe pulmonary valve (PV) and the anterior aspect of the aortic root; z
represents the right coronary-left coronary commissure (the septal commissure) of the aortic valve. This diagram represents a hypothetical case
where o is facing z; r is the point of intersection between the line CD andthe inner rim of the aortic root. L -left coronary cusp; LA = leftatrium; N noncoronary cusp (or posterior cusp); PV = pulmonaryvalve; R right coronary cusp; RA = right atrium; TV tricuspidvalve: (*) center of the circle circumscribing the inner rim of theaortic root.
Vol. 73, No. 5, May 1986
11...B
893
by guest on May 30, 2018
http://circ.ahajournals.org/D
ownloaded from
ISAAZ et al.
i, a
II
TV c
LCL
in
RVOCl
i
Cl
RA
trol group. The statistical comparisons are shown intable 3.
These measurements showed that the angle £ of theinteratrial septum was identical in patients with tetral-ogy of Fallot and normal subjects (87 vs 86 degrees,NS). This finding permitted us to take the line CD ofatrial septum as a reference for other measurements. Inpatients with tetralogy, the percent rightward displace-ment (d/a) of the aortic root in relation to the plane(CD) of the atrial septum averaged 55.5% (range 44%to 80%), which was significantly greater than the aver-age value for the normal subjects 23.6% (range 7% to39%; p < .001). In patients with tetralogy, the atrialseptum crossed the posterior aspect of the aortic root(point r) at the level of the left fourth of the noncoro-nary cusp in six of the 22 patients, at the right third ofthe left coronary cusp in two patients, and at the com-missure between these two cusps in 14 patients. In thecontrol group, point r was located at the middle of thenoncoronary cusp in 19 patients and at the right half ofthis cusp in four patients. The value of the angle 0 was
894
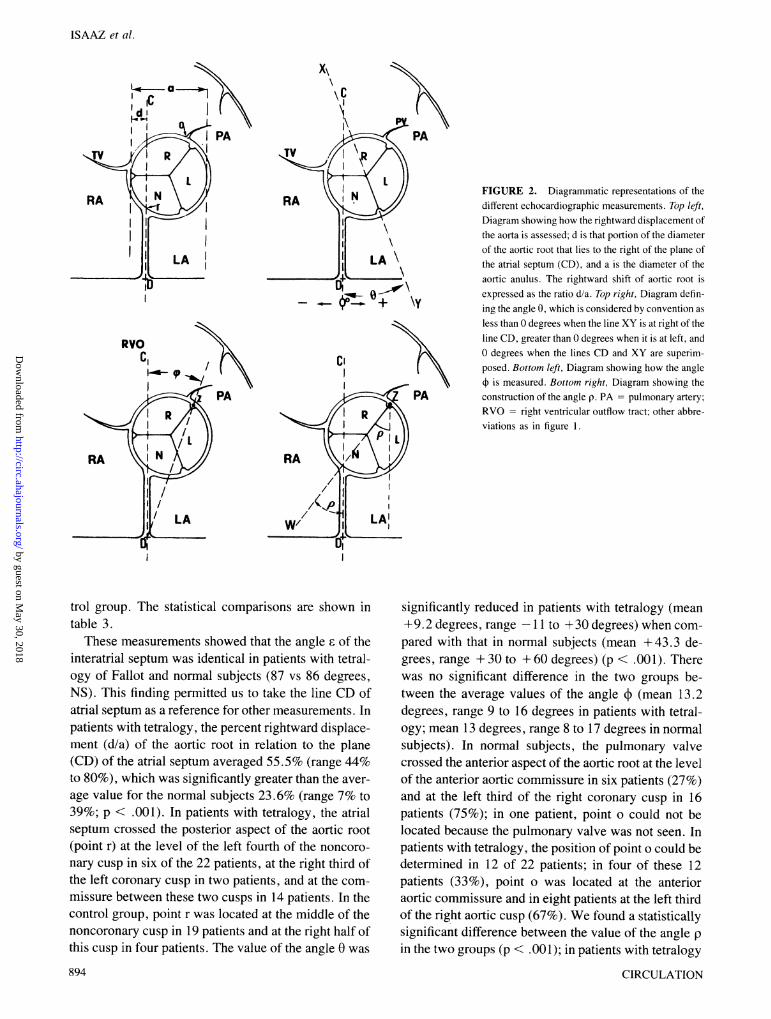
/1 FIGURE 2. Diagrammatic representations of thedifferent echocardiographic measurements. Top left,Diagram showing how the rightward displacement ofthe aorta is assessed; d is that portion of the diameterof the aortic root that lies to the right of the plane ofthe atrial septum (CD), and a is the diameter of the
-' aortic anulus. The rightward shift of aortic root isexpressed as the ratio d/a. Top right, Diagram defin-ing the angle 0, which is considered by convention asless than 0 degrees when the line XY is at right of theline CD, greater than 0 degrees when it is at left, andO degrees when the lines CD and XY are superim-posed. Bottom left, Diagram showing how the angle
001- + is measured. Bottom right, Diagram showing thePA construction of the angle p. PA = pulmonary artery;
RVO = right ventricular outflow tract; other abbre-viations as in figure 1.
significantly reduced in patients with tetralogy (mean+ 9.2 degrees, range - 1 1 to + 30 degrees) when com-pared with that in normal subjects (mean +43.3 de-grees, range +30 to + 60 degrees) (p < .00 1). Therewas no significant difference in the two groups be-tween the average values of the angle 4 (mean 13.2degrees, range 9 to 16 degrees in patients with tetral-ogy; mean 13 degrees, range 8 to 17 degrees in normalsubjects). In normal subjects, the pulmonary valvecrossed the anterior aspect of the aortic root at the levelof the anterior aortic commissure in six patients (27%)and at the left third of the right coronary cusp in 16patients (75%); in one patient, point o could not belocated because the pulmonary valve was not seen. Inpatients with tetralogy, the position of point o could bedetermined in 12 of 22 patients; in four of these 12patients (33%), point o was located at the anterioraortic commissure and in eight patients at the left thirdof the right aortic cusp (67%). We found a statisticallysignificant difference between the value of the angle pin the two groups (p < .001); in patients with tetralogy
CIRCULATION
by guest on May 30, 2018
http://circ.ahajournals.org/D
ownloaded from

PATHOPHYSIOLOGY AND NATURAL HISTORY-CONGENITAL HEART DISEASE
TABLE 1Clinical data and echocardiographic measurements in patients with tetralogy of Fallot
Patient d/aNo. Sex Age Management E (%) r 0 o0 p
1 M 2 mo Medical 98 54 Post. com. 0 Ant. com. 10 452 M 7 mo Medical 98 50 Post. com. 0 L 1/3 RCC 13 753 F 9 yr Cor. surg. 88 80 Post. com. +-30 R 2/3-L '/3 RCC 15 484 M 14 yr Cor. surg. 94 48 L ¼/4 NCC +20 Ant. com. 15 555 F 4 yr Cor. surg. 90 53 Post. com. 0 15 766 F 13 yr Cor. surg. 87 65 Post. com. 0 15 607 M 6 yr Cor. surg. 77 72 R '/3 LCC -11 16 808 F 4 yr Pal. surg. 89 50 L ¼/4 NCC +24 14 539 M 8 yr Cor. surg. 88 50 Post. com. + 11 R 2/3-L ½/3 RCC 11 4710 M 5 yr Pal. surg. 84 50 Post. com. 0 15 6511 F 9 mo Medical 80 50 Post. com. + 10 15 7012 M 1 yr Medical 80 60 Post. com. 0 15 6013 F 5 yr Cor. surg. 90 44 L l/4 NCC +28 13 4714 M 4 yr Pal. surg. 82 70 Post. com. +20 9 5615 M 4 yr Medical 83 54 L ¼/4 NCC +25 R 2/3-L l/3 RCC 11 4716 M 2 yr Pal. surg. 93 55 Post. com. 0 Ant. com. 13 5517 F 24 yr Cor. surg. 85 50 L l/4 NCC + 18 R 2/3-L ½13 RCC 13 5518 M 18 yr Cor. surg. 90 50 Post. com. 0 R 2/3-L '/3 RCC 16 7019 M 1 yr Pal. surg. 84 54 Post. com. + 10 11 7220 F 5 yr Cor. surg. 89 50 L ¼/4 NCC +26 R 2/3-L /3 RCC 13 4521 F 13 yr Cor. surg. 73 50 Post. com. 0 R 2/3-L '/3 RCC 13 5322 M 5 days Medical 78 63 R '/3 LCC -9 Ant. com. 11 70
Angles £, 0, 4, and p expressed in degrees.Ant. com. = anterior commissure (between right and left coronary cusps); Cor. surg. corrective surgery; L = left; LCC
left coronary cusp; NCC = noncoronary cusp; Pal. surg. = palliative surgery; Post. com. = posterior commissure (between leftcoronary and noncoronary cusps); R = right; RCC = right coronary cusp; R 2/3-L /3 RCC = junction of the right two-thirds withthe left third of the right coronary cusp.
of Fallot, the mean value of arngle p was 59.2 degrees(range 45 to 80 degrees), whereas in normal subjects itwas 23.4 degrees (range 10 to 39 degrees).
Figure 3 shows an example of tetralogy of Fallotwith the various measurements and calculations re-corded in this case. In figure 4 are shown the datarecorded in a control subject.
DiscussionThe echocardiographic criteria of true dextroposi-
tion have not been envisaged as yet. In this report, weattempted to clarify this point using two-dimensionalechocardiography to assess the spatial position of theaortic root in 22 patients with tetralogy of Fallot com-pared with 23 control subjects.
The values of percent rightward displacement (d/a)of the aortic root and especially the position of thecrossing-point (r) in relation to the aortic cusps showthat the aorta is abnormally displaced to the right inrelation to the atrial septum in tetralogy of Fallot whencompared with normal subjects. The change in therelationships between the atrial septum and the aorticroot determined by the position of point r confirms the
Vol. 73, No. 5, May 1986
real rightward displacement of the aorta in patientswith tetralogy of Fallot but does not indicate the re-sponsible mechanism. Indeed, the aortic root can bedisplaced to the right (dextroposed) as a result of threepossible mechanisms (figure 5): (1) rightward transla-tion, which we can speculate to be secondary to thelack of left migration of the conus from an embryolo-gic point of view, (2) clockwise rotation (lookingdownstream) about an eccentric axis, which we cansuppose to be secondary to the lack of conal rotation,or (3) a combination of both mechanisms. The constantposition of point z (anterior aortic commissure), asassessed by the identical value of angle ¢ in patientswith tetralogy and in normal subjects, excludes thepossibility of a rightward shift of the aorta by a transla-tion; should the aorta be rightward translated with orwithout additional rotation, then the angle ¢ would bediminished and the point z displaced to the right (figure5). The significant diminution of the angle 0 in patientswith tetralogy proves the clockwise rotation of theaortic root. The pivot of the rotation is the anterioraortic commissure as shown by the absence of differ-ence between the value of angle + in the two groups
895
by guest on May 30, 2018
http://circ.ahajournals.org/D
ownloaded from
ISAAZ et al.
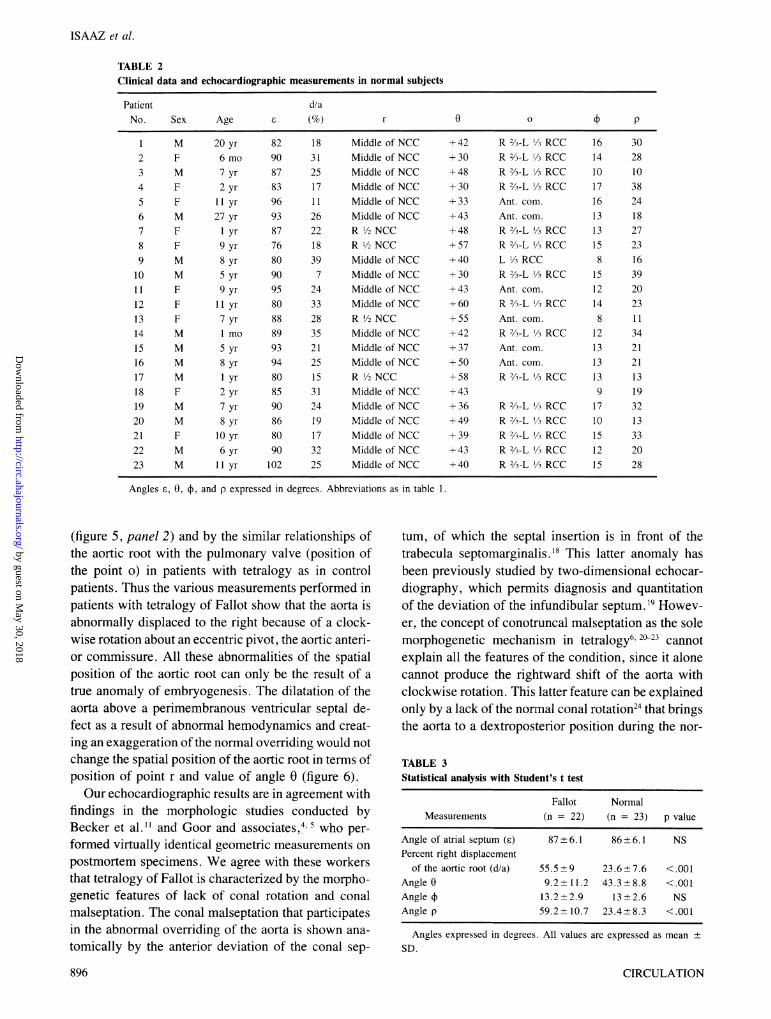
TABLE 2Clinical data and echocardiographic measurements in normal subjects
Patient d/aNo. Sex Age E (%) r 0 o0 p
1 M 20 yr 82 18 Middle of NCC +42 R 2/3-L 1/3 RCC 16 302 F 6 mo 90 31 Middle of NCC +30 R 2/3-L 1/3 RCC 14 283 M 7 yr 87 25 Middle of NCC +48 R 2/3-L 1/3 RCC 10 104 F 2 yr 83 17 Middle of NCC +30 R 2/3-L /3 RCC 17 385 F 11 yr 96 11 Middle of NCC +33 Ant. com. 16 246 M 27 yr 93 26 Middle of NCC +43 Ant. com. 13 187 F 1 yr 87 22 R ½/2 NCC +48 R 2/3-L '/A RCC 13 278 F 9 yr 76 18 R 1/2 NCC +57 R 2/3-LL/3 RCC 15 239 M 8 yr 80 39 Middle of NCC +40 L 13 RCC 8 1610 M 5 yr 90 7 Middle of NCC +30 R 2/3-L1-3 RCC 15 3911 F 9 yr 95 24 Middle of NCC +43 Ant. com. 12 2012 F 11 yr 80 33 Middle of NCC +60 R 2/3-L 1/3 RCC 14 2313 F 7 yr 88 28 R ½/2 NCC +55 Ant. com. 8 1114 M 1 mo 89 35 Middle of NCC +42 R 2/3-L /3 RCC 12 3415 M 5 yr 93 21 Middle of NCC +37 Ant. com. 13 2116 M 8 yr 94 25 Middle of NCC +50 Ant. com. 13 2117 M 1 yr 80 15 R ½/2 NCC +58 R 2/3-L 1/3 RCC 13 1318 F 2 yr 85 31 Middle of NCC +43 9 1919 M 7 yr 90 24 Middle of NCC +36 R 2/3-L 13 RCC 17 3220 M 8 yr 86 19 Middle of NCC +49 R 2/3-L 1/3 RCC 10 1321 F 10 yr 80 17 Middle of NCC +39 R 2/3-1 1/3 RCC 15 3322 M 6 yr 90 32 Middle of NCC +43 R 2/3-L 1/3 RCC 12 2023 M 11 yr 102 25 Middle of NCC +40 R 2/3-L H13 RCC 15 28
Angles £, 0, +, and p expressed in degrees. Abbreviations as in table 1.
(figure 5, panel 2) and by the similar relationships ofthe aortic root with the pulmonary valve (position ofthe point o) in patients with tetralogy as in controlpatients. Thus the various measurements performed inpatients with tetralogy of Fallot show that the aorta isabnormally displaced to the right because of a clock-wise rotation about an eccentric pivot, the aortic anteri-or commissure. All these abnormalities of the spatialposition of the aortic root can only be the result of atrue anomaly of embryogenesis. The dilatation of theaorta above a perimembranous ventricular septal de-fect as a result of abnormal hemodynamics and creat-ing an exaggeration of the normal overriding would notchange the spatial position of the aortic root in terms ofposition of point r and value of angle 0 (figure 6).Our echocardiographic results are in agreement with
findings in the morphologic studies conducted byBecker et al."1 and Goor and associates ,4 5who per-formed virtually identical geometric measurements onpostmortem specimens. We agree with these workersthat tetralogy of Fallot is characterized by the morpho-genetic features of lack of conal rotation and conalmalseptation. The conal malseptation that participatesin the abnormal overriding of the aorta is shown ana-tomically by the anterior deviation of the conal sep-
tum, of which the septal insertion is in front of thetrabecula septomarginalis.'8 This latter anomaly hasbeen previously studied by two-dimensional echocar-diography, which permits diagnosis and quantitationof the deviation of the infundibular septum. 19 Howev-er, the concept of conotruncal malseptation as the solemorphogenetic mechanism in tetralogy62"23 cannotexplain all the features of the condition, since it alonecannot produce the rightward shift of the aorta withclockwise rotation. This latter feature can be explainedonly by a lack of the normal conal rotation24 that bringsthe aorta to a dextroposterior position during the nor-
TABLE 3Statistical analysis with Student's t test
Fallot NormalMeasurements (n 22) (n = 23) p value
Angle of atrial septum (E) 87 +6.1 86-+ 6.1 NSPercent right displacement
of the aortic root (d/a) 55.5+9 23.6+7.6 <.001Angle 0 9.2+11.2 43.3+8.8 <.001Angle + 13.2+2.9 13+2.6 NSAngle p 59.2 10.7 23.4+8.3 <.001
Angles expressed in degrees. All values are expressed as mean +SD.
CIRCULATION896
by guest on May 30, 2018
http://circ.ahajournals.org/D
ownloaded from
PATHOPHYSIOLOGY AND NATURAL HISTORY-CONGENITAL HEART DISEASE
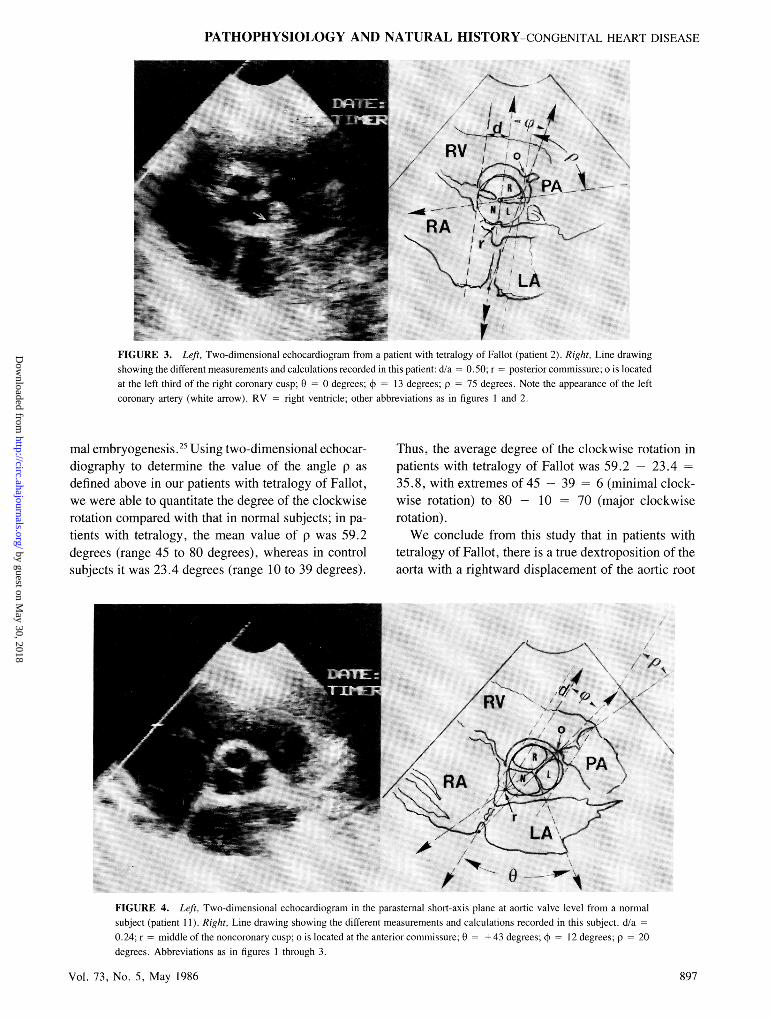
VrFIGURE 3. Left, Two-dimensional echocardiogram from a patient with tetralogy of Fallot (patient 2). Right, Line drawingshowing the different measurements and calculations recorded in this patient: d/a 0.50; r posterior commissure; o is locatedat the left third of the right coronary cusp; 0 = 0 degrees; 4 = 13 degrees; p = 75 degrees. Note the appearance of the leftcoronary artery (white arrow). RV - right ventricle; other abbreviations as in figures 1 and 2.
mal embryogenesis.25 Using two-dimensional echocar-diography to determine the value of the angle p asdefined above in our patients with tetralogy of Fallot,we were able to quantitate the degree of the clockwiserotation compared with that in normal subjects; in pa-tients with tetralogy, the mean value of p was 59.2degrees (range 45 to 80 degrees), whereas in controlsubjects it was 23.4 degrees (range 10 to 39 degrees).
Thus, the average degree of the clockwise rotation inpatients with tetralogy of Fallot was 59.2 - 23.435.8, with extremes of 45 -39 = 6 (minimal clock-wise rotation) to 80 - 10 = 70 (major clockwiserotation).We conclude from this study that in patients with
tetralogy of Fallot, there is a true dextroposition of theaorta with a rightward displacement of the aortic root
A:lp
A \0FIGURE 4. Left, Two-dimensional echocardiogram in the parasternal short-axis plane at aortic valve level from a normalsubject (patient 1 1). Right, Line drawing showing the different measurements and calculations recorded in this subject. d/a =
0.24; r = middle of the noncoronary cusp; o is located at the anterior commissure; 0 + 43 degrees; ¢ = 12 degrees; p 20degrees. Abbreviations as in figures 1 through 3.
Vol. 73, No. 5, May 1986 897
by guest on May 30, 2018
http://circ.ahajournals.org/D
ownloaded from
A
R PL
p
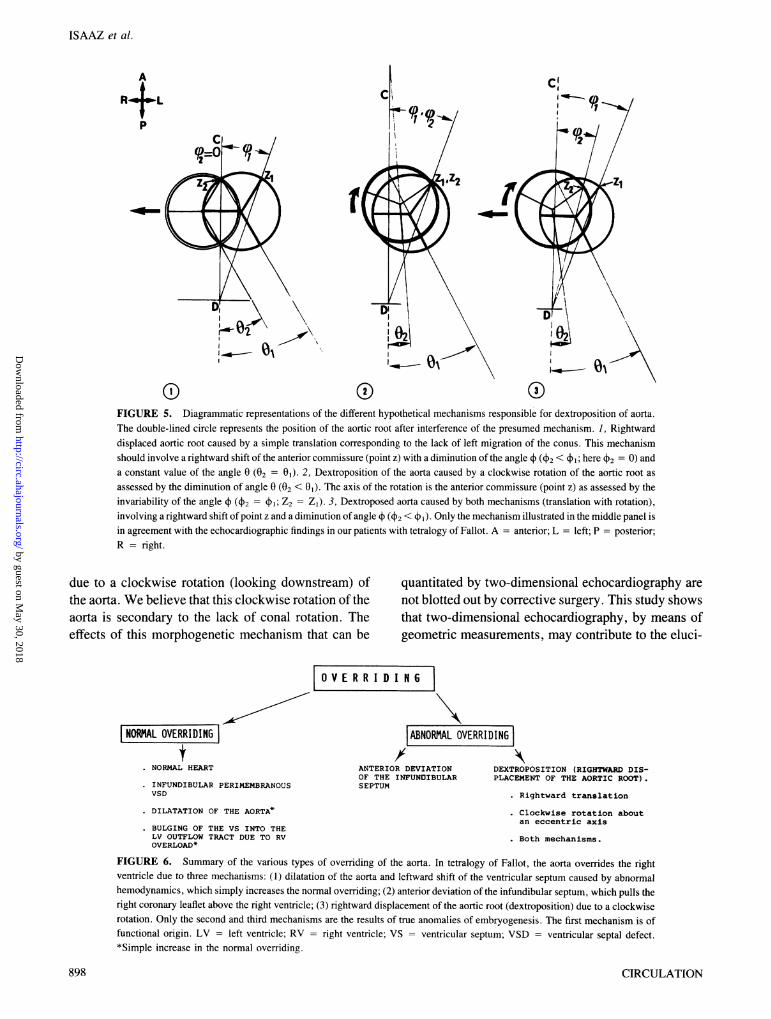
FIGURE 5. Diagrammatic representations of the different hypothetical mechanisms responsible for dextroposition of aorta.The double-lined circle represents the position of the aortic root after interference of the presumed mechanism. 1, Rightwarddisplaced aortic root caused by a simple translation corresponding to the lack of left migration of the conus. This mechanismshould involve a rightward shift of the anterior commissure (point z) with a diminution of the angle (42 < 1; here 42 = 0) anda constant value of the angle 0 (02 = 01). 2, Dextroposition of the aorta caused by a clockwise rotation of the aortic root as
assessed by the diminution of angle 0 (02 < 01). The axis of the rotation is the anterior commissure (point z) as assessed by theinvariability of the angle (42 = 4; Z2 = ZI). 3, Dextroposed aorta caused by both mechanisms (translation with rotation),involving a rightward shift of point z and a diminution of angle (42 < 1) Only the mechanism illustrated in the middle panel isin agreement with the echocardiographic findings in our patients with tetralogy of Fallot. A = anterior; L = left; P = posterior;R = right.
due to a clockwise rotation (looking downstream) ofthe aorta. We believe that this clockwise rotation of theaorta is secondary to the lack of conal rotation. Theeffects of this morphogenetic mechanism that can be
NORMAL OVERRIDINGt
. NORMAL HEART
. INFUNDIBULAR PERIMEMBRANOUSVSD
. DILATATION OF THE AORTA*
. BULGING OF THE VS INTO THELV OUTFLOW TRACT DUE TO RVOVERLOAD*
quantitated by two-dimensional echocardiography arenot blotted out by corrective surgery. This study showsthat two-dimensional echocardiography, by means ofgeometric measurements, may contribute to the eluci-
0 V E R R I D I R 6i
|ABNORMAL OVERRIDING|ANTERIOR DEVIATION DEXTROPOSITION (RIGHTWARD DIS-OF THE INFUNDIBULAR PLACEMENT OF THE AORTIC ROOT).SEPTUM
. Rightward translation
. Clockwise rotation aboutan eccentric axis
Both mechanisms.
FIGURE 6. Summary of the various types of overriding of the aorta. In tetralogy of Fallot, the aorta overrides the rightventricle due to three mechanisms: (1) dilatation of the aorta and leftward shift of the ventricular septum caused by abnormalhemodynamics, which simply increases the normal overriding; (2) anterior deviation of the infundibular septum, which pulls theright coronary leaflet above the right ventricle; (3) rightward displacement of the aortic root (dextroposition) due to a clockwiserotation. Only the second and third mechanisms are the results of true anomalies of embryogenesis. The first mechanism is offunctional origin. LV = left ventricle; RV = right ventricle; VS = ventricular septum; VSD = ventricular septal defect.*Simple increase in the normal overriding.
ISAAZ et al.
898 CIRCULATION
by guest on May 30, 2018
http://circ.ahajournals.org/D
ownloaded from

PATHOPHYSIOLOGY AND NATURAL HISTORY-CONGENITAL HEART DISEASE
dation of the difficult embryologic mechanisms of con-genital heart disease, providing the basis for furtherprospective studies to assess other conotruncal malfor-mations. Indeed, the geometric approach to cardiacanatomy originated by Van Praagh et al.26 and used onpostmortem specimens4 11 2629 can now be performedwith two-dimensional echocardiography, which pro-vides the advantages of a safe, noninvasive, and non-limiting method.
We gratefully acknowledge the secretarial assistance of Eve-lyne Marcilly and Marie-Odile Marchal. We thank RdgineChenu, Evelyne Fontaine, and Daniel Fernandez for their tech-nical assistance.
References1. Goor DA, Lillehei CW, Edwards JE: The sigmoid septum: vari-
ation in the contour of the left ventricular outlet. Am J Roentgenol107: 366, 1969
2. Goor DA, Lillehei CW, Rees R, Edwards JE: Isolated ventricularseptal defects: anatomical features and development. Chest 58:468, 1970
3. Becker AE, Anderson RH: Ventricular septal defect. In BeckerAE, Anderson RH, editors: Pathology of congenital heart disease.London, 1981, Butterworths, p 108
4. Goor DA, Lillehei CW, Edwards JE: Ventricular septal defects andpulmonic stenosis with and without dextroposition: anatomic fea-tures and embryologic implications. Chest 60: 117, 1971
5. Goor DA, Lillehei CW: Dextroposition of the aorta. In Goor DA,Lillehei CW, editors: Congenital malformations of the heart. NewYork, 1975, Grune & Stratton, p 169
6. Dor X, Corone P: Anomalies cono-troncales. In Embryologie nor-male et genese des cardiopathies congenitales. Encycl Med ChirParis, Coeur-Vaisseaux, 11001 C10:1- 12, 11001 C20:1-16, 1981
7. McCord MC, Van Elk J, Blount G: Tetralogy of Fallot: clinical andhemodynamic spectrum of combined pulmonary stenosis and ven-tricular septal defect. Circulation 16: 736, 1957
8. Van Praagh R, Van Praagh S, Nebesar RA, Muster AJ, Sinha SN,Paul MH: Tetralogy of Fallot: underdevelopment of the pulmonaryinfundibulum and its sequelae. Am J Cardiol 26: 25, 1970
9. Abbott ME, Lewis DS, Neattie WW: Differential study of a case ofpulmonary stenosis of inflammatory origin (ventricular septumclosed) and two-cases of a) pulmonary stenosis and b) pulmonaryatresia of developmental origin with associated ventricular septaldefect and death from paradoxical cerebral embolus. Am J Med Sci165: 635, 1923
10. Talley JE, Fowler K: Tetralogy of Fallot with hypoplasia of thedextroposed aorta. Am J Med Sci 191: 618, 1936
11. Becker AE, Connor M, Anderson RH: Tetralogy of Fallot: a mor-phometric and geometric study. Am J Cardiol 35: 402, 1975
12. Sahn DJ, Terry R, O'Rowke R, Leopold G, Friedman WF: Multi-
ple crystal cross-sectional echocardiography in the diagnosis ofcyanotic congenital heart disease. Circulation 50: 230, 1974
13. Lange LW, Sahn DJ, Allen HD, Goldberg SJ: Subxiphoid cross-sectional echocardiography in infants and children with congenitalheart disease. Circulation 59: 513, 1979
14. Hagler DJ, Tajik AJ, Seward JB, Mair DD, Ritter DG: Wide-angletwo-dimensional echocardiographic profiles of conotruncal abnor-malities. Mayo Clin Proc 55: 73, 1980
15. Sanders SP, Bierman FZ, Williams RG: Conotruncal malforma-tions: diagnosis in infancy using subxiphoid two-dimensional echo-cardiography. Am J Cardiol 50: 1361, 1982
16. De Maria A, Gramiak R, Henry WL, King DL, Kisslo JA, PoppRL, Sahn DJ, Schiller NB, Tajik A, Teichholz LE, Weyman AE:Standards and nomenclature for two-dimensional echocardiog-raphy. Report of the American Society of Echocardiography Com-mittee. In Schapira JN, editor: Two-dimensional echocardiog-raphy. Baltimore, 1982, Williams & Wilkins, p 1
17. Seward JB, Tajik A, Hagler D, Edwards WD: Update on nomen-clature, image orientation and anatomic-echocardiographic corre-lations, with new tomographic views. In Schapira JN, editor: Two-dimensional echocardiography. Baltimore, 1982, Williams &Wilkins, p 1 1
18. Becker AE, Anderson RH: Tetralogy of Fallot. In Becker AE,Anderson RH, editors: Pathology of congenital heart disease. Lon-don, 1981, Butterworths, p 191
19. Isaaz K, Cloez JL, Danchin N, Marcon F, Worms AM, Pemot C:Right ventricular outflow tract assessment by two-dimensionalechocardiography in children using a new subcostal view: Angio-cardiographic and morphologic correlative study. Am J Cardiol 56:539, 1985
20. Von Rokitansky KF: Die defekte der Scheidewinde des Herzens.Vienna, 1875, Braumulller
21. Abbot M: Congenital cardiac disease. In Osler and Melrae's mod-em medicine, vol. 4. Philadelphia, 1915, Lea and Febiger, p 354
22. De la Cruz MV, Da Rocha JP: An ontogenetic theory for theexplanation of congenital malformations involving the truncus andconus. Am Heart J 51: 782, 1956
23. Van Mierop LHS, Wiglesworth FW: Pathogenesis of transpositioncomplexes II. Anomalies due to faulty transfer of the posteriorgreat artery. Am J Cardiol 12: 226, 1963
24. Asami I: Beitrag zur Entwicklung des Kammerseptums in mensch-lichen Herzen mit besondere: beruicksichtigung der SogenarinterBulbusdrehung. Z Anat Entwicklungsgesch 128: 1, 1969
25. Goor DA, Dische R, Lillehei CW: The conotruncus. I. Its normalinversion and conus absorption. Circulation 46: 375, 1972
26. Van Praagh R, Ongley PA, Swan HJC: Anatomic types of single orcommon ventricle in man. Morphologic and geometric aspects of60 necropsied cases. Am J Cardiol 13: 367, 1964
27. Van Praagh R, Van Praagh S: Isolated ventricular inversion aconsideration of the morphogenesis, definition and diagnosis ofnontransposed and transposed great arteries. Am J Cardiol 17: 395,1966
28. Van Praagh R, Van Praagh S: Anatomically corrected transpositionof the great arteries. Br Heart J 29: 112, 1967
29. Melhvish BPP, Van Praagh R: Juxtaposition of the atrial appen-dages: a sign of severe cyanotic congenital heart disease. Br Heart J30: 269, 1968
Vol. 73, No. 5, May 1986 899
by guest on May 30, 2018
http://circ.ahajournals.org/D
ownloaded from

K Isaaz, J L Cloez, F Marçon, A M Worms and C Pernotechocardiographic answer.
Is the aorta truly dextroposed in tetralogy of Fallot? A two-dimensional
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1986 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.73.5.892
1986;73:892-899Circulation.
http://circ.ahajournals.org/content/73/5/892the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on May 30, 2018
http://circ.ahajournals.org/D
ownloaded from





























