Embed Size (px)
Citation preview

J Clin Pathol 1991;44:89-93
Laboratory handling of impalpable breast lesions:A review
J S Armstrong, J D Davies
IntroductionWith the accidental discovery of mammo-graphy by Stafford L Warren in 1926(published six years later),' a new tool becameavailable for clinically examining breasts forsmall carcinomas. The use of mammographyin screening for breast cancer was first sugges-ted in 1956,2 and the original trial, the Hospi-tal Insurance Plan (HIP) for women in NewYork, was inaugurated in 1963.3 Since theearly mammograms, an enormous improve-ment in quality has occurred4 making itpossible to detect small and impalpable breastcarcinomas.The implementation of the United King-
dom Breast Screening Programme up to theend of 1990 will result in an estimated 15 000biopsies a year5; of these, at least 40% will beimpalpable lesions,6 localised by the radiolo-gist before surgical excision.
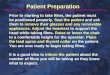
Several radiological methods are availableto guide the surgeon in his or her search formammographic abnormalities. These rangefrom simple painted skin markers such asmethylene blue7 or silver nitrate' to sophis-ticated hooks,9 10 and include the injection ofcoloured dyes." A common mistake is for thepathologist to assume that the marking isprecise. In fact the marker provides only afixed point for reference. The surgeon isdirected to the abnormality by the radiologist,who issues a written report stating the relationof the marker to the abnormality (fig 1).12 Thesurgical excision must be confirmed byspecimen radiology5 and further tissue mayneed to be excised.5
In handling these specimens the pathologistfaces three problems. First, there is often nopalpable or obvious visible abnormality. Thismeans that blocks for histological analysiscannot be selected by usual methods, andtherefore either all the tissue must be blockedor the abnormality needs to be located byanother means. Secondly, any histologicalabnormality detected must correspond to theradiological lesion detected on the originalmammogram which may be rather subtle.Thirdly, histological analysis may indicate aborderline lesion.'3Any method should thus involve block
selection by specimen radiology and primefixation is mandatory. The economic use ofthe laboratory technician and the pathologist'stime also needs to be considered.
General guidelines about specimen hand-ling have been included in the Sloanereports. '4'1' Other recent reviews have placedmore emphasis on logistical and organisational
Figure I Photoradiograph showing a mammolok hook inits final position, lying near to but not within an area ofsuspicious microcalcification (circled).
difficulties.'6 17 Anderson's article dealsparticularly with the problems of specimenhandling.'8 This review details simple prac-tical methods of dealing with impalpablescreened specimens.
Specimen radiologyA whole specimen radiograph needs to beperformed immediately after the biopsyspecimen is resected to confirm removal of theradiographic abnormality. A copy of thespecimen mammogram can be made at thispoint, at minimal extra cost. One copy shouldremain in the patient's notes as a record ofexcision, the second is for the pathologist'suse. A second set of mammograms is per-formed by the pathologist after fixation andslicing of the specimens.Specimen radiograms can be produced in
several ways. The most convenient method isto use a self-contained table-top unit designed
Department ofPathology, RoyalInfirmary,Marlborough Street,Bristol BS2 8HWJ S ArmstrongJ D DaviesCorrespondence to:Dr J D Davies, RegionalBreast Pathology Unit,Southmead Hospital, BristolBS1O 5NB, EnglandAccepted for publication19 July 1990
89
on August 18, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.44.2.89 on 1 February 1991. D
ownloaded from

Armstrong, Davies
for the purpose. Such units include the Faxi-tron 43855A with option A02 (Hewlett-Pack-ard, USA) and the JKJ Micro specimen unit(Xerox Medical Systems, USA). Carefulcalibration of both machines by qualifiedradiographers is essential to obtain optimalperformance, but the machines can beoperated by other staff. These units may besited in the departments of pathology,radiology, or in the operating theatres. If onemachine is situated at a site distant from thepathology department it may be desirable tohave a second machine for the pathologist'suse. For convenience, a rapid process film thatcan be processed automatically by the depart-ment of radiology should be used as thisavoids the problem of maintenance ofindividual processing units.
Individual settings for the machines varyaccording to the thickness and density of thetissue. As a rough guide the voltage should bebetween 25 and 35 kilovolts, and the exposuretime two or three seconds on the Faxitron,and 20 to 40 seconds using the Xeroxmachine. The machine should be calibrated(and maintained) by experienced radio-graphers. A table of settings can be left withthe machine so that laboratory technicians cantake high quality x-ray pictures.
Alternatively a straightforward clinicalmammogram machine can be used by placingthe biopsy specimen directly on to the stageand reducing the exposure time by one half toone quarter of that needed for clinicalmammography.'920 This machine does,however, need to be operated by a qualifiedradiographer. If no clinical mammogrammachine is available adequate visualisation ofmicrocalcification can be obtained on a stan-dard x-ray machine set at a low voltage (LowR, Frenchay Hospital, personal communica-tion). As the technical quality is inferior tomammography, however, this technique is notsuitable for use as a check of surgical excision.It might be useful to the pathologist for takingx ray pictures of the specimen to aid blockselection.
Radiological interpretation will be a newexperience for many pathologists. In theinitial stages guidance may be required fromthe radiologists involved in the screeningprogramme. Some pathologists may find iteasier to compare their specmen mammo-grams with the patients' preoperativemammograms. This will ensure that theabnormality they see in the specimenmammogram is the same as that in the originalfilm.Most mamographic lesions will be areas of
microcalcifications but some will concern softtissue abnormalities, such as distortion of thearchitecture, increased vascularity, or an areaof increased density (fig 2). Microcalcifica-tions vary in their histological appearance.Most are concentrically arranged deposits ofcalcium hydroxyapatite-Ca,0(PO4)6(OH)2-which are readily detected. A few calcificmammographic lesions (composed of Wed-dellite, calcium oxalate dihydrate) are notstained by haematoxylin and eosin and can
Figure 2 Whole specimen mammogram showing twocarcinomas. The hook lies close to an area ofmicrocalcification with the characteristic differences inparticle size and density seen in malignant calcification.The second lesion is the circular soft tissue densityshowing an irregular outline and distortion of thesurrounding tissue. The linear shadow is the skin ellipse.
only be recognised by using cross polarisedlight. These forms are easily overlookedunless the pathologist is alerted to theirpresence.2" 22
Many women requiring biopsies will havemore than one radiographic abnormality butonly one suspicious area. It is vital to takeblocks for histological analysis from thismammographically suspicious area, even ifthere is also an obvious visible or otherradiological abnormality.
Marking of resection marginsDuring the processing of breast biopsyspecimens it is important to mark accuratelythe margins of surgical excision. With the trendtowards conservative treatment for malignantbreast lesions some surgeons require differen-tial marking of the resection margins ofexcisional biopsy specimens. The biopsyspecimen is orientated for the pathologist bythe surgeon using sutures of different colours,or with differing numbers of sutures orknots.2324 If the skin is included the number ofmarking sutures may be reduced by the use ofan orientating arrow painted on the skin.25When marking these specimens it is import-
ant to use a radiolucent material. Unfortu-nately, inorganic artists' pigments," and to a
90
on August 18, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.44.2.89 on 1 February 1991. D
ownloaded from

Impalpable breast lesions
lesser extent, silver nitrate,27 both show up onsliced specimen mammograms, thus confusingradiological detail. India ink is possible but notideal: it is slow to dry and more seriously,spreads into the planes of the underlying con-nective tissue.27 Although drying problemsmay be obviated by mounting India ink inacetone,2829 by itself India ink does not permitidentification of the individual planes ofexcision. The same disadvantage applies toalcian blue30 and TippEx,'1 the latter also beingradio-opaque.
Differential marking of breast biopsyspecimens has previously been achieved usinginorganic artists' pigments,26 but as mentionedabove these are not suitable for subsequentsoft-tissue x ray pictures. We have recentlydeveloped a method of differential markingusing coloured gelatins.32
Methods of localising the mammo-graphic lesionSeveral methods can be used to find an invis-ible abnormality in a biopsy specimen. Thesimplest but most expensive would be toprocess all the tissue. Few laboratories wouldrelish the amount of work generated by thismethod. Some pathologists remain resistant tothe use of x ray pictures to locate the abnor-mality, feeling that this is time consuming. Thetissue around the tip of the hook is thereforeblocked, and if no abnormality is found in theinitial blocks more tissue is taken from thespecimen. This method is only effective if thehook is accurately placed in the abnormal area.We feel that the use of specimen mammo-
graphy to localise the abnormality in the biopsyspecimen before the block is selected is essen-tial. There are two basic methods usingmammography. They are outlined below.
BREAD SLICING METHODSOur modified "bread slicing" technique isbased on the original suggestions by HelenIngleby, dating from the 1930s, for handlingbreast biopsy specimens.33The fresh or partially fixed specimen, along
with a copy of the specimen mammogram isreceived in the laboratory. The specimenmammogram acts as a check of surgicalexcision. The specimen is then examinedmacroscopically and the excision margins iden-tified and marked. After overnight fixation thelesion is bisected along the line of the hook toshow the cut surface and the tip of the hook (fig3). If incision shows a discrete lesion corre-sponding to the mammographic abnormalitythis can be sampled directly. Further slicing isperformed thereafter. This time slicing is per-pendicular to the line ofthe hook and parallel inthe two halves of the biopsy specimen (fig 4).This produces many semicircular slices. Theaim of this is to produce slices thin and smallenough to fit into a cassette. To aid fine slicing ajig can be used."4The numbered slices are then placed in a
compartmentalised container with a lid, whichis filled with formol saline (fig 5). Each slice isthen x rayed.35 After studying the x ray pictures
r -'/
/I- - 7
'-V --ii
.%q. f
K, c'-J.
-I-,
Figure 3 After overnightfixation informol saline thespecimen is bisected along the track of the localisationwire as indicated by the arrow (left). This produces twopieces, one (A) containing the hook, the other (B)without the hook (right).
blocks are taken to include the areas ofmammographic abnormality, the adjacent nor-mal breast, and the resection margins. Anyvisible abnormality can also be sampled. Thesite of all blocks in the specimen should becarefully noted. The specimen can be stored ina plastic bag sealed into individual compart-ments (fig 6).
It has been suggested by some authors thatthis or similar methods are time consuming andinconvenient due to the need for repeatspecimen radiology.'6 We find that in routineuse this is not a real problem.The slicing techniques need no special
equipment other than access to a mammo-
Figure 4 Afterfurther overnightfixation the halves aresectioned at 2-4 mm intervals at 90° to the original cut.The sections are parallel in each half of the biopsyspecimen.
91
_:.- -7=;I -.
"J.-.
on August 18, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.44.2.89 on 1 February 1991. D
ownloaded from

92 Armstrong, Davies
Figure Metal container
with removable dividingstrips. This can be usedfor
transporting the sliced
biopsy specimen to the x-
ray facilities andfor short
term storage.
Figure 6 Sliced specimenafter blocks have beenselectedfor histologicalanalysis. Each slice has aseparate compartment inthe plastic bag, the numberis indicated on its outside.The specimen can be storedindefinitely in this way.
_ _Figure 7 Diagrammaticrepresentation of the gridsystem. The biopsyspecimen is attached to aperspex board, with metalwires running through it,in the operating theatre,and x-rayed on the board.Afterformalinfixation onthe board the tissuefromthe coordinates containingthe abnormality is blockedin its entirety.
graphic machine. Bisecting the lesion and anextra day of formalin fixation provide highquality histological results. Methodologicalslicing and taking x ray pictures mean that agood three dimensional picture of the lesion isobtained, with accurate correlation betweenhistology and radiology. Taking further blocksis extremely straightforward.
GRID METHODSThis approach is based on the principle that theintact specimen is attached to a wooden, card,or perspex board in the operating theatre. Thespecimen mammography is performed on thisboard and sections can then be taken from thespecimen directly. The advantages are thatonly one specimen radiograph needs to beperformed and that the radiologist can indicatethe area to be blocked on the specimenmammogram.Some methods have used tracings of the
abnormality from the x ray picture to localisethe lesion,37 while others use a card or grid withradiodense markings on it to provide a fixedreference point for histological sampling.3638The most sophisticated method consists of
attaching the fresh specimen in the operatingtheatre to a commercially available perspexgrid, which has 1-0 centimetre spaced metalwires running vertically and horizontallythrough it. These are visible as a grid on the xray picture, and blocks can be taken from theradiological abnormality (fig 7).36 The surgeoncan use sutures to indicate which margin iswhich, and appropriate blocks can be takenfrom each.The main advantage of the "grid" method is
the obviation of specimen mammography inthe laboratory. Tissue distortion is also claimedby some to be less than in more traditionalmethods of fixation.36Major disadvantages of the grid method are,
however, the danger ofmovement ofthe biopsyspecimen on the grid between x ray and dissec-tion, and the depth of substantial biopsyspecimens. In addition, there is the difficulty oftaking further blocks. Other logisticalproblems include the need for the surgeons touse the grid and securing an adequate supply inthe operating theatre.
Variations in techniqueIt is probably inappropriate to perform frozensection examination for diagnostic purposes.Techniques are described in the Americanscientific journals for removing representativetissue using radiographically guided biopsy.35This approach most certainly makes the biopsyspecimen difficult to handle subsequently.
If fresh tissue is required for advancedbioassay, immunohistochemical or geneticmethods of examination, it is possible to fineslice the biopsy specimen and to freeze down aproportion of the slices. Unfortunately, thismakes subsequent handling of the biopsyspecimen extremely difficult and is not to berecommended for general use. The relativelysmall size of some biopsy specimens and thestrictly focal nature of borderline lesions andmicroinvasion make the loss of vital diagnostic
tissue a distinct possibility.Gibbs has favoured an entirely different
approach to the examination of breast biopsyspecimens. The biopsy specimen is trans-versely sliced at 5 mm intervals. Specimenmammography is performed and theappropriate slices are processed, sectioned,mounted and stained in their entirety toproduce whole-slice mounts.39"' None the lessit must be pointed out that this procedurerequires the use of a specialised heavymicrotome and the production of high qualitysections for the assessment of possible border-line lesions. Neither requirement is readilyachieved.
Nevertheless, this method clearly has theadvantage of producing a complete section ofthe whole biopsy specimen with a clear recordofthe resection margins. We feel, however, thatthe disadvantages preclude its routine use.Special cassettes and containers for automaticprocessing are needed, and sections are cut on aheavy duty sledge microtome which is tech-nically detnanding. The quality of the sectionsproduced, unless highly skilled technicians areavailable, may be inferior, thus making diag-nosis more difficult. The method has the dualdisadvantages of increased cost and potentiallypoorer quality of the sections.
ConclusionsThe handling of mammographically detectedlesions is a complex and time consumingprocedure whatever method is used. Ifaccurateand meaningful results are to be obtained it isimportant to have a consistent method forhandling these specimens.
It is impossible to process these specimensproperly without specimen radiology. It isessential that the diagnostic blocks are takenfrom the abnormal area identified on theoriginal mammogram by the radiologist.Marking of the surgical resection margins is
necessary, before the lesion is dissected in anyway.As these lesions may be "borderline" good
fixation is vital.We recommend a two-stage bread-slicing
method for handling these specimens, althoughit is a little more time consuming and requires asecond set of specimen radiographs. Theadvantages are the lack of any specialist equip-ment, ease of block selection, excellent correla-tion between the radiology and histology andthe simplicity of taking extra blocks.The use of frozen section diagnosis is not
advised for general use.
We are grateful to Messrs C C Jeal and P Hall for photographicassistance, and to Mr A Armstrong for the line diagrams. Oursincere thanks are also due to Messrs P J Richardson, G Roberts,and their staff in the departments of radiodiagnosis and path-ology at Bristol, respectively, who have willingly and most ablyassisted in the development oftechniques for the examination ofbreast specimens for the past 18 years.
1 Warren SL. A roentgenologic study of the breast. Am JRoentgenol 1932;24: 113-24.
2 Gershon Cohen J, Ingleby H, Moore L. Can mass X-raysurveys be used in the detection of early cancer of thebreast? JAMA 1956;161:1069-72.
on August 18, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.44.2.89 on 1 February 1991. D
ownloaded from

Impalpable breast lesions
3 Shapiro S, Strax P, Venet L. Periodic breast cancer screen-ing in reducing mortality from breast cancer. JAMA1971;215:1777-85.
4 Anonymous: Breast Cancer Screening. Lancet 1987;i:543-4.
5 Forrest APM. Breast cancer screening: Report to the HealthMinisters of England, Wales, Scotland and NorthernIreland. London: HMSO, 1986.
6 Holmberg L, Adami H, Lundstrom T. Demands oninpatient services after mass mammographic screening. BrMed J 1986;293:779-82.
7 Preece PE, Gravelle IH, Hughes LE, Baum M, Fortt RW,Leopold JG. The operative management of subclinicalbreast cancer. Clin Oncol 1977;3:165-9.
8 Frankl G, Rosenfield DD. Xeroradiographic detection ofoccult breast cancer. Cancer 1975;35:542-8.
9 Chetty AE, Kirkpatrick AE, Anderson TJ, et al. Localisa-tion and excision of occult breast lesions. Br J Surg1983;70:607-10.
10 Homer MJ. Localisation of nonpalpable breast lesions withthe curved-end retractable wire. Am J Roentgenol 1988;151:919-20.
11 Frank HA, Hall FM, Steer ML. Preoperative localization ofnonpalpable breast lesions demonstrated by mammogra-phy. N EngI J Med 1976;295:259-60.
12 Reidy JF. Preoperative localisation of impalpable breastlesions. Bristol Med-Chir J 1989;104:43-5.
13 Page DL, Anderson TJ. Diagnostic histopathology of thebreast. Edinburgh: Churchill Livingstone 1987:120-57.
14 Sloane JP and members of the Royal College of Pathologists'Working Group. National Health Service breast screeningprogramme: guidelines for pathologists. Oxford: ScreeningPublications, 1990.
15 Sloane JP and members of the Royal College of Pathologists'Working Group. National Health Service breast screeningprogramme: pathology reporting in breast cancer screening.Oxford: Screening Publications, 1990.
16 Elston CW. The United Kingdom national breast screeningprogramme: implications for pathology departments. MedLab Sci 1989;46:223-9.
17 Elston CW, Ellis IO. Pathology and breast screening.Histopathology 1990;16:109-18.
18 Anderson TJ. Breast cancer screening: Principles and prac-ticalities for histopathologists. Recent advances in his-topathology 14. Edinburgh: Churchill Livingstone, 1989.
19 Davies JD, Roberts G, Richardson PJ. A serial whole-organslicing technique for examining surgically resectedbreasts. J Clin Pathol 1973;26:891-2.
20 Richardson PJ. The radiographic examination of slicedsurgically resected breasts. Radiography 1975;41:37-40.
21 Going JJ, Anderson TJ, Crocker PR, Levison DA. Wed-dellite calcification in the breast: eighteen cases withimplications for breast cancer screening. Histopathology1990;16:1 19-24.
22 Frappart L, Remy I, Lin HC, et al. Different types ofmicrocalcifications observed in breast pathology.Virchows Arch (Pathol Anat) 1986;410:179-87.
23 Davies JD. Pathology and screened breast lesions. CurrPract Surg 1989;1:147-51.
24 Fisher ER, et al. Pathologic findings from the nationalsurgical adjuvant breast project (Protocol 6). Cancer1986;57:1717-24.
25 Lawrence RD, Fox IS, Wood J. Mastectomy orientationarrow. Ant J Surg Pathol 1986;10:894.
26 Paterson DA, Davies JD. Marking planes of surgicalcxcision on breast biopsy specimens: use of artists' pig-ments suspended in acetone. J Clin Pathol 1988;41:1013-16.
27 Bogomoletz VW, Davies JD. Examination of breastspecimens. Association of Clinical Pathologists Broad-sheet 116 London: AC P/B MA, 1987.
28 Chan KW, Lui I, Chung WB. Marking planes of surgicalexcision with a mixture of India Ink and acetone. J ClinPathol 1989;42:893.
29 Davies JD, Armstrong JS, Paterson DA. Marking planes ofsurgical excision on specimens with mixture of India Inkand acetone. J Clin Pathol 1989;42:893.
30 Birch PJ, Jeffery MJ, Andrews MIJ. Alcian blue: a reliablerapid method for marking resection margins. J Clin Pathol1990;43:608-9.
31 Harris MD. Tipp-Ex: a novel marker for resection margins.J Pathol 1990;160:168.
32 Armstrong JS, Wiensweig P, Davies JD. Differential mark-ing excision planes of breast lesions by coloured gelatin. JClin Pathol 1990;43:604-7.
33 Ingleby H, Holly C. A method for the preparation of serialslices of the breast. J Tech Methods 1939;19:93-6.
34 Going JJ, Anderson TJ. Optimal handling of breast carcin-omas and breast localisation biopsies. J Pathol1989;157:164.
35 Rosen PP, Snyder RE, Robbins G. Specimen radiology fornonpalpable breast lesions found by mammography:procedures and results. Cancer 1974;34:2028-33.
36 Champ CS, Mason CH, Coghill SB, Robinson M. A perspexgrid for localisation of non-palpable mammographiclesions in breast biopsies. Histopathology 1989;14:311-5.
37 Stamp GWH, McDicken IW, Whitehouse GH. Histologicallocalisation of mammographic abnormalities in breastbiopsy specimens. J Clin Pathol 1982;30:1163-5.
38 Bentley PC. A simple specimen mount for the orientation ofbreast biopsies. Br J Surg 1989;76:312.
39 Gibbs NM. Large paraffin sections and chemical clearanceof axillary tissues as a routine procedure in the path-ological examination of the breast. Histopathology 1982;6:647-60.
40 Gad A. Screening for breast cancer: examination andreporting of histopathological preparations. Lancet 1988;ii:953.
93
on August 18, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.44.2.89 on 1 February 1991. D
ownloaded from





![RESEARCH ARTICLE Open Access Clinical and histological ...histochemistry (IHC) on formalin-fixed tissue samples may be an alternative test to confirm the diagnosis [26]. A study conducted](https://img.pdfslide.net/doc/110x75/5e8180c591c8c36d2d51f36b/research-article-open-access-clinical-and-histological-histochemistry-ihc.jpg)