Embed Size (px)
Citation preview
Jan LodderRob P.W. Rouhl, Robert J. van Oostenbrugge, Jan Damoiseaux, Jan-Willem Cohen Tervaert and
and Therapeutical ConceptsEndothelial Progenitor Cell Research in Stroke : A Potential Shift in Pathophysiological
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 2008 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/STROKEAHA.107.507251
2008;39:2158-2165; originally published online May 1, 2008;Stroke.
http://stroke.ahajournals.org/content/39/7/2158World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer process is available in the
Request Permissions in the middle column of the Web page under Services. Further information about thisOnce the online version of the published article for which permission is being requested is located, click
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Strokein Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on February 23, 2013http://stroke.ahajournals.org/Downloaded from
Endothelial Progenitor Cell Research in StrokeA Potential Shift in Pathophysiological and Therapeutical Concepts
Rob P.W. Rouhl, MD; Robert J. van Oostenbrugge, MD, PhD; Jan Damoiseaux, PhD;Jan-Willem Cohen Tervaert, MD, PhD; Jan Lodder, MD, PhD
Background and Purpose—Stroke is the leading cause of disability in the Western world; however, few therapies are athand to decrease this burden.
Summary of Review—Endothelial progenitor cells (EPCs) have been introduced in cardiovascular medicine as factotums.EPCs can repair damaged endothelium and attenuate the development and progression of atherosclerosis. Also, EPCscan form new vessels in ischemic areas and thus promote recovery after ischemic events. In stroke, however, EPCresearch is limited. In our overview, we provide background information on EPC use as a risk marker and as a potentialtherapeutic agent.
Conclusion—In our opinion, the lack of EPC studies in stroke should instigate vascular neurologists to participate in EPCresearch, as EPCs could also change pathophysiological concepts and improve clinical treatments in vascular neurology.(Stroke. 2008;39:2158-2165.)
Key Words: angiogenesis � atherosclerosis � cerebral infarct � endothelium � endothelial progenitor cells
Endothelial progenitor cells (EPCs) are immature endothelialcells which circulate in peripheral blood. These cells were
first described by Asahara et al.1 In their study, EPCs wereisolated from human blood and injected into animals with limbischemia. Subsequently, EPCs were found in the endothelium ofnewly formed vessels in ischemic regions, indicating that thereare cells in the human blood which were involved in theformation of new vessels after ischemia.
In another study, Griese et al injected EPCs into animalswith carotid balloon injury (a model of endothelial damage).After healing of the injury, EPCs were found in the recoveredendothelium,2 indicating that EPCs were also involved in therepair of damaged endothelium.
The regenerative potential of EPCs suggested by thesefindings has led to different clinical studies, based on thefollowing 2 hypotheses: (1) Patients with lower EPCnumbers are at higher risk for atherosclerotic events, and(2) patients with ischemic events may benefit from EPCadministration.
In the present overview, we will elaborate on these 2 clinicalhypotheses and provide background information of EPC char-acteristics, measurement, and use as a therapeutic agent. We willthen focus on EPCs in cerebrovascular disease. Unfortunately,most studies which are published up till now are small andperformed in animals or highly selected patients. Therefore,results have to be interpreted with caution.
EPC Characteristics and MeasurementEPCs are maturating cells, derived from immature stem cells.They enter peripheral blood in specific circumstances (seebelow). They are halfway in their maturation process tobecome endothelial cells. Therefore, EPCs possess functionaland structural characteristics of both stem cells and matureendothelial cells (see Table 1). During their development,EPCs gradually lose stem cell characteristics and progres-sively gain endothelial cell characteristics. Consequently, thespecific set of characteristics of an EPC on a given time pointdepends on its degree of maturation. For quantification, EPCsmust be defined accurately. Therefore, the combination ofstructural and functional characteristics should be carefullychosen to exclude other immature stem cells or matureendothelial cells.
There are 2 different quantification techniques. First, cellculture (lower part of Figure 1): isolated mononuclear cellsfrom peripheral blood are cultured for several days inconditions which selectively favor growth of EPCs. Theseconditions include coating of plates with macromolecules likegelatin and addition of endothelial growth factors to theculture medium. Therefore, quantification of EPCs byculture also depends on the EPC function (EPCs have to beviable and to be able to respond to the culture conditions; seeTable 1). EPCs form clusters from the third day on, and theseclusters are counted after 7 to 28 days. Further testing toconfirm the endothelial phenotype of the cells involves
Received October 16, 2007; final revision received November 30, 2007; accepted December 13, 2007.From the Departments of Neurology (R.P.W.R., R.J.v.O., J.L.) and Internal Medicine, Division of Clinical and Experimental Immunology (J.D.,
J.W.C.T.), University Hospital Maastricht, The Netherlands.Correspondence to R.P.W. Rouhl, Department of Neurology, University Hospital Maastricht, PO Box 5800, 6202 AZ Maastricht, The Netherlands.
E-mail [email protected]© 2008 American Heart Association, Inc.
Stroke is available at http://stroke.ahajournals.org DOI: 10.1161/STROKEAHA.107.507251
2158
Comments, Opinions, and Reviews
by guest on February 23, 2013http://stroke.ahajournals.org/Downloaded from
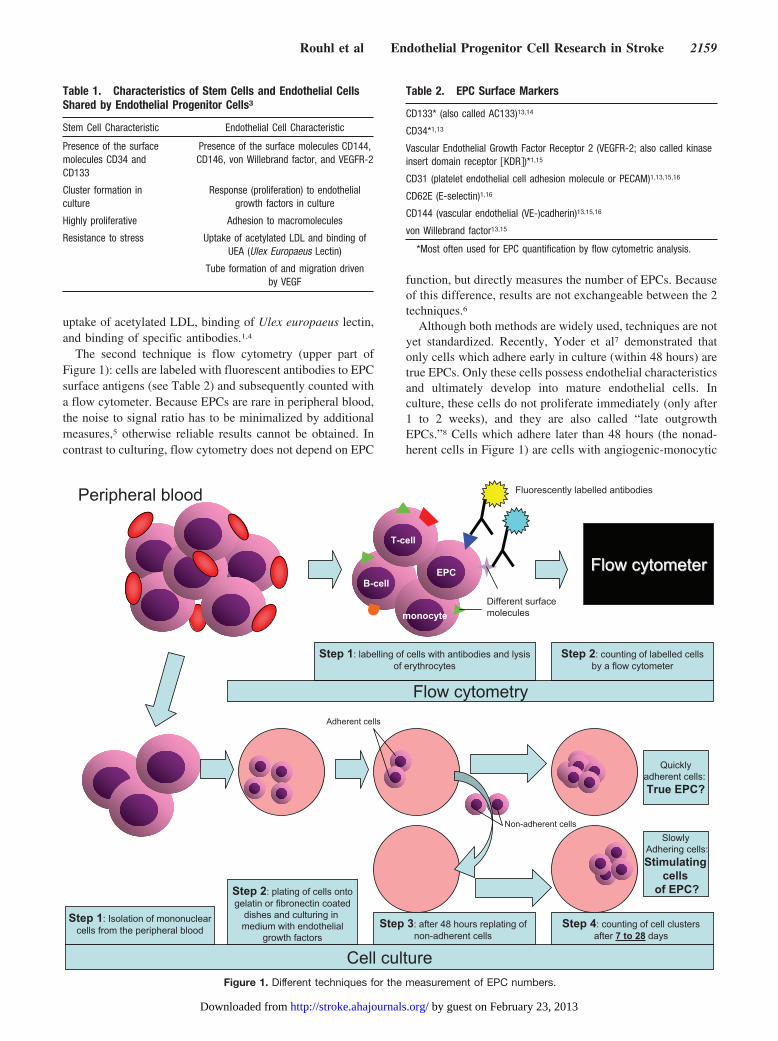
uptake of acetylated LDL, binding of Ulex europaeus lectin,and binding of specific antibodies.1,4
The second technique is flow cytometry (upper part ofFigure 1): cells are labeled with fluorescent antibodies to EPCsurface antigens (see Table 2) and subsequently counted witha flow cytometer. Because EPCs are rare in peripheral blood,the noise to signal ratio has to be minimalized by additionalmeasures,5 otherwise reliable results cannot be obtained. Incontrast to culturing, flow cytometry does not depend on EPC
function, but directly measures the number of EPCs. Becauseof this difference, results are not exchangeable between the 2techniques.6
Although both methods are widely used, techniques are notyet standardized. Recently, Yoder et al7 demonstrated thatonly cells which adhere early in culture (within 48 hours) aretrue EPCs. Only these cells possess endothelial characteristicsand ultimately develop into mature endothelial cells. Inculture, these cells do not proliferate immediately (only after1 to 2 weeks), and they are also called “late outgrowthEPCs.”8 Cells which adhere later than 48 hours (the nonad-herent cells in Figure 1) are cells with angiogenic-monocytic
T-cell
EPC
monocyte
B-cellFlowFlow cytometercytometer
Flow cytometry
Cell culture
Fluorescently labelled antibodies
Different surfacemolecules
Step 1: labelling of cells with antibodies and lysisof erythrocytes
Step 2: counting of labelled cellsby a flow cytometer
Step 1: Isolation of mononuclearcells from the peripheral blood
Step 2: plating of cells ontogelatin or fibronectin coated
dishes and culturing in medium with endothelial
growth factorsStep 3: after 48 hours replating of
non-adherent cellsStep 4: counting of cell clusters
after 7 to 28 days
Adherent cells
Non-adherent cells
Quicklyadherent cells: True EPC?
SlowlyAdhering cells:Stimulating
cellsof EPC?
Peripheral blood
Figure 1. Different techniques for the measurement of EPC numbers.
Table 1. Characteristics of Stem Cells and Endothelial CellsShared by Endothelial Progenitor Cells3
Stem Cell Characteristic Endothelial Cell Characteristic
Presence of the surfacemolecules CD34 andCD133
Presence of the surface molecules CD144,CD146, von Willebrand factor, and VEGFR-2
Cluster formation inculture
Response (proliferation) to endothelialgrowth factors in culture
Highly proliferative Adhesion to macromolecules
Resistance to stress Uptake of acetylated LDL and binding ofUEA (Ulex Europaeus Lectin)
Tube formation of and migration drivenby VEGF
Table 2. EPC Surface Markers
CD133* (also called AC133)13,14
CD34*1,13
Vascular Endothelial Growth Factor Receptor 2 (VEGFR-2; also called kinaseinsert domain receptor �KDR�)*1,15
CD31 (platelet endothelial cell adhesion molecule or PECAM)1,13,15,16
CD62E (E-selectin)1,16
CD144 (vascular endothelial (VE-)cadherin)13,15,16
von Willebrand factor13,15
*Most often used for EPC quantification by flow cytometric analysis.
Rouhl et al Endothelial Progenitor Cell Research in Stroke 2159
by guest on February 23, 2013http://stroke.ahajournals.org/Downloaded from

characteristics.9 These cells promote the functioning andoutgrowth of the EPCs by production of growth factors but donot mature into endothelial cells themselves. In culture, thesecells proliferate rapidly (after 1 to 2 days), and therefore, arealso called “early outgrowth EPCs.”8 Thus, in culture, at least2 different cell populations have characteristics of EPCs, butonly the population which adheres within the first 48 hourstruly becomes endothelial.
In addition, there is also discussion how to characterizeEPCs by flow cytometric analysis. Most important question iswhether CD34 should be included. Popa et al10 demonstratedthat cells with the surface marker CD34 (CD34�) arepossibly not true EPCs but only potent regulators of forma-tion of new vessels. These CD34� cells possibly resemblethe late adhering angiogenic cells demonstrated by Yoder etal7 in the culture technique. Furthermore, the process of invitro vascular tube formation was only enhanced if CD34�and CD34� cells were cocultured.11 Also, injection ofCD34� in combination with CD34� into animals withvascular injury led to more neovascularization than wheneither cell group alone was administered.12 From thesestudies, we suggest that CD34 potentially is not a crucialmarker for EPCs. In conclusion, 2 techniques are used toquantify EPCs. Results from flow cytometric and culturestudies are, however, not interchangeable and cannot beinterpreted without knowledge of the limitations of thesetechniques.
EPCs in Cardiovascular Risk AssessmentIn 2 prognostic studies, EPC numbers were found to berelated to cardiovascular risk. Werner et al17 followed 519stable coronary artery disease (CAD) patients for 12 monthsand found lower EPC numbers (in flow cytometry and in asubgroup in culture) in patients with a cardiovascular eventthan in event free patients. Schmidt-Lucke et al18 found in 77stable CAD patients and 43 disease free controls that lowerEPC numbers (in flow cytometry) related to a higher cardio-vascular event rate during 10 months follow-up. The inde-pendent association of lower EPC number with cardiovascu-lar prognosis strongly suggests that EPCs are a risk markerfor future cardiovascular events.
Are EPC measurements a more accurate vascular riskassessment than currently used clinico-epidemiological fac-tors? Unfortunately, there are some major caveats. First, EPCquantification is laborious. Second, for both culture and flowcytometric technique neither a golden standard methodologynor an international standard preparation enabling reliablecalibration is available.4,19 Third, slight modifications intechnique could result in the measurement of different (non-EPC) cell populations. Fourth, results from both techniquesare not exchangeable. Fifth, EPC quantification should not beperformed shortly after a vascular event, because EPC num-bers rise in response to ischemia (see next paragraph).Therefore, EPC numbers in the stable phase could be moreimportant for risk assessment than in an acute phase after avascular event. Finally, “normal” values of EPC numbers areunknown. So, we think that implementation of EPC quanti-fication as accurate vascular risk marker in standard medicine
will take some time, and published EPC studies need confir-mation by more research groups.
Furthermore, other questions have to be answered first: (1)does combination of the 2 EPC quantification techniquesresult in better risk assessment? (2) is EPC quantificationsuperior to other methods of risk assessment using highsensitivity C-Reactive Protein or Intima-Media Thicknessmeasurements? and (3) is there a pathophysiological mecha-nism behind the association between lower numbers of EPCsand a higher cardiovascular risk? Finally, it is pivotal to knowwhether an increase of low EPC numbers will also result inreduction of cardiovascular events. Until these questions areanswered, EPC measurement for vascular risk assessmentwill not be routinely performed in cardiovascular patients.
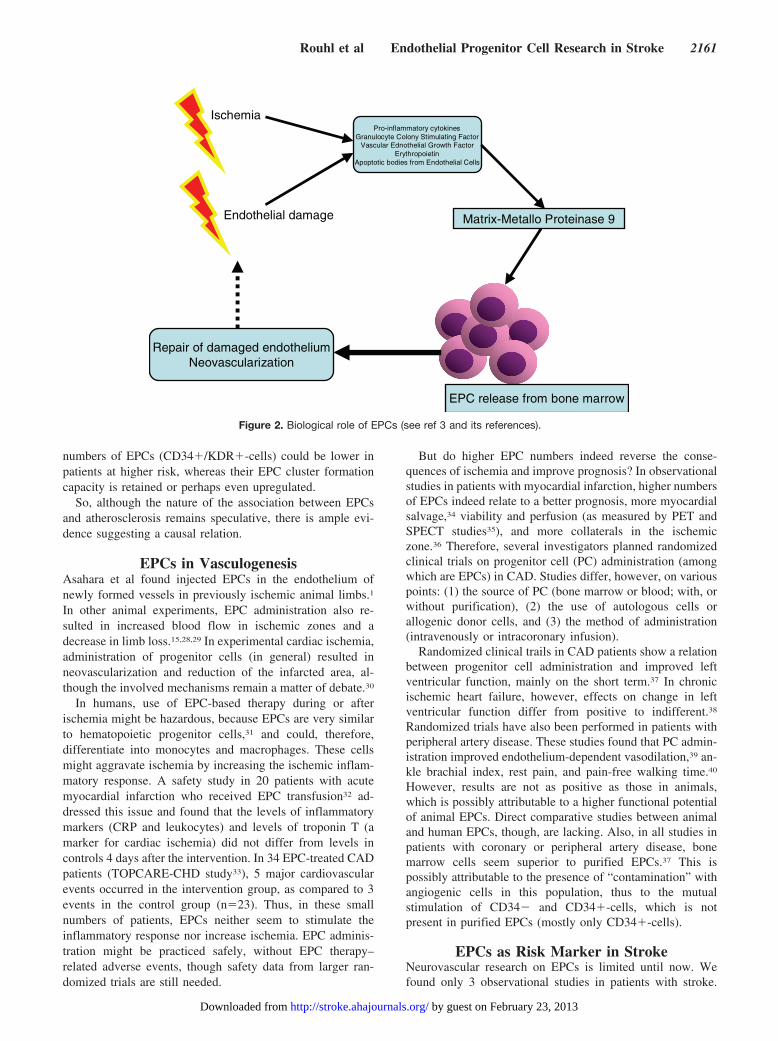
EPC Biology and AtherosclerosisThe nature of the association between lower EPC numbersand increased risk for cardiovascular events20 remains spec-ulative. Generally, it is interpreted as a causal one. BecauseEPC offspring is present in restored endothelium,2,21–23 EPCsare thought to repair damaged endothelium (see Figure 2).Damaged endothelium is, next to ischemia, responsible forEPC recruitment from the bone marrow (see Figure 2).Proinflammatory cytokines, granulocyte-colony stimulatingfactor, erythropoietin, and apoptotic bodies from endothelialcells all stimulate the release of EPCs into the circulation.3,4
Thus, in an acute stage after a vascular event, EPC numbersrise.
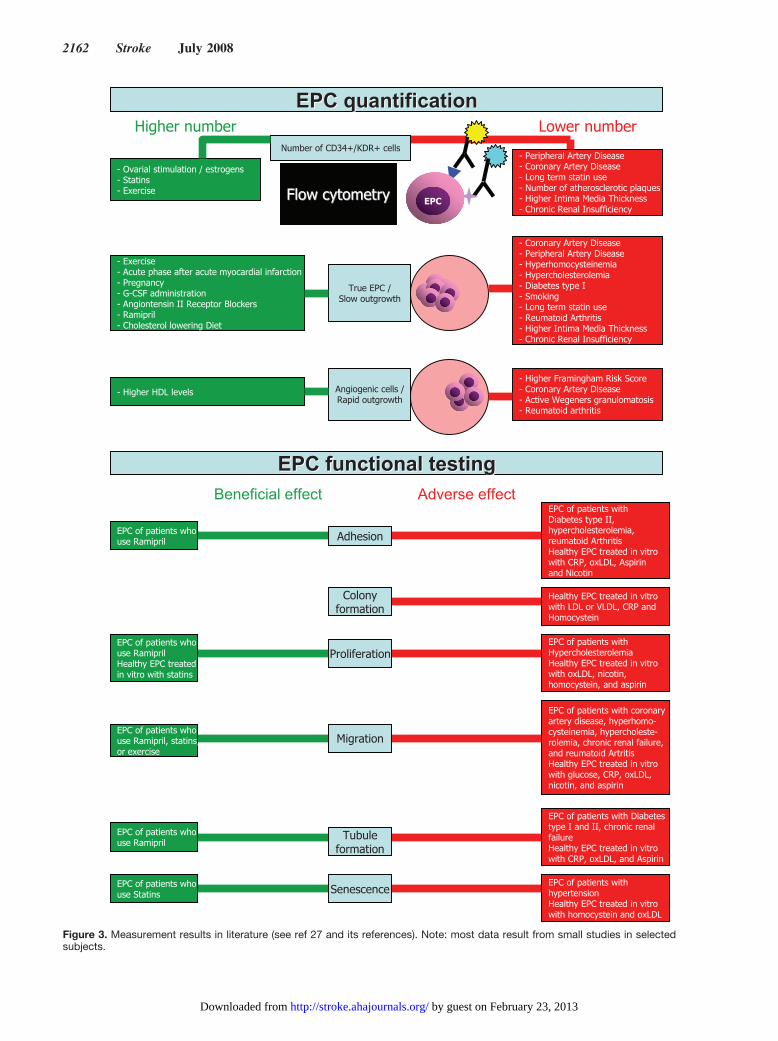
In a stable clinical condition, however, EPC numbers areinfluenced by several factors (see Figure 3). Interestingly,lower EPC numbers relate to different atherosclerotic riskfactors. It is, therefore, generally assumed that lower EPCnumbers reflect a higher consumption of EPCs for restorationof endothelial damage. Indeed, in patients with active vascu-litis, a disease with wide-spread endothelial damage, very lowEPC numbers are found.24 Damaged endothelium plays a rolein atherosclerotic lesion formation and progression; it stimu-lates a proatherogenic inflammatory response, mediated bymonocytes, macrophages, and T-cells.25 EPC numbers couldtherefore be lower as a consequence of a higher consumption,and run relatively short on restoring the damaged endotheli-um with consequent atherosclerosis and cardiovascularevents. Moreover, not only the number of EPCs is related tocardiovascular risk factors but also a disturbed EPC function.This association between lower results on functional EPCtests (see Figure 3) and atherosclerotic risk factors suggests adisturbance in the EPC itself. However, in a recentpopulation-based study in 542 subjects, higher EPC numbers(counted after 5 days in culture) correlated with lower age anduse of cardiovascular drugs. Higher EPC numbers were foundin subjects with higher Framingham Risk Scores.26 Thisseems to reject the hypothesis that lifestyle and cardiovascu-lar risk factors (indirectly) deplete the EPC resources. How-ever, these results may be explained by a lower expression ofrisk factors in the study population attributable to the subjectselection procedure. Possibly, the result even reflects thehealthy status of the participants with a higher potential ofEPC production as appropriate compensation mechanism.The authors do not present flow cytometric data; absolute
2160 Stroke July 2008
by guest on February 23, 2013http://stroke.ahajournals.org/Downloaded from
numbers of EPCs (CD34�/KDR�-cells) could be lower inpatients at higher risk, whereas their EPC cluster formationcapacity is retained or perhaps even upregulated.
So, although the nature of the association between EPCsand atherosclerosis remains speculative, there is ample evi-dence suggesting a causal relation.
EPCs in VasculogenesisAsahara et al found injected EPCs in the endothelium ofnewly formed vessels in previously ischemic animal limbs.1
In other animal experiments, EPC administration also re-sulted in increased blood flow in ischemic zones and adecrease in limb loss.15,28,29 In experimental cardiac ischemia,administration of progenitor cells (in general) resulted inneovascularization and reduction of the infarcted area, al-though the involved mechanisms remain a matter of debate.30
In humans, use of EPC-based therapy during or afterischemia might be hazardous, because EPCs are very similarto hematopoietic progenitor cells,31 and could, therefore,differentiate into monocytes and macrophages. These cellsmight aggravate ischemia by increasing the ischemic inflam-matory response. A safety study in 20 patients with acutemyocardial infarction who received EPC transfusion32 ad-dressed this issue and found that the levels of inflammatorymarkers (CRP and leukocytes) and levels of troponin T (amarker for cardiac ischemia) did not differ from levels incontrols 4 days after the intervention. In 34 EPC-treated CADpatients (TOPCARE-CHD study33), 5 major cardiovascularevents occurred in the intervention group, as compared to 3events in the control group (n�23). Thus, in these smallnumbers of patients, EPCs neither seem to stimulate theinflammatory response nor increase ischemia. EPC adminis-tration might be practiced safely, without EPC therapy–related adverse events, though safety data from larger ran-domized trials are still needed.
But do higher EPC numbers indeed reverse the conse-quences of ischemia and improve prognosis? In observationalstudies in patients with myocardial infarction, higher numbersof EPCs indeed relate to a better prognosis, more myocardialsalvage,34 viability and perfusion (as measured by PET andSPECT studies35), and more collaterals in the ischemiczone.36 Therefore, several investigators planned randomizedclinical trials on progenitor cell (PC) administration (amongwhich are EPCs) in CAD. Studies differ, however, on variouspoints: (1) the source of PC (bone marrow or blood; with, orwithout purification), (2) the use of autologous cells orallogenic donor cells, and (3) the method of administration(intravenously or intracoronary infusion).
Randomized clinical trails in CAD patients show a relationbetween progenitor cell administration and improved leftventricular function, mainly on the short term.37 In chronicischemic heart failure, however, effects on change in leftventricular function differ from positive to indifferent.38
Randomized trials have also been performed in patients withperipheral artery disease. These studies found that PC admin-istration improved endothelium-dependent vasodilation,39 an-kle brachial index, rest pain, and pain-free walking time.40
However, results are not as positive as those in animals,which is possibly attributable to a higher functional potentialof animal EPCs. Direct comparative studies between animaland human EPCs, though, are lacking. Also, in all studies inpatients with coronary or peripheral artery disease, bonemarrow cells seem superior to purified EPCs.37 This ispossibly attributable to the presence of “contamination” withangiogenic cells in this population, thus to the mutualstimulation of CD34� and CD34�-cells, which is notpresent in purified EPCs (mostly only CD34�-cells).
EPCs as Risk Marker in StrokeNeurovascular research on EPCs is limited until now. Wefound only 3 observational studies in patients with stroke.
Pro-inflammatory cytokinesGranulocyte Colony Stimulating Factor
Vascular Ednothelial Growth FactorErythropoietin
Apoptotic bodies from Endothelial Cells
Matrix-Metallo Proteinase 9
EPC release from bone marrow
Repair of damaged endotheliumNeovascularization
Ischemia
Endothelial damage
Figure 2. Biological role of EPCs (see ref 3 and its references).
Rouhl et al Endothelial Progenitor Cell Research in Stroke 2161
by guest on February 23, 2013http://stroke.ahajournals.org/Downloaded from
FlowFlow cytometrycytometry
Number of CD34+/KDR+ cells
- Ovarial stimulation / estrogens- Statins- Exercise
- Peripheral Artery Disease- Coronary Artery Disease- Long term statin use- Number of atherosclerotic plaques- Higher Intima Media Thickness- Chronic Renal Insufficiency
True EPC /Slow outgrowth
- Exercise- Acute phase after acute myocardial infarction- Pregnancy- G-CSF administration- Angiontensin II Receptor Blockers- Ramipril- Cholesterol lowering Diet
- Coronary Artery Disease- Peripheral Artery Disease- Hyperhomocysteinemia- Hypercholesterolemia- Diabetes type I- Smoking- Long term statin use- Reumatoid Arthritis- Higher Intima Media Thickness- Chronic Renal Insufficiency
EPC
Angiogenic cells /Rapid outgrowth
- Higher HDL levels- Higher Framingham Risk Score- Coronary Artery Disease- Active Wegeners granulomatosis- Reumatoid arthritis
EPCEPC functionalfunctional testingtesting
Migration
EPCEPC quantificationquantificationHigher number Lower number
MigrationMigrationMigrationMigration
EPC of patients whouse Ramipril
EPC of patients whouse RamiprilHealthy EPC treatedin vitro with statins
EPC of patients whouse Ramipril, statins,or exercise
EPC of patients withhypertensionHealthy EPC treated in vitrowith homocystein and oxLDL
EPC of patients with Diabetes type I and II, chronic renalfailureHealthy EPC treated in vitrowith CRP, oxLDL, and Aspirin
EPC of patients with coronaryartery disease, hyperhomo-cysteinemia, hypercholeste-rolemia, chronic renal failure,and reumatoid ArtritisHealthy EPC treated in vitrowith glucose, CRP, oxLDL,nicotin, and aspirin
EPC of patients withHypercholesterolemiaHealthy EPC treated in vitrowith oxLDL, nicotin, homocystein, and aspirin
EPC of patients withDiabetes type II, hypercholesterolemia, reumatoid ArthritisHealthy EPC treated in vitrowith CRP, oxLDL, Aspirinand Nicotin
Healthy EPC treated in vitrowith LDL or VLDL, CRP and Homocystein
MigrationMigration
Senescence
Tubuleformation
Migration
Proliferation
Adhesion
Colonyformation
Beneficial effect Adverse effect
EPC of patients whouse Ramipril
EPC of patients whouse Statins
Figure 3. Measurement results in literature (see ref 27 and its references). Note: most data result from small studies in selectedsubjects.
2162 Stroke July 2008
by guest on February 23, 2013http://stroke.ahajournals.org/Downloaded from

Taguchi et al41 measured CD34�-cells by flow cytometry in25 patients with an ischemic stroke. They found peak valuesafter 7 days, and values similar to baseline (as measuredshortly after stroke) after 30 days. Higher CD34�-cell-levelsat 30 days related to higher numbers of infarcts on magneticresonance imaging and also to cerebrovascular function asmeasured with positron emission tomography scanning (ce-rebral metabolic rate of oxygen, and cerebral blood flow).Ghani et al42 reported a decreased number of clusters ofrapidly adhering cells after stroke and in “stable cerebrovas-cular disease,” compared to controls free of vascular disease.Higher age and the presence of cerebrovascular disease ingeneral independently related to lower EPC numbers. Unfor-tunately, the authors did not match controls for age. Further-more both studies lack methodological design for conclusionsregarding a causal role of EPCs in cerebrovascular disease.
For future studies on the role of EPCs in stroke, severalcaveats have to be borne in mind. First, general recommen-dations (like basing sample sizes on appropriate powercalculations, correction for possible confounders (see Figure2), and the inclusion of healthy controls43), have to befulfilled. Second, the laboratory technique of EPC quantifi-cation should be standardized as much as possible. Becausethere is no standard protocol at hand, one single method,preferably after discussion with an experienced center in EPCresearch, should be chosen. Also, the timing of blood sam-pling (directly after the stroke or in a stable phase) should beconsidered, as values in the acute stage could differ fromthose in a chronic phase. Third, and probably most important,different stroke causes have to be distinguished, becauseendothelial involvement in the pathogenesis of differentforms of stroke could be different.
EPCs may be considered as a marker for endothelialinvolvement. In atherosclerotic ischemic stroke the pathogen-esis of the vascular occlusion is more or less similar to that incoronary and peripheral artery disease. Therefore, EPCscould be a marker of future events in atherosclerotic strokeand a marker of the endothelial repair mechanism. Cardio-embolic stroke, though, has a different pathogenesis (withdifferent endothelial involvement), and consequently EPCquantification may be less significant as a risk marker. EPCsmight also differentiate between endothelially mediated andnonendothelially mediated causes of stroke.
EPCs as Therapeutic Agent in StrokeUp till now, studies on EPCs as a therapeutic agent have beenreported in animal stroke models. A variety of human celltypes (neural stem cells, immortalized neural cell lines, andhematopoeitic progenitor cells) have already been tested inanimals.44 Use of cells derived from peripheral blood or bonemarrow, among which are the EPCs, has 2 main advantagesabove the other cell types. First it avoids ethical limitations(because there is no need to work with fetal or embryonictissue). Second, there is a host of experience on use ofhematopoeitic progenitor cells in hemato-oncology, andtherefore a lot is known about tolerability and side effects oftreatment.
In an observational study in mice, higher EPC numbersrelated to physical exercise, a better functional motor out-
come after middle cerebral artery occlusion, increased neo-vascularization and enhanced blood flow in ischemic zones.45
In 48 stroke patients, Sobrino et al46 demonstrated that anobserved increase of EPC cluster numbers 7 and 90 days aftera stroke also related to a good functional outcome. Experi-mental administration of EPCs in animals furthermore in-duces an increase in the formation of new blood vessels andalso of blood flow in cerebral ischemia.47 However, fewtransplanted cells are actually found in the brain,44 and thesecells are only infrequently of endothelial phenotype.48
Does this formation of new vessels result in a better strokerecovery? Other neovascularization stimulating agents (likeVEGF and other growth factors) administered several daysafter stroke potentially improve outcome by decreasing theischemic penumbra.49 Importantly, however, these agentsalso cause an increase in endothelial permeability resulting inbrain edema.49 Neovascularization thus seems important inrecovery, but the adverse effects of neovascularization stim-ulating agents cause some concern. Whether neovasculariza-tion by EPCs improves stroke outcome is not known, thoughEPCs could be a valuable alternative for neovascularizationstimulating agents. Furthermore, the beneficial effects ofEPCs in the brain are probably not limited to neovascular-ization. In an observational study in rats with experimentalstroke, neovascularization related to neurogenesis (from neu-ral progenitor cells present in the brain), and also to migrationof these neural progenitor cells along the newly formedvessels.50 VEGF plays a regulating role in this process ofneurogenesis and angiogenesis in the brain.51 After experi-mental progenitor cell administration in rats, VEGF levelswere higher in the ischemic border zone,52 whereas neuro-genesis and angiogenesis were reciprocally increased in thiszone.53 Thus, administered (endothelial) progenitor cells mayenhance the proliferation of endogenous neuronal progenitorcells in the brain. This pathway could be more important thanangiogenesis itself, as the EPC-induced vessels are those ofsmall calibre (capillaries), insufficient to restore large perfu-sion defects. Next to this paracrine stimulation of neurogen-esis, progenitor cells can also adapt neural characteristicsthemselves. However, in animal experiments incorporationinto neuronal circuits of these cells seemed unlikely.54 Inde-pendent of the possible mechanism of action, the intravenousadministration of human umbilical cord blood (a rich sourceof various progenitor cells, among which are EPCs) led tobetter recovery of motor function in rats.55,56
There are more potential benefits of EPCs for patients withcerebrovascular disease. Next to the potential effects of EPCsin acute cerebral ischemia, EPCs could be of benefit forpatients with leukoaraiosis and vascular dementia. In endo-thelial cells that are found in white matter lesion vessels,markers of endothelial and microglial activation, and immu-noreactivity to hypoxia-inducible factors are elevated.57 Allthese changes relate to a chronic hypoxic state. Also, endo-thelial injury and breakdown of the blood-brain barrier havebeen implicated in the pathogenesis of leukoaraiosis anddementia.58 Moreover, EPCs might reverse the hypoxic stateby neovascularization and restore the endothelial injury andin these 2 ways prevent the progression of leukoaraiosis.
Rouhl et al Endothelial Progenitor Cell Research in Stroke 2163
by guest on February 23, 2013http://stroke.ahajournals.org/Downloaded from

There is some evidence that suggests that EPCs areinvolved in attenuating the progression of leukoaraiosis.Patients who take ACE-inhibitors, which increase circulatingEPC numbers, show less progression of white matter lesionsin the PROGRESS study.59 Of course, this effect could alsobe attributable to a blood pressure lowering effect. BecauseEPC numbers were not measured in this study, we areuncertain what caused the effect on the progression.
Should clinical trials on EPC injection in cerebrovasculardisease be started? EPCs seem safe in cardiac studies, butcerebral vessels and cerebral ischemia react differently, asalso evidenced by the potentially deleterious brain edema instudies that enhanced cerebral neovascularization with VEGF.49
Furthermore, the role of EPCs in the pathophysiology ofcerebrovascular disease is no more than speculative at pres-ent. Therefore, it seems wise to plan more studies on the roleof EPCs in different forms of stroke, before planning clinicaltrials with EPC injection. In addition, several points need tobe clarified before clinical studies can be started, like the timepoint of transplantation, the cerebral lesions which are fit forEPC treatment, the route and site of cell delivery, and themonitoring of the recovery.44 Other methods to increase EPCnumbers, like drugs (statins, ACE-inhibitors, angiotensinreceptor blockers, and erythropoietin) or growth factorswhich stimulate EPC release from the bone marrow, perhapsalso deserve attention.
ConclusionIn conclusion, EPCs hold great promise in cardiovascularmedicine, both as a marker for an increased cardiovascularrisk and as a therapeutic agent. However, as knowledge onEPCs grows, finetuning is needed on all aspects, from basicscience to clinical practice, to obtain the best possible results.The lack of EPC studies in stroke should instigate vascularneurologists to participate in this interesting line of research,as EPCs could also change pathophysiological and therapeu-tical concepts, which will hopefully improve clinical treat-ments in vascular neurology.
Sources of FundingR.P.W. Rouhl is funded by a research grant of the Netherlands HeartFoundation (grant number 2005 B 022).
DisclosuresNone.
References1. Asahara T, Murohara T, Sullivan A, Silver M, van der Zee R, Li T,
Witzenbichler B, Schatteman G, Isner JM. Isolation of putative progenitorendothelial cells for angiogenesis. Science. 1997;275:964–967.
2. Griese DP, Ehsan A, Melo LG, Kong D, Zhang L, Mann MJ, Pratt RE,Mulligan RC, Dzau VJ. Isolation and transplantation of autologous cir-culating endothelial cells into denuded vessels and prosthetic grafts:Implications for cell-based vascular therapy. Circulation. 2003;108:2710–2715.
3. Urbich C, Dimmeler S. Endothelial progenitor cells: Characterization androle in vascular biology. Circ Res. 2004;95:343–353.
4. Hristov M, Erl W, Weber PC. Endothelial progenitor cells: Mobilization,differentiation, and homing. Arterioscler Thromb Vasc Biol. 2003;23:1185–1189.
5. Khan SS, Solomon MA, McCoy JP Jr. Detection of circulating endothe-lial cells and endothelial progenitor cells by flow cytometry. Cytometry BClin Cytom. 2005;64:1–8.
6. George J, Shmilovich H, Deutsch V, Miller H, Keren G, Roth A. Com-parative analysis of methods for assessment of circulating endothelialprogenitor cells. Tissue Eng. 2006;12:331–335.
7. Yoder MC, Mead LE, Prater D, Krier TR, Mroueh KN, Li F, Krasich R,Temm CJ, Prchal JT, Ingram DA. Redefining endothelial progenitor cellsvia clonal analysis and hematopoietic stem/progenitor cell principals.Blood. 2007;109:1801–1809.
8. Young PP, Vaughan DE, Hatzopoulos AK. Biologic properties ofendothelial progenitor cells and their potential for cell therapy. ProgCardiovasc Dis. 2007;49:421– 429.
9. Zhang SJ, Zhang H, Wei YJ, Su WJ, Liao ZK, Hou M, Zhou JY, Hu SS.Adult endothelial progenitor cells from human peripheral blood maintainmonocyte/macrophage function throughout in vitro culture. Cell Res.2006;16:577–584.
10. Popa ER, Harmsen MC, Tio RA, van der Strate BW, Brouwer LA,Schipper M, Koerts J, De Jongste MJ, Hazenberg A, Hendriks M, vanLuyn MJ. Circulating cd34� progenitor cells modulate host angiogenesisand inflammation in vivo. J Mol Cell Cardiol. 2006;41:86–96.
11. Rookmaaker MB, Verhaar MC, Loomans CJ, Verloop R, Peters E, West-erweel PE, Murohara T, Staal FJ, van Zonneveld AJ, Koolwijk P,Rabelink TJ, van Hinsbergh VW. Cd34� cells home, proliferate, andparticipate in capillary formation, and in combination with cd34� cellsenhance tube formation in a 3-dimensional matrix. Arterioscler ThrombVasc Biol. 2005;25:1843–1850.
12. Harraz M, Jiao C, Hanlon HD, Hartley RS, Schatteman GC. Cd34�blood-derived human endothelial cell progenitors. Stem Cells. 2001;19:304–312.
13. Reyes M, Dudek A, Jahagirdar B, Koodie L, Marker PH, Verfaillie CM.Origin of endothelial progenitors in human postnatal bone marrow. J ClinInvest. 2002;109:337–346.
14. Yin AH, Miraglia S, Zanjani ED, Almeida-Porada G, Ogawa M, LearyAG, Olweus J, Kearney J, Buck DW. Ac133, a novel marker for humanhematopoietic stem and progenitor cells. Blood. 1997;90:5002–5012.
15. Murohara T, Ikeda H, Duan J, Shintani S, Sasaki K, Eguchi H, OnitsukaI, Matsui K, Imaizumi T. Transplanted cord blood-derived endothelialprecursor cells augment postnatal neovascularization. J Clin Invest. 2000;105:1527–1536.
16. Peichev M, Naiyer AJ, Pereira D, Zhu Z, Lane WJ, Williams M, Oz MC,Hicklin DJ, Witte L, Moore MA, Rafii S. Expression of vegfr-2 andac133 by circulating human cd34(�) cells identifies a population offunctional endothelial precursors. Blood. 2000;95:952–958.
17. Werner N, Kosiol S, Schiegl T, Ahlers P, Walenta K, Link A, Bohm M,Nickenig G. Circulating endothelial progenitor cells and cardiovascularoutcomes. N Engl J Med. 2005;353:999–1007.
18. Schmidt-Lucke C, Rossig L, Fichtlscherer S, Vasa M, Britten M, KamperU, Dimmeler S, Zeiher AM. Reduced number of circulating endothelialprogenitor cells predicts future cardiovascular events: Proof of conceptfor the clinical importance of endogenous vascular repair. Circulation.2005;111:2981–2987.
19. Xu QB. Endothelial progenitor cells in angiogenesis. Sheng Li Xue Bao.2005;57:1–6.
20. Hill JM, Zalos G, Halcox JP, Schenke WH, Waclawiw MA, QuyyumiAA, Finkel T. Circulating endothelial progenitor cells, vascular function,and cardiovascular risk. N Engl J Med. 2003;348:593–600.
21. Walter DH, Rittig K, Bahlmann FH, Kirchmair R, Silver M, MurayamaT, Nishimura H, Losordo DW, Asahara T, Isner JM. Statin therapyaccelerates reendothelialization: A novel effect involving mobilizationand incorporation of bone marrow-derived endothelial progenitor cells.Circulation. 2002;105:3017–3024.
22. Werner N, Junk S, Laufs U, Link A, Walenta K, Bohm M, Nickenig G.Intravenous transfusion of endothelial progenitor cells reduces neointimaformation after vascular injury. Circ Res. 2003;93:e17–e24.
23. Fujiyama S, Amano K, Uehira K, Yoshida M, Nishiwaki Y, Nozawa Y,Jin D, Takai S, Miyazaki M, Egashira K, Imada T, Iwasaka T, MatsubaraH. Bone marrow monocyte lineage cells adhere on injured endothelium ina monocyte chemoattractant protein-1-dependent manner and acceleratereendothelialization as endothelial progenitor cells. Circ Res. 2003;93:980–989.
24. Holmen C, Elsheikh E, Stenvinkel P, Qureshi AR, Pettersson E, JalkanenS, Sumitran-Holgersson S. Circulating inflammatory endothelial cellscontribute to endothelial progenitor cell dysfunction in patients withvasculitis and kidney involvement. J Am Soc Nephrol. 2005;16:3110–3120.
25. Ross R. Atherosclerosis–an inflammatory disease. N Engl J Med. 1999;340:115–126.
2164 Stroke July 2008
by guest on February 23, 2013http://stroke.ahajournals.org/Downloaded from
26. Xiao Q, Kiechl S, Patel S, Oberhollenzer F, Weger S, Mayr A, Metzler B,Reindl M, Hu Y, Willeit J, Xu Q. Endothelial progenitor cells, cardio-vascular risk factors, cytokine levels and atherosclerosis-results from alarge population-based study. PLoS ONE. 2007;2:e975.
27. Fadini GP, Agostini C, Sartore S, Avogaro A. Endothelial progenitor cellsin the natural history of atherosclerosis. Atherosclerosis. 2007;194:46–54.
28. Schatteman GC, Hanlon HD, Jiao C, Dodds SG, Christy BA. Blood-derived angioblasts accelerate blood-flow restoration in diabetic mice.J Clin Invest. 2000;106:571–578.
29. Kalka C, Masuda H, Takahashi T, Gordon R, Tepper O, Gravereaux E,Pieczek A, Iwaguro H, Hayashi SI, Isner JM, Asahara T. Vascularendothelial growth factor(165) gene transfer augments circulating endo-thelial progenitor cells in human subjects. Circ Res. 2000;86:1198–1202.
30. Yoon YS, Lee N, Scadova H. Myocardial regeneration with bone-marrow-derived stem cells. Biol Cell. 2005;97:253–263.
31. Carmeliet P. Angiogenesis in health and disease. Nat Med. 2003;9:653–660.
32. Assmus B, Schachinger V, Teupe C, Britten M, Lehmann R, Dobert N,Grunwald F, Aicher A, Urbich C, Martin H, Hoelzer D, Dimmeler S,Zeiher AM. Transplantation of progenitor cells and regenerationenhancement in acute myocardial infarction (topcare-ami). Circulation.2002;106:3009–3017.
33. Assmus B, Honold J, Schachinger V, Britten MB, Fischer-Rasokat U,Lehmann R, Teupe C, Pistorius K, Martin H, Abolmaali ND, Tonn T,Dimmeler S, Zeiher AM. Transcoronary transplantation of progenitorcells after myocardial infarction. N Engl J Med. 2006;355:1222–1232.
34. Numaguchi Y, Sone T, Okumura K, Ishii M, Morita Y, Kubota R,Yokouchi K, Imai H, Harada M, Osanai H, Kondo T, Murohara T. Theimpact of the capability of circulating progenitor cell to differentiate onmyocardial salvage in patients with primary acute myocardial infarction.Circulation. 2006;114:I114–119.
35. Dobert N, Britten M, Assmus B, Berner U, Menzel C, Lehmann R,Hamscho N, Schachinger V, Dimmeler S, Zeiher AM, Grunwald F.Transplantation of progenitor cells after reperfused acute myocardialinfarction: Evaluation of perfusion and myocardial viability with fdg-petand thallium spect. Eur J Nucl Med Mol Imaging. 2004;31:1146–1151.
36. Lev EI, Kleiman NS, Birnbaum Y, Harris D, Korbling M, Estrov Z.Circulating endothelial progenitor cells and coronary collaterals inpatients with non-st segment elevation myocardial infarction. J Vasc Res.2005;42:408–414.
37. Hristov M, Heussen N, Schober A, Weber C. Intracoronary infusion ofautologous bone marrow cells and left ventricular function after acutemyocardial infarction: A meta-analysis. J Cell Mol Med. 2006;10:727–733.
38. Dimmeler S, Zeiher AM, Schneider MD. Unchain my heart: The sci-entific foundations of cardiac repair. J Clin Invest. 2005;115:572–583.
39. Higashi Y, Kimura M, Hara K, Noma K, Jitsuiki D, Nakagawa K, OshimaT, Chayama K, Sueda T, Goto C, Matsubara H, Murohara T, YoshizumiM. Autologous bone-marrow mononuclear cell implantation improvesendothelium-dependent vasodilation in patients with limb ischemia.Circulation. 2004;109:1215–1218.
40. Tateishi-Yuyama E, Matsubara H, Murohara T, Ikeda U, Shintani S,Masaki H, Amano K, Kishimoto Y, Yoshimoto K, Akashi H, Shimada K,Iwasaka T, Imaizumi T. Therapeutic angiogenesis for patients with limbischaemia by autologous transplantation of bone-marrow cells: A pilotstudy and a randomised controlled trial. Lancet. 2002;360:427–435.
41. Taguchi A, Matsuyama T, Moriwaki H, Hayashi T, Hayashida K,Nagatsuka K, Todo K, Mori K, Stern DM, Soma T, Naritomi H. Circu-lating cd34-positive cells provide an index of cerebrovascular function.Circulation. 2004;109:2972–2975.
42. Ghani U, Shuaib A, Salam A, Nasir A, Shuaib U, Jeerakathil T, Sher F,O’Rourke F, Nasser AM, Schwindt B, Todd K. Endothelial progenitorcells during cerebrovascular disease. Stroke. 2005;36:151–153.
43. Ciulla MM, Giorgetti A, Giordano R, Silvestris I, Cortiana M, Paliotti R,Lazzari L. Circulating endothelial progenitor cell colony-forming
capacity in healthy subjects: How does an endothelial colony look like?Am J Cardiol. 2007;100:559–560.
44. Bliss T, Guzman R, Daadi M, Steinberg GK. Cell transplantation therapyfor stroke. Stroke. 2007;38:817–826.
45. Gertz K, Priller J, Kronenberg G, Fink KB, Winter B, Schrock H, Ji S,Milosevic M, Harms C, Bohm M, Dirnagl U, Laufs U, Endres M.Physical activity improves long-term stroke outcome via endothelialnitric oxide synthase-dependent augmentation of neovascularization andcerebral blood flow. Circ Res. 2006;99:1132–1140.
46. Sobrino T, Hurtado O, Moro MA, Rodriguez-Yanez M, Castellanos M,Brea D, Moldes O, Blanco M, Arenillas JF, Leira R, Davalos A,Lizasoain I, Castillo J. The increase of circulating endothelial progenitorcells after acute ischemic stroke is associated with good outcome. Stroke.2007;38:2759–2764.
47. Zhang ZG, Zhang L, Jiang Q, Chopp M. Bone marrow-derived endothe-lial progenitor cells participate in cerebral neovascularization after focalcerebral ischemia in the adult mouse. Circ Res. 2002;90:284–288.
48. Galimi F, Summers RG, van Praag H, Verma IM, Gage FH. A role forbone marrow-derived cells in the vasculature of noninjured cns. Blood.2005;105:2400–2402.
49. Slevin M, Kumar P, Gaffney J, Kumar S, Krupinski J. Can angiogenesisbe exploited to improve stroke outcome? Mechanisms and therapeuticpotential. Clin Sci (Lond). 2006;111:171–183.
50. Thored P, Wood J, Arvidsson A, Cammenga J, Kokaia Z, Lindvall O.Long-term neuroblast migration along blood vessels in an area withtransient angiogenesis and increased vascularization after stroke. Stroke.2007;38:3032–3039.
51. Schanzer A, Wachs FP, Wilhelm D, Acker T, Cooper-Kuhn C, Beck H,Winkler J, Aigner L, Plate KH, Kuhn HG. Direct stimulation of adultneural stem cells in vitro and neurogenesis in vivo by vascular endothelialgrowth factor. Brain Pathol. 2004;14:237–248.
52. Chen J, Zhang ZG, Li Y, Wang L, Xu YX, Gautam SC, Lu M, Zhu Z,Chopp M. Intravenous administration of human bone marrow stromalcells induces angiogenesis in the ischemic boundary zone after stroke inrats. Circ Res. 2003;92:692–699.
53. Taguchi A, Soma T, Tanaka H, Kanda T, Nishimura H, Yoshikawa H,Tsukamoto Y, Iso H, Fujimori Y, Stern DM, Naritomi H, Matsuyama T.Administration of cd34� cells after stroke enhances neurogenesis viaangiogenesis in a mouse model. J Clin Invest. 2004;114:330–338.
54. Zhao LR, Duan WM, Reyes M, Keene CD, Verfaillie CM, Low WC.Human bone marrow stem cells exhibit neural phenotypes and ameliorateneurological deficits after grafting into the ischemic brain of rats. ExpNeurol. 2002;174:11–20.
55. Chen J, Sanberg PR, Li Y, Wang L, Lu M, Willing AE, Sanchez-RamosJ, Chopp M. Intravenous administration of human umbilical cord bloodreduces behavioral deficits after stroke in rats. Stroke. 2001;32:2682–2688.
56. Vendrame M, Cassady J, Newcomb J, Butler T, Pennypacker KR, ZigovaT, Sanberg CD, Sanberg PR, Willing AE. Infusion of human umbilicalcord blood cells in a rat model of stroke dose-dependently rescuesbehavioral deficits and reduces infarct volume. Stroke. 2004;35:2390–2395.
57. Fernando MS, Simpson JE, Matthews F, Brayne C, Lewis CE, Barber R,Kalaria RN, Forster G, Esteves F, Wharton SB, Shaw PJ, O’Brien JT,Ince PG. White matter lesions in an unselected cohort of the elderly:Molecular pathology suggests origin from chronic hypoperfusion injury.Stroke. 2006;37:1391–1398.
58. Wardlaw JM, Sandercock PA, Dennis MS, Starr J. Is breakdown of theblood-brain barrier responsible for lacunar stroke, leukoaraiosis, anddementia? Stroke. 2003;34:806–812.
59. Dufouil C, Chalmers J, Coskun O, Besancon V, Bousser MG, Guillon P,MacMahon S, Mazoyer B, Neal B, Woodward M, Tzourio-Mazoyer N,Tzourio C. Effects of blood pressure lowering on cerebral white matterhyperintensities in patients with stroke: The progress (perindopril pro-tection against recurrent stroke study) magnetic resonance imagingsubstudy. Circulation. 2005;112:1644–1650.
Rouhl et al Endothelial Progenitor Cell Research in Stroke 2165
by guest on February 23, 2013http://stroke.ahajournals.org/Downloaded from





























