Embed Size (px)
Citation preview
CHRONIC PAIN MANAGEMENT TRAINING MODULE FOR PRIMARY CARE MINISTRY OF HEALTH MALAYSIA
Dr Ruziaton bt Hasim
Dr Salinah bt Mohd Mudri
Pakar Perubatan Keluarga
JOINT PAIN In Primary Care
CHRONIC PAIN MANAGEMENT TRAINING MODULE FOR PRIMARY CARE MINISTRY OF HEALTH MALAYSIA
INTRODUCTION
• Joint pain is discomfort that arises from any joint
• It is sometimes called arthritis, arthralgia and rheumatism1
• Arthritis: an inflammatory conditions of the joints
• Arthralgia: joint pain of non inflammatory conditions
• Rheumatism: pain at or around a joint which is not due to joint2
• Chronic pain is defined as a pain that lasts longer than 3 months.
CHRONIC PAIN MANAGEMENT TRAINING MODULE FOR PRIMARY CARE MINISTRY OF HEALTH MALAYSIA
• Pain
• Stiffness
• Swelling
• Limitation of motion
• Weakness
• Inflammatory joint disease : pain occur at rest and with motion, worse at the beginning of usage than at the end.
• Non-inflammatory joint disease (ie, traumatic, or mechanical): pain occurs during movement, improves quickly with rest
SIGNS AND SYMPTOMS OF JOINT PAIN
CHRONIC PAIN MANAGEMENT TRAINING MODULE FOR PRIMARY CARE MINISTRY OF HEALTH MALAYSIA
SHOULDER PAIN
CHRONIC PAIN MANAGEMENT TRAINING MODULE FOR PRIMARY CARE MINISTRY OF HEALTH MALAYSIA
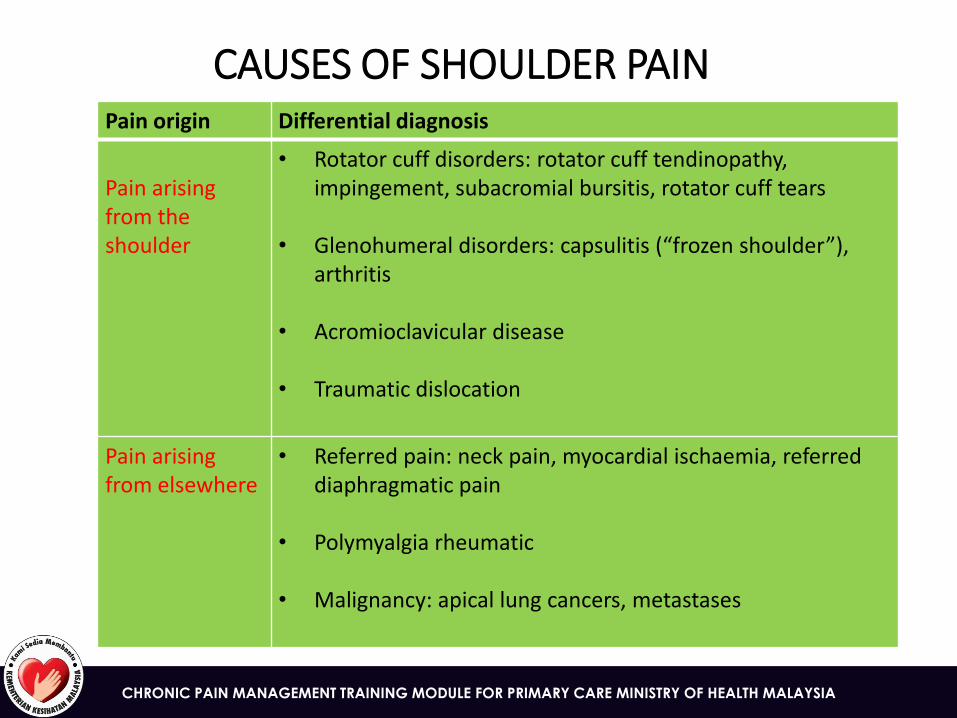
CAUSES OF SHOULDER PAIN Pain origin Differential diagnosis
Pain arising from the shoulder
• Rotator cuff disorders: rotator cuff tendinopathy, impingement, subacromial bursitis, rotator cuff tears
• Glenohumeral disorders: capsulitis (“frozen shoulder”), arthritis
• Acromioclavicular disease
• Traumatic dislocation
Pain arising from elsewhere
• Referred pain: neck pain, myocardial ischaemia, referred diaphragmatic pain
• Polymyalgia rheumatic
• Malignancy: apical lung cancers, metastases
CHRONIC PAIN MANAGEMENT TRAINING MODULE FOR PRIMARY CARE MINISTRY OF HEALTH MALAYSIA
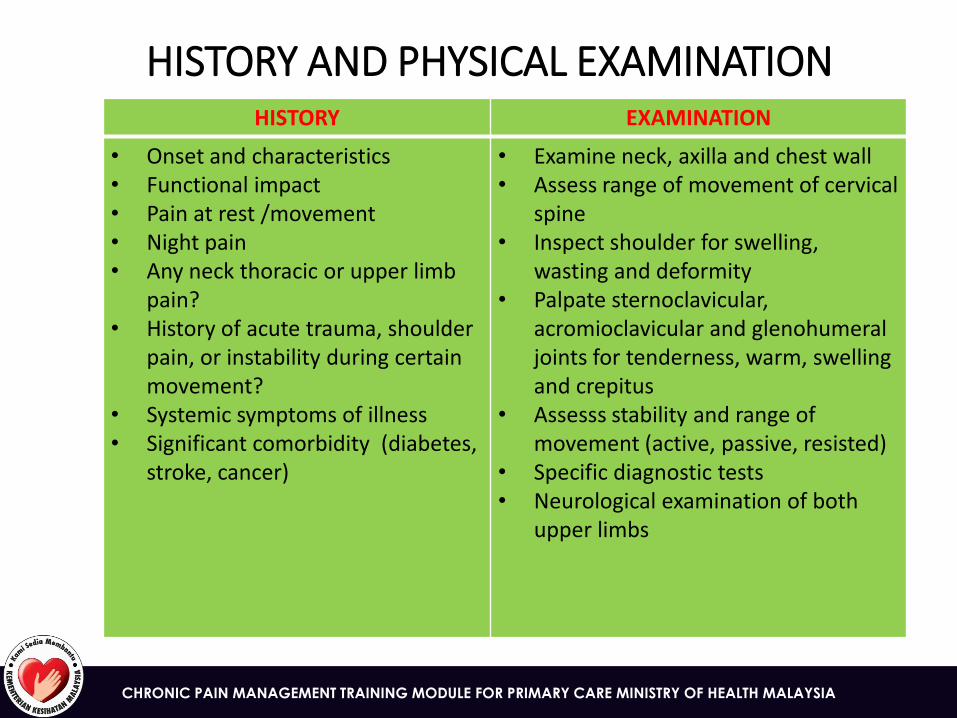
HISTORY AND PHYSICAL EXAMINATION HISTORY EXAMINATION
• Onset and characteristics • Functional impact • Pain at rest /movement • Night pain • Any neck thoracic or upper limb
pain? • History of acute trauma, shoulder
pain, or instability during certain movement?
• Systemic symptoms of illness • Significant comorbidity (diabetes,
stroke, cancer)
• Examine neck, axilla and chest wall • Assess range of movement of cervical
spine • Inspect shoulder for swelling,
wasting and deformity • Palpate sternoclavicular,
acromioclavicular and glenohumeral joints for tenderness, warm, swelling and crepitus
• Assesss stability and range of movement (active, passive, resisted)
• Specific diagnostic tests • Neurological examination of both
upper limbs
CHRONIC PAIN MANAGEMENT TRAINING MODULE FOR PRIMARY CARE MINISTRY OF HEALTH MALAYSIA
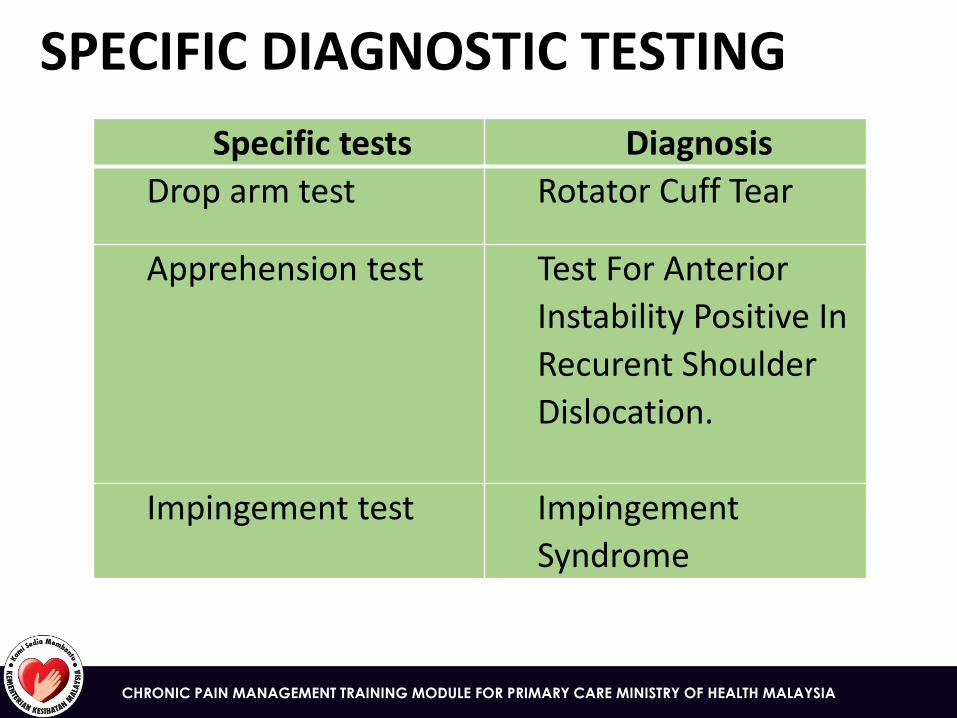
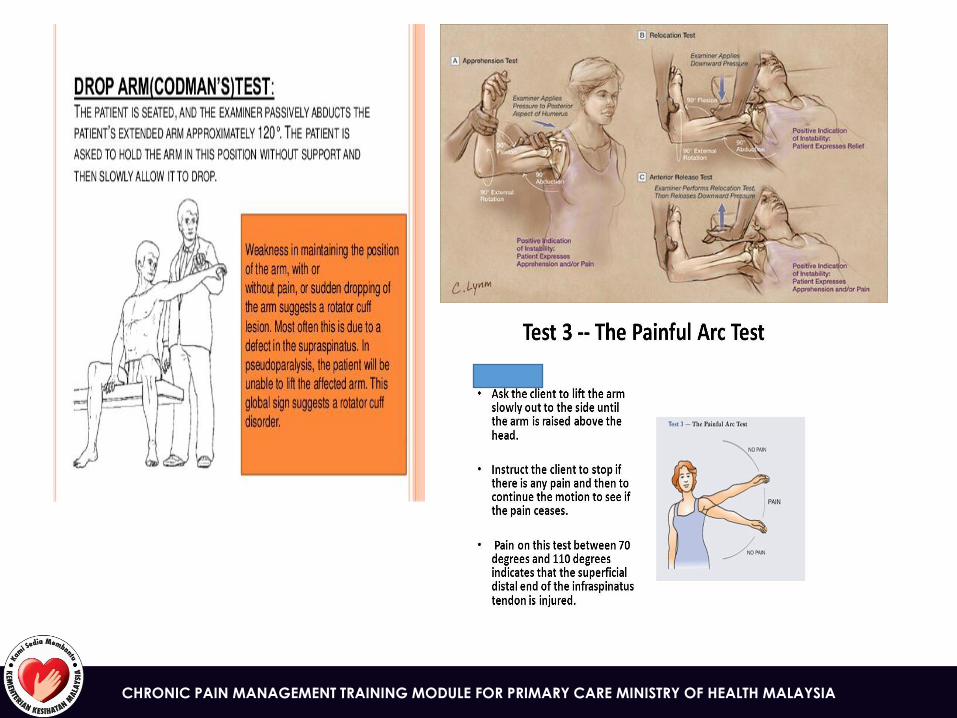
SPECIFIC DIAGNOSTIC TESTING
Specific tests Diagnosis
Drop arm test Rotator Cuff Tear
Apprehension test Test For Anterior
Instability Positive In
Recurent Shoulder
Dislocation.
Impingement test Impingement
Syndrome
CHRONIC PAIN MANAGEMENT TRAINING MODULE FOR PRIMARY CARE MINISTRY OF HEALTH MALAYSIA
CHRONIC PAIN MANAGEMENT TRAINING MODULE FOR PRIMARY CARE MINISTRY OF HEALTH MALAYSIA
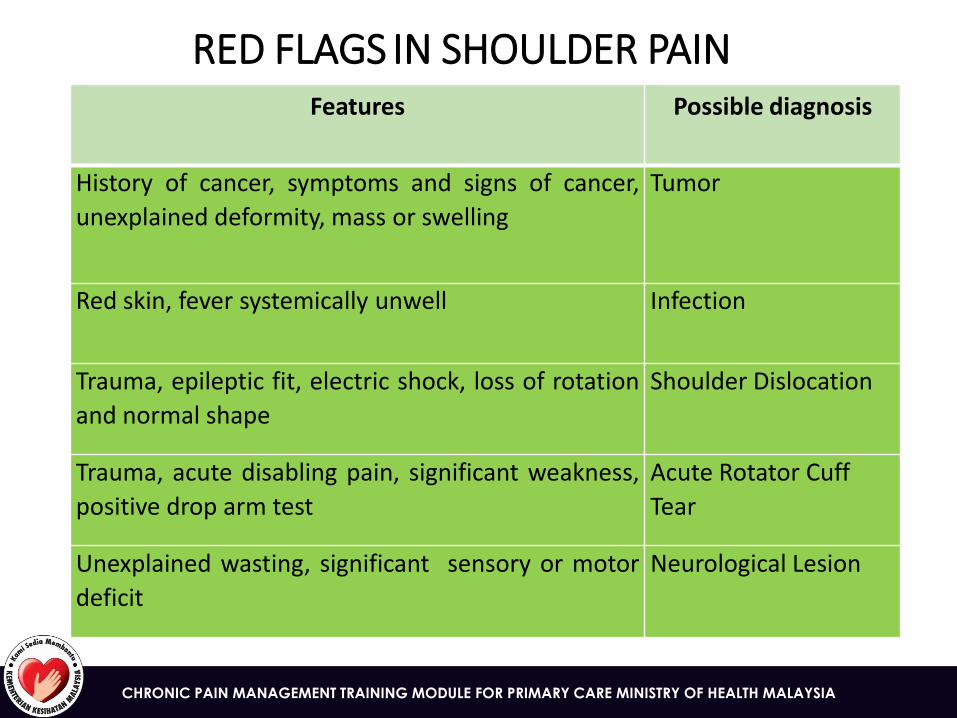
RED FLAGS IN SHOULDER PAIN Features Possible diagnosis
History of cancer, symptoms and signs of cancer,
unexplained deformity, mass or swelling
Tumor
Red skin, fever systemically unwell Infection
Trauma, epileptic fit, electric shock, loss of rotation
and normal shape
Shoulder Dislocation
Trauma, acute disabling pain, significant weakness,
positive drop arm test
Acute Rotator Cuff
Tear
Unexplained wasting, significant sensory or motor
deficit
Neurological Lesion
CHRONIC PAIN MANAGEMENT TRAINING MODULE FOR PRIMARY CARE MINISTRY OF HEALTH MALAYSIA
CHRONIC PAIN MANAGEMENT TRAINING MODULE FOR PRIMARY CARE MINISTRY OF HEALTH MALAYSIA
TREATMENT
• A holistic approach: pharmacological & non-pharmacological
• Adequate analgesia (paracetamol, NSAIDs drugs - regular / PRN basis)
• Self-motivation
• Encourage activity
• Give written patient information sheet.
REFERRAL CRITERIA
• Pain lasting more than 6 months with functional disability
• Diagnostic uncertainty
• Positive Red flags.
CHRONIC PAIN MANAGEMENT TRAINING MODULE FOR PRIMARY CARE MINISTRY OF HEALTH MALAYSIA
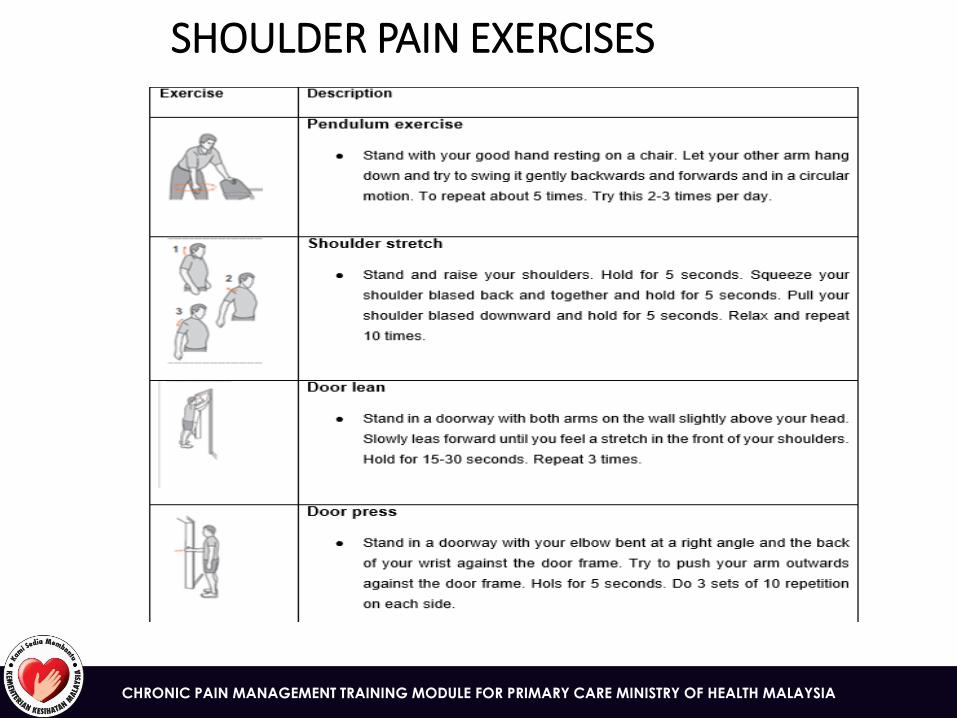
SHOULDER PAIN EXERCISES
CHRONIC PAIN MANAGEMENT TRAINING MODULE FOR PRIMARY CARE MINISTRY OF HEALTH MALAYSIA
HIP PAIN
CHRONIC PAIN MANAGEMENT TRAINING MODULE FOR PRIMARY CARE MINISTRY OF HEALTH MALAYSIA
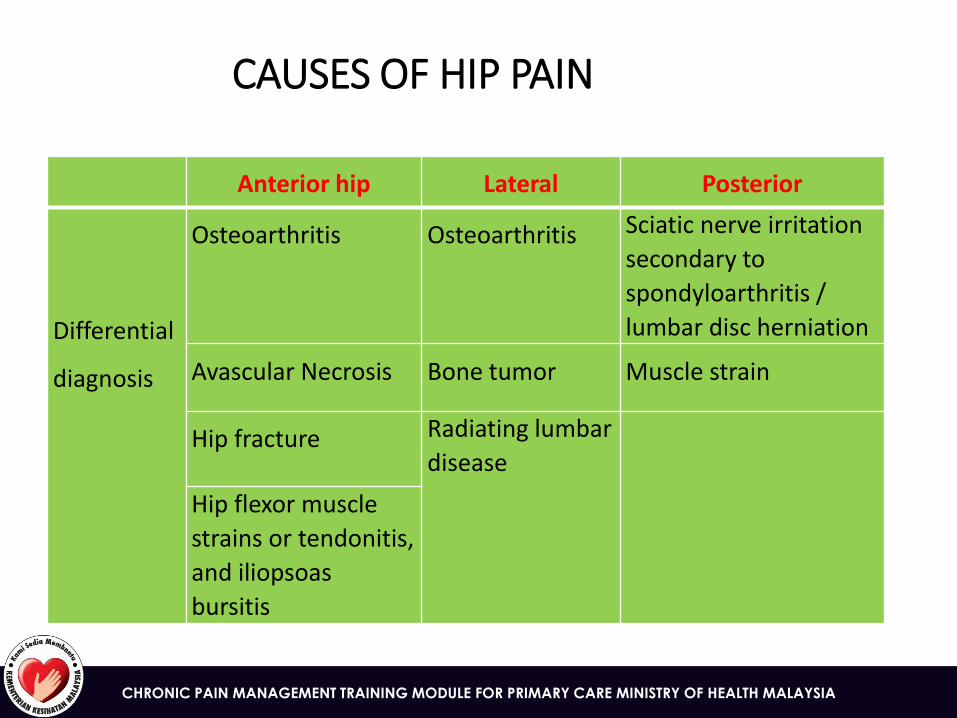
CAUSES OF HIP PAIN
Anterior hip Lateral Posterior
Differential
diagnosis
Osteoarthritis Osteoarthritis Sciatic nerve irritation
secondary to
spondyloarthritis /
lumbar disc herniation
Avascular Necrosis Bone tumor Muscle strain
Hip fracture Radiating lumbar
disease
Hip flexor muscle
strains or tendonitis,
and iliopsoas
bursitis
CHRONIC PAIN MANAGEMENT TRAINING MODULE FOR PRIMARY CARE MINISTRY OF HEALTH MALAYSIA
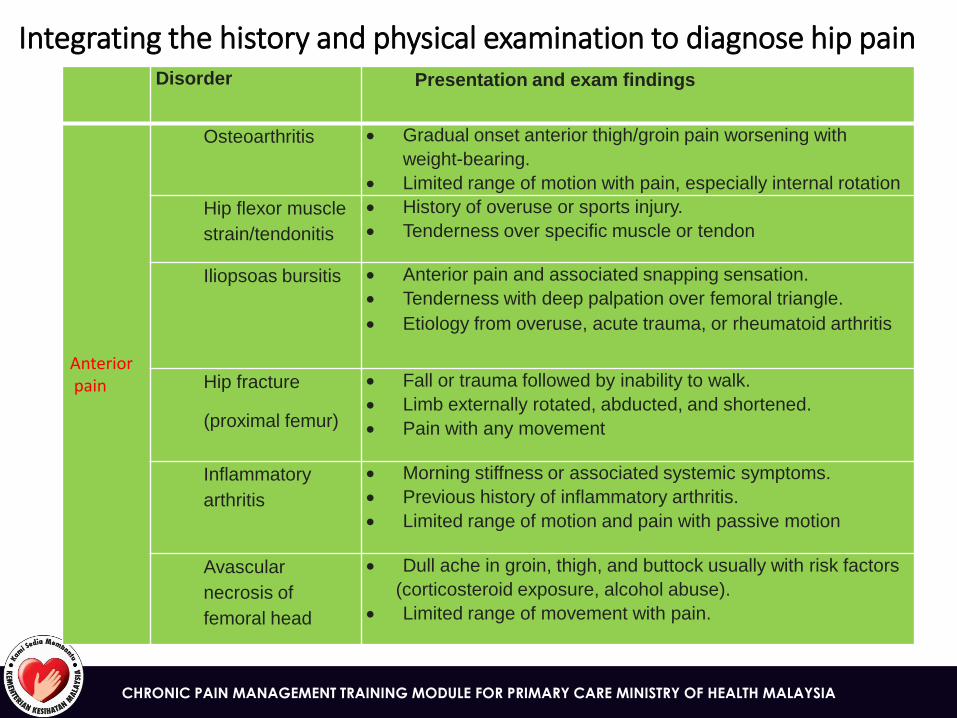
Integrating the history and physical examination to diagnose hip pain Disorder
Presentation and exam findings
Anterior pain
Osteoarthritis Gradual onset anterior thigh/groin pain worsening with
weight-bearing.
Limited range of motion with pain, especially internal rotation
Hip flexor muscle
strain/tendonitis
History of overuse or sports injury.
Tenderness over specific muscle or tendon
Iliopsoas bursitis Anterior pain and associated snapping sensation.
Tenderness with deep palpation over femoral triangle.
Etiology from overuse, acute trauma, or rheumatoid arthritis
Hip fracture
(proximal femur)
Fall or trauma followed by inability to walk.
Limb externally rotated, abducted, and shortened.
Pain with any movement
Inflammatory
arthritis
Morning stiffness or associated systemic symptoms.
Previous history of inflammatory arthritis.
Limited range of motion and pain with passive motion
Avascular
necrosis of
femoral head
Dull ache in groin, thigh, and buttock usually with risk factors
(corticosteroid exposure, alcohol abuse).
Limited range of movement with pain.
CHRONIC PAIN MANAGEMENT TRAINING MODULE FOR PRIMARY CARE MINISTRY OF HEALTH MALAYSIA
RED FLAGS OF HIP PAIN
• Fever, malaise
• Night sweats, night pain, weight loss
• Previous history of cancer
• Trauma/assault (fall, blow, lifting)
• Intravenous drug abuse
• Long term use of immunosuppressants
• Pain that is not relieved with rest and continues through the night
** An accumulation of multiple red flags requires immediate medical referral
CHRONIC PAIN MANAGEMENT TRAINING MODULE FOR PRIMARY CARE MINISTRY OF HEALTH MALAYSIA
CHRONIC PAIN MANAGEMENT TRAINING MODULE FOR PRIMARY CARE MINISTRY OF HEALTH MALAYSIA
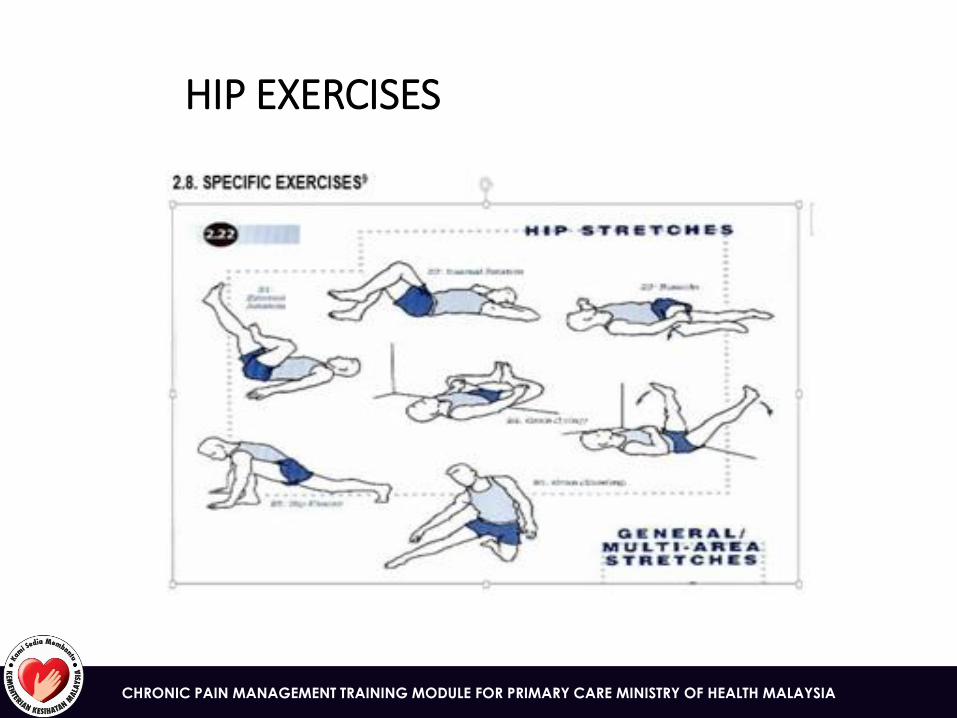
HIP EXERCISES

CHRONIC PAIN MANAGEMENT TRAINING MODULE FOR PRIMARY CARE MINISTRY OF HEALTH MALAYSIA
KNEE PAIN
CHRONIC PAIN MANAGEMENT TRAINING MODULE FOR PRIMARY CARE MINISTRY OF HEALTH MALAYSIA
CAUSES OF KNEE PAIN
• The knee joint is prone to injury because of its complexity and weight bearing function.
• The most common knee problem in primary care are:
• Ligament injuries
• Meniscus injuries
• Osteoarthritis
CHRONIC PAIN MANAGEMENT TRAINING MODULE FOR PRIMARY CARE MINISTRY OF HEALTH MALAYSIA
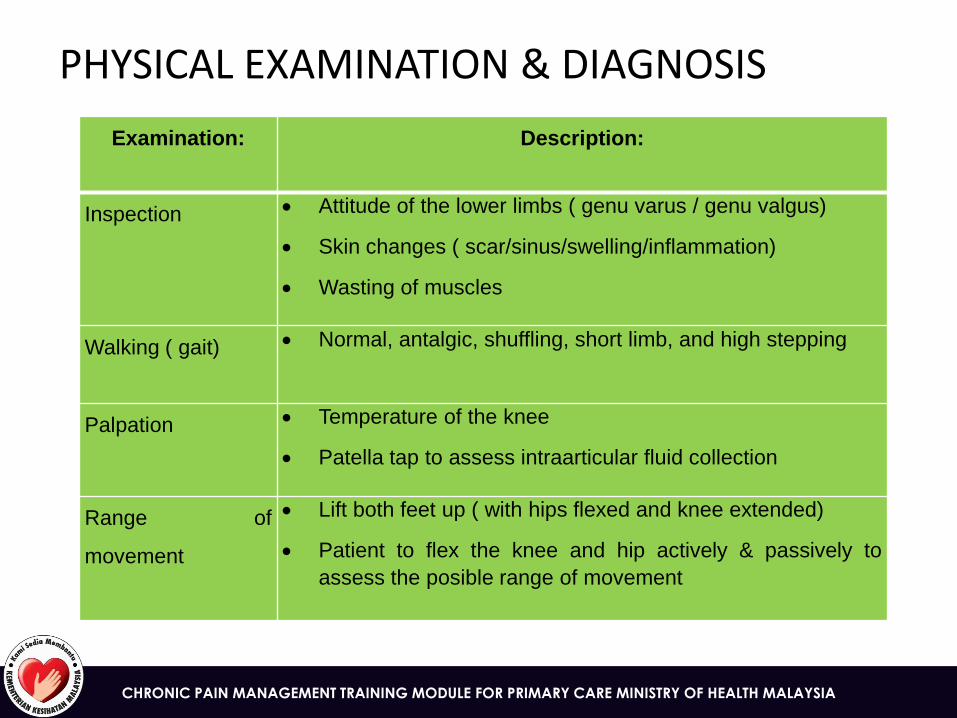
PHYSICAL EXAMINATION & DIAGNOSIS
Examination: Description:
Inspection Attitude of the lower limbs ( genu varus / genu valgus)
Skin changes ( scar/sinus/swelling/inflammation)
Wasting of muscles
Walking ( gait) Normal, antalgic, shuffling, short limb, and high stepping
Palpation Temperature of the knee
Patella tap to assess intraarticular fluid collection
Range of
movement
Lift both feet up ( with hips flexed and knee extended)
Patient to flex the knee and hip actively & passively to
assess the posible range of movement
CHRONIC PAIN MANAGEMENT TRAINING MODULE FOR PRIMARY CARE MINISTRY OF HEALTH MALAYSIA
KNEE LIGAMENTAL INJURIES
SIGNS AND SYMPTOMS
• Ligaments injuries involve high energy injuries
• Patients may present with knee swelling within an hour or two and associated with ‘clunk’ or ‘popping’ sensation at the time of injury
• Once pain subsides patients would feel instability
CHRONIC PAIN MANAGEMENT TRAINING MODULE FOR PRIMARY CARE MINISTRY OF HEALTH MALAYSIA
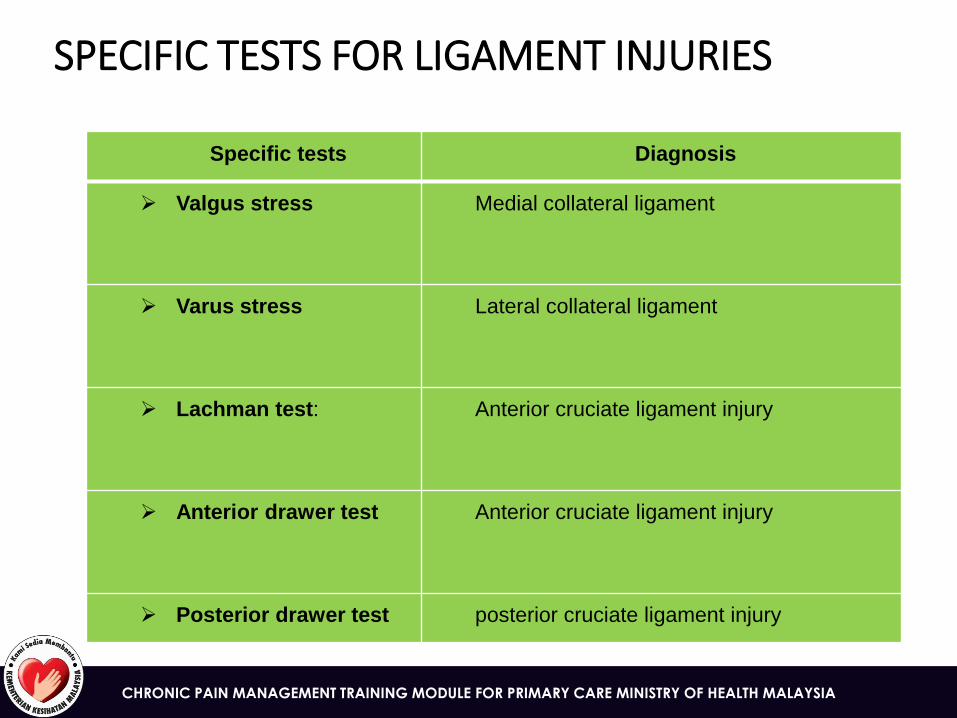
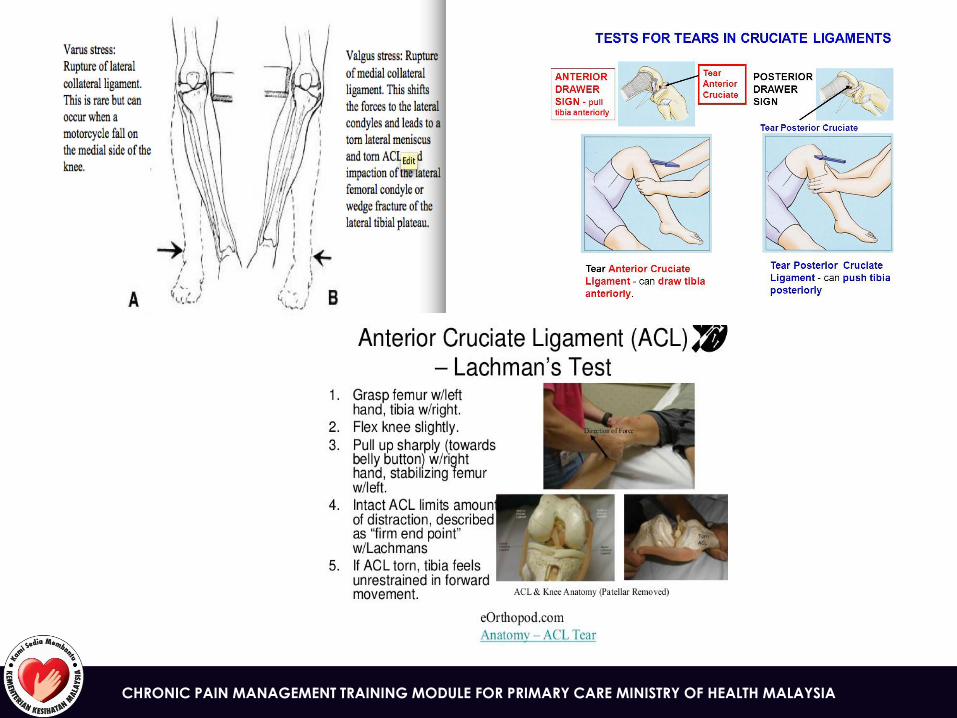
SPECIFIC TESTS FOR LIGAMENT INJURIES
Specific tests Diagnosis
Valgus stress Medial collateral ligament
Varus stress Lateral collateral ligament
Lachman test: Anterior cruciate ligament injury
Anterior drawer test Anterior cruciate ligament injury
Posterior drawer test posterior cruciate ligament injury
CHRONIC PAIN MANAGEMENT TRAINING MODULE FOR PRIMARY CARE MINISTRY OF HEALTH MALAYSIA
CHRONIC PAIN MANAGEMENT TRAINING MODULE FOR PRIMARY CARE MINISTRY OF HEALTH MALAYSIA
LIGAMENTAL INJURIES:TREATMENT OPTIONS
• In general, torn collateral ligaments heal without surgery whilst torn cruciate ligaments require surgery.
• Non pharmacology treatment: ACL performance brace
• Surgery: ligaments replacement with a graft.
CHRONIC PAIN MANAGEMENT TRAINING MODULE FOR PRIMARY CARE MINISTRY OF HEALTH MALAYSIA
Signs and symptoms:
• Presented with pain associated with trauma, mechanical symptoms and joints swelling.
• History of locking episodes.
Physical examination & diagnosis:
• Joint line tenderness & joint line pain with deep flexion associated with swelling / effusion over the point tenderness
MENISCUS INJURIES
CHRONIC PAIN MANAGEMENT TRAINING MODULE FOR PRIMARY CARE MINISTRY OF HEALTH MALAYSIA
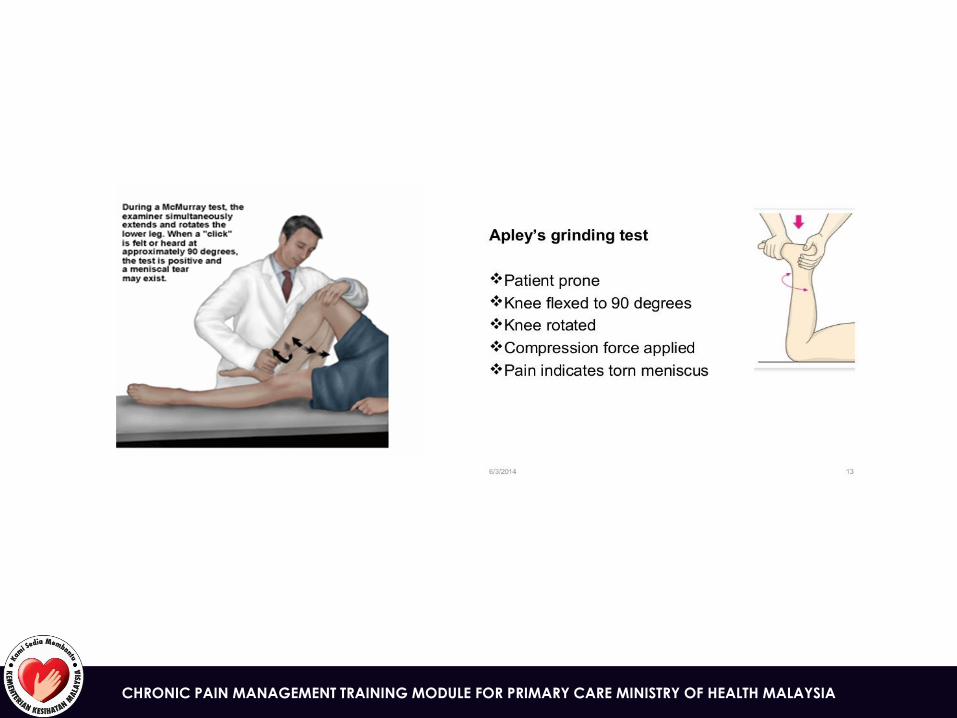
SPECIFIC TESTS FOR MENISCUS INJURY
Specific
tests
How to perform the test Diagnosis
MC
MURRAY’S
TEST
• Physicians flexing the patient hip &
knee and palpating for a pop or click as
the tibia is externally or internally
rotated.
• Assess medial / lateral
meniscus tear
APLEY /
GRINDING
TEST
• Test was performed with patient in
prone position by rotating the tibia on
the femur and applying compression to
reproduce join line pain.
• Medial knee join line
tenderness indicates medial
meniscus tear & lateral knee
join line pain tenderness
indicates lateral meniscus
tear.
CHRONIC PAIN MANAGEMENT TRAINING MODULE FOR PRIMARY CARE MINISTRY OF HEALTH MALAYSIA
CHRONIC PAIN MANAGEMENT TRAINING MODULE FOR PRIMARY CARE MINISTRY OF HEALTH MALAYSIA
MENISCUS INJURY: TREATMENT OPTIONS
• Surgery: in general meniscus tear require arthroscopy surgery to maximize the shock absorption in the joint.
• Removal: if repair can’t be done, removal of the torn meniscus will be done and the particular cartilage will now take over the role of absorber.
CHRONIC PAIN MANAGEMENT TRAINING MODULE FOR PRIMARY CARE MINISTRY OF HEALTH MALAYSIA
Signs and symptoms
• joint pain, stiffness and reduced range of motions.
Physical examination & dignosis
• joint line tenderness, effusion & reduce range of movement
KNEE OSTEOARTHRITIS
CHRONIC PAIN MANAGEMENT TRAINING MODULE FOR PRIMARY CARE MINISTRY OF HEALTH MALAYSIA
KNEE ARTHRITIS: TREATMENT OPTIONS
Non surgical treatment:
• Anti- inflammatory medicines
• Supplements
• Braces
• Corticosteroids shots / therapeutics injections
• Viscosupplementation shots
• Weight loss
• Cane, crutches, walker
• Physiotherapy
Surgical treatment:
• Unicompartmental knee replacement
• Total knee replacement
CHRONIC PAIN MANAGEMENT TRAINING MODULE FOR PRIMARY CARE MINISTRY OF HEALTH MALAYSIA
KNEE ARTHRITIS
Red flags in knee pain:
• Systemic Complaints – fever, weight loss, pain at rest, night pain
When to refer
• Inability to bear weight
• Extreme of age
• Locking
• Bilateral knee pain
• Other joint involvement – e.g: Hip
CHRONIC PAIN MANAGEMENT TRAINING MODULE FOR PRIMARY CARE MINISTRY OF HEALTH MALAYSIA
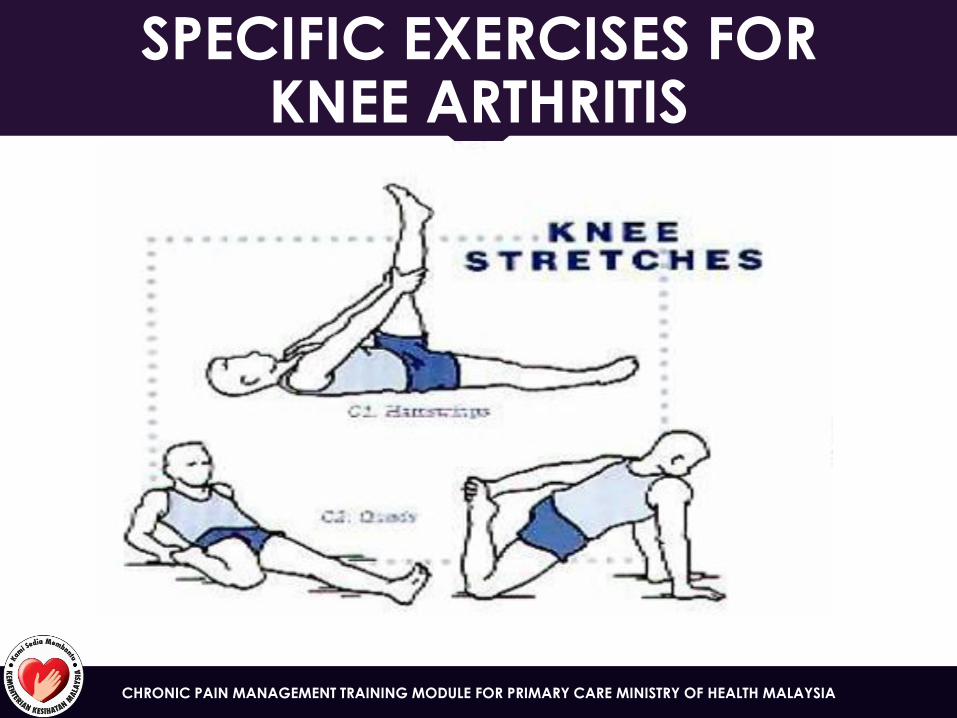
SPECIFIC EXERCISES FOR KNEE ARTHRITIS

CHRONIC PAIN MANAGEMENT TRAINING MODULE FOR PRIMARY CARE MINISTRY OF HEALTH MALAYSIA
Thank you