Embed Size (px)
Citation preview

ANZHSN Bulletin - www.horizonscanning.gov.au
In This Issue... Internet delivered cognitive behavioural therapy .................................... 2 Transvaginal cholecystectomy using natural orifice transluminal endoscopic survery (NOTES) ........................................ 3 Percutaneous pulmonary valve implantation ................................................ 4 Rapid Chlamydia test for Chlamydia trachomatis ................................................ 6 Robot assisted thyroidectomy ................... 7 Other new and emerging technologies..... 9
Issue 13, December 2009
ANZHSN Bulletin ‘New health technologies identified through the Australia and New Zealand Horizon Scanning Network (ANZHSN)’
From the Chair’s desk
More recently, the Canadian HTA agency, CADTH, has produced a publication on the use of self- monitoring blood glucose levels using blood glucose test strips for the management of non-insulin dependent diabetes mellitus type II diabetes in adults. The results of this study suggests that self-monitoring of blood glucose on a daily basis produces benefits, but compared with no testing, has an incremental cost per quality-adjusted life year of $113,643 Canadian. They conclude that for most patients with type II diabetes, daily use of blood glucose test strips for self-monitoring does not represent efficient use of health care resources, although periodic testing, 1-2 times a week may be cost effective.
The examination using HTA of existing health care technologies is a complex issue and HPACT will carefully consider how it might effectively enter this field during 2010.
Yours sincerely
Brendon Kearney Chair of HealthPACT
Dear Colleagues
Welcome to the New Year!
HPACT is looking forward to a busy and productive year. It is now a sub-committee of CTEPC, which is major committee of AHMAC. HPACT will be reviewing its work programme during the year, having submitted some suggested changes. These include the use of health technology assessment to review existing health care services. Health technology assessment is principally used in the Australian setting for assessment of the introduction of new drugs, devices, diagnostics, procedures etc. However, it is important that we apply the same rigor to existing health care services to ensure that there is an effective and efficient use of scarce resources for the provision of health care services.
Last year the Monash Medical Centre hosted a workshop, in which two case studies on the review of existing health care services using health technology assessment were discussed. This included the value of surgical procedures in sleep apnoea where the evidence suggested often little benefit or sometimes harm, and a review of two randomised controlled trials examining the use of verterboplasty.

Depression is a common disorder but is poorly diagnosed and the number of people who either receive appropriate or actively seek treatment is low (2). One of the main barriers to patients receiving appropriate psychotherapy, such as cognitive-behavioural therapy (CBT), is the lack of clinicians (psychologists, psychiatrists and counsellors) able to provide this service, especially in rural and remote areas.
HOW IT WORKS CBT is defined as any specific psychological or psychosocial intervention that is short-term and goal-orientated. CBT is based on learning the principles of behaviour change and is directed at effecting change in a clinical outcome (1). CBT assists the patient to understand, manage and change their thoughts (cognitions) and actions (behaviour). CBT is designed to replace negative thoughts for positive ones and to reinforce positive actions (4). Internet based CBT is a virtual clinic which uses the same techniques as face-to-face therapy but delivers it via a web site.
THE EVIDENCE Five good quality studies were included for assessment in this summary. Only the results from one study are described here, the remaining information can be obtained from the Horizon Scanning web site. All studies included for assessment reported significant improvements in the symptoms of depression after using internet delivered CBT when compared to control patients and this improvement appeared to be maintained over time (4, 8 and 12-months).
A recent Australian RCT enrolled depressed people via the Sadness programme. Patients were randomised to the Sadness programme (n=29) or to a wait-list control group (n=19), the majority of participants were female. The programme consisted of six online lessons, homework, online discussion forums and email contact with a mental health clinician, conducted over an eight-week period.
Primary outcome measures were changes in the Beck Depression Index (BDI) and Patient Health Questionnaire Nine Item (PHQ-9) scores (see original summary for definitions). Post-treatment scores for both BDI and PHQ-9 were significantly lower than baseline scores (p<0.02 and p<0.01, respectively) in the treatment group compared to the control group. It should also be noted that post-treatment scores within the treatment group and control groups were significantly lower than pre-treatment scores for both BDI and PHQ-9 scores. Prior to treatment 81% of the treatment group
ANZHSN Bulletin
Internet delivered cognitive behavioural therapy
2. Issue 13 December 2009
and 94% of the control group had a PHQ-9 score >10, indicating a diagnosis of depression. After treatment, the number of patients with a PHQ-9 score >10 in the treatment group was significantly reduced (44%) with little change in the control group (89%). Although other researchers have stated that a BDI <10 is a “recovery from depression” score, the BDI in this study was much higher than 10 post-treatment (mean 17.30). It is unclear how many patients achieved a score less than 10. The mean therapist time per participant was 111 minutes which included monitoring of the discussion forum and feedback. A mean of 8.33 emails were sent to each participant in the treatment group. The initial diagnostic interview and other administrative tasks required a further 30 minutes per patient (3).
.FUTURE STEPS Good quality evidence indicates a potential for the uptake of this technology in rural and remote areas, and the possible ability to overcome barriers to increase the treatment options especially in males. The programme, as offered in Australia, is inexpensive. HealthPACT have recommended that this summary be disseminated in the jurisdictions and to Beyond Blue, with a view to writing a more in-depth report.
Written by Linda Mundy (AHTA)
REFERENCES
1. Fulcher, C. D., Badger, T. et al (2008). 'Putting evidence into practice: interventions for depression', Clin J Oncol Nurs, 12 (1), 131-140.
2. Kaltenthaler, E., Parry, G. et al (2008). 'Computerised cognitive-behavioural therapy for depression: systematic review', Br J Psychiatry, 193 (3), 181-184.
3. Perini, S., Titov, N. & Andrews, G. (2009). 'Clinician-assisted Internet-based treatment is effective for depression: randomized controlled trial', Aust N Z J Psychiatry, 43 (6), 571-578.
4. ReachOut Australia (2009). Cognitive behavioural therapy (CBT) [Internet]. Available from: http://au.reachout.com/find/articles/cognitive-behavioural-therapy-cbt [Accessed 14th October].

Natural orifice transluminal endoscopic surgery (NOTES) is an emerging surgical procedure which may potentially be less invasive than laparoscopic surgery.
HOW IT WORKS During a NOTES procedure a flexible endoscope is passed through a natural orifice, such as the mouth, vagina or rectum to perform intra-abdominal procedures. The technique has been touted as less invasive than laparoscopic surgery by virtually eliminating incision-related complications such as scars, hernias, pain, adhesions and surgical site infections (McGee et al 2006, Merrifield et al 2006). To date, the best portal for access has not been determined, but all have been evaluated in various animal studies (Box et al 2009). There are major concerns with regards to transgastric approaches to NOTES as improper gastric closure may lead to postoperative leakage and peritonitis. Transvaginal NOTES has the potential advantages of easy access and closure under direct vision. The experience gained from experimental settings has suggested that with current available technology, procedures involving in the upper part of the abdomen are better undertaken via natural orifices located in the pelvis (Pearl & Ponsky 2008). From 2007, several techniques for transvaginal cholecystectomy using flexible endoscopes with minimal laparoscopic assistance have been described (Pugliese 2009). In virtually all human trials to date, a hybrid procedure was adopted where the operators utilised a fusion of minilaparoscopy and NOTES (Noguera et al 2009).
THE EVIDENCE Study description
Three case series were included for assessment in this summary based. Only the results of the largest are presented here, the details of the remaining two studies may be accessed on the Horizon Scanning web site.
The retrospective case series study by Zornig et al (2009) reported on the safety and effectiveness of transvaginal NOTES in 68 patients treated for symptomatic cholecystolithiasis, 11 of whom had acute or chronic inflammation of the bladder. The mean age was 50 years (range 16-76) and mean BMI was 25.4 kg/m2 (range 16-35). Patients were interviewed 3-10 months after surgery. A hybrid NOTES procedure was utilised, as an abdominal trocar was used during the operation.
Three patients had severe adhesions in the lesser pelvis during diagnostic laparoscopy and these patients were converted to conventional laparoscopic cholecystectomy. There were no intra-operative complications, but in three cases (4.4%) an additional abdominal trocar was necessary. The in-hospital post-operative course was uneventful in all patients with no patients reporting pain as a result of vaginal manipulation. At 1-week follow up (n=59), none of the patients had any complaints, and physical examination including vaginal endosonography revealed no pathological findings. However, one patient who did not undergo the 1-week follow up examination presented with an abscess in the pouch of Douglas 3 weeks after surgery. When patients were interviewed 3 to 10 months after surgery there were no complaints regarding the procedure. A total of 48 patients (70.5%) had sexual intercourse after the operation (mean time not stated) and did not notice any changes. The mean operative time was 51 minutes (range: 30-100 minutes).
.FUTURE STEPS Additional studies are required before transvaginal NOTES can be performed routinely. Considering the interest and the potentially rapid diffusion of this technique, it is recommended that transvaginal cholecystectomy is monitored for 12 months for new evidence.
Written by Irving Lee (ASERNIP-S)
ANZHSN Bulletin
Transvaginal cholecystectomy using natural orifice transluminal endoscopic surgery (NOTES)
REFERENCES
1. Box G.N., Bessler M. & Clayman RV (2009). ‘Transvaginal access: current experience and potential implications for urologic applications.’ Journal of Endourology; 23(5):753-757.
2. McGee M.F., Rosen M.J., Marks J. Et al (2006). ‘A primer on natural orifice transluminal endoscopic surgery: building a new paradigm.’ Surgical Innovation; 13(2): 86-93.
3. Merrifield B.F., Wagh M.S. & Thompson CC. (2006) ‘Peroral transgastric organ resection: a feasibility study in pigs.’ Gastrointestinal Endoscopy; 63(4): 693-697.
4. Noguera J., Dolz C., Cuadrado A. Et al (2009) ‘Hybrid transvaginal cholecystectomy, NOTES, and minilaparoscopy: analysis of a prospective clinical series.’ Surg Endos, 23(4):876-81.
5. Pearl J.P. and Ponsky J.L. (2008). ‘Natural orifice translumenal endoscopic surgery: a critical review.’ Journal of Gastrointestinal Surgery, 12(7): 1293-1300.
6. Pugliese R., Forgione A., Sansonna F. Et al (2009). ‘Hybrid NOTES transvaginal cholecystectomy: operative and long-term results after 18 cases.’ Langenbecks Archives of Surgery; [Epub ahead of print].
7. Zornig C., Mofid H., Siemssen L. Et al (2009). ‘Transvaginal NOTES hybrid cholecystectomy: feasibility results in 68 cases with mid-term follow-up.’ Endoscopy; 41(5): 391-394.
December 2009 Issue 12 3.

operative period were reported although one patient had a guide wire injury which resulted in minor lung bleeding.
Total procedure time, including catheterisation and fluoroscopy, was 209 ± 14 minutes. The BMS and PPVI procedures were successful in all patients. BMS achieved significant reduction in mean right ventricular systolic pressure, mean pulmonary artery to right ventricular pullback gradient and the mean ratio of right ventricular to systemic pressure. However, PPVI did not produce any statistically significant changes in these measurements. The mean pulmonary artery diastolic pressure increased significantly after PPVI compared to BMS, indicating that pulmonary valvular competence was restored. There were no statistically significant changes in systemic pressures after BMS, although there was a slight but not statistically significant increase after PPVI. Magnetic resonance readings indicated that there was a significant increase in pulmonary regurgitant factor after BMS compared to before BMS. In addition, there was a decrease in right ventricular end-systolic volume and an increase in total right ventricular stroke volume and right ventricular ejection fraction as a result of a reduction in ventricular after load after BMS compared to pre-BMS measurements. Despite these improvements, the lack of overall gain in effective right ventricular stroke volume (33.8 mL/m2 vs. 32.6 mL/m2) after BMS indicated that these changes did not compensate for the pulmonary regurgitation induced by BMS.
In contrast, pulmonary regurgitation was virtually eliminated following PPVI as indicated by measurements of pulmonary regurgitation fraction (41.4% after BMS vs. 3.6% after PPVI; p<0.001). Right ventricular end diastolic volume was also significantly lower and there was a significant improvement in effective right ventricular stroke volume after PPVI compared with the post-BMS state. However, there were no significant
ANZHSN Bulletin
Percutaneous pulmonary valve implantation
4. Issue 13 December 2009
Percutaneous pulmonary valve implantation (PPVI) is an alternative to stenting for the treatment of a dysfunctional right ventricle to pulmonary artery conduit. The use of PPVI can potentially treat conduit dysfunction without sacrificing valvular competence, and may reduce the need for subsequent surgical repair.
HOW IT WORKS Obstruction of blood flow from the right ventricle to the pulmonary artery, the right ventricular outflow tract (RVOT), is a common feature of a number of congenital heart diseases. Surgical reconstruction of the RVOT is an integral part of treatment and is one of the most commonly performed operations in patients with congenitally malformed hearts. Dysfunction of the pulmonary valve, which results in pulmonary stenosis and/or backflow of blood (regurgitation), is relatively common post-surgery. The conduits used have a short lifespan (<10 yrs) (Lurz and Bonhoeffer 2008) and patients often require multiple operations during their lifetime to prevent or reverse valvular incompetence or obstruction (Bove et al 1985, Eyskens et al 2000).
To reduce the need for reoperation, percutaneous dilation and stenting (bare-metal stenting or BMS) are used to treat degenerated conduits. Although BMS relieves the obstruction to blood flow, it also results in pulmonary valve regurgitation (Gatzoulis et al 2000, Frigiola et al 2004). There has been interest in PPVI as an alternative to BMS.
THE EVIDENCE Study description
One prospective, non-randomised comparative study on PPVI was identified for inclusion, and 7 prospective case series studies were identified. Only the results from the comparative study will be summarised here. All other results and raw data from the Lurz study may be accessed via the horizon scanning web site.
Lurz et al (2009) enrolled 14 consecutive adolescents (median age 12.9 yrs, range 9.9-17.8) with a clinical indication for PPVI in the context of significant RVOT. Patients underwent BMS followed by PPVI, which confounds the results for PPVI, however this study was assessed due to the paucity of evidence available on PPVI. Magnetic resonance imaging was utilised before and after both procedures to assess acute physiological changes.
No major complications for BMS or PPVI in the peri-

Percutaneous pulmonary valve implantation
ANZHSN Bulletin
December 2009 Issue 12 5.
NEWS FLASH
In the November 2nd edition of the Medical Journal of Australia (vol 191 (9):487-91), Gialamas et al reported the results of an Australian RCT on point-of care-testing (PoCT) “Does point-of-care testing lead to the same or better adherence to medication? A randomised controlled trial: the PoCT in General Practice Trial.”
The objective was to measure patient compliance to medication when PoCT was used compared to conventional pathology testing. Australian general practices (n=53) in urban, rural and remote areas across three Australian states participated during the period September 2005 to February 2007. Patients with established type 1 or type 2 diabetes, established hyperlipidaemia, or requiring anticoagulant therapy were recruited to the study. A total of 4381 were included in the analysis (2585 in the intervention group and 1796 in the control group). Medication adherence was assessed twice (in April 2006 and January 2007) by a self-administered questionnaire. The intervention group had blood and urine samples tested using PoCT devices within their general practices and the control group had samples tested by their usual pathology laboratories.
PoCT was non-inferior to pathology laboratory testing in relation to the proportion of questionnaire responses indicating medication adherence (39.3% v 37.0%, difference 2.3% , p < 0.001). Non-inferiority could also be concluded separately for patients with diabetes (38.5% v 37.3%, difference 1.2% p = 0.01); hyperlipidaemia (38.3% v 37.3%, difference 1.0%, p < 0.001) and for patients requiring anticoagulant therapy (44.5% v 41.4%, difference 3.1%, p = 0.01).
PoCT was found to be the same or better than pathology laboratory testing for most tests, suggesting that PoCT could assist GPs in better management of some chronic conditions. The results also suggested that having an immediate test result was beneficial for patients in terms of medication compliance. PoCT is not publicly funded.
changes in right ventricular end systolic volume or right ventricular ejection fraction after PPVI, compared with post-BMS measurements.
Both BMS and PPVI had an effect on left ventricular volumes and function as left ventricular end diastolic volume decreased slightly after BMS but significantly increased after PPVI. Similarly, effective left ventricular stroke volume did not change after BMS, but increased significantly after PPVI. The significant increase in effective right and left ventricular stroke volume following PPVI was accompanied by a significant reduction in heart rate relative to post-BMS measurements. As a result, there was no significant change in cardiac output after PPVI.
The relevance of these results is severely limited since PPVI results were confounded by the presence of the BMS.
.FUTURE STEPS The limited evidence from a single case series study suggests that PPVI is associated with low mortality rates and is relatively safe with encouraging short term results. There are no data on the longevity of the Melody valve. The paucity of long-term data is unlikely to be addressed in the near future.
However, there is limited evidence that PPVI is feasible despite the high revision rates. It is recommended that PPVI is monitored for 24 months with the view of retrieving some data on the longevity of these valves.
Written by Irving Lee (ASERNIP-S)
REFERENCES
1. Bove E.L., Kavey R.E., Byrum C.J. et al (1985). ‘Improved right ventricular function following late pulmonary valve replacement for residual pulmonary insufficiency or stenosis.’ Journal of Thoracic and Cardiovascular Surgery; 90(1): 50-55.
2. Eyskens B., Reybrouck T., Bogaert J.et al (2000). ‘Homograft insertion for pulmonary regurgitation after repair of tetralogy of fallot improves cardiorespiratory exercise performance.’ American Journal of Cardiology; 85(2): 221-225.
3. Frigola A., Redington A.N., Cullen S. et al (2004). ‘Pulmonary regurgitation is an important determinant of right ventricular contractile dysfunction in patient with surgically repaired tetralogy of Fallot.’ Circulation; 110: II153-II157.
4. Gatzoulis M.A., Balaji S., Webber S.A. et al (2000). ‘Risk factors for arrhythmia and sudden cardiac death late after repaid of tetralogy of Fallot: a multicentre study.’ Lancet; 356: 975-981.
5. Lurz P. and Bonhoeffer P. (2008). ‘Percutaneous implantation of pulmonary valves for treatment of right ventricular outflow tract dysfunction.’ Cardiol Young; 18: 260-267.
6. Lurz P., Nordmeyer J., Muthurangu V. et al (2009). ‘Comparison of bare metal stenting and percutaneous pulmonary valve implantation for treatment of right ventricular outflow tract obstruction.’ Circulation; 199: 2995-3001.

ANZHSN Bulletin
Rapid Chlamydia test for Chlamydia trachomatis
6. Issue 13 December 2009
REFERENCES
1. Nadala, E. C., Goh, B. T. et al (2009). 'Performance evaluation of a new rapid urine test for chlamydia in men: prospective cohort study', BMJ, 339, b2655.
2. Vajdic, C. M., Middleton, M. et al (2005). 'The prevalence of genital Chlamydia trachomatis in Australia 1997-2004: a systematic review', Sex Health, 2 (3), 169-183.
In Australia and New Zealand, the rate of chlamydia infection has been steadily increasing for a number of years, with chlamydia now the most common notifiable disease. Notification rates are likely to be an underestimate of the true rate of chlamydia infection as the majority of tests are performed on symptomatic patients and approximately 40-85% of infected individuals may be asymptomatic (Vajdic et al 2005). The Rapid Chlamydia urine test will enable a test and treat regimen, with patients undergoing the test, obtaining the result and if needed receiving treatment all in the one clinic visit.
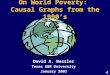
HOW IT WORKS The Rapid Chlamydia urine test requires subjects to provide a urine sample, collected using the FirstBurst urine collection device which collects the first 4-5 ml of urine. The urine is centrifuged and the pellet is extracted by the sequential addition of the three kit solutions. The extracted sample is added to a tube which contains amplification and detection reagents. A test strip embedded with a monoclonal antibody to chlamydial lipoploysaccharide is then added to the solution and incubated at room temperature for 25 minutes (Figure 1). If chlamydia is present in the sample a line appears on the test strip (Nadala et al 2009).
THE EVIDENCE Three good quality diagnostic comparative studies were included for assessment in this summary. Only the results from one study are included, the remaining information can be obtained from the Horizon Scanning web site.
Nadala et al (2009) enrolled 1,277 young males (>16 years) attending a sexual health clinic and a genitourinary clinic in the United Kingdom. Enrolled subjects provided a urine sample, with the first 4-5ml collected using the FirstBurst collection
Above: The Rapid Chlamydia test, showing test strip with a result line indicating the presence of Chlamydia (printed with permission of Wellcome)
device. The majority of men attending site one were asymptomatic Samples were tested for the presence of chlamydia using the Rapid Chlamydia test and the reference standard, PCR. Twenty participants were identified as positive for chlamydia infection by PCR at site one (4%) and 90 (12%) at site two. The overall sensitivity and specificity of the Rapid Chlamydia test was 81.8 and 98.5 per cent, respectively and the overall positive and negative predictive value was 84 and 98 per cent. There was a significant difference between the PPV and NPV values obtained at the two sites (p=0.009 and p=0.028, respectively), which may reflect differences in prevalence of chlamydia infection between the two sites. Of the 20 participants found to be positive for chlamydia at site one, 18 (90%) were asymptomatic at presentation. At site two, 28 (31%) of those found to be positive had no symptoms. Of these asymptomatic men, 16/18 (89%) and 20/28 (71%) tested positive for chlamydia using the Rapid Chlamydia test, giving an overall test sensitivity of 78 per cent (36/46) for asymptomatic men. The combined sensitivity for symptomatic men testing positive at both sites was higher at 84 per cent. The majority of participants preferred giving a urine sample (89%), with seven per cent preferring a swab and four per cent willing to provide either. However as participants were not asked to provide a swab, this preference may not be valid. The majority of subjects (96%) indicated that they were willing to wait an hour or more for test results with only four per cent unwilling to wait an hour.
.FUTURE STEPS The rapid Chlamydia test may be of use in rural and remote areas and in public hospital settings. Whether or not this test may be useful for screening populations remains to be ascertained. However, based on initial promising results from studies, the rapid increase in infection rates and the need to reduce the number of new chlamydia infections in the population by identifying asymptomatic individuals HealthPACT have recommended that this technology be monitored for further information in 12-months time.
Written by Linda Mundy (AHTA)

Robot-assisted thyroidectomy may addresses the limitations of conventional endoscopic surgery, as it allows for haptic feedback, three-dimensional optics and utilises flexible endoscopic instruments. This is expected to improve patient outcomes while simultaneously reducing operator stress due to better instrumentation and ergonomics.
HOW IT WORKS Despite the advantages of endoscopic surgery, there are some inherent limitations to this technique, including limited visualisation and difficulty with the precision of instruments. The da Vinci® robotic surgical system was developed to address the limitations of endoscopic surgery and has been utilised in abdominal and thoracic surgery. The da Vinci system allows for operational manipulations through a three-dimensional magnified field of view, multi-articulated instruments and an ergonomic workspace (Kang et al 2009b).
THE EVIDENCE Three published papers on robot-assisted endoscopic thyroidectomy using the da Vinci system were included for assessment. There was a substantial patient overlap for two
papers published by the same research group (Kang et al 2009a, Kang et al 2009b), therefore only one study (Kang et al 2009b) w a s i n c l u d e d f o r assessment.
A total of 200 consecutive patients (192 female; mean age: 40.3 ± 9.5 years) diagnosed with papillary thyroid carcinoma under-wen t robo t - a s s i s t ed endoscopic thyroidectomy using a gasless transaxillary approach. Eligible patients had well-differentiated thyroid carcinoma and a
tumour size of ≤ 2cm. Patients with extrathyroidal tumour invasion, multiple lateral neck node metastases, perinodal infiltration at a metastatic lymph node, or distant metastasis or a lesion located in the thyroid dorsal area were excluded. 155 patients underwent Partial thyroidectomy was performed in 155 patients and the remaining 45 had total
thyroidectomies. Mean follow up duration was 328.3 days (range 206-485 days). These patients were compared with historical data of patients who underwent conventional open thyroidectomy for papillary thyroid microcarcinoma.
There were no conversions to open surgery and the mean total operative time was 141.1 ± 38.8 minutes. Postoperative complications included transient hypocalcaemia (6%), transient hoarseness (4%), seroma (1%) and permanent recurrent laryngeal nerve (RLN) palsy (0.5%). The patient with RLN palsy did not recover vocal cord movement. In patients who experienced transient hypocalcemia, serum parathyroid hormone levels reduced slightly during the immediate postoperative period (up to 7 days). In most patients, calcium and parathyroid hormone levels normalised within one month after surgery. The investigators reported that 38/45 patients who underwent bilateral total thyroidectomy (7 low risk patients excluded) underwent radioactive iodine (RAI) ablation 4 to 6 weeks postsurgery and iodine131 whole body scans 2 days after RAI ablation. No patient had abnormal RAI uptake. There were no signs of local recurrence throughout the follow up period (mean: 328.3 days).
Complications observed in patients who underwent open surgery included temporary hypocalcaemia (38.5%), temporary hoarseness (2.2%), seroma (0.4%) and haematoma (0.9%). Patients who experienced hypocalcaemia or hoarseness recovered within 1-month and there were no cases of permanent hypocalcaemia or RLN palsy in either group.
.FUTURE STEPS Based on the limited evidence available, robot-assisted endoscopic thyroidectomy should be attempted in a clinical trial setting with a select patient group. Additional long-term studies are warranted, as robotic surgery continues to diffuse widely across various surgical specialties. It is recommended that robot-assisted endoscopic thyroidectomy be monitored for 12 months for additional evidence of its long-term effectiveness.
Written by Irving Lee (ASERNIP-S)
ANZHSN Bulletin
Robot assisted thyroidectomy
REFERENCES
1. Kang S.W., Jeong J.J., Yun J.S. et al (2009a). ‘Robot-assisted endoscopic surgery for thyroid cancer: experience with the first 100 patients.’ Surgical Endoscopy 2009a [Epub ahead of print].
2. Kang S.W., Jeong J.J., Nam K.H. et al (2009b). ‘Robot-assisted endoscopic thyroidectomy for thyroid malignancies using a gasless transaxillary approach.’ Journal of the American College of Surgeons; 209(2): e1-7.
December 2009 Issue 12 7.
Above: The da Vinci Surgical System.
Source: http://commons.wikimedia.org/wiki/File:Laproscopic_Surgery_robot.jpg

ANZHSN Bulletin
NEWS FLASH In the November 5th 2009 issue of JAMA (Vol 302 number 17: pages
1888-1895) (doi:10.1001/jama.2009.1535), The Australia and New
Zealand Extracorporeal Membrane Oxygenation (ANZ ECMO)
Influenza Investigator group published their article entitled
“Extracorporeal Membrane Oxygenation for 2009 Influenza A (H1N1)
Acute Respiratory Distress Syndrome”. This was an observational study of all patients (n=68) with 2009 influenza A (H1N1)–associated acute
respiratory distress syndrome (ARDS) treated with extracorporeal
membrane oxygenation (ECMO) in 15 intensive care units (ICUs) in Australia and New Zealand between June 1 and August
31, 2009.
Results: Sixty-eight patients with severe influenza-associated ARDS were treated with ECMO, of whom 61 had either confirmed 2009 influenza A (H1N1) (n=53) or influenza A not subtyped (n=8), representing an incidence rate of 2.6 ECMO
cases per million population. An additional 133 patients with influenza A received mechanical ventilation but no ECMO in the
same ICUs. The 68 patients who received ECMO had a median (interquartile range [IQR]) age of 34.4 (26.6-43.1) years and 34
patients (50%) were men. Before ECMO, patients had severe respiratory failure despite advanced mechanical ventilatory
support with a median (IQR) PaO2/fraction of inspired oxygen (FIO2) ratio of 56 (48-63), positive end-expiratory pressure of 18 (15-20) cm H2O, and an acute lung injury score of 3.8 (3.5-4.0). The median (IQR) duration of ECMO support was 10 (7-
15) days. At the time of reporting, 48 of the 68 patients (71%; 95% CI [60, 82]) had survived to ICU discharge, of whom 32
had survived to hospital discharge and 16 remained as hospital inpatients. Fourteen patients (21%; 95% CI [11, 30]) had died
and 6 remained in the ICU, 2 of whom were still receiving ECMO.
Conclusions: In Australia and New Zealand, during the 2009 influenza A (H1N1) winter pandemic, there was a large increase
in the use of ECMO for ARDS in patients compared with the winter of 2008. Despite their illness severity and the prolonged use of life support, most of these patients survived. This information should facilitate health care planning and clinical
management for these complex patients during the ongoing pandemic. These findings have implications for health care
planning and the clinical management of patients with 2009 influenza A (H1N1) during the 2009-2010 northern hemisphere
winter. These results indicate that the incidence of ARDS is sufficient to warrant consideration of ECMO.
INTERESTING LINKS
The Victorian Department of Health issues a regular
Health Technology newsletter containing the latest health
technology news and views from Victoria.
The New Zealalnd Ministry of Health also produces a
newsletter which provides links to systematic reviews and important research on health innovations and emerging
new technologies.
8. Issue 13 December 2009

PRODUCTION NOTES
The ANZHSN Bulletin is published by Adelaide Health Technology Assessment (AHTA) on behalf of the Health Policy Advisory Committee on Technology (HealthPACT) and funded by the Australian Government Department of Health and Ageing.
- - - - - - - - - - - - - - - - - - - - - - - -
Editor: Linda Mundy Design: Lashan Clifton Writers/Information Specialists: Deanne Leopardi, Linda Mundy, Adrian Purins, Caryn Perera, Janet Hiller, Annette Braunack-Mayer. Contact: Adelaide Health Technology Assessment (AHTA) Discipline of Public Health, Mail Drop DX 650 545 The University of Adelaide Adelaide, South Australia 5005 Australia email: [email protected] Tel: +61 8 8303 4617 Fax: +61 8 8303 6899 www.adelaide.edu.au/ahta
- - - - - - - - - - - - - - - - - - - - - - - -
WE VALUE YOUR FEEDBACK!
Please forward Newsletter feedback to:
Lashan Clifton
Tel: +61 8 8303 4617
Email: [email protected]
Contact us with medical or surgical technologies,
procedures, or health programs that are new or
emerging in Australia.
Please forward to: Linda Mundy
Tel: +61 8 8303 6256
Email: [email protected]
Other New and Emerging Technologies
The following additional technologies were considered by the Health Policy Advisory Committee on Technology (HealthPACT) in November 2009.
CervistaTM HPV 16/18 for the identification of strains of the human papillomavirus (HPV) associated with cervical cancer.
Wearable Artificial Kidney (WAK) for portable dialysis for patients with chronic kidney disease.
Total mesometrial resection for early stage cervical cancer.
Percutaneous Aortic Vale Replacement for patients with aortic vale disease [evidence update].
Halo360 circumferential radiofrequency ablation system for patients with Barrett’s Oesophagus [evidence update].
ProACTTM Therapy for male stress urinary incontinence [evidence update].
Percutaneous endoscopic colostomy for patients with colonic dysfunction [evidence update].
LifePort(R) Kidney transporter [evidence update].
NMP22 BladderChekTM for the diagnosis for bladder cancer [evidence update].
Tomotherapy Hi-Art System(R) for radiotherapy planning and treatment for cancer patients [evidence update].
Non-invasive prenatal diagnostic test for trisomy-21 (Down’s Syndrome) [evidence update].
0.2-0.5 Tesla MRI for the detection of arthritis and musculoskeletal disease [evidence update].
Breast Tomosynthesis for breast cancer screening [evidence update].
Narrow band imaging for the improved detection of precancerous lesions during colonoscopy [evidence update].
Further information on the health technologies included in the Bulletin can be accessed on the following link:
http://www.horizonscanning.gov.au
ANZHSN Bulletin
9 Issue 13 December 2009